
Predictors of Survival, Treatment Modalities, and Clinical Outcomes of Diffuse Large B-Cell Lymphoma in Patients Older Than 70 Years Still an Unmet Medical Need in 2024 Based on Real-World Evidence
 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Ethical Issues
2.2. Patients, Elegibility Criteria, and Staging Procedures
2.3. Up-front Therapy, Response Assessment, and Follow-Up
2.4. Histopathological Diagnosis
2.5. Statistical Analysis
3. Results
3.1. Clinical, Epidemiological, Laboratorial, and Histopathological Findings
3.2. Up-Front Therapy for Elderly DLBCL, NOS Patients: Modalities, Responses, and Toxicities
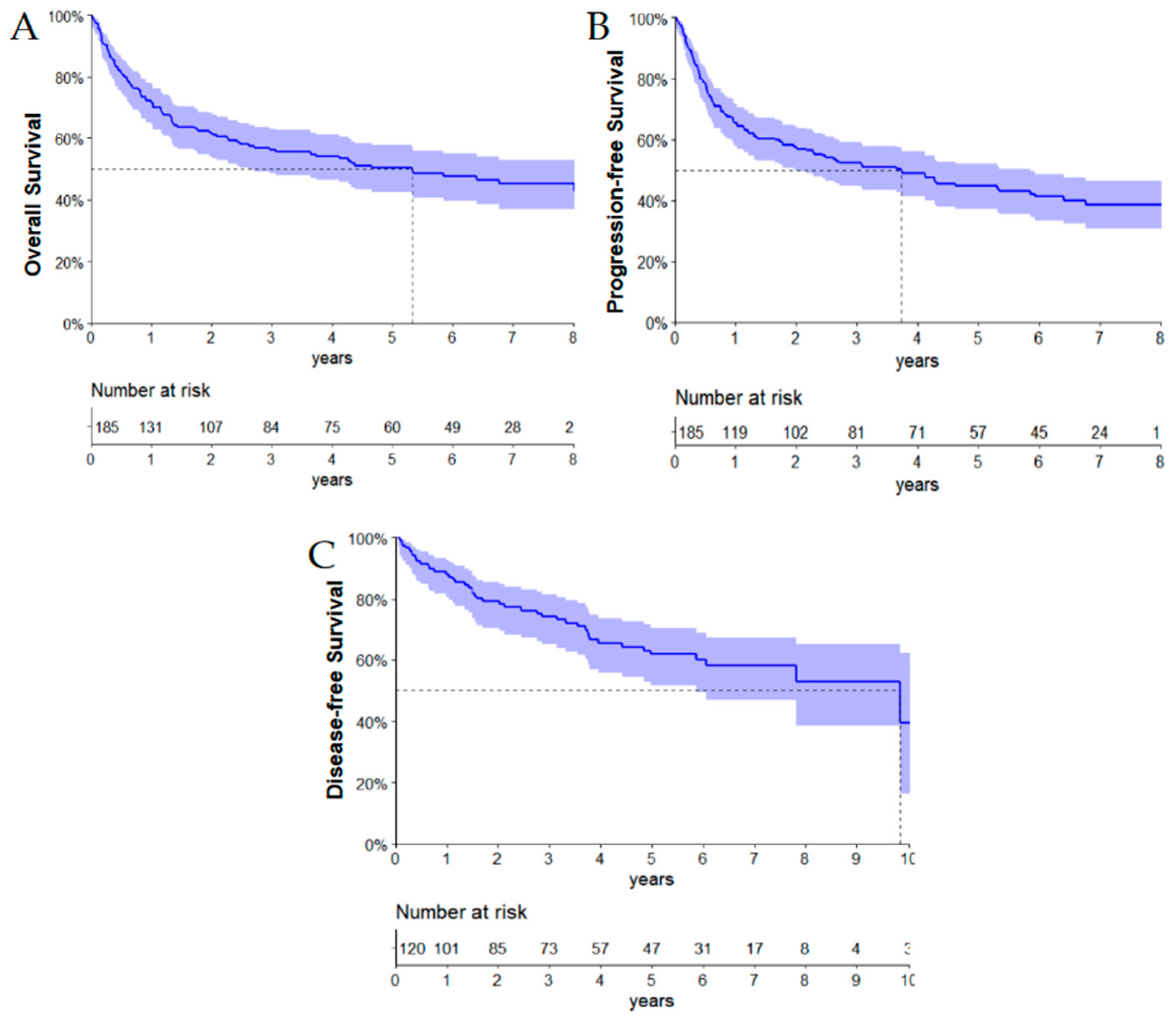
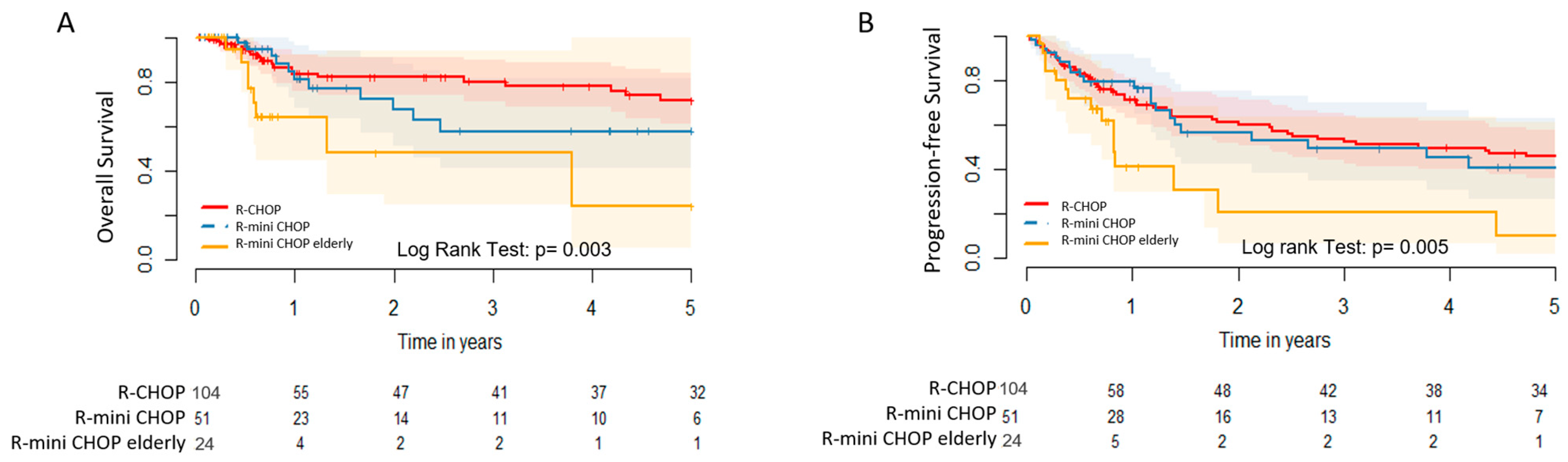
3.3. Clinical Outcomes
3.4. Prognostic Factors: Univariate and Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef]
- Sehn, L.H.; Salles, G. Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2021, 384, 842–858. [Google Scholar] [CrossRef]
- Poletto, S.; Novo, M.; Paruzzo, L.; Frascione, P.M.M.; Vitolo, U. Treatment strategies for patients with diffuse large B-cell lymphoma. Cancer Treat. Rev. 2022, 110, 102443. [Google Scholar] [CrossRef]
- Martelli, M.; Ferreri, A.J.; Agostinelli, C.; Di Rocco, A.; Pfreundschuh, M.; Pileri, S.A. Diffuse large B-cell lymphoma. Crit. Rev. Oncol./Hematol. 2013, 87, 146–171. [Google Scholar] [CrossRef] [PubMed]
- Kanas, G.; Ge, W.; Quek, R.G.W.; Keeven, K.; Nersesyan, K.; Jon, E.A. Epidemiology of diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL) in the United States and Western Europe: Population-level projections for 2020-2025. Leuk. Lymphoma 2022, 63, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Campisi, J. Aging, cellular senescence, and cancer. Annu. Rev. Physiol. 2013, 75, 685–705. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, S.E.; Gladyshev, V.N.; Aryee, M.J.; Bernstein, B.E. Epigenetic clocks, aging, and cancer. Science 2022, 378, 1276–1277. [Google Scholar] [CrossRef]
- López-Otín, C.; Pietrocola, F.; Roiz-Valle, D.; Galluzzi, L.; Kroemer, G. Meta-hallmarks of aging and cancer. Cell Metab. 2023, 35, 12–35. [Google Scholar] [CrossRef]
- Moccia, A.A.; Thieblemont, C. Curing diffuse large B-cell lymphomas in elderly patients. Eur. J. Intern. Med. 2018, 58, 14–21. [Google Scholar] [CrossRef]
- Chiappella, A.; Castellino, A.; Nicolosi, M.; Santambrogio, E.; Vitolo, U. Diffuse Large B-cell Lymphoma in the elderly: Standard treatment and new perspectives. Expert Rev. Hematol. 2017, 10, 289–297. [Google Scholar] [CrossRef]
- Allen, P. Diffuse Large B-Cell Lymphoma in the Elderly: Current Approaches. Curr. Oncol. Rep. 2020, 22, 114. [Google Scholar] [CrossRef]
- Grann, V.R.; Hershman, D.; Jacobson, J.S.; Tsai, W.Y.; Wang, J.; McBride, R.; Mitra, N.; Grossbard, M.L.; Neugut, A.I. Outcomes and diffusion of doxorubicin-based chemotherapy among elderly patients with aggressive non-Hodgkin lymphoma. Cancer 2006, 107, 1530–1541. [Google Scholar] [CrossRef]
- Caimi, P.F.; Barr, P.M.; Berger, N.A.; Lazarus, H.M. Non-Hodgkin’s lymphoma in the elderly. Drugs Aging 2010, 27, 211–238. [Google Scholar] [CrossRef]
- Tucci, A.; Martelli, M.; Rigacci, L.; Riccomagno, P.; Cabras, M.G.; Salvi, F.; Stelitano, C.; Fabbri, A.; Storti, S.; Fogazzi, S.; et al. Comprehensive geriatric assessment is an essential tool to support treatment decisions in elderly patients with diffuse large B-cell lymphoma: A prospective multicenter evaluation in 173 patients by the Lymphoma Italian Foundation (FIL). Leuk. Lymphoma 2015, 56, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Tilly, H.; Morschhauser, F.; Sehn, L.H.; Friedberg, J.W.; Trněný, M.; Sharman, J.P.; Herbaux, C.; Burke, J.M.; Matasar, M.; Rai, S.; et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 351–363. [Google Scholar] [CrossRef] [PubMed]
- Nastoupil, L.J.; Bartlett, N.L. Navigating the Evolving Treatment Landscape of Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2023, 41, 903–913. [Google Scholar] [CrossRef]
- Tavares, A.; Moreira, I. Diffuse large B-cell lymphoma in very elderly patients: Towards best tailored treatment—A systematic review. Crit. Rev. Oncol. /Hematol. 2021, 160, 103294. [Google Scholar] [CrossRef] [PubMed]
- Spinner, M.A.; Advani, R.H. Current Frontline Treatment of Diffuse Large B-Cell Lymphoma. Oncology 2022, 36, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Lin, T.L.; Kuo, M.C.; Shih, L.Y.; Dunn, P.; Wang, P.N.; Wu, J.H.; Tang, T.C.; Chang, H.; Hung, Y.S. The impact of age, Charlson comorbidity index, and performance status on treatment of elderly patients with diffuse large B cell lymphoma. Ann. Hematol. 2012, 91, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N. Engl. J. Med. 1993, 329, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Sehn, L.H.; Berry, B.; Chhanabhai, M.; Fitzgerald, C.; Gill, K.; Hoskins, P.; Klasa, R.; Savage, K.J.; Shenkier, T.; Sutherland, J.; et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood 2007, 109, 1857–1861. [Google Scholar] [CrossRef]
- Zhou, Z.; Sehn, L.H.; Rademaker, A.W.; Gordon, L.I.; Lacasce, A.S.; Crosby-Thompson, A.; Vanderplas, A.; Zelenetz, A.D.; Abel, G.A.; Rodriguez, M.A.; et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 2014, 123, 837–842. [Google Scholar] [CrossRef]
- Hans, C.P.; Weisenburger, D.D.; Greiner, T.C.; Gascoyne, R.D.; Delabie, J.; Ott, G.; Müller-Hermelink, H.K.; Campo, E.; Braziel, R.M.; Jaffe, E.S.; et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004, 103, 275–282. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Di, M.; Huntington, S.F.; Olszewski, A.J. Challenges and Opportunities in the Management of Diffuse Large B-Cell Lymphoma in Older Patients. Oncol. 2021, 26, 120–132. [Google Scholar] [CrossRef]
- Khan, Y.; Brem, E.A. Considerations for the Treatment of Diffuse Large B Cell Lymphoma in the Elderly. Curr. Hematol. Malig. Rep. 2019, 14, 228–238. [Google Scholar] [CrossRef]
- Peyrade, F.; Jardin, F.; Thieblemont, C.; Thyss, A.; Emile, J.F.; Castaigne, S.; Coiffier, B.; Haioun, C.; Bologna, S.; Fitoussi, O.; et al. Attenuated immunochemotherapy regimen (R-miniCHOP) in elderly patients older than 80 years with diffuse large B-cell lymphoma: A multicentre, single-arm, phase 2 trial. Lancet. Oncol. 2011, 12, 460–468. [Google Scholar] [CrossRef]
- Meguro, A.; Ozaki, K.; Sato, K.; Oh, I.; Fujiwara, S.; Hosonuma, R.; Sasazaki, M.; Kikuchi, Y.; Hirata, Y.; Yamamoto, C.; et al. Rituximab plus 70% cyclophosphamide, doxorubicin, vincristine and prednisone for Japanese patients with diffuse large B-cell lymphoma aged 70 years and older. Leuk. Lymphoma 2012, 53, 43–49. [Google Scholar] [CrossRef]
- Wang, Y.; Ren, X.; Huang, K.; Liang, X.; Pu, L.; Hu, L.; Zhai, Z. Comparison of first-line treatments for elderly patients with diffuse large B-cell lymphoma: A systematic review and network meta-analysis. Front. Immunol. 2022, 13, 1082293. [Google Scholar] [CrossRef]
- Coiffier, B.; Lepage, E.; Briere, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Feugier, P.; Van Hoof, A.; Sebban, C.; Solal-Celigny, P.; Bouabdallah, R.; Fermé, C.; Christian, B.; Lepage, E.; Tilly, H.; Morschhauser, F.; et al. Long-term results of the R-CHOP study in the treatment of elderly patients with diffuse large B-cell lymphoma: A study by the Groupe d’Etude des Lymphomes de l’Adulte. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 4117–4126. [Google Scholar] [CrossRef]
- Pfreundschuh, M.; Schubert, J.; Ziepert, M.; Schmits, R.; Mohren, M.; Lengfelder, E.; Reiser, M.; Nickenig, C.; Clemens, M.; Peter, N.; et al. Six versus eight cycles of bi-weekly CHOP-14 with or without rituximab in elderly patients with aggressive CD20+ B-cell lymphomas: A randomised controlled trial (RICOVER-60). Lancet. Oncol. 2008, 9, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Delarue, R.; Tilly, H.; Mounier, N.; Petrella, T.; Salles, G.; Thieblemont, C.; Bologna, S.; Ghesquières, H.; Hacini, M.; Fruchart, C.; et al. Dose-dense rituximab-CHOP compared with standard rituximab-CHOP in elderly patients with diffuse large B-cell lymphoma (the LNH03-6B study): A randomised phase 3 trial. Lancet. Oncol. 2013, 14, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Hawkes, E.A.; Jack, A.; Qian, W.; Smith, P.; Mouncey, P.; Pocock, C.; Ardeshna, K.M.; Radford, J.A.; McMillan, A.; et al. Rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone in patients with newly diagnosed diffuse large B-cell non-Hodgkin lymphoma: A phase 3 comparison of dose intensification with 14-day versus 21-day cycles. Lancet 2013, 381, 1817–1826. [Google Scholar] [CrossRef]
- Kühnl, A.; Cunningham, D.; Counsell, N.; Hawkes, E.A.; Qian, W.; Smith, P.; Chadwick, N.; Lawrie, A.; Mouncey, P.; Jack, A.; et al. Outcome of elderly patients with diffuse large B-cell lymphoma treated with R-CHOP: Results from the UK NCRI R-CHOP14v21 trial with combined analysis of molecular characteristics with the DSHNHL RICOVER-60 trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Corazzelli, G.; Frigeri, F.; Arcamone, M.; Lucania, A.; Rosariavilla, M.; Morelli, E.; Amore, A.; Capobianco, G.; Caronna, A.; Becchimanzi, C.; et al. Biweekly rituximab, cyclophosphamide, vincristine, non-pegylated liposome-encapsulated doxorubicin and prednisone (R-COMP-14) in elderly patients with poor-risk diffuse large B-cell lymphoma and moderate to high ‘life threat’ impact cardiopathy. Br. J. Haematol. 2011, 154, 579–589. [Google Scholar] [CrossRef]
- Merli, F.; Luminari, S.; Rossi, G.; Mammi, C.; Marcheselli, L.; Tucci, A.; Ilariucci, F.; Chiappella, A.; Musso, M.; Di Rocco, A.; et al. Cyclophosphamide, doxorubicin, vincristine, prednisone and rituximab versus epirubicin, cyclophosphamide, vinblastine, prednisone and rituximab for the initial treatment of elderly “fit” patients with diffuse large B-cell lymphoma: Results from the ANZINTER3 trial of the Intergruppo Italiano Linfomi. Leuk. Lymphoma 2012, 53, 581–588. [Google Scholar] [CrossRef]
- Park, S.I.; Grover, N.S.; Olajide, O.; Asch, A.S.; Wall, J.G.; Richards, K.L.; Sobol, A.L.; Deal, A.M.; Ivanova, A.; Foster, M.C.; et al. A phase II trial of bendamustine in combination with rituximab in older patients with previously untreated diffuse large B-cell lymphoma. Br. J. Haematol. 2016, 175, 281–289. [Google Scholar] [CrossRef]
- Fields, P.A.; Townsend, W.; Webb, A.; Counsell, N.; Pocock, C.; Smith, P.; Jack, A.; El-Mehidi, N.; Johnson, P.W.; Radford, J.; et al. De novo treatment of diffuse large B-cell lymphoma with rituximab, cyclophosphamide, vincristine, gemcitabine, and prednisolone in patients with cardiac comorbidity: A United Kingdom National Cancer Research Institute trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 282–287. [Google Scholar] [CrossRef]
- Shen, Q.D.; Zhu, H.Y.; Wang, L.; Fan, L.; Liang, J.H.; Cao, L.; Wu, W.; Xia, Y.; Li, J.Y.; Xu, W. Gemcitabine-oxaliplatin plus rituximab (R-GemOx) as first-line treatment in elderly patients with diffuse large B-cell lymphoma: A single-arm, open-label, phase 2 trial. Lancet. Haematol. 2018, 5, e261–e269. [Google Scholar] [CrossRef]
- Moccia, A.A.; Schaff, K.; Hoskins, P.; Klasa, R.; Savage, K.J.; Shenkier, T.; Gascoyne, R.D.; Connors, J.M.; Sehn, L.H. R-CHOP with Etoposide Substituted for Doxorubicin (R-CEOP): Excellent Outcome in Diffuse Large B Cell Lymphoma for Patients with a Contraindication to Anthracyclines. Blood 2009, 114, 408. [Google Scholar] [CrossRef]
- Merli, F.; Luminari, S.; Rossi, G.; Mammi, C.; Marcheselli, L.; Ferrari, A.; Spina, M.; Tucci, A.; Stelitano, C.; Capodanno, I.; et al. Outcome of frail elderly patients with diffuse large B-cell lymphoma prospectively identified by Comprehensive Geriatric Assessment: Results from a study of the Fondazione Italiana Linfomi. Leuk. Lymphoma 2014, 55, 38–43. [Google Scholar] [CrossRef]
- Ong, D.M.; Ashby, M.; Grigg, A.; Gard, G.; Ng, Z.Y.; Huang, H.E.; Chong, Y.S.; Cheah, C.Y.; Devitt, B.; Chong, G.; et al. Comprehensive geriatric assessment is useful in an elderly Australian population with diffuse large B-cell lymphoma receiving rituximab-chemotherapy combinations. Br. J. Haematol. 2019, 187, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Spina, M.; Balzarotti, M.; Uziel, L.; Ferreri, A.J.; Fratino, L.; Magagnoli, M.; Talamini, R.; Giacalone, A.; Ravaioli, E.; Chimienti, E.; et al. Modulated chemotherapy according to modified comprehensive geriatric assessment in 100 consecutive elderly patients with diffuse large B-cell lymphoma. Oncol. 2012, 17, 838–846. [Google Scholar] [CrossRef]
- Olivieri, A.; Gini, G.; Bocci, C.; Montanari, M.; Trappolini, S.; Olivieri, J.; Brunori, M.; Catarini, M.; Guiducci, B.; Isidori, A.; et al. Tailored therapy in an unselected population of 91 elderly patients with DLBCL prospectively evaluated using a simplified CGA. Oncol. 2012, 17, 663–672. [Google Scholar] [CrossRef]
- Marchesi, F.; Cenfra, N.; Altomare, L.; Dessanti, M.L.; Mecarocci, S.; Cerchiara, E.; Rago, A.; D’Andrea, M.; Tomarchio, V.; Olimpieri, O.M.; et al. A retrospective study on 73 elderly patients (≥75years) with aggressive B-cell non Hodgkin lymphoma: Clinical significance of treatment intensity and comprehensive geriatric assessment. J. Geriatr. Oncol. 2013, 4, 242–248. [Google Scholar] [CrossRef]
- Vitolo, U.; Chiappella, A.; Franceschetti, S.; Carella, A.M.; Baldi, I.; Inghirami, G.; Spina, M.; Pavone, V.; Ladetto, M.; Liberati, A.M.; et al. Lenalidomide plus R-CHOP21 in elderly patients with untreated diffuse large B-cell lymphoma: Results of the REAL07 open-label, multicentre, phase 2 trial. Lancet. Oncol. 2014, 15, 730–737. [Google Scholar] [CrossRef]
- Thieblemont, C.; Tilly, H.; Gomes da Silva, M.; Casasnovas, R.O.; Fruchart, C.; Morschhauser, F.; Haioun, C.; Lazarovici, J.; Grosicka, A.; Perrot, A.; et al. Lenalidomide Maintenance Compared With Placebo in Responding Elderly Patients With Diffuse Large B-Cell Lymphoma Treated With First-Line Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2473–2481. [Google Scholar] [CrossRef]
- Younes, A.; Sehn, L.H.; Johnson, P.; Zinzani, P.L.; Hong, X.; Zhu, J.; Patti, C.; Belada, D.; Samoilova, O.; Suh, C.; et al. Randomized Phase III Trial of Ibrutinib and Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone in Non-Germinal Center B-Cell Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 1285–1295. [Google Scholar] [CrossRef]
- Ram, R.; Grisariu, S.; Shargian-Alon, L.; Amit, O.; Bar-On, Y.; Stepensky, P.; Yeshurun, M.; Avni, B.; Hagin, D.; Perry, C.; et al. Toxicity and efficacy of chimeric antigen receptor T-cell therapy in patients with diffuse large B-cell lymphoma above the age of 70 years compared to younger patients—A matched control multicenter cohort study. Haematologica 2022, 107, 1111–1118. [Google Scholar] [CrossRef]
- Thieblemont, C.; Phillips, T.; Ghesquieres, H.; Cheah, C.Y.; Clausen, M.R.; Cunningham, D.; Do, Y.R.; Feldman, T.; Gasiorowski, R.; Jurczak, W.; et al. Epcoritamab, a Novel, Subcutaneous CD3xCD20 Bispecific T-Cell-Engaging Antibody, in Relapsed or Refractory Large B-Cell Lymphoma: Dose Expansion in a Phase I/II Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2023, 41, 2238–2247. [Google Scholar] [CrossRef]
- Olszewski, A.J.; Avigdor, A.; Babu, S.; Levi, I.; Eradat, H.; Abadi, U.; Holmes, H.; McKinney, M.; Woszczyk, D.; Giannopoulos, K.; et al. Mosunetuzumab Monotherapy Continues to Demonstrate Promising Efficacy and Durable Complete Responses in Elderly/Unfit Patients with Previously Untreated Diffuse Large B-Cell Lymphoma. Blood 2022, 140, 1778–1780. [Google Scholar] [CrossRef]
- Balducci, L.; Beghe, C. The application of the principles of geriatrics to the management of the older person with cancer. Crit. Rev. Oncol. /Hematol. 2000, 35, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Tucci, A.; Ferrari, S.; Bottelli, C.; Borlenghi, E.; Drera, M.; Rossi, G. A comprehensive geriatric assessment is more effective than clinical judgment to identify elderly diffuse large cell lymphoma patients who benefit from aggressive therapy. Cancer 2009, 115, 4547–4553. [Google Scholar] [CrossRef] [PubMed]
- van Spronsen, D.J.; Janssen-Heijnen, M.L.; Lemmens, V.E.; Peters, W.G.; Coebergh, J.W. Independent prognostic effect of co-morbidity in lymphoma patients: Results of the population-based Eindhoven Cancer Registry. Eur. J. Cancer 2005, 41, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Janssen-Heijnen, M.L.; van Spronsen, D.J.; Lemmens, V.E.; Houterman, S.; Verheij, K.D.; Coebergh, J.W. A population-based study of severity of comorbidity among patients with non-Hodgkin’s lymphoma: Prognostic impact independent of International Prognostic Index. Br. J. Haematol. 2005, 129, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Fujita, K.; Morishita, T.; Negoro, E.; Oiwa, K.; Tsukasaki, H.; Yamamura, O.; Ueda, T.; Yamauchi, T. Prognostic utility of a geriatric nutritional risk index in combination with a comorbidity index in elderly patients with diffuse large B cell lymphoma. Br. J. Haematol. 2021, 192, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Borg, I.H.; Bendtsen, M.D.; Bøgsted, M.; Madsen, J.; Severinsen, M.T. Incidence of venous thromboembolism in patients with diffuse large B-cell lymphoma. Leuk. Lymphoma 2016, 57, 2771–2776. [Google Scholar] [CrossRef] [PubMed]
- Mareschal, S.; Lanic, H.; Ruminy, P.; Bastard, C.; Tilly, H.; Jardin, F. The proportion of activated B-cell like subtype among de novo diffuse large B-cell lymphoma increases with age. Haematologica 2011, 96, 1888–1890. [Google Scholar] [CrossRef] [PubMed]
- Klapper, W.; Kreuz, M.; Kohler, C.W.; Burkhardt, B.; Szczepanowski, M.; Salaverria, I.; Hummel, M.; Loeffler, M.; Pellissery, S.; Woessmann, W.; et al. Patient age at diagnosis is associated with the molecular characteristics of diffuse large B-cell lymphoma. Blood 2012, 119, 1882–1887. [Google Scholar] [CrossRef]
- Reddy, A.; Zhang, J.; Davis, N.S.; Moffitt, A.B.; Love, C.L.; Waldrop, A.; Leppa, S.; Pasanen, A.; Meriranta, L.; Karjalainen-Lindsberg, M.L.; et al. Genetic and Functional Drivers of Diffuse Large B Cell Lymphoma. Cell 2017, 171, 481–494.e415. [Google Scholar] [CrossRef]
- Li, C.; Li, W.; Xu, G.; You, M.; Wu, W.; Kuang, L. Relationship between the absolute lymphocyte count/absolute monocyte count ratio, soluble interleukin 2 receptor level, serum programmed cell death 1 level, and the prognosis of patients with diffuse large B-cell lymphoma. Ann. Palliat. Med. 2021, 10, 10938–10945. [Google Scholar] [CrossRef]
- Yin, T.; Qi, L.; Zhou, Y.; Kong, F.; Wang, S.; Yu, M.; Li, F. CD5+ diffuse large B-cell lymphoma has heterogeneous clinical features and poor prognosis: A single-center retrospective study in China. J. Int. Med. Res. 2022, 50, 3000605221110075. [Google Scholar] [CrossRef]
- Porrata, L.F.; Ristow, K.; Habermann, T.; Inwards, D.J.; Micallef, I.N.; Markovic, S.N. Predicting survival for diffuse large B-cell lymphoma patients using baseline neutrophil/lymphocyte ratio. Am. J. Hematol. 2010, 85, 896–899. [Google Scholar] [CrossRef] [PubMed]
- Rambaldi, A.; Boschini, C.; Gritti, G.; Delaini, F.; Oldani, E.; Rossi, A.; Barbui, A.M.; Caracciolo, D.; Ladetto, M.; Gueli, A.; et al. The lymphocyte to monocyte ratio improves the IPI-risk definition of diffuse large B-cell lymphoma when rituximab is added to chemotherapy. Am. J. Hematol. 2013, 88, 1062–1067. [Google Scholar] [CrossRef]
- Li, Z.M.; Huang, J.J.; Xia, Y.; Sun, J.; Huang, Y.; Wang, Y.; Zhu, Y.J.; Li, Y.J.; Zhao, W.; Wei, W.X.; et al. Blood lymphocyte-to-monocyte ratio identifies high-risk patients in diffuse large B-cell lymphoma treated with R-CHOP. PLoS ONE 2012, 7, e41658. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | N = 185 (%; 95% CI) |
|---|---|
| Gender | |
| Male | 76 (41.1%; 34.3–48.4%) |
| Female | 109 (58.9%; 51.8–65.9%) |
| Median age (range) | 75 years (70–97 years) |
| Caucasian ethnicity | 142 (76.7%; 69.5–81.8%) |
| ≥1 comorbidity | 117 (63.2%; 56.2–70.1%) |
| Immobilism | 36 (19.5%; 13.7–25.2%) |
| Polypharmacy (≥5 drugs) | 46 (24.8%; 18.6–30.9%) |
| Desnutrition (geriatric BMI < 22) | 52 (28.1%; 21.6–34.5%) |
| Categorization according to KPS | |
| Fit (KPS > 70) | 104 (56.2%; 46.5–65.8%) |
| Unfit (KPS 50–70) | 51 (27.6%; 15.3–39.8%) |
| Frail (KPS < 50) | 30 (16.2%; 2.9–29.5%) |
| B-symptoms | 117 (63.2%; 56.2–70.1%) |
| Bulky disease ≥ 7 cm | 90 (48.6%; 41.4–55.7%) |
| Extranodal involvement | 141 (76.2%; 70.0–82.3%) |
| ≥2 extranodal sites | 69 (37.2%; 30.2–44.1%) |
| BM infiltration | 7 (3.8%; 1.0–6.5%) |
| CNS infiltration | 7 (3.8%; 1.0–6.5%) |
| Advanced-stage III or IV | 134 (72.4%; 66.0–78.7%) |
| Intermediate–high/high-risk IPI | 124 (67.0%; 60.2–73.7%) |
| Intermediate–high/high-risk NCCN-IPI | 163 (88.1%; 83.4–92.7%) |
| LDH ≥ 1.5 × UVN | 48 (25.9%; 19.5–32.2%) |
| Hypoalbuminemia (<3.5 g/dL) | 52 (28.6%; 22.0–35.1%)—N miss = 3 |
| Hypogammaglobulinemia (<1.5 g/dL) | 2 (1.1%; 0.4–1.7% )—N miss = 5 |
| COO according to IHC (Hans algorithm) GCB-like phenotype ABC-like phenotype | N = 109 57 (52.3%; 42.9–61.9%) 52 (47.7%; 38.2–57.2%) |
| R-CHOP-21 (N = 104; 95% CI) | R-MiniCHOP (N = 51; 95% CI) | R-Mini-CHOP of the Elderly (N = 24; 95% CI) | p-Value | |
|---|---|---|---|---|
| Median age | 73 years | 78 years | 83 years | 0.367 * |
| CCI score | 5.5 points | 6.0 points | 6.0 points | 0.998 * |
| LDH ratio > 1.5 | 21 (20.4%; 12.6–28.1%) | 16 (31.4%; 18.6–44.1%) | 7 (29.2%; 11.0–47.3%) | 0.269 ** |
| Albumin < 3.5g/dL | 19 (18.8%; 11.2–26.3%) | 16 (31.4%; 18.6–44.1%) | 13 (54.2%; 34.2–74.2%) | 0.001 ** |
| IPI ≥ 3 | 60 (57.7%; 48.1–67.2%) | 40 (78.4%; 67.0–89.7%) | 19 (79.2%; 62.9–95.4%) | 0.013 ** |
| NCCN-IPI ≥ 3 | 83 (79.8%; 72.0–87.5%) | 50 (98.0%; 94.1–100%) | 24 (100%) | 0.002 ** |
| G3/4 neutropenia | 103 (99.0%; 97.0–100%) | 47 (92.2%; 84.8–99.5%) | 20 (83.3%; 68.3–98.2%) | 0.003 ** |
| Febrile neutropenia | 57 (54.8%; 45.2–64.3%) | 27 (52.9%; 39.1–66.6%) | 12 (50.0%; 29.9–70.1%) | 0.907 ** |
| G3/4 thrombocytopenia | 22 (21.2%; 13.3–29.0%) | 12 (23.5%; 11.8–35.1%) | 9 (37.5%; 18.1–56.9%) | 0.238 ** |
| Therapy interruption | 13 (12.5%; 6.1–18.8%) | 4 (7.8%; 0.4–15.1%) | 3 (12.5%; 6.2–18.8%) | 0.671 ** |
| Mortality during induction regimen | 18 (17.3%; 10.1–24.5%) | 10 (19.6%; 8.6–30.5%) | 6 (25.0%; 7.7–42.2%) | 0.681 ** |
| ORR | 75 (72.1%; 63.4–80.7%) | 36 (70.6%; 58.1–83.0%) | 11 (45.6%; 25.6–65.6%) | 0.040 ** |
| Variable | OS Univariate | OS Multivariate | PFS Univariate | PFS Multivariate |
|---|---|---|---|---|
| Age ≥ 75 years | HR: 2.08, 95% CI: 1.35–3.20, p = 0.001 | HR: 2.22, 95% CI: 1.42–3.47, p = 0.001 | HR: 2.00, 95% CI: 1.33–3.01, p = 0.001 | HR: 2.33, 95% CI: 1.52–3.58, p < 0.001 |
| Non-Caucasian ethnicity | HR: 1.80, 95% CI: 1.14–2.83, p = 0.012 | HR: 1.68, 95% CI: 1.09–2.60, p = 0.020 | ||
| Neurologic comorbidity | HR: 2.37, 95% CI: 1.19–4.72, p = 0.014 | HR: 2.76, 95% CI: 1.38–5.49, p = 0.004 | ||
| LDH > UVN | HR: 1.60, 95% CI: 1.07–2.41, p = 0.023 | HR: 1.48, 95% CI: 1.00–2.17, p = 0.048 | HR: 1.09, 95% CI: 1.00–1.18, p = 0.047 | |
| Leukocytosis | HR: 2.61, 95% CI: 1.59–4.28, p < 0.001 | HR: 2.26, 95% CI: 1.38–3.69, p = 0.001 | ||
| Neutrophilia | HR: 2.32, 95% CI: 1.46–3.67, p < 0.001 | HR: 2.18, 95% CI: 1.23–3.84, p = 0.007 | HR: 2.09, 95% CI: 1.34–3.27, p = 0.001 | HR: 2.25, 95% CI: 1.41–3.59, p = 0.001 |
| Monocytosis | HR: 2.01, 95% CI: 1.17–3.02, p < 0.001 | HR: 1.97, 95% CI: 1.24–2.73, p = 0.007 | ||
| L/M ratio < median | HR: 2.19, 95% CI: 1.32–3.64, p = 0.002 | HR: 1.98, 95% CI: 1.18–3.32, p = 0.010 | HR: 2.04, 95% CI: 1.25–3.33, p = 0.004 | HR: 2.08, 95% CI: 1.25–3.46, p = 0.005 |
| Hypoalbuminemia | HR: 1.59, 95% CI: 1.03–2.46, p = 0.036 | HR: 1.50, 95% CI: 1.08–2.27, p = 0.049 | ||
| Ann Arbor CS III/IV | HR: 2.36, 95% CI: 1.38–4.04, p = 0.002 | HR: 2.36, 95% CI: 1.34–4.13, p = 0.003 | HR: 2.58, 95% CI: 1.53–4.34, p < 0.001 | HR: 2.38, 95% CI: 1.38–4.11, p = 0.002 |
| B-symptoms | HR: 1.89, 95% CI: 1.21–2.93, p = 0.005 | HR: 1.84, 95% CI: 1.21–2.80, p = 0.004 | HR: 1.62, 95% CI: 1.04–2.52, p = 0.032 | |
| ≥2 extranodal sites | HR: 2.73, 95% CI: 1.19–6.26, p = 0.018 | HR: 2.38, 95% CI: 1.04–5.45, p = 0.039 |
| Modality | Trial | Phase | Treatment | N | ORR % | PFS % | OS % |
|---|---|---|---|---|---|---|---|
| Anthracycline full dose | LNH98-5 [32] | 3 | CHOP R-CHOP | 399 | 69 83 | 30 (5y) 54 (5y) | 45 (5y) 58 (5y) |
| RICOVER [34] | 3 | R-CHOP + 2xR R-CHOP + 2xR + RT | 166 | 76 (CR) 78 (CR) | 72 (3y) 73 (3y) | 77 (3y) 78 (3y) | |
| UK NCRI [37] | 3 | R-CHOP14 R-CHOP21 | 604 | 91 91 | 64 (5y) | 69 (5y) | |
| LNH03-6B [35] | 3 | R-CHOP14 R-CHOP21 | 602 | 87 86 | 60 (3y) 62 (3y) | 69 (3y) 72 (3y) | |
| Corazzelli et al., 2011 [38] | 2 | R-COMP14 | 41 | 73 | 77 (4y) | 67 (4y) | |
| Anthracycline dose attenuated | Peyrade et al., 2011 [29] | 2 | R-MiniCHOP of the elderly | 150 | 73 | 47 (2y) | 59 (2y) |
| ANZINTER3 [39] | 3 | R-MiniCEOP* R-CHOP | 224 | 81 87 | 46 (5y) 48 (5y) | 63 (5y) 62 (5y) | |
| Non-anthracycline | Park et al., 2016 [40] | 2 | BR | 23 | 78 | 5.4 months (median) | 10.2 months (median) |
| Fields et al., 2014 [41] | 2 | R-GCVP | 62 | 61.3 | 50 (2y) | 56 (2y) | |
| Qui-Dan et al., 2018 [42] | 2 | R-GEMOX | 60 | 49 | 49 (3y) | 65 (3y) |
| Study | Design | N | Median Age | Stratification | Outcomes |
|---|---|---|---|---|---|
| Tucci et al., 2015 Italy [15] | Prospective | 173 | 77 | Fit 46% Unfit 16% Frail 38% | 2-year OS: Fit: 84% Non-fit 47% |
| Merli et al., 2014 Italy [44] | Prospective | 318 | Fit 72 Frail 78 | Fit 70% Frail 30% | 5-year OS: Fit: 71.5% Frail: 23.8% Whole cohort: 28% |
| Ong et al., 2019 Australia [45] | Retrospective | 205 | 73 | Fit 41% Unfit 21% Frail 38% | 3-year OS: Fit: 82% Unfit: 60% Frail: 53% |
| Spina et al., 2012 Italy [46] | Prospective | 100 | 75 | Fit 55% Unfit 32% Frail 13% | 5-year OS: Whole cohort: 60% |
| Olivieri et al., 2012 Italy [47] | Prospective | 91 | 74 | Fit 59% Unfit 24% Frail 17% | 5-year OS: Whole cohort: 46% 5-year EFS: Whole cohort: 31% |
| Marchesi et al., 2013 Italy [48] | Retrospective | 73 | 78 | Fit 29% Unfit 38% Frail 33% | 2-year OS: Fit: 58.3% Non-fit: 24.3% 2-year PFS: Fit: 47.2% Non-fit 21.6% |
| Lage et al., 2024 Brazil (This study) | Retrospective | 185 | 75 | * Fit 56.2% Unfit 27.6% Frail 16.2% | 5-year OS: Fit: 71.6% Unfit: 57.8% Frail **: 24.1% Whole cohort: 50.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Pádua Covas Lage, L.A.; De Vita, R.N.; de Oliveira Alves, L.B.; Jacomassi, M.D.; Culler, H.F.; Reichert, C.O.; de Freitas, F.A.; Rocha, V.; Siqueira, S.A.C.; de Oliveira Costa, R.; et al. Predictors of Survival, Treatment Modalities, and Clinical Outcomes of Diffuse Large B-Cell Lymphoma in Patients Older Than 70 Years Still an Unmet Medical Need in 2024 Based on Real-World Evidence. Cancers 2024, 16, 1459. https://doi.org/10.3390/cancers16081459
de Pádua Covas Lage LA, De Vita RN, de Oliveira Alves LB, Jacomassi MD, Culler HF, Reichert CO, de Freitas FA, Rocha V, Siqueira SAC, de Oliveira Costa R, et al. Predictors of Survival, Treatment Modalities, and Clinical Outcomes of Diffuse Large B-Cell Lymphoma in Patients Older Than 70 Years Still an Unmet Medical Need in 2024 Based on Real-World Evidence. Cancers. 2024; 16(8):1459. https://doi.org/10.3390/cancers16081459
Chicago/Turabian Stylede Pádua Covas Lage, Luís Alberto, Rita Novello De Vita, Lucas Bassolli de Oliveira Alves, Mayara D’Auria Jacomassi, Hebert Fabrício Culler, Cadiele Oliana Reichert, Fábio Alessandro de Freitas, Vanderson Rocha, Sheila Aparecida Coelho Siqueira, Renata de Oliveira Costa, and et al. 2024. "Predictors of Survival, Treatment Modalities, and Clinical Outcomes of Diffuse Large B-Cell Lymphoma in Patients Older Than 70 Years Still an Unmet Medical Need in 2024 Based on Real-World Evidence" Cancers 16, no. 8: 1459. https://doi.org/10.3390/cancers16081459
APA Stylede Pádua Covas Lage, L. A., De Vita, R. N., de Oliveira Alves, L. B., Jacomassi, M. D., Culler, H. F., Reichert, C. O., de Freitas, F. A., Rocha, V., Siqueira, S. A. C., de Oliveira Costa, R., & Pereira, J. (2024). Predictors of Survival, Treatment Modalities, and Clinical Outcomes of Diffuse Large B-Cell Lymphoma in Patients Older Than 70 Years Still an Unmet Medical Need in 2024 Based on Real-World Evidence. Cancers, 16(8), 1459. https://doi.org/10.3390/cancers16081459