
The Impact of Adjunct Medical Therapy on Survival after Spine Metastasis: A Systematic Review and Pooled Data Analysis
 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Electronic Database Search Strategy
2.2. Exclusion and Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Methods
3. Results
3.1. Study Selection
3.2. Study Demographics
3.3. Patient Demographics
3.4. Median Overall Survival (mOS)
3.5. Impact of Medical Therapy on mOS
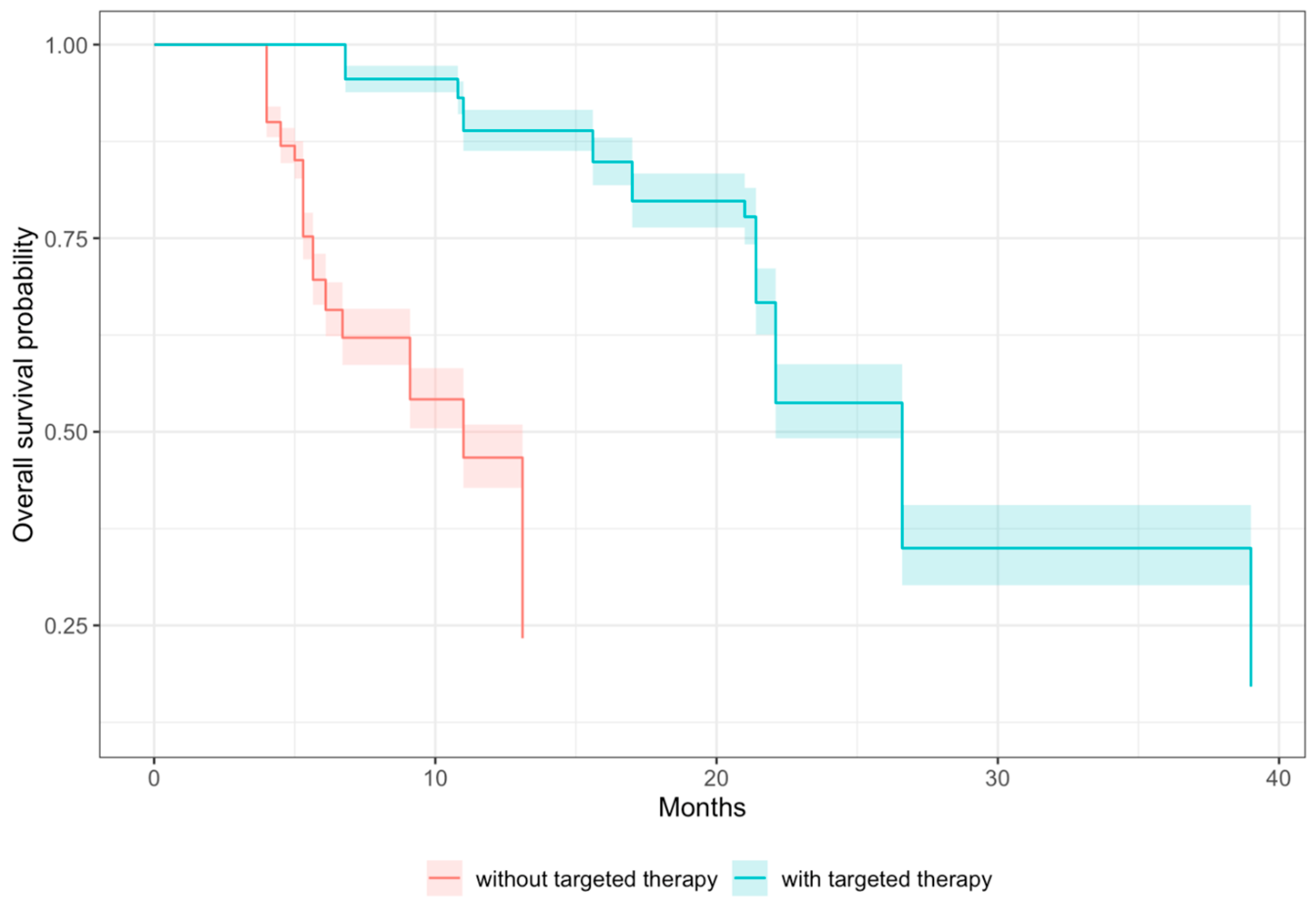
3.5.1. Targeted Therapy (TT)
3.5.2. Chemotherapy
3.5.3. Radiation Therapy (RT)
3.5.4. Immunotherapy
3.5.5. Bisphosphonate Therapy
3.6. Impact of Receptor Status on mOS
3.7. Impact of Histology on mOS
3.8. Impact of Spine Surgery on mOS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
- (“melanoma”[MeSH Terms] OR “melanoma”[Text Word] OR “skin cancer”[Text Word] OR “skin tumor*”[Text Word] OR “skin tumour*”[Text Word]) AND (“molecular targeted therapy”[MeSH Terms] OR “targeted therap*”[Text Word] OR “CTLA 4”[Text Word] OR “anti-PD-1”[Text Word] OR BRAF[Text Word] OR E3[Text Word] OR MEK[Text Word]) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word])
- (“prostatic neoplasms”[MeSH Terms] OR “prostat* cancer”[TW] OR (prostate AND (tumor OR tumour OR cancer OR carcinoma OR “squamous cell carcinoma” OR scc OR “transitional cell carcinoma” OR tcc OR “small cell”))) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word]) AND (“molecular targeted therapy”[MeSH Terms] OR ”androgen receptor antagonist” OR MET OR VEGFR2 OR EGFR OR “anti-CTLA4” OR “targeted therap*” OR PARP OR BRCA)
- (“osteosarcoma” [MeSH Terms] OR (bone AND (tumor OR tumour OR cancer OR sarcoma OR osteosarcoma))) AND (“molecular targeted therapy”[MeSH Terms] OR (“targeted therap*” OR “kinase inhibitor” OR RANKL OR NTRK OR “neurotrophic receptor tyrosine kinase” OR “immune checkpoint inhibitors” OR “PD-1” OR “interferon-alpha” OR “IFN-α” OR “interferon-alpha-2b” OR “IFN-α2b”)) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word])
- (“Stomach neoplasms” [MeSH Terms] OR((gastric OR stomach) AND (tumor OR tumour OR cancer OR adenocarcinoma OR “gastrointestinal stromal tumor” OR GIST OR “neuroendocrine tumor” OR carcinoid OR lymphoma))) AND (“molecular targeted therapy”[MeSH Terms] OR (“targeted therap*” OR VEGF* OR HER2* OR “ER+” OR “MSI-H“ OR dMMR OR “anti-CLDN18.2” OR “endothelial growth factor receptor” OR EGFR OR “tyrosine receptor kinase” OR TRK OR TRKI OR “TRK inhibitor” OR NTRK)) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word])
- (“thyroid neoplasms” [MeSH Terms] OR (Thyroid AND (tumor OR tumour OR cancer OR carcinoma OR papillary OR follicular OR medullary OR anaplastic))) AND (“molecular targeted therapy”[MeSH Terms] OR (“targeted therap*” OR RET OR “kinase inhibitor” OR “protein kinase” OR RET OR NTRK OR BRAF OR MEK OR “multikinase inhibitor”)) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word])
- (“Breast neoplasms” [MeSH Terms] OR (breast AND (tumor OR tumour OR cancer OR carcinoma OR adenocarcinoma OR “squamous cell carcinoma” OR scc OR “large cell carcinoma” OR “small cell”))) AND (“molecular targeted therapy”[MeSH Terms] OR “ER+” OR HER2 OR “anti-VEGF” OR mTOR OR “cyclin-dependent kinase 4/6” OR “CDK4/6” OR CDK4 OR CDK6 OR TP53 OR “tumor protein 53” OR “tumour protein 53” OR “phosphatidylinositol-4,5-bisphosphate 3-kinase” OR PIK3CA OR “fibroblast growth factor receptor” OR FGFR OR “cyclin D1 gene” OR CCND1 OR AKT1 OR Src OR “phosphatase and tension homolog” OR PTEN OR KRAS OR “anaphase promoting complex” OR “APC” or “NF1” OR “neurofibromatosis 1” OR MAP2K4 OR MAP3K1 OR AKT2 OR uPA OR “PAI-1” OR “targeted therap*” OR “PR+” or “PR positive”) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word])
- (“Lung neoplasms” [MeSH Terms] OR (lung AND (tumor OR tumour OR cancer OR carcinoma OR adenocarcinoma OR “squamous cell” OR SCC OR “large cell” OR “small cell” OR “small-cell” OR “large-cell” OR “nonsquamous cell” OR NSCLC tumor OR tumour))) AND (“molecular targeted therapy”[MeSH Terms] OR (“endothelial growth factor receptor” OR EGFR OR “tyrosine kinase inhibitors” OR TKI OR “TK inhibitors” OR RTK OR “c-Met” OR ErbB OR HER2 Or HER4 OR “human epidermal growth factor receptor 2” OR VEGF OR “vascular endothelial growth factor” OR “targeted therap*” OR “immune checkpoint inhibitors” OR CTLA4 OR “cytotoxic T-lymphocyte associated protein 4” OR “Anti-programmed death 1” OR “anti-PD1” OR “anti-programmed death ligand 1” OR “anti-PD-L1” OR “echinoderm microtubule-associated protein-like 4-anaplastic lymphoma kinase” OR “EML4-ALK” OR ALK OR BRAF OR MAP2K OR “mitogen-activated protein kinase 2”)) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word] OR “sacrum*”[Text Word])
- (“Kidney neoplasms” [MeSH Terms] OR ((renal OR kidney) AND (tumor OR tumour OR cancer OR cell OR sarcoma OR carcinoma OR RCC OR Wilm*))) AND (“molecular targeted therapy”[MeSH Terms] OR cytokines OR mTOR OR IL-2 OR RTK OR TKI OR mTOR OR VEGF or “interferon-alpha” OR “IFN-α” OR “anti-PD1” OR “anti-CTLA4” OR “targeted therap*”) AND (“spine”[MeSH Terms] OR “spine*”[Text Word] OR “spinal”[Text Word] OR “vertebra*”[Text Word] OR “column*”[Text Word] OR “coccyx”[Text Word])
References
- Fomchenko, E.I.; Bayley, J.C.; Alvarez-Breckenridge, C.; Rhines, L.D.; Tatsui, C.E. Spinal Metastases and the Evolving Role of Molecular Targeted Therapy, Chemotherapy, and Immunotherapy. Neurospine 2022, 19, 978–993. [Google Scholar] [CrossRef] [PubMed]
- Tokuhashi, Y.; Ajiro, Y.; Oshima, M. Algorithms and planning in metastatic spine tumors. Orthop. Clin. N. Am. 2009, 40, 37–46, v–vi. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; Ferrone, M.L.; Blucher, J.A.; Agaronnik, N.; Nguyen, L.; Tobert, D.G.; Balboni, T.A.; Schwab, J.H.; Shin, J.H.; Sciubba, D.M.; et al. Prospective comparison of the accuracy of the New England Spinal Metastasis Score (NESMS) to legacy scoring systems in prognosticating outcomes following treatment of spinal metastases. Spine J. 2022, 22, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Batista, N.; Tee, J.; Sciubba, D.; Sahgal, A.; Laufer, I.; Weber, M.; Gokaslan, Z.; Rhines, L.; Fehlings, M.; Patel, S.; et al. Emerging and established clinical, histopathological and molecular parametric prognostic factors for metastatic spine disease secondary to lung cancer: Helping surgeons make decisions. J. Clin. Neurosci. 2016, 34, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Aoude, A.; Amiot, L.P. A comparison of the modified Tokuhashi and Tomita scores in determining prognosis for patients afflicted with spinal metastasis. Can. J. Surg. 2014, 57, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Aoude, A.; Fortin, M.; Aldebeyan, S.; Ouellet, J.; Amiot, L.P.; Weber, M.H.; Jarzem, P. The revised Tokuhashi score; analysis of parameters and assessment of its accuracy in determining survival in patients afflicted with spinal metastasis. Eur. Spine J. 2018, 27, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Pennington, Z.; Ehresman, J.; Cottrill, E.; Lubelski, D.; Lehner, K.; Feghali, J.; Ahmed, A.K.; Schilling, A.; Sciubba, D.M. To operate, or not to operate? Narrative review of the role of survival predictors in patient selection for operative management of patients with metastatic spine disease. J. Neurosurg. Spine 2020, 34, 135–149. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Guo, L.; Guo, B.; Zhang, P.; Wang, J.; Wang, X.; Yao, W. Evaluation of different scoring systems for spinal metastases based on a Chinese cohort. Cancer Med. 2023, 12, 4125–4136. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xiao, J.; Yang, X.; Zhang, F.; Yuan, W. Preoperative scoring systems and prognostic factors for patients with spinal metastases from hepatocellular carcinoma. Spine 2010, 35, E1339–E1346. [Google Scholar] [CrossRef]
- Morgen, S.S.; Lund-Andersen, C.; Larsen, C.F.; Engelholm, S.A.; Dahl, B. Prognosis in patients with symptomatic metastatic spinal cord compression: Survival in different cancer diagnosis in a cohort of 2321 patients. Spine 2013, 38, 1362–1367. [Google Scholar] [CrossRef]
- Tokuhashi, Y.; Uei, H.; Oshima, M.; Ajiro, Y. Scoring system for prediction of metastatic spine tumor prognosis. World J. Orthop. 2014, 5, 262–271. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Amelot, A.; Terrier, L.M.; Cristini, J.; Buffenoir, K.; Pascal-Moussellard, H.; Carpentier, A.; Bonaccorsi, R.; Le Nail, L.R.; Mathon, B. Survival in breast cancer patients with spine metastases: Prognostic assessment involving molecular markers. Eur. J. Surg. Oncol. 2020, 46, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Amelot, A.; Terrier, L.M.; Cristini, J.; Buffenoir, K.; Pascal-Moussellard, H.; Carpentier, A.; Bonaccorsi, R.; Le Nail, L.R.; Mathon, B. Spinal metastases from lung cancer: Survival depends only on genotype, neurological and personal status, scarcely of surgical resection. Surg. Oncol. 2020, 34, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Bollen, L.; Wibmer, C.; Wang, M.; van der Linden, Y.M.; Leithner, A.; Bünger, C.E.; Jensen, A.B.; Fiocco, M.; Bratschitsch, G.; Pondaag, W.; et al. Molecular phenotype is associated with survival in breast cancer patients with spinal bone metastases. Clin. Exp. Metastasis 2015, 32, 1–5. [Google Scholar] [CrossRef]
- Dohzono, S.; Sasaoka, R.; Takamatsu, K.; Nakamura, H. Overall survival and prognostic factors in patients with spinal metastases from lung cancer treated with and without epidermal growth factor receptor tyrosine kinase inhibitors. Int. J. Clin. Oncol. 2017, 22, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Lei, M.; Liu, Y.; Liu, S.; Wang, L.; Zhou, S.; Zhou, J. Individual strategy for lung cancer patients with metastatic spinal cord compression. Eur. J. Surg. Oncol. 2016, 42, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Tang, X.; Yang, R.; Yan, T.; Guo, W. Modified score based on revised Tokuhashi score is needed for the determination of surgical intervention in patients with lung cancer metastases to the spine. World J. Surg. Oncol. 2019, 17, 194. [Google Scholar] [CrossRef]
- Kumar, N.; Tan, K.A.; Tan, J.H.; Zaw, A.S.; Hey, H.W.D.; Ruiz, J.; Stone, E. The Influence of Histologic Subtype in Predicting Survival of Lung Cancer Patients with Spinal Metastases. Clin. Spine Surg. 2018, 31, E1–E7. [Google Scholar] [CrossRef]
- Kato, S.; Demura, S.; Murakami, H.; Yoshioka, K.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Kawahara, N.; Tsuchiya, H. Clinical outcomes and prognostic factors following the surgical resection of renal cell carcinoma spinal metastases. Cancer Sci. 2021, 112, 2416–2425. [Google Scholar] [CrossRef] [PubMed]
- Dohzono, S.; Sasaoka, R.; Takamatsu, K.; Hoshino, M.; Nakamura, H. Low paravertebral muscle mass in patients with bone metastases from lung cancer is associated with poor prognosis. Support. Care Cancer 2020, 28, 389–394. [Google Scholar] [CrossRef]
- Komatsu, T.; Kunieda, E.; Oizumi, Y.; Tamai, Y.; Akiba, T. An analysis of the survival rate after radiotherapy in lung cancer patients with bone metastasis: Is there an optimal subgroup to be treated with high-dose radiation therapy? Neoplasma 2012, 59, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.H.; Chiu, C.H.; Chou, P.H.; Ma, H.L.; Wang, J.P.; Wang, S.T.; Liu, C.L.; Chang, M.C. Functional outcomes and survival after surgical stabilization for inoperable non-small-cell lung cancer with spinal metastasis of the thoracic and lumbar spines: A retrospective comparison between epidermal growth factor receptor-tyrosine kinase inhibitor and platinum-based chemotherapy groups. Spinal Cord. 2020, 58, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Nagata, M.; Kudoh, S.; Mitsuoka, S.; Suzumura, T.; Umekawa, K.; Tanaka, H.; Matsuura, K.; Kimura, T.; Yoshimura, N.; Hirata, K. Skeletal-related events in advanced lung adenocarcinoma patients evaluated EGFR mutations. Osaka City Med. J. 2013, 59, 45–52. [Google Scholar] [PubMed]
- Tang, Y.; Qu, J.; Wu, J.; Li, S.; Zhou, Y.; Xiao, J. Metastatic Spinal Cord Compression from Non-Small-Cell Lung Cancer Treated with Surgery and Adjuvant Therapies: A Retrospective Analysis of Outcomes and Prognostic Factors in 116 Patients. J. Bone Jt. Surg. Am. 2015, 97, 1418–1425. [Google Scholar] [CrossRef] [PubMed]
- Mannavola, F.; Mandala, M.; Todisco, A.; Sileni, V.C.; Palla, M.; Minisini, A.M.; Pala, L.; Morgese, F.; Di Guardo, L.; Stucci, L.S.; et al. An Italian Retrospective Survey on Bone Metastasis in Melanoma: Impact of Immunotherapy and Radiotherapy on Survival. Front. Oncol. 2020, 10, 1652. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Zhang, Z.; Zhong, N.; Fan, T.; Gao, X.; Wu, Z.; Li, Z.; Liu, T.; Xiao, J. Outcomes and prognostic factors for surgically treated patients with breast cancer spine metastases. J. Bone Oncol. 2018, 12, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Ha, K.Y.; Kim, S.I.; Kim, Y.S.; Joh, Y.; Kim, Y.H. When Should Spinal Surgery Be Considered for Spinal Metastasis from Non-Small Cell Lung Cancer?—Propensity Score Matched Study between Surgery with Radiotherapy and Radiotherapy Alone. J. Clin. Med. 2023, 12, 4683. [Google Scholar] [CrossRef]
- Shankar, G.M.; Choi, B.D.; Grannan, B.L.; Oh, K.; Shin, J.H. Effect of Immunotherapy Status on Outcomes in Patients with Metastatic Melanoma to the Spine. Spine 2017, 42, E721–E725. [Google Scholar] [CrossRef]
- Zang, S.; He, Q.; Bao, Q.; Shen, Y.; Zhang, W. Establishment and validation of a novel survival prediction scoring algorithm for patients with non-small-cell lung cancer spinal metastasis. Int. J. Clin. Oncol. 2019, 24, 1049–1060. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.H.; Tan, K.A.; Zaw, A.S.; Thomas, A.C.; Hey, H.W.; Soo, R.A.; Kumar, N. Evaluation of Scoring Systems and Prognostic Factors in Patients with Spinal Metastases from Lung Cancer. Spine 2016, 41, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Rabah, N.M.; Jarmula, J.; Hamza, O.; Khan, H.A.; Chakravarthy, V.; Habboub, G.; Wright, J.M.; Steinmetz, M.P.; Wright, C.H.; Krishnaney, A.A. Metastatic Breast Cancer to the Spine: Incidence of Somatic Gene Alterations and Association of Targeted Therapies with Overall Survival. Neurosurgery 2023, 92, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Xu, W.; Liu, T.; Yang, X.; Wang, P.; Wu, S.; Wei, H.; Zhao, J.; Yang, C.; Xiao, J. Development and Validation of a Novel Survival Prediction Model in Patients with Spinal Metastasis from Non-small Cell Lung Cancer. Spine 2019, 44, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Gómez-León, N.; Pacheco-Barcia, V.; Ballesteros, A.I.; Fraga, J.; Colomer, R.; Friera, A. Skeletal muscle and solitary bone metastases from malignant melanoma: Multimodality imaging and oncological outcome. Melanoma Res. 2018, 28, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Zhai, S.; Hu, P.; Liu, X.; Li, Z.; Wang, B.; Zhou, H.; Liu, Z.; Liu, X.; Li, Y.; Wei, F. Prognostic Analysis of Spinal Metastasis Secondary to Lung Cancer after Surgeries: A Unicentric, Large-Cohort, Retrospective Study. Orthop. Surg. 2023, 15, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.A.; Tan, J.H.; Zaw, A.S.; Tan, J.Y.H.; Hey, H.W.D.; Kumar, N. Evaluation of Prognostic Factors and Proposed Changes to the Modified Tokuhashi Score in Patients with Spinal Metastases from Breast Cancer. Spine 2018, 43, 512–519. [Google Scholar] [CrossRef]
- Shankar, G.M.; Van Beaver, L.A.; Choi, B.D.; Hadzipasic, M.; Sivaganesan, A.; Karhade, A.V.; Ferrone, M.L.; Harris, M.B.; Schoenfeld, A.J.; Sadow, P.M.; et al. Survival after Surgery for Renal Cell Carcinoma Metastatic to the Spine: Impact of Modern Systemic Therapies on Outcomes. Neurosurgery 2020, 87, 1174–1180. [Google Scholar] [CrossRef]
- Park, S.; Kim, K.H.; Rhee, W.J.; Lee, J.; Cho, Y.; Koom, W.S. Treatment outcome of radiation therapy and concurrent targeted molecular therapy in spinal metastasis from renal cell carcinoma. Radiat. Oncol. J. 2016, 34, 128–134. [Google Scholar] [CrossRef]
- Chen, Q.; Chen, X.; Zhou, L.; Chen, F.; Hu, A.; Wang, K.; Liang, H.; Jiang, L.; Li, X.; Dong, J. The emergence of new prognostic scores in lung cancer patients with spinal metastasis: A 12-year single-center retrospective study. J. Cancer 2021, 12, 5644–5653. [Google Scholar] [CrossRef]
- Kato, S.; Demura, S.; Yokogawa, N.; Shimizu, T.; Kobayashi, M.; Yamada, Y.; Murakami, H.; Tsuchiya, H. Metastasectomy of spinal lesions from thyroid carcinomas. Bone Jt. J. 2023, 105, 575–582. [Google Scholar] [CrossRef] [PubMed]
- McGrath, S.; Zhao, X.; Qin, Z.Z.; Steele, R.; Benedetti, A. One-sample aggregate data meta-analysis of medians. Stat. Med. 2019, 38, 969–984. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. Ser. B 1972, 34, 187–202. [Google Scholar] [CrossRef]
- Cochrane. Random Effects (DerSimonian and Laird Method for Meta-Analysis); Cochrane: Singapore, 2011. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Ben-Aharon, O.; Magnezi, R.; Leshno, M.; Goldstein, D.A. Median Survival or Mean Survival: Which Measure Is the Most Appropriate for Patients, Physicians, and Policymakers? Oncologist 2019, 24, 1469–1478. [Google Scholar] [CrossRef]
- Burki, T.K. Late detection of lung cancer. Lancet Oncol. 2014, 15, e590. [Google Scholar] [CrossRef]
- Aebi, M. Spinal metastasis in the elderly. Eur. Spine J. 2003, 12 (Suppl. S2), S202–S213. [Google Scholar] [CrossRef]
- Hirota, R.; Teramoto, A.; Iesato, N.; Chiba, M.; Yamashita, T. Ten-year trends in the treatment and intervention timing for patients with metastatic spinal tumors: A retrospective observational study. J. Orthop. Surg. Res. 2023, 18, 26. [Google Scholar] [CrossRef]
- Ziu, E.; Viswanathan, V.K.; Mesfin, F.B. Spinal Metastasis. In StatPearls; StatPearls Publishing Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Rief, H.; Bischof, M.; Bruckner, T.; Welzel, T.; Askoxylakis, V.; Rieken, S.; Lindel, K.; Combs, S.; Debus, J. The stability of osseous metastases of the spine in lung cancer—A retrospective analysis of 338 cases. Radiat. Oncol. 2013, 8, 200. [Google Scholar] [CrossRef]
- Hong, S.; Youk, T.; Lee, S.J.; Kim, K.M.; Vajdic, C.M. Bone metastasis and skeletal-related events in patients with solid cancer: A Korean nationwide health insurance database study. PLoS ONE 2020, 15, e0234927. [Google Scholar] [CrossRef]
- Goodwin, C.R.; Khattab, M.H.; Sankey, E.W.; Elder, B.D.; Kosztowski, T.A.; Sarabia-Estrada, R.; Bydon, A.; Witham, T.F.; Wolinsky, J.P.; Gokaslan, Z.L.; et al. Factors Associated with Life Expectancy in Patients with Metastatic Spine Disease from Adenocarcinoma of the Lung. Glob. Spine J. 2015, 5, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Uei, H.; Tokuhashi, Y.; Maseda, M. Treatment Outcome of Metastatic Spine Tumor in Lung Cancer Patients: Did the Treatments Improve Their Outcomes? Spine 2017, 42, E1446–E1451. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rudin, C.M.; Brambilla, E.; Faivre-Finn, C.; Sage, J. Small-cell lung cancer. Nat. Rev. Dis. Primers 2021, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Sellin, J.N.; Gressot, L.V.; Suki, D.; St Clair, E.G.; Chern, J.; Rhines, L.D.; McCutcheon, I.E.; Rao, G.; Tatsui, C.E. Prognostic Factors Influencing the Outcome of 64 Consecutive Patients Undergoing Surgery for Metastatic Melanoma of the Spine. Neurosurgery 2015, 77, 386–393, discussion 393. [Google Scholar] [CrossRef] [PubMed]
- Gokaslan, Z.L.; Aladag, M.A.; Ellerhorst, J.A. Melanoma metastatic to the spine: A review of 133 cases. Melanoma Res. 2000, 10, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Bozzo, A.; Deng, J.; Abbas, U.; Bhasin, R.; Deodat, M.; Wariach, S.; Sanger, S.; Axelrod, D.; Masrouha, K.; Turcotte, R.; et al. Which Bone-Modifying Agent is Associated with Better Outcomes in Patients with Skeletal Metastases from Lung Cancer? A Systematic Review and Network Meta-analysis. Clin. Orthop. Relat. Res. 2021, 479, 2047–2057. [Google Scholar] [CrossRef] [PubMed]
- Sugita, S.; Ogiso, S.; Fujiwara, M.; Morita, E.; Koyama, T.; Hozumi, T. The Outcome of Molecularly Targeted Therapy after Surgical Treatment of Spinal Metastasis. J. Clin. Med. 2023, 12, 3920. [Google Scholar] [CrossRef]
- The National Institute for Health and Care Excellence. Metastatic Spinal Cord Compression in Adults. Quality Standard [QS56]. Available online: https://www.nice.org.uk/guidance/qs56 (accessed on 6 January 2024).
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS framework: Approach to the treatment of spinal metastatic tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Grover, P.; Karivedu, V.; Zhu, Z.; Jandarov, R.; Wise-Draper, T.M. Bone metastases treated with immune checkpoint inhibitors: A single center experience. J. Clin. Oncol. 2019, 37, e14105. [Google Scholar] [CrossRef]
- Eckstein, J.; Gogineni, E.; Sidiqi, B.; Lisser, N.; Parashar, B. Effect of Immunotherapy and Stereotactic Body Radiation Therapy Sequencing on Local Control and Survival in Patients with Spine Metastases. Adv. Radiat. Oncol. 2023, 8, 101179. [Google Scholar] [CrossRef]
- Bayat Mokhtari, R.; Homayouni, T.S.; Baluch, N.; Morgatskaya, E.; Kumar, S.; Das, B.; Yeger, H. Combination therapy in combating cancer. Oncotarget 2017, 8, 38022–38043. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Component | Inclusion | Exclusion |
|---|---|---|
| Participants | A pathology of spinal cord metastases secondary to lung cancer, breast cancer, bone cancer, GI cancer, prostate cancer, thyroid cancer, melanoma, or kidney cancer | A pathology of inflammation, infection, or trauma |
| Interventions and comparators | Patients undergoing surgery, radiation therapy, targeted therapy, chemotherapy treatment, bisphosphonate therapy, immunotherapy, or no treatment for their spinal cord metastases | |
| Outcomes | Life expectancy based on survivorship and prognostic factors specific to patients with spinal cord metastases | Does not include the outcome of interest |
| Study designs | Present an original article reporting a case series greater than 5 patients: RCTs, clinical case series | Case reports, reviews |
| Publication | English studies published in a peer-reviewed, PubMed-indexed journal after 2005 | Abstracts, editorials, letters, and duplicate studies or repeat publications of the same patient group; non-English papers; and papers published before 2005 |
| No. | Reference | Year of Publication | Study Period | Design | Multicenter | Primary Cancer | LoE |
|---|---|---|---|---|---|---|---|
| 1 | Amelot et al. [14] | 2019 | 2014–2017 | Prospective | Yes | Breast | IV |
| 2 | Amelot et al. [15] | 2020 | 2014–2017 | Prospective | Yes | Lung | IV |
| 3 | Bollen et al. [16] | 2014 | 2005–2012 | Retrospective | Yes | Breast | IV |
| 4 | Dohzono et al. [17] | 2017 | 2009–2016 | Retrospective | No | Lung | IV |
| 5 | Lei et al. [18] | 2016 | 2005–2015 | Retrospective | No | Lung | IV |
| 6 | Cai et al. [19] | 2019 | 2010–2018 | Retrospective | No | Lung | IV |
| 7 | Kumar et al. [20] | 2018 | 2001–2012 | Retrospective | No | Lung | IV |
| 8 | Kato et al. [21] | 2021 | 1995–2017 | Retrospective | No | Renal | IV |
| 9 | Dohzono et al. [22] | 2020 | 2009–2017 | Retrospective | Yes | Lung | IV |
| 10 | Komatsu et al. [23] | 2012 | 2004–2009 | Retrospective | No | Lung | IV |
| 11 | Lin et al. [24] | 2020 | 2001–2011 | Retrospective | No | Lung | IV |
| 12 | Nagata et al. [25] | 2013 | 2007–2009 | Retrospective | No | Lung | IV |
| 13 | Tang et al. [26] | 2015 | 2002–2013 | Retrospective | No | Lung | IV |
| 14 | Mannavola et al. [27] | 2020 | 1984–2019 | Retrospective | Yes | Melanoma | IV |
| 15 | Zhao et al. [28] | 2018 | 2005–2015 | Retrospective | No | Breast | IV |
| 16 | Park et al. [29] | 2023 | 2011–2017 | Retrospective | No | Lung | IV |
| 17 | Shankar et al. [30] | 2017 | 2012–2015 | Retrospective | No | Melanoma | IV |
| 18 | Zang et al. [31] | 2019 | 2006–2017 | Retrospective | No | Lung | IV |
| 19 | Tan et al. [32] | 2016 | 2001–2012 | Retrospective | No | Lung | III |
| 20 | Rabah et al. [33] | 2022 | 2010–2020 | Retrospective | Yes | Breast | IV |
| 21 | Yang et al. [34] | 2018 | 2010–2016 | Retrospective | No | Lung | IV |
| 22 | Gómez-León et al. [35] | 2018 | 2006–2016 | Retrospective | No | Melanoma | IV |
| 23 | Zhai et al. [36] | 2022 | 2009–2020 | Retrospective | No | Lung | IV |
| 24 | Tan et al. [37] | 2018 | 2001–2012 | Retrospective | No | Breast | III |
| 25 | Shankar et al. [38] | 2020 | 2010–2017 | Retrospective | No | Renal | IV |
| 26 | Park et al. [39] | 2016 | 2009–2015 | Retrospective | No | Renal | IV |
| 27 | Chen et al. [40] | 2021 | 2009–2021 | Retrospective | No | Renal | IV |
| 28 | Kato et al. [41] | 2023 | 1992–2017 | Retrospective | No | Thyroid | IV |
| Primary Cancer Location | ||||||||
|---|---|---|---|---|---|---|---|---|
| Lung, n = 16 | Breast, n = 5 | Renal, n = 3 | Melanoma, n = 3 | Thyroid, n = 1 | ||||
| Treatment type | ||||||||
| Bisphosphonate therapy [n] | 2 | 1 | 0 | 1 | 1 | |||
| Isolated use [n] | 2 | 1 | 0 | 1 | 1 | |||
| Participant number reported for both groups [n] | 2 | 1 | 0 | 1 | 1 | |||
| Median OS or OS rate reported for both groups [n] | 2 | 1 | 0 | 1 | 1 | |||
| Univariable Cox regression hazard ratio reported [n] | 1 | 0 | 0 | 0 | 0 | |||
| Multivariable Cox regression hazard ratio reported [n] | 2 | 0 | 0 | 1 | 0 | |||
| Chemotherapy [n] | 11 | 2 | 0 | 2 | 0 | |||
| Isolated use [n] | 11 | 2 | 0 | 2 | 0 | |||
| Participant number reported for both groups [n] | 9 | 2 | 0 | 2 | 0 | |||
| Median OS or OS rate reported for both groups [n] | 5 | 1 | 0 | 1 | 0 | |||
| Univariable Cox regression hazard ratio reported [n] | 2 | 0 | 0 | 0 | 0 | |||
| Multivariable Cox regression hazard ratio reported [n] | 3 | 1 | 0 | 0 | 0 | |||
| Immunotherapy [n] | 1 | 1 | 2 | 2 | 0 | |||
| Isolated use [n] | 1 | 1 | 2 | 2 | 0 | |||
| Participant number reported for both groups [n] | 1 | 1 | 1 | 2 | 0 | |||
| Median OS or OS rate reported for both groups [n] | 0 | 0 | 0 | 1 | 0 | |||
| Univariable Cox regression hazard ratio reported [n] | 1 | 0 | 0 | 1 | 0 | |||
| Multivariable Cox regression hazard ratio reported [n] | 0 | 0 | 0 | 0 | 0 | |||
| Radiation therapy [n] | 11 | 5 | 1 | 1 | 1 | |||
| Isolated use [n] | 11 | 5 | 1 | 1 | 1 | |||
| Participant number reported for both groups [n] | 9 | 4 | 1 | 1 | 1 | |||
| Median OS or OS rate reported for both groups [n] | 3 | 2 | 0 | 1 | 1 | |||
| Univariable Cox regression hazard ratio reported [n] | 2 | 1 | 0 | 0 | 0 | |||
| Multivariable Cox regression hazard ratio reported [n] | 1 | 0 | 0 | 1 | 0 | |||
| Targeted therapy [n] | 15 | 3 | 3 | 3 | 1 | |||
| Isolated use [n] | 15 | 3 | 2 | 3 | 1 | |||
| Participant number reported for both groups [n] | 15 | 3 | 1 | 3 | 1 | |||
| Median OS or OS rate reported for both groups [n] | 11 | 2 | 0 | 1 | 0 | |||
| Univariable Cox regression hazard ratio reported [n] | 6 | 1 | 0 | 2 | 0 | |||
| Multivariable Cox regression hazard ratio reported [n] | 10 | 1 | 0 | 1 | 0 | |||
| Cohort median overall survival reported [n] | 12 | 4 | 2 | 3 | 1 | |||
| Lung | Breast | Renal | Melanoma | Thyroid | |
|---|---|---|---|---|---|
| n | 2137 | 591 | 167 | 321 | 22 |
| Weighted mean age [years] | 58.3 | 58.3 | 61.9 | 56.3 | 58.1 |
| Histology [n] | NSCLC: 2020 SCLC: 104 Others: 13 | Nodular: 98 SSM: 90 Acral: 10 Other or NR: 123 | Follicular: 16 Papillary: 6 | ||
| Male sex, n (%) | 1299 (60.8) | 3 (0.5) | 124 (74.2) | 3 (13.6) | |
| Pooled mOS (95% CI) [months] | 6.7 (4.8–11.6) | 28.3 (18.0–159.8) | 58.3 (23.6–100.0) | 10.6 (3.9–18.0) | 123.0 (NR) |
| Primary Cancer Location | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lung | Breast | Renal | Melanoma | Thyroid | ||||||
| Patients [n] | Pooled Median OS (95% CI) [Months] | Pooled HR (95% CI), p-Value | Patients [n] | Pooled Median OS (95% CI) [Months] | Patients [n] | Patients [n] | Patients [n] | |||
| Treatment Type | ||||||||||
| Bisphosphonate therapy | ||||||||||
| Yes | 105 | 0.933 (0.579–1.503), 0.776 | 59 | 0 | 119 | 13 | ||||
| No | 131 | – | 25 | 0 | 173 | 9 | ||||
| Chemotherapy | ||||||||||
| Yes | 598 | 14.2 (5.5–19.9) | 0.604 (0.248–1.467), 0.265 | 205 | 0 | 24 | 0 | |||
| No | 721 | 8.5 (4.6–11.0) | – | 64 | 0 | 280 | 0 | |||
| Immunotherapy | ||||||||||
| Yes | 23 | 14 | 23 | 122 | 0 | |||||
| No | 187 | 171 | 42 | 187 | 0 | |||||
| Radiation therapy | ||||||||||
| Yes | 740 | 13.5 (5.1–22.9) | 254 | 45.8 (45.7–46.0) | 2 | 108 | 16 | |||
| No | 618 | 12.2 (6.5–15.2) | 152 | 33.5 (29.0–39.6) | 22 | 182 | 6 | |||
| Targeted therapy | ||||||||||
| Yes | 717 | 21.4 (11.0–23.6) | 0.395 (0.296–0.527), <0.0001 | 191 | 83.2 (53.0–94.2) | 9 | 70 | 4 | ||
| No | 1168 | 5.7 (4.0–10.9) | – | 166 | 32.9 (25.0–54.3) | 56 | 252 | 18 | ||
| Patients [n] | Pooled Median OS (95% CI) [Months] | Pooled HR (95% CI), p-Value | ||||
|---|---|---|---|---|---|---|
| Primary Cancer Location | ||||||
| Lung | ||||||
| EFGR | ||||||
| Yes | 367 | 24.9 (23.9–25.3) | 0.664 (0.510–0.865), 0.002 | |||
| No | 467 | 8.8 (5.2–14.6) | – | |||
| Breast | ||||||
| Luminal A | 113 | 27.8 (22.5–35.6) | ||||
| Luminal B | 34 | 43.0 (26.9–48.8) | ||||
| Basal (Triple- negative) | 88 | 11.6 (5.5–17.3) | 3.204 (1.175–8.738), 0.023 | |||
| HER2+ | 106 | 38.2 (20.9–74.5) | 0.449 (0.187–1.083), 0.075 | |||
| ER+ | 162 | 37.0 (32.0–61.0) | 0.323 (0.187–0.559), <0.0001 | |||
| PR+ | 140 | 37.7 (36.0–49.0) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groszman, L.; Hubermann, J.A.; Kooner, P.; Alamiri, N.; Bozzo, A.; Aoude, A. The Impact of Adjunct Medical Therapy on Survival after Spine Metastasis: A Systematic Review and Pooled Data Analysis. Cancers 2024, 16, 1425. https://doi.org/10.3390/cancers16071425
Groszman L, Hubermann JA, Kooner P, Alamiri N, Bozzo A, Aoude A. The Impact of Adjunct Medical Therapy on Survival after Spine Metastasis: A Systematic Review and Pooled Data Analysis. Cancers. 2024; 16(7):1425. https://doi.org/10.3390/cancers16071425
Chicago/Turabian StyleGroszman, Lilly, Jonathan A. Hubermann, Paul Kooner, Nawaf Alamiri, Anthony Bozzo, and Ahmed Aoude. 2024. "The Impact of Adjunct Medical Therapy on Survival after Spine Metastasis: A Systematic Review and Pooled Data Analysis" Cancers 16, no. 7: 1425. https://doi.org/10.3390/cancers16071425
APA StyleGroszman, L., Hubermann, J. A., Kooner, P., Alamiri, N., Bozzo, A., & Aoude, A. (2024). The Impact of Adjunct Medical Therapy on Survival after Spine Metastasis: A Systematic Review and Pooled Data Analysis. Cancers, 16(7), 1425. https://doi.org/10.3390/cancers16071425