
Specific Combinations of Inflammatory, Angiogenesis and Vascular Integrity Biomarkers Are Associated with Clinical Severity, Coma and Mortality in Beninese Children with Plasmodium Falciparum Malaria

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Blood and Data Collection
2.3. Quantification of Plasma Bioactive Molecules
2.4. Statistical Analysis
3. Results
3.1. Cohort Description
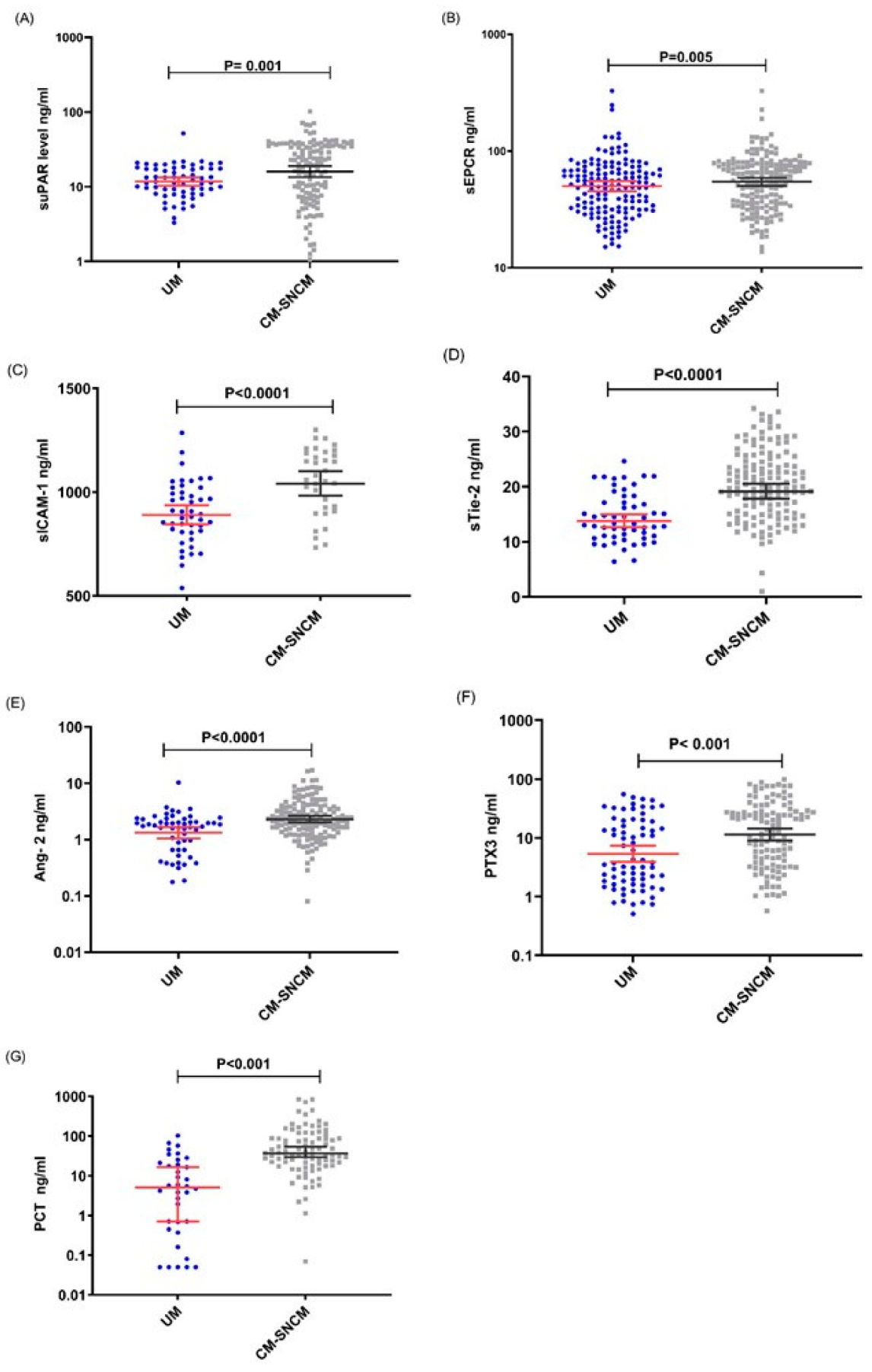
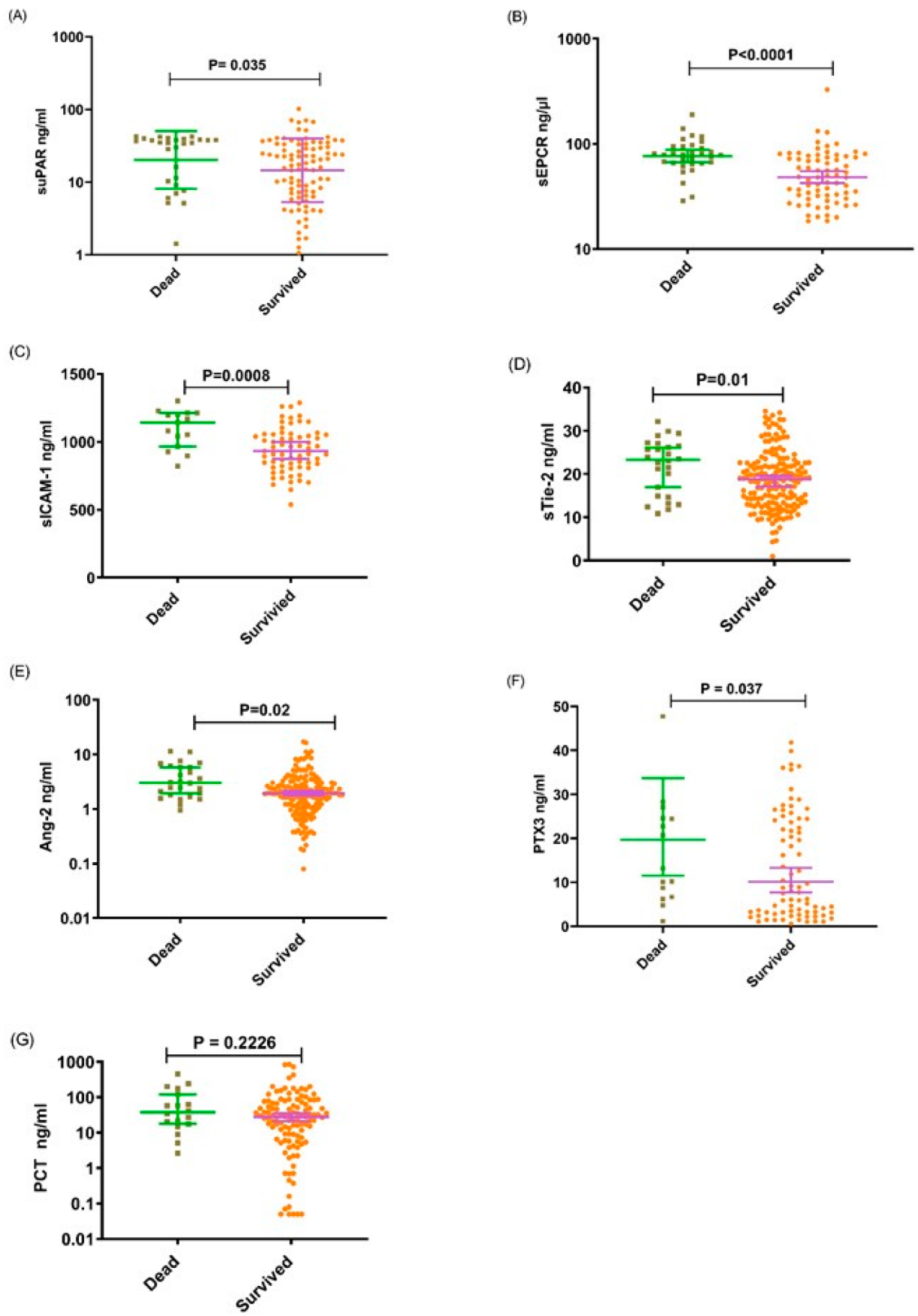
3.2. Immune and Endothelial Activators Are Associated with Malaria-Related Severity, Coma and Mortality
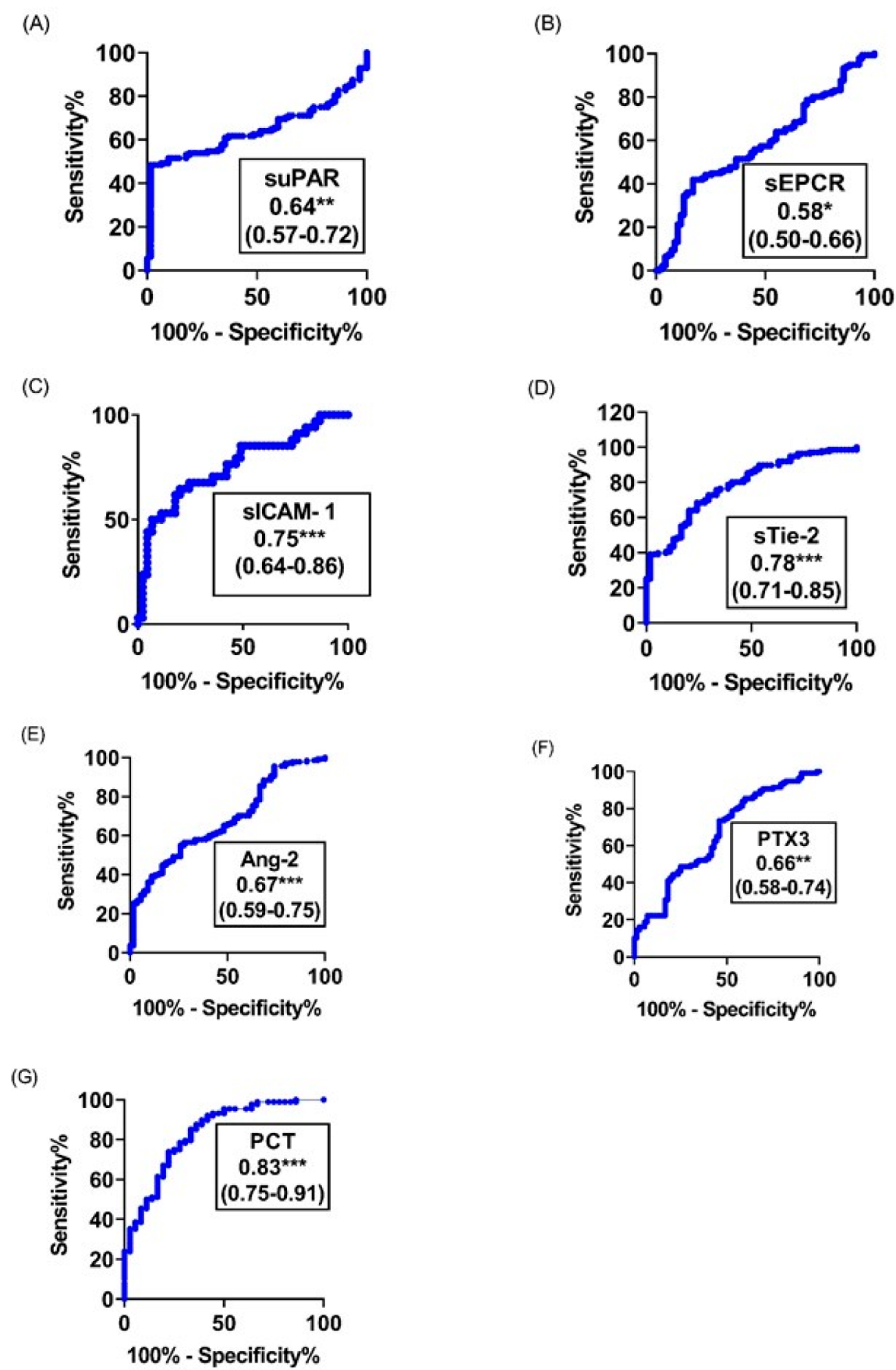
3.3. Predictive Accuracy of Analytes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Ang-2 | angiopoietin 2 |
| AUC | Area Under the ROC Curve |
| BCS | Blantyre Coma Score |
| CM | Cerebral Malaria |
| IFN-γ | Interferon gamma |
| IL-1β | Interleukin 1 beta |
| IL-10 | Interleukin 10 |
| iRBCs | Infected red blood cells |
| MIG | Monokine-induced by IFN-γ |
| ROC | Receiver Operating Characteristic |
| PCT | Procalcitonin |
| P. falciparum | Plasmodium falciparum |
| PTX3 | Pentraxine 3 |
| sEPCR | Soluble Endothelial Protein C Receptor |
| SM | Severe Malaria |
| sICAM-1 | Soluble Intercellular-Adhesion-Molecule-1 |
| suPAR | Soluble urokinase-plasminogen-activator-receptor |
| TGF-β1 | Transforming-growth-factor-beta-1 |
| Tie-2 | tyrosine-kinase-receptor 2 |
| TNF-α | Tumor-Necrosis-Factor-alpha |
| UM | Uncomplicated Malaria |
| vs | Versus |
| WHO | World Health Organization clinical malaria definition criteria |
References
- World Health Organization. World Malaria Report 2021. Licence 2021, CC BY-NC-SA 3.0 IGO. 2021, pp. 18–19. Available online: https://www.who.int/publications/i/item/9789240040496 (accessed on 4 February 2022).
- World Health Organization. World Malaria Report. Geneva 2019 Licence: CC BY-NC-SA 3.0 IGO. 2019. Available online: https://www.who.int/publications/i/item/9789241565721 (accessed on 4 February 2022).
- World Malaria Report; World Health Organization: Geneva, Switzerland, 2019.
- de Kossodo, S.; Grau, G.E. Role of cytokines and adhesion molecules in malaria immunopathology. Stem Cells 1993, 11, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Coban, C.; Lee, M.S.J.; Ishii, K.J. Tissue-specific immunopathology during malaria infection. Nat. Rev. Immunol. 2018, 18, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Moxon, C.A.; Wassmer, S.C.; Milner, D.A., Jr.; Chisala, N.V.; Taylor, T.E.; Seydel, K.B.; Molyneux, M.E.; Faragher, B.; Esmon, C.T.; Downey, C.; et al. Loss of endothelial protein C receptors links coagulation and inflammation to parasite sequestration in cerebral malaria in African children. Blood 2013, 122, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Turner, G.D.; Morrison, H.; Jones, M.; Davis, T.M.; Looareesuwan, S.; Buley, I.D.; Gatter, K.C.; Newbold, C.I.; Pukritayakamee, S.; Nagachinta, B.; et al. An immunohistochemical study of the pathology of fatal malaria. Evidence for widespread endothelial activation and a potential role for intercellular adhesion molecule-1 in cerebral sequestration. Am. J. Pathol. 1994, 145, 1057–1069. [Google Scholar]
- Moussiliou, A.; Alao, M.J.; Denoeud-Ndam, L.; Tahar, R.; Ezimegnon, S.; Sagbo, G.; Amoussou, A.; Luty, A.J.; Deloron, P.; Tuikue Ndam, N. High plasma levels of soluble endothelial protein C receptor are associated with increased mortality among children with cerebral malaria in Benin. J. Infect. Dis. 2015, 211, 1484–1488. [Google Scholar] [CrossRef] [Green Version]
- Fauser, S.; Deininger, M.H.; Kremsner, P.G.; Magdolen, V.; Luther, T.; Meyermann, R.; Schluesener, H.J. Lesion associated expression of urokinase-type plasminogen activator receptor (uPAR, CD87) in human cerebral malaria. J. Neuroimmunol. 2000, 111, 234–240. [Google Scholar] [CrossRef]
- Tahar, R.; Albergaria, C.; Zeghidour, N.; Ngane, V.F.; Basco, L.K.; Roussilhon, C. Plasma levels of eight different mediators and their potential as biomarkers of various clinical malaria conditions in African children. Malar J. 2016, 15, 337. [Google Scholar] [CrossRef]
- Conroy, A.L.; Glover, S.J.; Hawkes, M.; Erdman, L.K.; Seydel, K.B.; Taylor, T.E.; Molyneux, M.E.; Kain, K.C. Angiopoietin-2 levels are associated with retinopathy and predict mortality in Malawian children with cerebral malaria: A retrospective case-control study. Crit. Care Med. 2012, 40, 952–959. [Google Scholar] [CrossRef] [Green Version]
- Akogbeto, M. Entomological study on the malaria transmission in coastal and lagoon areas: The case of a village built on a brackish lake. Ann. Soc. Belg. Med. Trop. 1995, 75, 219–227. [Google Scholar]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- de Bock, C.E.; Wang, Y. Clinical significance of urokinase-type plasminogen activator receptor (uPAR) expression in cancer. Med. Res. Rev. 2004, 24, 13–39. [Google Scholar] [CrossRef]
- Sidenius, N.; Sier, C.F.; Ullum, H.; Pedersen, B.K.; Lepri, A.C.; Blasi, F.; Eugen-Olsen, J. Serum level of soluble urokinase-type plasminogen activator receptor is a strong and independent predictor of survival in human immunodeficiency virus infection. Blood 2000, 96, 4091–4095. [Google Scholar] [CrossRef]
- Wittenhagen, P.; Kronborg, G.; Weis, N.; Nielsen, H.; Obel, N.; Pedersen, S.S.; Eugen-Olsen, J. The plasma level of soluble urokinase receptor is elevated in patients with Streptococcus pneumoniae bacteraemia and predicts mortality. Clin. Microbiol. Infect. 2004, 10, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukudome, K.; Kurosawa, S.; Stearns-Kurosawa, D.J.; He, X.; Rezaie, A.R.; Esmon, C.T. The endothelial cell protein C receptor. Cell surface expression and direct ligand binding by the soluble receptor. J. Biol. Chem. 1996, 271, 17491–17498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundaram, J.; Keshava, S.; Gopalakrishnan, R.; Esmon, C.T.; Pendurthi, U.R.; Rao, L.V. Factor VIIa binding to endothelial cell protein C receptor protects vascular barrier integrity in vivo. J. Thromb. Haemost. 2014, 12, 690–700. [Google Scholar] [CrossRef] [Green Version]
- Turner, L.; Lavstsen, T.; Berger, S.S.; Wang, C.W.; Petersen, J.E.; Avril, M.; Brazier, A.J.; Freeth, J.; Jespersen, J.S.; Nielsen, M.A.; et al. Severe malaria is associated with parasite binding to endothelial protein C receptor. Nature 2013, 498, 502–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, S.J.; Purcell, L.A.; Silver, K.L.; Tran, V.; Crowley, V.; Hawkes, M.; Conroy, A.L.; Opoka, R.O.; Hay, J.G.; Quaggin, S.E.; et al. Dysregulation of angiopoietin-1 plays a mechanistic role in the pathogenesis of cerebral malaria. Sci. Transl. Med. 2016, 8, 358ra128. [Google Scholar] [CrossRef]
- Prapansilp, P.; Medana, I.; Mai, N.T.; Day, N.P.; Phu, N.H.; Yeo, T.W.; Hien, T.T.; White, N.J.; Anstey, N.M.; Turner, G.D. A clinicopathological correlation of the expression of the angiopoietin-Tie-2 receptor pathway in the brain of adults with Plasmodium falciparum malaria. Malar J. 2013, 12, 50. [Google Scholar] [CrossRef] [Green Version]
- Fiedler, U.; Reiss, Y.; Scharpfenecker, M.; Grunow, V.; Koidl, S.; Thurston, G.; Gale, N.W.; Witzenrath, M.; Rosseau, S.; Suttorp, N.; et al. Angiopoietin-2 sensitizes endothelial cells to TNF-alpha and has a crucial role in the induction of inflammation. Nat. Med. 2006, 12, 235–239. [Google Scholar] [CrossRef]
- Alawo, D.O.A.; Tahir, T.A.; Fischer, M.; Bates, D.G.; Amirova, S.R.; Brindle, N.P.J. Regulation of Angiopoietin Signalling by Soluble Tie2 Ectodomain and Engineered Ligand Trap. Sci. Rep. 2017, 7, 3658. [Google Scholar] [CrossRef] [Green Version]
- Mondino, A.; Blasi, F. uPA and uPAR in fibrinolysis, immunity and pathology. Trends Immunol. 2004, 25, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Hodges, G.; Lyngbaek, S.; Selmer, C.; Ahlehoff, O.; Theilade, S.; Sehestedt, T.B.; Abildgaard, U.; Eugen-Olsen, J.; Galloe, A.M.; Hansen, P.R.; et al. SuPAR is associated with death and adverse cardiovascular outcomes in patients with suspected coronary artery disease. Scand. Cardiovasc. J. 2020, 54, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Fernebro, E.; Madsen, R.R.; Ferno, M.; Brunner, N.; Bendahl, P.; Christensen, I.J.; Johnson, A.; Nilbert, M. Prognostic importance of the soluble plasminogen activator receptor, suPAR, in plasma from rectal cancer patients. Eur. J. Cancer 2001, 37, 486–491. [Google Scholar] [CrossRef]
- Perch, M.; Kofoed, P.; Fischer, T.K.; Có, F.; Rombo, L.; Aaby, P.; Eugen-Olsen, J. Serum levels of soluble urokinase plasminogen activator receptor is associated with parasitemia in children with acute Plasmodium falciparum malaria infection. Parasite Immunol. 2004, 26, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, N.; Mihalcioiu, C.; Rabbani, S.A. Multifaceted Role of the Urokinase-Type Plasminogen Activator (uPA) and Its Receptor (uPAR): Diagnostic, Prognostic, and Therapeutic Applications. Front. Oncol. 2018, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Rovina, N.; Akinosoglou, K.; Eugen-Olsen, J.; Hayek, S.; Reiser, J.; Giamarellos-Bourboulis, E.J. Soluble urokinase plasminogen activator receptor (suPAR) as an early predictor of severe respiratory failure in patients with COVID-19 pneumonia. Crit. Care 2020, 24, 187. [Google Scholar] [CrossRef]
- Song, S.; Jia, Q.; Chen, X.; Lei, Z.; He, X.; Leng, Z.; Chen, S. Serum suPAR associated with disease severity and mortality in elderly patients with community-acquired pneumonia. Scand. J. Clin. Lab. Investig. 2020, 80, 515–522. [Google Scholar] [CrossRef]
- Chiwakata, C.B.; Manegold, C.; Bonicke, L.; Waase, I.; Julch, C.; Dietrich, M. Procalcitonin as a parameter of disease severity and risk of mortality in patients with Plasmodium falciparum malaria. J. Infect. Dis. 2001, 183, 1161–1164. [Google Scholar] [CrossRef]
- Braun, N.; Marfo, Y.; Von Gartner, C.; Burchard, G.D.; Zipfel, P.F.; Browne, N.E.; Fleischer, B.; Broker, B.M. CTLA-4 positive T cells in contrast to procalcitonin plasma levels discriminate between severe and uncomplicated Plasmodium falciparum malaria in Ghanaian children. Trop. Med. Int. Health 2003, 8, 1018–1024. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: A patient level meta-analysis. Lancet Infect. Dis. 2018, 18, 95–107. [Google Scholar] [CrossRef] [Green Version]
- Carabias, C.S.; Gomez, P.A.; Panero, I.; Eiriz, C.; Castano-Leon, A.M.; Egea, J.; Lagares, A.; i+12 Neurotraumatology Group, C. Chitinase-3-Like Protein 1, Serum Amyloid A1, C-Reactive Protein, and Procalcitonin Are Promising Biomarkers for Intracranial Severity Assessment of Traumatic Brain Injury: Relationship with Glasgow Coma Scale and Computed Tomography Volumetry. World Neurosurg. 2020, 134, e120–e143. [Google Scholar] [CrossRef] [PubMed]
- Jaillon, S.; Bonavita, E.; Gentile, S.; Rubino, M.; Laface, I.; Garlanda, C.; Mantovani, A. The long pentraxin PTX3 as a key component of humoral innate immunity and a candidate diagnostic for inflammatory diseases. Int. Arch. Allergy Immunol. 2014, 165, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Valentino, S.; Gentile, S.; Inforzato, A.; Bottazzi, B.; Garlanda, C. The long pentraxin PTX3: A paradigm for humoral pattern recognition molecules. Ann. N. Y. Acad. Sci. 2013, 1285, 1–14. [Google Scholar] [CrossRef]
- Parente, R.; Sobacchi, C.; Bottazzi, B.; Mantovani, A.; Grcevic, D.; Inforzato, A. The Long Pentraxin PTX3 in Bone Homeostasis and Pathology. Front. Immunol. 2019, 10, 2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rovere, P.; Peri, G.; Fazzini, F.; Bottazzi, B.; Doni, A.; Bondanza, A.; Zimmermann, V.S.; Garlanda, C.; Fascio, U.; Sabbadini, M.G.; et al. The long pentraxin PTX3 binds to apoptotic cells and regulates their clearance by antigen-presenting dendritic cells. Blood 2000, 96, 4300–4306. [Google Scholar] [CrossRef]
- Baruah, P.; Dumitriu, I.E.; Peri, G.; Russo, V.; Mantovani, A.; Manfredi, A.A.; Rovere-Querini, P. The tissue pentraxin PTX3 limits C1q-mediated complement activation and phagocytosis of apoptotic cells by dendritic cells. J. Leukoc. Biol. 2006, 80, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Brunetta, E.; Folci, M.; Bottazzi, B.; De Santis, M.; Gritti, G.; Protti, A.; Mapelli, S.N.; Bonovas, S.; Piovani, D.; Leone, R.; et al. Macrophage expression and prognostic significance of the long pentraxin PTX3 in COVID-19. Nat. Immunol. 2021, 22, 19–24. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severe Cerebral Malaria (CM) (n = 101) | Severe Non-Cerebral Malaria (SNCM) (n = 133) | Uncomplicated Malaria (UM) (n = 105) | p-Value | |
|---|---|---|---|---|
| Age (months), [IQR] | 30 [5–60] | 36 [4–60] | 36 [5–66] | |
| Sex ratio (female/male) | 45/56 | 72/61 | 48/57 | |
| Temperature, median [IQR] | 38.7 [36.3–41.4] | 38,3 [36.5–41.5] | 38.5 [36–40.8] | |
| Parasitaemia (P/μL), median [IQR] | 44,000 [240–196,875] | 65,457 [275–349,650] | 64,533.5 [218–992,000] | |
| Haemoglobin (g/dL), median [IQR] | 5.2 [2.3–12.9] | 1.92 [0.6–12.8] | 9.215 [5–15.1] | <0.0001 |
| Blantyre coma score, median [IQR] | [0–2] | [3–5] | 5 | <0.0001 |
| Severe malaria anemia (%) | 39 (41%) | 53 (39.84%) | 0 | <0.0001 |
| Number of deaths | 29 | 11 | 0 | 0.0005 |
| Severity: CM/SM versus UM | Coma: BCS < 3 versus BCS > 2 among SM and CM Group | Mortality: Survivors versus Dead | ||||
|---|---|---|---|---|---|---|
| Molecules | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| suPAR | 1.06 (1.03.1.09) | <0.001 | 1.04 (1.02.1.07) | <0.001 | 1.03 (1.01.1.05) | 0.014 |
| sEPCR | 1.00 (1.00.1.00) | 0.461 | 1.00 (1.00.1.00) | 0.648 | 1.02(1.0.1.03) | 0.003 |
| sICAM-1 | 1.01 (1.00.1.01) | <0.001 | 1.00 (1.00.1.01) | 0.004 | 1.0 (1.00.1.01) | 0.199 |
| sTie-2 | 1.21 (1.13.1.30) | <0.001 | 1.08 (1.03.1.14) | 0.001 | 1.04 (0.97.1.12) | 0.314 |
| Ang-2 | 1.51 (1.17.1.94) | 0.002 | 1.05 (0.94.1.19) | 0.353 | 1.08 (0.94.1.23) | 0.302 |
| PTX 3 | 1.03 (1.01.1.05) | 0.002 | 1.04 (1.03.1.06) | <0.001 | 1.02 (1.00.1.04) | 0.0453 |
| PCT | 1.04 (1.02.1.07) | <0.001 | 1.00 (1.00.1.00) | 0.975 | 1.00 (1.00.1.00) | 0.75 |
| Severity | Coma | Death |
|---|---|---|
| PCT (0.83) (acute phase reactant increased by inflammation) | PTX3 (0.78) (inflammation-angiogenesis regulator) | sEPCR (0.77) (increased by inflammation) |
| sTie-2 (0.78) (angiogenesis control) | sICAM-1 (0.71) (inflammation, tissue damage) | sICAM-1 (0.77) (inflammation, tissue damage) |
| sICAM-1 (0.75) (inflammation, tissue damage) | suPAR (0.66) (inflammation-angiogenesis) | Ang-2 (0.68) (angiogenesis activator) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tornyigah, B.; Blankson, S.O.; Adamou, R.; Moussiliou, A.; Rietmeyer, L.; Tettey, P.; Dikroh, L.; Addo, B.; Lamptey, H.; Alao, M.J.; et al. Specific Combinations of Inflammatory, Angiogenesis and Vascular Integrity Biomarkers Are Associated with Clinical Severity, Coma and Mortality in Beninese Children with Plasmodium Falciparum Malaria. Diagnostics 2022, 12, 524. https://doi.org/10.3390/diagnostics12020524
Tornyigah B, Blankson SO, Adamou R, Moussiliou A, Rietmeyer L, Tettey P, Dikroh L, Addo B, Lamptey H, Alao MJ, et al. Specific Combinations of Inflammatory, Angiogenesis and Vascular Integrity Biomarkers Are Associated with Clinical Severity, Coma and Mortality in Beninese Children with Plasmodium Falciparum Malaria. Diagnostics. 2022; 12(2):524. https://doi.org/10.3390/diagnostics12020524
Chicago/Turabian StyleTornyigah, Bernard, Samuel Odarkwei Blankson, Rafiou Adamou, Azizath Moussiliou, Lauriane Rietmeyer, Patrick Tettey, Liliane Dikroh, Bernard Addo, Helena Lamptey, Maroufou J. Alao, and et al. 2022. "Specific Combinations of Inflammatory, Angiogenesis and Vascular Integrity Biomarkers Are Associated with Clinical Severity, Coma and Mortality in Beninese Children with Plasmodium Falciparum Malaria" Diagnostics 12, no. 2: 524. https://doi.org/10.3390/diagnostics12020524