
Validation of the Standardized Needs Evaluation Questionnaire in Polish Cancer Patients
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Selection of an Instrument to Assess the Needs of Polish Cancer Patients
2.2. Preparation of Polish Version of the NEQ
2.3. Assessment of the NEQ
2.3.1. NEQ Comprehensibility and Acceptability
2.3.2. Content Analysis
2.3.3. Validation of the Polish Version of the NEQ
Reliability
Construct Validity
2.4. Patients
3. Results
3.1. Patient Characteristics
3.2. Willingness to Participate in the Survey
3.3. Prevalence of Needs
3.4. Comprehensibility and Acceptability of the Questionnaire
3.5. Content Analysis
3.6. Reliability
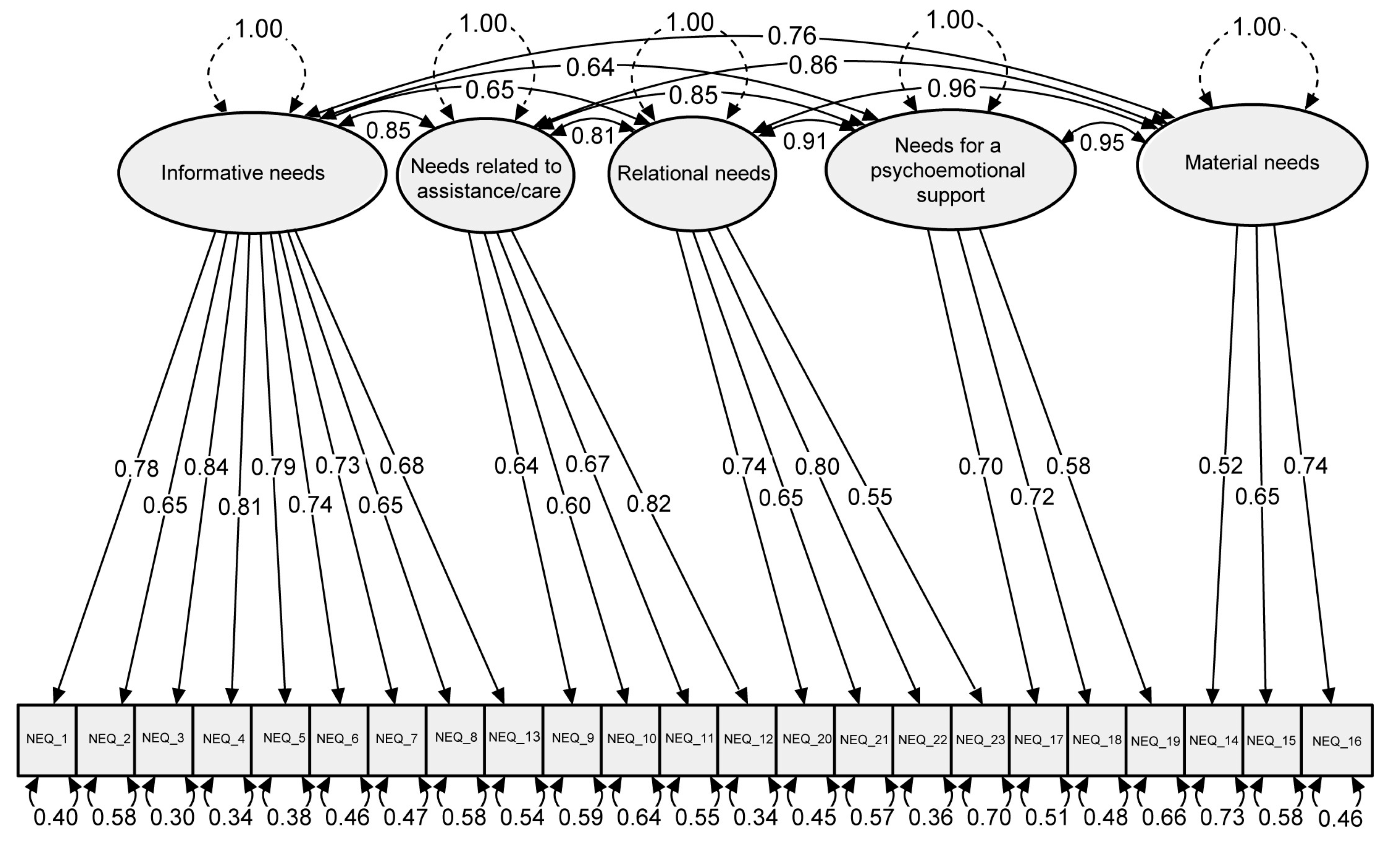
3.7. Construct Validity
4. Discussion
4.1. Clinical Implications
4.2. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moghaddam, N.; Coxon, H.; Nabarro, S.; Hardy, B.; Cox, K. Unmet care needs in people living with advanced cancer: A systematic review. Support. Care Cancer 2016, 24, 3609–3622. [Google Scholar] [CrossRef]
- Okediji, P.T.; Salako, O.; Fatiregun, O.O. Pattern and predictors of unmet supportive care needs in cancer patients. Cureus 2017, 9, e1234. [Google Scholar] [CrossRef] [PubMed]
- Graf, J.; Junne, F.; Ehrenthal, J.C.; Schäffeler, N.; Schwille-Kiuntke, J.; Stengel, A.; Mehnert-Theuerkauf, A.; Marwedel, L.; Brucker, S.Y.; Zipfel, S.; et al. Unmet supportive care needs among women with breast and gynecological cancer: Relevance of attachment anxiety and psychological distress. Front. Psychol. 2020, 11, 558190. [Google Scholar] [CrossRef] [PubMed]
- Driessen, H.P.A.; Busschbach, J.J.V.; van der Rijt, C.C.D.; Elfrink, E.J.; Raijmakers, N.J.H.; Van Roij, J.; Rietjens, J.; Kranenburg, L.W. Unmet care needs of patients with advanced cancer and their relatives: Multicentre observational study. BMJ Support. Palliat. Care 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Okamura, M.; Fujimori, M.; Sato, A.; Uchitomi, Y. Unmet supportive care needs and associated factors among young adult cancer patients in Japan. BMC Cancer 2021, 21, 17. [Google Scholar] [CrossRef] [PubMed]
- Sodergren, S.C.; Wheelwright, S.J.; Permyakova, N.V.; Patel, M.; Calman, L.; Smith, P.W.F.; Din, A.; Richardson, A.; Fenlon, D.; Winter, J.; et al. Supportive care needs of patients following treatment for colorectal cancer: Risk factors for unmet needs and the association between unmet needs and health-related quality of life-results from the ColoREctal Wellbeing (CREW) study. J. Cancer Surviv. 2019, 13, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Evans Webb, M.; Murray, E.; Younger, Z.W.; Goodfellow, H.; Ross, J. The supportive care needs of cancer patients: A systematic review. J. Cancer Educ. 2021, 36, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Tamburini, M.; Gangeri, L.; Brunelli, C.; Boeri, P.; Borreani, C.; Bosisio, M.; Karmann, C.F.; Greco, M.; Miccinesi, G.; Murru, L.; et al. Cancer patients’ needs during hospitalization: A quantitative and qualitative study. BMC Cancer 2003, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Willems, R.A.; Bolman, C.A.; Mesters, I.; Kanera, I.M.; Beaulen, A.A.J.M.; Lechner, L. Cancer survivors in the first year after treatment: The prevalence and correlates of unmet needs in different domains. Psychooncology 2016, 25, 51–57. [Google Scholar] [CrossRef]
- Girgis, A.; Boyes, A.; Sanson-Fisher, R.W.; Burrows, S. Perceived needs of women diagnosed with breast cancer: Rural versus urban location. Aust. N. Z. J. Public Health 2000, 24, 166–173. [Google Scholar] [CrossRef]
- Sutherland, G.; Hill, D.; Morand, M.; Pruden, M.; Mclachlan, S.-A. Assessing the unmet supportive care needs of newly diagnosed patients with cancer. Eur. J. Cancer Care 2009, 18, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Williams, P.; Redman, S.; White, K.; King, E. Assessing the practical and psychosocial needs of rural women with early breast cancer in Australia. Soc. Work Health Care 2003, 36, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Soothill, K.; Morris, S.M.; Harman, J.; Francis, B.; Thomas, C.; McIllmurray, M.B. The significant unmet needs of cancer patients: Probing psychosocial concerns. Support. Care Cancer 2001, 9, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Clavarino, A.M.; Lowe, J.B.; Carmont, S.-A.; Balanda, K. The needs of cancer patients and their families from rural and remote areas of Queensland. Aust. J. Rural. Health 2002, 10, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Bonacchi, A.; Rossi, A.; Bellotti, L.; Franco, S.; Toccafondi, A.; Miccinesi, G.; Rosselli, M. Assessment of psychological distress in cancer patients: A pivotal role for clinical interview. Psychooncology 2010, 19, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Nixon, A.; Narayanasamy, A. The spiritual needs of neurooncology patients from patients’ perspective. J. Clin. Nurs. 2010, 19, 2259–2370. [Google Scholar] [CrossRef] [PubMed]
- Wen, K.Y.; Gustafson, D.H. Needs assessment for cancer patients and their families. Health Qual. Life Outcomes 2004, 2, 11. [Google Scholar] [CrossRef]
- Cassileth, B.R.; Zupkis, R.V.; Sutton-Smith, K.; March, V. Information and participation preferences among cancer patients. Ann. Intern. Med. 1980, 92, 832–836. [Google Scholar] [CrossRef]
- Lupton, D. Your life in their hands: Trust in the medical encounter. In Health and the Sociology of Emotions; James, V., Gave, J., Eds.; Blackwell: Oxford, UK, 1996; pp. 157–172. [Google Scholar]
- Harrison, J.; Maguire, P.; Pitceathly, C. Confiding in crisis: Gender differences in pattern of confiding among cancer patients. Soc. Sci. Med. 1995, 41, 1255–1260. [Google Scholar] [CrossRef]
- Osowiecka, K.; Środa, R.; Saied, A.; Szwiec, M.; Mangold, S.; Osuch, D.; Nawrocki, S.; Rucinska, M. Patients’ non-medical and organizational needs during cancer diagnosis and treatment. Int. J. Environ. Res. Public Health 2020, 17, 5841. [Google Scholar] [CrossRef]
- Baum, M. What are the needs of patients diagnosed with cancer? Psychooncology 2004, 13, 850–852. [Google Scholar] [CrossRef]
- Carey, M.; Lambert, S.; Smits, R.; Paul, C.; Sanson-Fisher, R.; Clinton-McHarg, T. The unfulfilled promise: A systematic review of interventions to reduce the unmet supportive care needs of cancer patients. Support. Care Cancer 2012, 20, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.D.; Young, J.M.; Price, M.A.; Butow, P.N.; Solomon, M.J. What are the unmet supportive care needs of people with cancer? A systematic review. Support. Care Cancer 2009, 17, 1117–1128. [Google Scholar] [CrossRef] [PubMed]
- Fitch, M. Supportive care for cancer patients. Hosp. Q3 2000, 3, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Sanson-Fisher, R.; Girgis, A.; Boyes, A.; Bonevski, B.; Burton, L.; Cook, P. The unmet supportive care needs of patients with cancer. Supportive Care Review Group. Cancer 2000, 88, 226–237. [Google Scholar] [CrossRef]
- Uchwała nr 10 Rady Ministrów z dnia 4 lutego 2020 r. w Sprawie Przyjęcia Programu Wieloletniego pn. Narodowa Strategia Onkologiczna na Lata 2020–2030. Monitor Polski. 18 lutego 2020 poz. 189. Available online: https://eli.gov.pl/eli/MP/2020/189/ogl/pol (accessed on 15 May 2022).
- Richardson, A.; Medina, J.; Brown, V.; Sitzia, J. Patients’ needs assessment in cancer care: A review of assessment tools. Support. Care Cancer 2007, 15, 1125–1144. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, B.; Crowe, L.; Todd, A.; Sharp, L. Assessing unmet needs in advanced cancer patients: A systematic review of the development, content, and quality of available instruments. J. Cancer Surviv. 2022, 16, 960–975. [Google Scholar] [CrossRef]
- Annunziata, M.A.; Muzzatti, B.; Altoè, G. A contribution to the validation of the Needs Evaluation Questionnaire (NEQ): A study in the Italian context. Psychooncology 2009, 18, 549–553. [Google Scholar] [CrossRef]
- Tamburini, M.; Gangeri, L.; Brunelli, C.; Beltrami, E.; Boeri, P.; Borreani, C.; Fusco Karmann, C.; Greco, M.; Miccinesi, G.; Murru, L.; et al. Assessment of hospitalized cancer patients’ needs by the Needs Evaluation Questionnaire. Ann. Oncol. 2000, 11, 31–37. [Google Scholar] [CrossRef]
- Bonacchi, A.; Fazzini, E.; Messina, S.; Muraca, M.G.; Pacetti, P.; Di Miceli, S.; Miccinesi, G. Sociodemographic, clinical, and psychological characteristics identify groups of Italian cancer patients with high rates of unmet needs. Tumori 2019, 105, 288–295. [Google Scholar] [CrossRef]
- Bonacchi, A.; Miccinesi, G.; Galli, S.; Primi, C.; Chiesi, F.; Lippi, D.; Muraca, M.; Toccafondi, A. Use of the Needs Evaluation Questionnaire with cancer outpatients. Support. Care Cancer 2016, 24, 3507–3515. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, T.I.; Spinthouri, M.; Ramoutsaki, A.; Marnelou, A.; Kritsotakis, G.; Govina, O. Assessment of unmet supportive care needs in haematological cancer survivors. Asian Pac. J. Cancer Prev. 2019, 20, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Chiesi, F.; Bonacchi, A.; Primi, C.; Miccinesi, G. Assessing unmet needs in patients with cancer: An investigation of differential item functioning of the Needs Evaluation Questionnaire across gender, age and phase of the disease. PLoS ONE 2017, 12, e0179765. [Google Scholar] [CrossRef] [PubMed]
- Ripamonti, C.I.; Miccinesi, G.; Pessi, M.A.; Di Pede, P.; Ferrari, M. Is it possible to encourage hope in non-advanced cancer patients? We must try. Ann. Oncol. 2016, 27, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Romito, F.; Corvasce, C.; Montanaro, R.; Mattioli, V. Do elderly cancer patients have different care needs compared with younger ones? Tumori 2011, 97, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Gangeri, L.; Tamburini, M.; Borreani, C.; Brunelli, C.; Miccinesi, G.; Murru, L.; Boeri, P.; Mazzaferro, V. Candidates for liver transplantation for cancer: Physical, psychological, and social conditions. Transplantation 2002, 73, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Scaratti, C.; Leonardi, M.; Saladino, A.; Anghileri, E.; Broggi, M.; Lamperti, E.; Fariselli, L.; Ayadi, R.; Tringali, G.; Schiavolin, S. Needs of neuro-oncological patients and their caregivers during the hospitalization and after discharge: Results from a longitudinal study. Support. Care Cancer 2017, 25, 2137–2145. [Google Scholar] [CrossRef] [PubMed]
- Lucchiari, C.; Botturi, A.; Pravettoni, G. The impact of decision models on self-perceived quality of life: A study on brain cancer patients. Ecancermedicalscience 2010, 4, 187. [Google Scholar]
- Bonacchi, A.; Di Miceli, S.; Lippi, D.; Muraca, M.G.; Miccinesi, G. Unmet needs of Italian cancer patients in different stages of the disease and care process. Tumori 2018, 104, 285–291. [Google Scholar] [CrossRef]
- Włostowska, K.; Doboszynska, A.; Trylinska-Tekielska, E. Assessment of the needs of hospice patients and their relatives by the Needs Evaluation Questionnaire. Palliat. Med. Pract. 2018, 12, 186–192. [Google Scholar] [CrossRef]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Jöreskog, K.G. A general approach to confirmatory maximum likelihood factor analysis. Psychometrika 1969, 34, 183–202. [Google Scholar] [CrossRef]
- Fan, X.; Thompson, B.; Wang, L. Effects of sample size, estimation methods, and model specification on structural equation modeling fit indexes. Struct. Equ. Model. 1999, 6, 56–83. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Muller, H. Evaluating the fit of structural equation models: Tests of significance and goodness-of-fit models. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of test. Psychometrika 1951, 16, 197–334. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]


{kind=link}
| n | % | ||
|---|---|---|---|
| Gender | |||
| female | 72 | 59.5 | |
| male | 49 | 40.5 | |
| Age (years) range; median (25–75% IQR) | 30–88; 66 (55–70) | ||
| Education | |||
| primary | 14 | 11.6 | |
| secondary | 80 | 66.1 | |
| high | 27 | 22.3 | |
| Place of residence | |||
| city | 82 | 67.8 | |
| village | 39 | 32.2 | |
| Professional activity | |||
| active | 3 | 2.5 | |
| active, but on sick leave | 28 | 23.2 | |
| unemployed | 1 | 0.8 | |
| pensioner | 77 | 63.6 | |
| disability pensioner | 12 | 9.9 | |
| Marital status | |||
| married or in a stable informal relationship | 76 | 62.8 | |
| relationship broken during disease or in relation to disease | 0 | 0 | |
| single | 8 | 6.6 | |
| divorced | 11 | 9.1 | |
| widow/widower | 26 | 21.5 | |
| Living with | |||
| partner | 52 | 43.0 | |
| partner and child/children | 25 | 20.7 | |
| child/children | 10 | 8.3 | |
| another family member | 7 | 5.7 | |
| partner and another family member | 2 | 1.6 | |
| alone | 25 | 7 | |
| Having a medical doctor amongst close family or friends | |||
| yes | 19 | 15.7 | |
| no | 101 | 83.5 | |
| unknown | 1 | 0.8 | |
| Cancer | |||
| head and neck | 9 | 7.4 | |
| upper digestive system | 10 | 8.3 | |
| lower digestive system | 36 | 29.7 | |
| lung | 10 | 8.3 | |
| breast | 28 | 23.1 | |
| gynecological | 9 | 7.4 | |
| prostate | 14 | 11.6 | |
| brain | 2 | 1.7 | |
| unknown | 3 | 2.5 |
| n | % | |||
|---|---|---|---|---|
| Q1 | I need more information about my diagnosis | yes | 47 | 38.8 |
| no | 74 | 61.2 | ||
| Q2 | I need more information about my future condition | yes | 62 | 51.2 |
| no | 59 | 48.8 | ||
| Q3 | I need more information about the exams I am undergoing | yes | 47 | 38.9 |
| no | 73 | 60.3 | ||
| missing data | 1 | 0.8 | ||
| Q4 | I need more explanations of treatments | yes | 46 | 38.0 |
| no | 74 | 61.2 | ||
| missing data | 1 | 0.8 | ||
| Q5 | I need to be more involved in therapeutic choices | yes | 35 | 28.9 |
| no | 84 | 69.4 | ||
| missing data | 2 | 1.7 | ||
| Q6 | I need clinicians and nurses to give me more comprehensible information | yes | 46 | 38.0 |
| no | 74 | 61.2 | ||
| missing data | 1 | 0.8 | ||
| Q7 | I need clinicians to be more sincere with me | yes | 51 | 42.1 |
| no | 70 | 57.9 | ||
| Q8 | I need to have a better dialogue with clinicians | yes | 36 | 29.7 |
| no | 83 | 68.6 | ||
| missing data | 2 | 1.7 | ||
| Q9 | I need my symptoms (pain, nausea, insomnia, etc.)to be better controlled | yes | 45 | 37.2 |
| no | 76 | 62.8 | ||
| Q10 | I need more help with eating, dressing, and going to the bathroom | yes | 22 | 18.2 |
| no | 98 | 81.0 | ||
| missing data | 1 | 0.8 | ||
| Q11 | I need better respect for my intimacy | yes | 28 | 23.1 |
| no | 93 | 76.9 | ||
| Q12 | I need better attention from nurses | yes | 23 | 19.0 |
| no | 98 | 81.0 | ||
| Q13 | I need to be more reassured by the clinicians | yes | 45 | 37.2 |
| no | 76 | 62.8 | ||
| Q14 | I need better services from the hospital (bathrooms, meals, cleaning) | yes | 72 | 59.5 |
| no | 49 | 40.5 | ||
| Q15 | I need to have more economic insurance information (tickets, invalidity, etc.) in relation to my illness | yes | 54 | 44.6 |
| no | 66 | 54.6 | ||
| missing data | 1 | 0.8 | ||
| Q16 | I need economic help | yes | 33 | 27.3 |
| no | 88 | 72.7 | ||
| Q17 | I need to speak with a psychologist | yes | 30 | 24.8 |
| no | 90 | 74.4 | ||
| missing data | 1 | 0.8 | ||
| Q18 | I need to speak with a spiritual advisor | yes | 23 | 19.0 |
| no | 98 | 81.0 | ||
| Q19 | I need to speak with people who have had this same experience | yes | 50 | 41.3 |
| no | 71 | 58.7 | ||
| Q20 | I need to be more reassured by my relatives | yes | 29 | 24.0 |
| no | 92 | 76.0 | ||
| Q21 | I need to feel more useful within my family | yes | 44 | 36.4 |
| no | 76 | 62.8 | ||
| missing data | 1 | 0.8 | ||
| Q22 | I need to feel less abandoned | yes | 35 | 28.9 |
| no | 86 | 71.1 | ||
| Q23 | I need to receive less commiseration from other people | yes | 42 | 34.7 |
| no | 79 | 65.3 | ||
| n | % | |
|---|---|---|
| Is the form of the questionnaire good in your opinion? | ||
| yes | 119 | 98.4 |
| no | 1 | 0.8 |
| no data | 1 | 0.8 |
| Is the font size big enough in your opinion? | ||
| yes | 113 | 93.4 |
| no | 7 | 5.8 |
| no data | 1 | 0.8 |
| Do you think that the questionnaire is sufficiently long? | ||
| yes | 98 | 81.0 |
| no, should be shorter | 19 | 15.7 |
| no, should be longer | 4 | 3.3 |
| Are the questions generally understandable in your opinion? | ||
| yes | 105 | 86.8 |
| no | 16 | 13.2 |
| Are any questions difficult for you to answer clearly? | ||
| yes | 20 | 16.5 |
| no | 100 | 82.7 |
| no data | 1 | 0.8 |
| Are there any questions you do not want to answer? | ||
| yes | 8 | 6.6 |
| no | 112 | 92.6 |
| no data | 1 | 0.8 |
| Is there anything else you would like to discuss about your needs? | ||
| yes | 10 | 8.3 |
| no | 109 | 90.0 |
| no data | 2 | 1.7 |
| Do you think that completing this questionnaire may facilitate better contact with the doctor/nurse/other staff? | ||
| yes | 96 | 79.3 |
| no | 25 | 20.7 |
| Did you identify any important needs that you did not recognize before the questionnaire? | ||
| yes | 8 | 6.6 |
| no | 112 | 92.6 |
| no data | 1 | 0.8 |
| Item Number | % of Consensus Responses | Cohen’s Kappa | Asymptotic Error of Kappa | p |
|---|---|---|---|---|
| Q1 | 93.5 | 0.78 ** | 0.12 | <0.001 |
| Q2 | 91.3 | 0.80 ** | 0.09 | <0.001 |
| Q3 | 93.3 | 0.83 * | 0.09 | <0.001 |
| Q4 | 91.3 | 0.70 ** | 0.14 | <0.001 |
| Q5 | 97.7 | 0.93 * | 0.07 | <0.001 |
| Q6 | 91.1 | 0.72 ** | 0.13 | <0.001 |
| Q7 | 95.7 | 0.90 * | 0.07 | <0.001 |
| Q8 | 95.6 | 0.86 * | 0.10 | <0.001 |
| Q9 | 87.0 | 0.60 *** | 0.14 | <0.001 |
| Q10 | 97.8 | 0.85 * | 0.15 | <0.001 |
| Q11 | 95.7 | 0.81 * | 0.13 | <0.001 |
| Q12 | 93.5 | 0.69 ** | 0.17 | <0.001 |
| Q13 | 93.5 | 0.83 * | 0.10 | <0.001 |
| Q14 | 91.3 | 0.81 * | 0.09 | <0.001 |
| Q15 | 97.8 | 0.95 * | 0.05 | <0.001 |
| Q16 | 97.8 | 0.88 * | 0.12 | <0.001 |
| Q17 | 100.0 | 1.00 * | 0.00 | <0.001 |
| Q18 | 97.8 | 0.90 * | 0.10 | <0.001 |
| Q19 | 95.7 | 0.83 * | 0.10 | <0.001 |
| Q20 | 95.7 | 0.86 * | 0.10 | <0.001 |
| Q21 | 88.9 | 0.64 ** | 0.15 | <0.001 |
| Q22 | 95.7 | 0.83 * | 0.12 | <0.001 |
| Q23 | 100.0 | 1.00 * | 0.00 | <0.001 |
| Item Number | Cronbach’s α | 95% CI | |
|---|---|---|---|
| Informative needs | Q1–Q8, Q13 | 0.91 | 0.88–0.93 |
| Needs related to assistance/care | Q9–Q12 | 0.74 | 0.65–0.80 |
| Material needs | Q14–Q16 | 0.70 | 0.59–0.78 |
| Need for psycho-emotional support | Q17–Q19 | 0.65 | 0.52–0.74 |
| Relational needs | Q20–Q23 | 0.78 | 0.70–0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osowiecka, K.; Dolińska, A.; Szwiec, M.; Działach, E.; Nowakowski, J.J.; Rucińska, M. Validation of the Standardized Needs Evaluation Questionnaire in Polish Cancer Patients. Cancers 2024, 16, 1451. https://doi.org/10.3390/cancers16081451
Osowiecka K, Dolińska A, Szwiec M, Działach E, Nowakowski JJ, Rucińska M. Validation of the Standardized Needs Evaluation Questionnaire in Polish Cancer Patients. Cancers. 2024; 16(8):1451. https://doi.org/10.3390/cancers16081451
Chicago/Turabian StyleOsowiecka, Karolina, Anna Dolińska, Marek Szwiec, Eliza Działach, Jacek J. Nowakowski, and Monika Rucińska. 2024. "Validation of the Standardized Needs Evaluation Questionnaire in Polish Cancer Patients" Cancers 16, no. 8: 1451. https://doi.org/10.3390/cancers16081451