
Assessing the Conceptualizations of Coping and Resilience in LGBTQ2S+ People with Cancer: Working towards Greater Awareness in Cancer Care




Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Current Considerations and Experiences of LGBTQ2S+ Cancer Patients
1.2. Strengths-Based Research: Coping and Resilience
1.3. Primary Study Aims
2. Materials and Methods
2.1. Study Design
Utilizing a Patient Oriented Approach
2.2. Participants
Sample Size Justification
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Sample Demographics
3.2. Qualitative Findings
3.2.1. Experiencing Support Professionally and Interpersonally
“It was also very trauma-based, trauma-informed. As somebody who has trauma, most queer people do, but as somebody who has trauma and also had trauma around this biopsy, [the health care provider] even sent me to places where they would not misgender me.”(S10)
“I think most of the doctors lack understanding and sensitivity, they don’t know how to deal with [LGBTQ2S+ people with cancer], they don’t know how they can handle us.”(S4)
“I talked to my friends. I talked, I talked, and I talked. And I was uninhibited about what I said. I just let it all out. Let it all out, release it. I wasn’t looking for advice, and they knew that. I wasn’t looking for how could they give me advice? What could they say? But they were listening. They were good sounding boards, and that’s what I needed for me, good sounding boards.”(S6)
3.2.2. Regaining Control in Life
“I think coping is getting along with a certain condition, with a certain thing.”(S4)
“Even like I said, with my discussion of my identity, it kind of feels like all those years [during cancer treatment?] were sort of just spent lived in like a weird dream, rather than something that I went through.”(S1)
“Maybe eating a healthy diet. I think, by that I was taking care of myself, and maybe finding ways to manage my stress because sometimes I was stressed, and I think it was not good for my health.”(S4)
“So, I struggled a lot with really restrictive eating. I struggled with just really severe control over my body and body image. Just control and a lot of avenues in my life became a huge way of coping with illness. But I think in my mind, I saw it as just something else. I was like, no, you just—you know, you probably don’t have an eating problem or image problems and I really didn’t make the connection.”(S1)
3.2.3. Making Meaning of Conflicting Identities
“Cancer is a very alienating thing, because it’s hard to understand if you’ve not gone through it. And for a lot of people, and certainly for a large portion of my life, being queer was a very alienating thing. And adding the two together is, I was just going say it’s doubly hard.”(S2)
“Everything I’ve read at first about mastectomies was about like deciding about reconstruction. And I just, I wanted to hear from people who had made the choice not to have reconstruction, or people who—I wanted to hear from queer people, I wanted to know how someone who wasn’t concerned about femininity or someone who might be gender fluid felt about having a very strongly gendered cancer.”(S2)
“So, maybe—let me use myself—let me just explain it to you. So, I had breast cancer, and I was trying to access healthcare. So, I went to the first doctor, and he was like, “you know, you, you, you look like you are a man, and you have breasts”, so things like that.”(S4)
“All the health professionals that I encounter, not that every one of them knows that I’m gay, I mean, some of them don’t need that information, unless I disclose that to them.”(S3)
“Well, it was kind of frustrating because I knew there had to be some books out there that weren’t about becoming beautiful again, after breast cancer or whatever. There’s a whole hell of a lot of pink books, they’ve all got cupcakes on the cover, because cupcakes apparently are the pastry that looks most like breasts, you can put them on the cover of a book. So, I was doing a lot of eye rolling when I was trying to look.”(S2)
“It’s very much parallel to the feeling you get when you recognize queer experience right? And so, reading the books I would have that same experience, but a sort of a double I see you, in the sense of, oh, I see you as a queer person. I see you as a queer person with a highly gendered cancer that is marketed in ways that are, super tied to femininity, which is a thing that many queer women who have breast cancer have had to struggle with already at some point. And so, it was just that it’s—it was exactly like being out in the world and encountering someone where there’s that moment of acknowledgement.”(S2)
“Even in kind of, for example, queer-related resources for oncology. Maybe having some nuance for minority groups within that. So, I obviously am Indian, like a person of color. So, I think having something with this. I know, now we’re looking for a subgroup within that gay survivor subgroup, and that Indian gay survivors are going to be very few people, I’m sure, but just to have a resource or something.”(S9)
3.2.4. Drawing on Existing Coping Strategies
“I guess in my awareness of my cancer journey, I would say there’s definitely been a marked difference in the point in time when I recognized that cancer was something that actually was a problem.”(S1)
“Yeah, just the sort of sense of, I will have to shift my sense of self in order to sort of accept what my limits are on a given day. So that was a big part of it for me, during treatment.”(S2)
“I joined the Thyroid Cancer Association as soon as I found out, so they had lot of literature, researchers that were extremely helpful. Pamphlets, free information, so I did my own research a lot.”(S3)
“I think it kind of became this weird cycle of—I would share my story. And obviously, I would kind of come across in this way where it’s, “I’m getting through it, and I’m fine”. I’ll get a lot of positive response and praise on that, where it’s like, “oh, you’re so strong and, I can’t believe you’re able to get through it like this”. And it kind of became this, feedback cycle where it’s, the more I repress my emotions, the more positive response.”(S2)
“I think there’s definitely kind of an awareness and a healing component to resilience to where there actually is a part of you that does deal with the problems you’re facing.”(S1)
“I started seeing a therapist back when I was at the Children’s too. So, their psychosocial oncology team, I had someone with me, I think got assigned pretty soon after my cancer journey started there. I mean, yeah, I think having a person there, that’s not part of the rest of your life is just extremely helpful and kind of navigating school’s challenges, especially someone who’s knowledgeable in cancer.”(S1)
3.2.5. Current Gaps in Service Provision
“And I was saying to my therapist, I said there needs to be a rehab. After you are all done, and they send you off, go fend for yourself, there needs to be a rehab. You need to get a dietitian in there. You need to get a physical therapist in there. You got to get a massager in there. You need a mental health person in there. There needs to be a rehab center for after cancer.”(S6)
“One thing that I would like to see maybe is understanding of healthcare providers and the support team at the hospitals. Maybe—if they can gain more understanding of, of LGBTQ individuals, I think it can be better. That’s the only thing I think maybe they’re lacking.”(S4)
“So later on, I went back and I told that nurse about Queering Cancer. And she said, well, thanks for letting me know, that’s really great. I’ll take a look at it, we have to take a look at all of our resources and sort of, vet them first to decide what we include in our official patient information... But I was really disappointed because my last appointment in October they had updated the brochure, and they did not have that included. And that was a shame, I thought, because even though the proportion of their patients who are queer is probably relatively small, we’re still there. And we still need information and stories and that kind of thing. So, I wish that had taken me up on that.”(S2)
“I think definitely someone telling me you can grieve about this, you’re allowed to, you know, want these resources and you’re allowed to be upset and you’re allowed to be affected. I think for me, that’s probably the only thing that might have, kind of gone through to me to say, okay, maybe I will look at some of [these resources].”(S1)
4. Discussion
4.1. Conceptualization of Coping and Resilience
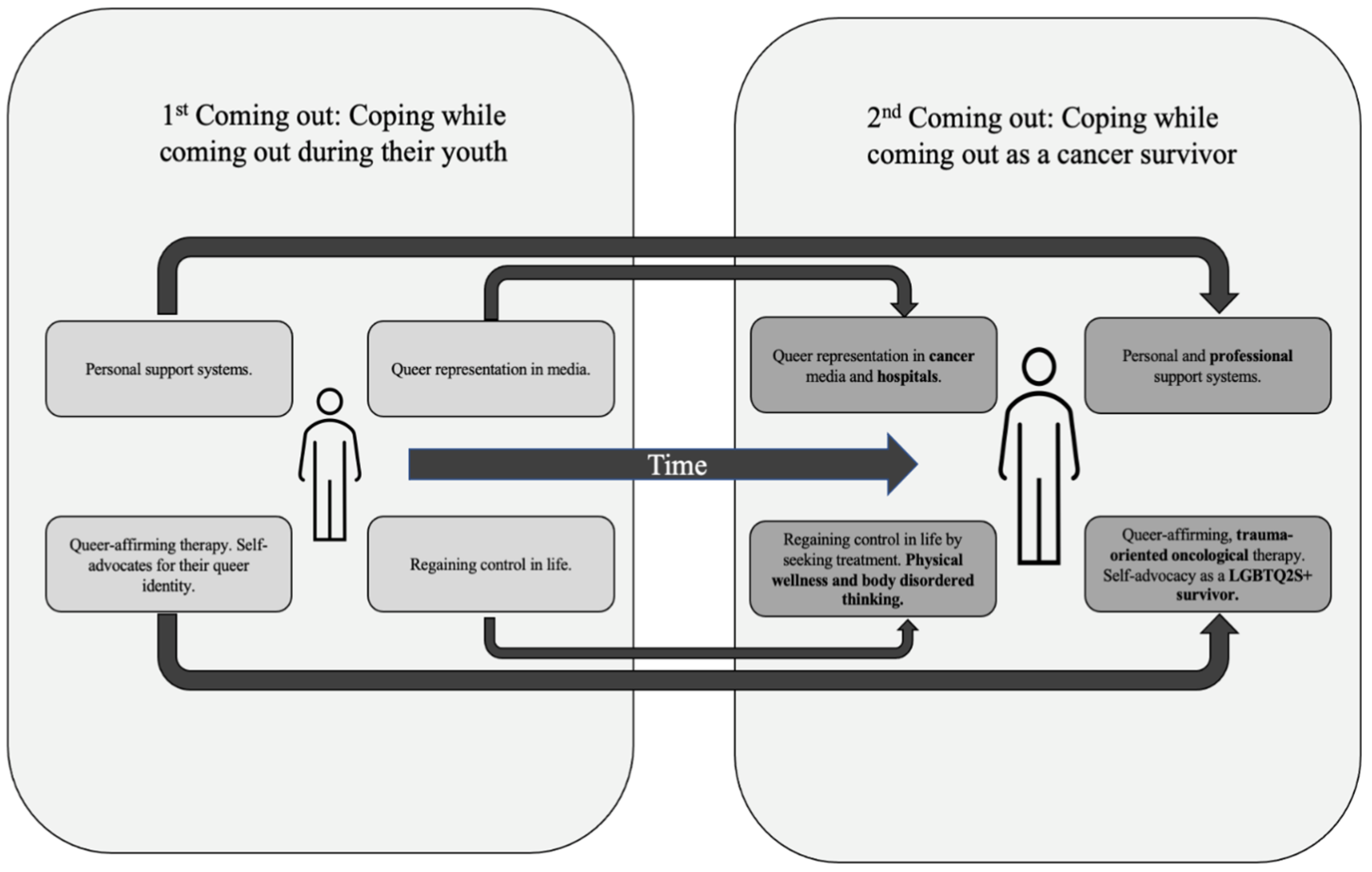
4.2. Exploring the ‘Second Coming-Out’ Phenomenon
4.2.1. Support Systems
4.2.2. Regaining Control
4.2.3. Queer Representation in Media
4.2.4. Queer-Affirming Support and Self-Advocacy
4.3. Implications and Future Directions: A Model for LGBTQ2S+ Resilience-Focused Care
4.4. Strengths and Limitations
5. Conclusions
“But just that having cancer is alienating from the world around you. Because when you’re in the midst of it, no one else can really understand it because it’s so very, very isolating. And then being queer is, can also involve a lot of that feeling of being isolated. And so, when you find people who care or understand or are interested, that’s just such a good feeling. And so, thank you for doing this research, because that’s how this feels.”(S2)
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- (1)
- What is your current age in years and date of birth?
- (2)
- What is your gender?
- Man
- Woman
- Non-binary
- Transgender
- Genderqueer
- Genderfluid
- Agender
- Two-Spirit
- Other (please specify)
- Prefer not to answer
- (3)
- What is your sexual orientation?
- Heterosexual
- Lesbian
- Gay
- Bisexual
- Queer
- Asexual
- Pansexual
- Demisexual
- Questioning
- Other (please specify)
- Prefer not to answer
- (4)
- What is your ethnicity?
- Caucasian/White
- First Nations (North American Indian)
- African American/Black
- South Asian/Chinese/Filipino
- Indian subcontinent
- Arab
- Other (please specify)
- (5)
- What is your citizenship?
- Canadian citizen or permanent resident
- Temporary resident in Canada
- (6)
- What is your first language?
- English
- Other (specify)
- (7)
- Where were you born?
- Canada
- United States
- Africa (please specify)
- Asia (please specify)
- Europe (please specify)
- Australia/New Zealand
- (8)
- What is your highest level of education?
- Elementary to high school
- Trade school
- Community College
- University (undergraduate)
- University (professional/postgraduate/doctoral)
- (9)
- What is your occupation?
- (10)
- What is your average annual income?
- <30,000
- 30,000–50,000
- 51,000–80,000
- 81,000–120,000
- >120,000
- (11)
- What is your main source of income?
- Employment/business/investment
- Pension/retirement
- Social assistance
- Family support (spouse, parents)
- Others (please specify)
- (12)
- What is your marital status?
- Single (never legally married)
- Married
- Common-law
- Divorced
- Separated
- Widowed
- (13)
- Which of the following best describes your living arrangements?
- Living with a partner (e.g., boy/girlfriend, spouse)
- Living with roommate(s)
- Living with family (e.g., sibling(s), parent(s))
- Living alone
- (14)
- What type of area do you live in?
- Metropolitan
- Regional/remote
- (15)
- Do you have private health insurance?
- Yes (employer-sponsored/self-sponsored)
- No
Appendix B
- Generally speaking how have your experiences in medical settings been?
- Do you feel your sexual or gender identity has influenced this? Why or why not?
- Please describe your experiences during the cancer treatment and recovery process?
- Do you feel your sexual or gender identity has influenced this? Why or why not? If why, how has it influenced the process?
- How has cancer and cancer treatment influenced your own identity or perceptions of your identity? If no influence, why not?
- How has cancer survivorship been part of your identity?
- How have you understood or conceptualized having these multiple identities?
- How would you define coping and resilience, particularly in a cancer context?
- How do you feel coping or resilience was part of your cancer journey?
- What coping mechanisms did you use in your cancer journey?
- How do you feel your sexual or gender identity influenced your coping process? If not, why not?
- What are supports for coping or resilience you would have liked to see during your cancer process?
- How do you feel your cancer experience could have been improved?
Appendix C
| SS Reflexivity Statement |
| Reflexivity statements serve as an opportunity for researchers to acknowledge the position they arrive to the research with. Our position in the world, through our identity or background, can influence how we act, think, and research. I come to this research project as an LGBTQ2S+-identifying person, recognizing my own personal connection to the community and my own background as an advocate for LGBTQ2S+ health. I do not, however, have any background as a cancer survivor and in particular have not previously been acquainted with the LGBTQ2S+ oncology community. In this way, I come to the research with some knowledge on the subject but a complete lack of knowledge in other aspects. My own personal education in public and population health, however, has primed me to recognize the social determinants of health and how socially relevant identities (such as LGBTQ2S+ status) influence health. My work has consistently been guided by principles of health equity and I bring that lens of social health and health equity into all my research work. This project is no exception. I recognize that, particularly in qualitative work, there is the opportunity for my own personal beliefs to spill into the work. By first recognizing my position, as is being done in this reflexivity statement, I can attempt to recognize these understandings and fully analyze the findings through the perspectives of the participants themselves. |
| AS Reflexivity Statement |
| Acknowledging one’s positionality is an essential practice in qualitative research and I recognize that the construction of the present study, my conceptualization of the data, and the act of writing and refining this manuscript is, in part, shaped by my lived experience and personal identities. As a white cisgender bisexual woman, I carry my lived experience navigating Canadian culture and my own internal insecurities, uncertainties, and pride surrounding my identity into the research we have produced; in many ways, my proximity to this research motivated me to engage with the data in a truly immersive way; however, it also may have impacted what concepts within the data stood out to me. Moreover, my education in health science often came through the lens of critical disability theory, and consequently, when considering health provision, I typically focus on structural barriers and consider the ways in which society shapes individual experience. I also recognize that the LGBTQ2S+ community is highly heterogeneous and the experiences of myself, as a bisexual woman, can be extremely different from other members of the community. Moreover, LGBTQ2S+ identities are often inextricably intersectional, and thus, the privileged position I hold as a white person who was born in an urban community to a wealthy family separates my experience from that of many other LGBTQ2S+ people in the present study and within the broader community. I also have never been diagnosed with cancer, and thus have not faced the physical or psychosocial challenges of cancer, treatment, survivorship, or grappled with the choice of self-disclosure in these settings. I am grateful to have worked alongside my co-authors on this study, and to have had the opportunity for the iterative and reflexive nature of this project to change my relationship with my own identities. |
References
- Stein, K.D.; Syrjala, K.L.; Andrykowski, M.A. Physical and psychological long-term and late effects of cancer. Cancer 2008, 112, 2577–2592. [Google Scholar] [CrossRef] [PubMed]
- Polsky, D.; Doshi, J.A.; Marcus, S.; Oslin, D.; Rothbard, A.; Thomas, N.; Thompson, C.L. Long-term risk for depressive symptoms after a medical diagnosis. Arch. Intern. Med. 2005, 165, 1260–1266. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Angen, M.; Cullum, J.; Goodey, E.; Koopmans, J.; Lamont, L.; MacRae, J.H.; Martin, M.; Pelletier, G.; Robinson, J.; et al. High levels of untreated distress and fatigue in cancer patients. Br. J. Cancer 2004, 90, 2297–2304. [Google Scholar] [CrossRef]
- Boehmer, U.; Miao, X.; Ozonoff, A. Cancer survivorship and sexual orientation. Cancer 2011, 117, 3796–3804. [Google Scholar] [CrossRef] [PubMed]
- Weyers, S.; Villeirs, G.; Vanherreweghe, E.; Verstraelen, H.; Monstrey, S.; Van den Broecke, R.; Gerris, J. Mammography and breast sonography in transsexual women. Eur. J. Radiol. 2010, 74, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Coulter, R.W.; Kenst, K.S.; Bowen, D.J. Research funded by the National Institutes of Health on the health of lesbian, gay, bisexual, and transgender populations. Am. J. Public Health 2014, 104, e105–e112. [Google Scholar] [CrossRef]
- Schefter, A.; Thomaier, L.; Jewett, P.; Brown, K.; Stenzel, A.E.; Blaes, A.; Teoh, D.; Vogel, R.I. Cross-sectional study of psychosocial well-being among lesbian, gay, bisexual, and heterosexual gynecologic cancer survivors. Cancer Rep. 2022, 5, e1461. [Google Scholar] [CrossRef]
- Boehmer, U.; Gereige, J.; Winter, M.; Ozonoff, A. Cancer survivors’ access to care and quality of life: Do sexual minorities fare worse than heterosexuals? Cancer 2019, 125, 3079–3085. [Google Scholar] [CrossRef]
- Carr, E. The personal experience of LGBT patients with cancer. Semin. Oncol. Nurs. 2018, 34, 72–79. [Google Scholar] [CrossRef]
- Brown, M.T.; McElroy, J.A. Unmet support needs of sexual and gender minority breast cancer survivors. Support. Care Cancer 2018, 26, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Colpitts, E.; Gahagan, J. The utility of resilience as a conceptual framework for understanding and measuring LGBTQ health. Int. J. Equity Health 2016, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, K.A.; Abreu, R.L.; Arora, S.; Lockett, G.M.; Sostre, J. “Previous resilience has taught me that I can survive anything:” LGBTQ resilience during the COVID-19 pandemic. Psychol. Sex. Orientat. Gend. Divers. 2021, 8, 133. [Google Scholar] [CrossRef]
- Harms, C.A.; Cohen, L.; Pooley, J.A.; Chambers, S.K.; Galvão, D.A.; Newton, R.U. Quality of life and psychological distress in cancer survivors: The role of psycho-social resources for resilience. Psycho-Oncology 2019, 28, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Kupst, M.J. Coping with pediatric cancer: Theoretical and research perspectives. In Pediatric Psychooncology: Psychological Perspectives on Children with Cancer; Oxford University Press: Oxford, UK, 1994; Volume 26, pp. 35–60. [Google Scholar]
- Russell, A.M.; Galvin, K.M.; Harper, M.M.; Clayman, M.L. A comparison of heterosexual and LGBTQ cancer survivors’ outlooks on relationships, family building, possible infertility, and patient-doctor fertility risk communication. J. Cancer Surviv. 2016, 10, 935–942. [Google Scholar] [CrossRef]
- Pooley, J.A.; Cohen, L. Resilience: A definition in context. Aust. Community Psychol. 2010, 22, 30–37. [Google Scholar]
- Woodgate, R.L. Conceptual understanding of resilience in the adolescent with cancer: Part I. J. Pediatr. Oncol. Nurs. 1999, 16, 35–43. [Google Scholar] [CrossRef]
- Deshields, T.L.; Heiland, M.F.; Kracen, A.C.; Dua, P. Resilience in adults with cancer: Development of a conceptual model. Psycho-Oncology 2016, 25, 11–18. [Google Scholar] [CrossRef]
- Canadian Institutes of Health Research. Strategy for Patient-Oriented Research. Available online: https://cihr-irsc.gc.ca/e/41204.html (accessed on 23 March 2023).
- Noon, E.J. Interpretive phenomenological analysis: An appropriate methodology for educational research. J. Perspect. Appl. Acad. Pract. 2018, 6, 75–83. [Google Scholar] [CrossRef]
- Snapp, S.D.; Watson, R.J.; Russell, S.T.; Diaz, R.M.; Ryan, C. Social support networks for LGBT young adults: Low cost strategies for positive adjustment. Fam. Relat. 2015, 64, 420–430. [Google Scholar] [CrossRef]
- Ybarra, M.L.; Mitchell, K.J.; Palmer, N.A.; Reisner, S.L. Online social support as a buffer against online and offline peer and sexual victimization among US LGBT and non-LGBT youth. Child Abus. Negl. 2015, 39, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Fong, A.J.; Scarapicchia, T.M.; McDonough, M.H.; Wrosch, C.; Sabiston, C.M. Changes in social support predict emotional well-being in breast cancer survivors. Psycho-Oncology 2017, 26, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, D. Cancer care disparities in the LGBT community. Curr. Opin. Support. Palliat. Care 2021, 15, 174–179. [Google Scholar] [CrossRef]
- Chopra, I.; Chopra, A. Follow-up care for breast cancer survivors: Improving patient outcomes. Patient Relat. Outcome Meas. 2014, 2014, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.; de Heer, H.D.; Bea, J.W. Initiating exercise interventions to promote wellness in cancer patients and survivors. Oncology 2017, 31, 711. [Google Scholar]
- McClain, Z.; Peebles, R. Body image and eating disorders among lesbian, gay, bisexual, and transgender youth. Pediatr. Clin. 2016, 63, 1079–1090. [Google Scholar] [CrossRef]
- Arch, J.J.; Mitchell, J.L. An Acceptance and Commitment Therapy (ACT) group intervention for cancer survivors experiencing anxiety at re-entry. Psycho-Oncology 2016, 25, 610–615. [Google Scholar] [CrossRef]
- McInroy, L.B.; Craig, S.L. Perspectives of LGBTQ emerging adults on the depiction and impact of LGBTQ media representation. J. Youth Stud. 2017, 20, 32–46. [Google Scholar] [CrossRef]
- Hagan, T.L.; Donovan, H.S. Ovarian cancer survivors’ experiences of self-advocacy: A focus group study. Oncol. Nurs. Forum 2013, 40, 140. [Google Scholar] [CrossRef]
- Schalk, S. Reevaluating the supercrip. J. Lit. Cult. Disabil. Stud. 2016, 10, 71–86. [Google Scholar] [CrossRef]
- Tamargo, C.L.; Quinn, G.P.; Sanchez, J.A.; Schabath, M.B. Cancer and the LGBTQ population: Quantitative and qualitative results from an oncology providers’ survey on knowledge, attitudes, and practice behaviors. J. Clin. Med. 2017, 6, 93. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.P.; Sanchez, J.A.; Sutton, S.K.; Vadaparampil, S.T.; Nguyen, G.T.; Green, B.L.; Kanetsky, P.A.; Schabath, M.B. Cancer and lesbian, gay, bisexual, transgender/transsexual, and queer/questioning (LGBTQ) populations. CA Cancer J. Clin. 2015, 65, 384–400. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, J.; Shaver, J.; Stephenson, R. Outness, stigma, and primary health care utilization among rural LGBT populations. PLoS ONE 2016, 11, e0146139. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Ethnicity * | ||
| White | 4 | 40 |
| First Nations | 1 | 10 |
| Black | 3 | 30 |
| South Asian | 1 | 10 |
| East Asian | 1 | 10 |
| South-East Asian | 1 | 10 |
| First language | ||
| English | 9 | 90 |
| Chinese | 1 | 10 |
| Place of birth | ||
| Canada | 8 | 80 |
| United States | 1 | 10 |
| Asia | 1 | 10 |
| Highest level of education | ||
| High school | 1 | 10 |
| College/trade school | 2 | 20 |
| University (undergraduate) | 5 | 50 |
| University (professional/postgraduate/doctoral) | 2 | 20 |
| Income | ||
| Less than $30,000 | 2 | 20 |
| $30,001–50,000 | 2 | 20 |
| $50,001–80,000 | 4 | 40 |
| $80,001–120,000 | 2 | 20 |
| Main source of income | ||
| Employment/business | 6 | 60 |
| Retirement/pension | 1 | 10 |
| Family support | 2 | 20 |
| Marital status | ||
| Single (never legally married) | 4 | 40 |
| Married | 4 | 40 |
| Common-law | 1 | 10 |
| Divorced | 1 | 10 |
| Living situation | ||
| Living with a partner | 6 | 60 |
| Living with family | 2 | 20 |
| Living alone | 2 | 20 |
| Community | ||
| Urban | 8 | 80 |
| Rural | 2 | 20 |
| Province of residence | ||
| Alberta | 2 | 20 |
| New Brunswick | 1 | 10 |
| Ontario | 7 | 70 |
| Private health insurance | ||
| Yes | 7 | 70 |
| No | 3 | 30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, S.; Spiropoulos, A.; Deleemans, J.; Carlson, L.E. Assessing the Conceptualizations of Coping and Resilience in LGBTQ2S+ People with Cancer: Working towards Greater Awareness in Cancer Care. Cancers 2024, 16, 2996. https://doi.org/10.3390/cancers16172996
Singh S, Spiropoulos A, Deleemans J, Carlson LE. Assessing the Conceptualizations of Coping and Resilience in LGBTQ2S+ People with Cancer: Working towards Greater Awareness in Cancer Care. Cancers. 2024; 16(17):2996. https://doi.org/10.3390/cancers16172996
Chicago/Turabian StyleSingh, Sarthak, Athina Spiropoulos, Julie Deleemans, and Linda E. Carlson. 2024. "Assessing the Conceptualizations of Coping and Resilience in LGBTQ2S+ People with Cancer: Working towards Greater Awareness in Cancer Care" Cancers 16, no. 17: 2996. https://doi.org/10.3390/cancers16172996