
Effect of the COVID-19 Pandemic on the Psychological Health of Patients Who Underwent Liver Transplantation Due to Hepatocellular Carcinoma

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type, Place, and Duration of Research
2.2. Study Protocol and Ethics Committee Approval
2.3. The Population of the Research and Determination of the Groups
2.4. Inclusion and Exclusion Criteria
2.5. Parameters and Scales Used in the Study
2.5.1. Sociodemographic Characteristics Form
2.5.2. Coronavirus Anxiety Scale-Short Form (CAS-SF)
2.5.3. Depression, Stress and Anxiety Scale-Short Form (DASS-21)
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Anwanwan, D.; Singh, S.K.; Singh, S.; Saikam, V.; Singh, R. Challenges in liver cancer and possible treatment approaches. Biochim. Biophys. Acta (BBA) Rev. Cancer 2019, 1873, 188314. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Center, M.M.; Jemal, A. International Trends in Liver Cancer Incidence Rates. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2362–2368. [Google Scholar] [CrossRef] [PubMed]
- Sia, D.; Villanueva, A.; Friedman, S.L.; Llovet, J.M. Liver Cancer Cell of Origin, Molecular Class, and Effects on Patient Prognosis. Gastroenterology 2017, 152, 745–761. [Google Scholar] [CrossRef]
- Bian, Y.; Guo, D. Targeted Therapy for Hepatocellular Carcinoma: Co-Delivery of Sorafenib and Curcumin Using Lactosylated pH-Responsive Nanoparticles. Drug Des. Dev. Ther. 2020, ume 14, 647–659. [Google Scholar] [CrossRef]
- Grandhi, M.S.; Kim, A.K.; Ronnekleiv-Kelly, S.M.; Kamel, I.R.; Ghasebeh, M.A.; Pawlik, T.M. Hepatocellular carcinoma: From diagnosis to treatment. Surg. Oncol. 2016, 25, 74–85. [Google Scholar] [CrossRef]
- Bertuccio, P.; Turati, F.; Carioli, G.; Rodriguez, T.; La Vecchia, C.; Malvezzi, M.; Negri, E. Global trends and predictions in hepatocellular carcinoma mortality. J. Hepatol. 2017, 67, 302–309. [Google Scholar] [CrossRef]
- Petrick, J.L.; Florio, A.A.; Znaor, A.; Ruggieri, D.; Laversanne, M.; Alvarez, C.S.; Ferlay, J.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in hepatocellular carcinoma incidence, 1978–2012. Int. J. Cancer 2019, 147, 317–330. [Google Scholar] [CrossRef]
- Chen, Q.-F.; Li, W.; Yu, S.C.-H.; Chou, Y.-H.; Rhim, H.; Yang, X.; Shen, L.; Dong, A.; Huang, T.; Huang, J.; et al. Consensus of Minimally Invasive and Multidisciplinary Comprehensive Treatment for Hepatocellular Carcinoma—2020 Guangzhou Recommendations. Front. Oncol. 2021, 11, 621834. [Google Scholar] [CrossRef]
- Wang, K.; Wang, C.; Jiang, H.; Zhang, Y.; Lin, W.; Mo, J.; Jin, C. Combination of Ablation and Immunotherapy for Hepatocellular Carcinoma: Where We Are and Where to Go. Front. Immunol. 2021, 12, 792781. [Google Scholar] [CrossRef]
- Huang, A.; Yang, X.-R.; Chung, W.-Y.; Dennison, A.R.; Zhou, J. Targeted therapy for hepatocellular carcinoma. Signal Transduct. Target. Ther. 2020, 5, 146. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.C.; Kabacam, G.; Vibert, E.; Germani, G.; Petrowsky, H. Current status of liver transplantation in Europe. Int. J. Surg. 2020, 82, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Shingina, A.; Vutien, P.; Uleryk, E.; Shah, P.S.; Renner, E.; Bhat, M.; Tinmouth, J.; Kim, J. Long-term Outcomes of Pediatric Living Versus Deceased Donor Liver Transplantation Recipients: A Systematic Review and Meta-analysis. Liver Transplant. 2021, 28, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Muthiah, M.D.; Zhou, L.; Jumat, H.; Tan, W.X.; Lee, G.H.; Lim, S.G.; Kow, A.; Bonney, G.; Shridhar, I.; et al. Predicting HCC Response to Multikinase Inhibitors With In Vivo Cirrhotic Mouse Model for Personalized Therapy. Cell. Mol. Gastroenterol. Hepatol. 2020, 11, 1313–1325. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.H.; Tan, D.J.H.; Ong, Y.; Lim, W.H.; Ng, C.H.; Tay, P.W.L.; Yong, J.N.; Muthiah, M.D.; Tan, E.X.; Pang, N.Q.; et al. Liver resection versus liver transplantation for hepatocellular carcinoma within Milan criteria: A meta-analysis of 18,421 patients. HepatoBiliary Surg. Nutr. 2022, 11, 78–93. [Google Scholar] [CrossRef]
- Mehta, N.; Yao, F.Y. What Are the Optimal Liver Transplantation Criteria for Hepatocellular Carcinoma? Clin. Liver Dis. 2019, 13, 20–25. [Google Scholar] [CrossRef]
- El Kassas, M.; Alboraie, M.; Al Balakosy, A.; Abdeen, N.; Afify, S.; Abdalgaber, M.; Sherief, A.F.; Madkour, A.; Ahmed, M.A.; Eltabbakh, M.; et al. Liver transplantation in the era of COVID-19. Arab. J. Gastroenterol. 2020, 21, 69–75. [Google Scholar] [CrossRef]
- Haybar, H.; Kazemnia, K.; Rahim, F. Underlying Chronic Disease and COVID-19 Infection: A State-of-the-Art Review. Jundishapur. J. Chronic Dis. Care 2020, 9, e103452. [Google Scholar] [CrossRef]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Golfieri, L.; Gitto, S.; Vukotic, R.; Andreone, P.; Marra, F.; Morelli, M.C.; Cescon, M.; Grandi, S. Impact of psychosocial status on liver transplant process. Ann. Hepatol. 2019, 18, 804–809. [Google Scholar] [CrossRef]
- Yıldız, E. The Relationship Between Anxiety and Intolerance of Uncertainty Levels in Individuals Who Received Liver Transplant: A Descriptive Cross-Sectional Study. Clin. Nurs. Res. 2020, 30, 548–557. [Google Scholar] [CrossRef]
- Varshney, M.; Choudhury, A.; Sahoo, B.; Pamecha, V.; Sinha, P.; Patil, N.; Mohapatra, N.; Sharma, V.; Kumar, R. Impact of COVID-19 pandemic on quality of life and psychosocial difficulties among liver transplant recipients. J. Fam. Med. Prim. Care 2022, 11, 744. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 52, 3750–3752. [Google Scholar] [CrossRef]
- Ikiışık, H.; Sezerol, M.A.; Taşçı, Y.; Maral, I. COVID-19 vaccine hesitancy: A community-based research in Turkey. Int. J. Clin. Pract. 2021, 75, e14336. [Google Scholar] [CrossRef]
- Ikiışık, H.; Sezerol, M.A.; Taşçı, Y.; Maral, I. COVID-19 vaccine hesitancy and related factors among primary healthcare workers in a district of Istanbul: A cross-sectional study from Turkey. Fam. Med. Community Health 2022, 10, e001430. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Lee, S.A. Coronavirus Anxiety Scale: A Brief Mental Health Screener for COVID-19 Related Anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Biçer, I.; Çakmak, C.; Demir, H. Coronavirus Anxiety Scale Short Form: Turkish Validity and Reliability Study. Anadolu Klin. Tıp Bilim. Derg. 2020, 25, 216–225. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef]
- Yilmaz, O.; Boz, H.; Arslan, A. The validity and reliability of depression stress and anxiety scale (DASS 21) Turkish short form. Res. Financ. Econ. Soc. Stud. 2017, 2, 78–91. [Google Scholar]
- Cohen, J. The earth is round (p < 0.05). Am. Psychol. 1994, 49, 997–1003. [Google Scholar] [CrossRef]
- Ripley, B.; Venables, B.; Bates, D.M.; Hornik, K.; Gebhardt, A.; Firth, D.; Ripley, M.B. Package ‘mass’. Cran r 2013, 538, 113–120. [Google Scholar]
- Hlavac, M.; Hlavac, M.M. Package ‘Stargazer’. 2018. Available online: https://sites.google.com/site/marekhlavac/software/stargazer (accessed on 18 February 2023).
- Golfieri, L.; Gitto, S.; Morelli, M.C.; Pinna, A.D.; Grandi, S.; Andreone, P. Impact of hepatitis C virus infection on health-related quality of life before and after liver transplantation: A multidisciplinary point of view. Expert Rev. Anti-Infect. Ther. 2017, 15, 759–765. [Google Scholar] [CrossRef]
- Akbulut, S.; Ozer, A.; Saritas, H.; Yilmaz, S. Factors affecting anxiety, depression, and self-care ability in patients who have undergone liver transplantation. World J. Gastroenterol. 2021, 27, 6967–6984. [Google Scholar] [CrossRef]
- Chao, L.; Liu, C.; Sutthawongwadee, S.; Li, Y.; Lv, W.; Chen, W.; Yu, L.; Zhou, J.; Guo, A.; Li, Z.; et al. Effects of Probiotics on Depressive or Anxiety Variables in Healthy Participants Under Stress Conditions or With a Depressive or Anxiety Diagnosis: A Meta-Analysis of Randomized Controlled Trials. Front. Neurol. 2020, 11, 421. [Google Scholar] [CrossRef]
- Miller, K.; Massie, M.J. Depression and Anxiety. Cancer J. 2006, 12, 388–397. [Google Scholar] [CrossRef]
- Baghernezhad, M.; Mani, A.; Ayoobzadehshirazi, A.; Roozbeh, J.; Zare, M.; Nikeghbalian, S.; Malek-Hosseini, S.A.; Gholam, S.; Bazargan-Hejazi, S. Psychologic Evaluation in Liver Transplantation: Assessment of Psychologic Profile of End-Stage Liver Disease Patients Before and After Transplant. Exp. Clin. Transplant. 2020, 18, 339–344. [Google Scholar] [CrossRef]
- Fidan, C.; Akdur, A.; Kirnap, M.; Selcuk, H.; Yildirim, S.; Moray, G.; Haberal, M. Analysis of Quality of Life, Depression, and Sexual Function in Patients on the Liver Transplant List. Turk. J. Gastroenterol. 2021, 32, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Ni, K.; Li, C.; Qian, Y.; Sun, X.; Zhan, Y.; Zeng, T.; Zhu, S.; Xia, Q.; Feng, W.; Luo, Y. MELD Score Reflects the Mood, Sleep, and Daily Living Ability in Liver Transplantation Candidates: A Descriptive Study. Ann. Transplant. 2020, 25, e926857-1. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, S.; Tamer, M.; Kucukakcali, Z.; Akyuz, M.; Saritas, H.; Bagci, N.; Ciftci, F.; Akbulut, M.S.; Karabulut, E.; Yilmaz, S. Factors affecting anxiety, depression, and stress among patients with hepatocellular carcinoma during COVID-19 pandemic. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.; Noh, O.K.; Oh, Y.-T.; Chun, M.; Kim, L. Psychiatric comorbidities among patients undergoing liver transplantation in South Korea: A nationwide population-based study. Hepatol. Int. 2018, 12, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Essau, C.A.; Lewinsohn, P.M.; Seeley, J.R.; Sasagawa, S. Gender differences in the developmental course of depression. J. Affect. Disord. 2010, 127, 185–190. [Google Scholar] [CrossRef]
- Johnson, D.P.; Whisman, M.A. Gender differences in rumination: A meta-analysis. Pers. Individ. Differ. 2013, 55, 367–374. [Google Scholar] [CrossRef]
- Slavich, G.M.; Sacher, J. Stress, sex hormones, inflammation, and major depressive disorder: Extending Social Signal Transduction Theory of Depression to account for sex differences in mood disorders. Psychopharmacology 2019, 236, 3063–3079. [Google Scholar] [CrossRef]
- Di Marco, F.; Verga, M.; Reggente, M.; Casanova, F.M.; Santus, P.; Blasi, F.; Allegra, L.; Centanni, S. Anxiety and depression in COPD patients: The roles of gender and disease severity. Respir. Med. 2006, 100, 1767–1774. [Google Scholar] [CrossRef] [PubMed]
- Grenier, S.; Payette, M.; Gunther, B.; Askari, S.; Desjardins, F.F.; Raymond, B.; Berbiche, D. Association of age and gender with anxiety disorders in older adults: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2018, 34, 397–407. [Google Scholar] [CrossRef]
- Hajebi, A.; Motevalian, S.A.; Rahimi-Movaghar, A.; Sharifi, V.; Amin-Esmaeili, M.; Radgoodarzi, R.; Hefazi, M. Major anxiety disorders in Iran: Prevalence, sociodemographic correlates and service utilization. BMC Psychiatry 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Siegmann, E.-M.; Müller, H.H.O.; Luecke, C.; Philipsen, A.; Kornhuber, J.; Grömer, T.W. Association of Depression and Anxiety Disorders With Autoimmune Thyroiditis. JAMA Psychiatry 2018, 75, 577–584. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Bendau, A.; Kunas, S.L.; Wyka, S.; Petzold, M.B.; Plag, J.; Asselmann, E.; Ströhle, A. Longitudinal changes of anxiety and depressive symptoms during the COVID-19 pandemic in Germany: The role of pre-existing anxiety, depressive, and other mental disorders. J. Anxiety Disord. 2021, 79, 102377. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.; Van de Velde, S.; Vilagut, G.; de Graaf, R.; O’neill, S.; Florescu, S.; Alonso, J.; Kovess-Masfety, V. Gender differences in mental disorders and suicidality in Europe: Results from a large cross-sectional population-based study. J. Affect. Disord. 2015, 173, 245–254. [Google Scholar] [CrossRef]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2016, 4, 146–158. [Google Scholar] [CrossRef]
- Li, S.H.; Graham, B.M. Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiatry 2016, 4, 73–82. [Google Scholar] [CrossRef]
- Williams, S.E. What are the factors that contribute to parental vaccine-hesitancy and what can we do about it? Hum. Vaccines Immunother. 2014, 10, 2584–2596. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E. Major depression in individuals with chronic medical disorders: Prevalence, correlates and association with health resource utilization, lost productivity and functional disability. Gen. Hosp. Psychiatry 2007, 29, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Afrisham, R.; Paknejad, M.; SoliemaniFar, O.; Sadegh-Nejadi, S.; Meshkani, R.; Ashtary-Larky, D. The Influence of Psychological Stress on the Initiation and Progression of Diabetes and Cancer. Int. J. Endocrinol. Metab. 2019, 17, e67400. [Google Scholar] [CrossRef]
- Rogal, S.S.; Dew, M.A.; Fontes, P.; DiMartini, A.F. Early Treatment of Depressive Symptoms and Long-Term Survival After Liver Transplantation. Am. J. Transplant. 2013, 13, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Annema, C.; Drent, G.; Roodbol, P.F.; Stewart, R.E.; Metselaar, H.J.; van Hoek, B.; Porte, R.J.; Ranchor, A.V. Trajectories of Anxiety and Depression After Liver Transplantation as Related to Outcomes During 2-Year Follow-Up: A Prospective Cohort Study. Psychosom. Med. 2018, 80, 174–183. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | HCC (n = 252) | Non-HCC (n = 252) | ES | p | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Gender | 0.255 | <0.001 * | ||||
| ⠀⠀Female | 39 | 28.9 | 96 | 71.1 | ||
| ⠀⠀Male | 213 | 57.7 | 156 | 42.3 | ||
| Marital Status | 0.209 | 0.009 ** | ||||
| ⠀⠀Married | 237 | 51.9 | 220 | 48.1 | ||
| ⠀⠀Single | 15 | 31.9 | 32 | 68.1 | ||
| Educational Level | 0.154 | 0.018 * | ||||
| ⠀⠀Illiterate a | 29 | 39.2 | 45 | 60.8 | ||
| ⠀⠀Primary school a,b | 106 | 48.6 | 112 | 51.4 | ||
| ⠀⠀Secondary school b | 55 | 65.5 | 29 | 34.5 | ||
| ⠀⠀High school a,b | 43 | 47.3 | 48 | 52.7 | ||
| ⠀⠀University a,b | 19 | 51.4 | 18 | 48.6 | ||
| Monthly Income | 0.236 | <0.001 * | ||||
| ⠀⠀Low a | 33 | 29.5 | 79 | 70.5 | ||
| ⠀⠀Moderate b | 195 | 57.9 | 142 | 42.1 | ||
| ⠀⠀Good b | 24 | 43.6 | 31 | 56.4 | ||
| Place of Residence | 0.198 | <0.001 * | ||||
| ⠀⠀City center a | 175 | 58.1 | 126 | 41.9 | ||
| ⠀⠀District b | 54 | 38.0 | 88 | 62.0 | ||
| ⠀⠀Village b | 23 | 37.7 | 38 | 62.3 | ||
| Smoking | 0.005 | 0.905 * | ||||
| ⠀⠀Yes | 43 | 50.6 | 42 | 49.4 | ||
| ⠀⠀No | 209 | 49.9 | 210 | 50.1 | ||
| Chronic disease | 0.118 | 0.008 * | ||||
| ⠀⠀Yes | 83 | 42.6 | 112 | 57.4 | ||
| ⠀⠀No | 169 | 54.7 | 140 | 45.3 | ||
| Variables | HCC (n = 252) | Non-HCC (n = 252) | ES | p | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Exposure to COVID-19 | 0.028 | 0.530 * | ||||
| ⠀⠀Yes | 63 | 52.5 | 57 | 47.5 | ||
| ⠀⠀No | 189 | 49.2 | 195 | 50.8 | ||
| Need for Hospitalization Due to COVID-19 | 0.098 | 0.620 ** | ||||
| ⠀⠀Yes | 18 | 60.0 | 12 | 40.0 | ||
| ⠀⠀No | 42 | 48.0 | 44 | 51.2 | ||
| Vaccination for COVID-19 | 0.099 | 0.026 * | ||||
| ⠀⠀Yes | 217 | 52.3 | 198 | 47.7 | ||
| ⠀⠀No | 35 | 39.3 | 54 | 60.7 | ||
| COVID-19 Vaccine Doses | 0.187 | 0.001 * | ||||
| ⠀⠀1 dose a | 13 | 27.7 | 34 | 72.3 | ||
| ⠀⠀2 doses a,b | 103 | 52.3 | 94 | 47.7 | ||
| ⠀⠀3 doses a,b | 101 | 59.1 | 70 | 40.9 | ||
| Type of COVID-19 Vaccine | 0.139 | 0.019 * | ||||
| ⠀⠀Sinovac™ a,b | 89 | 48.6 | 94 | 51.4 | ||
| ⠀⠀Biontech™ a,b | 64 | 48.1 | 69 | 51.9 | ||
| ⠀⠀Both a | 64 | 64.6 | 35 | 35.4 | ||
| Postvaccination COVID-19 Exposure | 0.063 | 0.259 ** | ||||
| ⠀⠀Yes | 16 | 42.1 | 22 | 57.9 | ||
| ⠀⠀No | 203 | 53.3 | 179 | 46.7 | ||
| Hesitancy to Vaccinate for COVID-19 | 0.009 | 0.846 * | ||||
| ⠀⠀Yes | 74 | 49.3 | 76 | 50.7 | ||
| ⠀⠀No | 178 | 50.3 | 176 | 49.7 | ||
| Belief in the Efficacy of the COVID-19 Vaccine | 0.128 | 0.016 * | ||||
| ⠀⠀Yes a | 192 | 53.3 | 168 | 46.7 | ||
| ⠀⠀No b | 10 | 29.4 | 24 | 70.6 | ||
| ⠀⠀No idea a,b | 50 | 45.5 | 60 | 54.5 | ||
| Approval of the Mandatory Vaccination for COVID-19 | 0.259 | <0.001 * | ||||
| ⠀⠀Yes a | 139 | 47.4 | 154 | 52.6 | ||
| ⠀⠀No b | 11 | 20.4 | 43 | 79.6 | ||
| ⠀⠀No idea c | 102 | 65.0 | 55 | 35.0 | ||
| Variables [Median (IQR)] | DASS-21 Stress | DASS-21 Anxiety | DASS-21 Depression | DASS-21 Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Med. | IQR | ES | p | Med. | IQR | ES | p | Med. | IQR | ES | p | Med. | IQR | ES | p | |
| Group | 0.281 | 0.002 * | 0.535 | <0.001 * | 0.309 | <0.001 * | 0.398 | <0.001 * | ||||||||
| ⠀⠀HCC | 1.0 | 3.50 | 0.0 | 1.00 | 0.0 | 2.00 | 3.0 | 6.00 | ||||||||
| ⠀⠀Non-HCC | 2.0 | 3.00 | 1.0 | 2.00 | 1.0 | 3.00 | 4.0 | 7.00 | ||||||||
| Gender | 0.188 | 0.032 * | 0.424 | <0.001 * | 0.268 | 0.001 * | 0.284 | 0.001 * | ||||||||
| ⠀⠀Female | 2.0 | 3.00 | 1.0 | 3.00 | 1.0 | 4.00 | 5.0 | 9.00 | ||||||||
| ⠀⠀Male | 2.0 | 4.00 | 0.0 | 1.00 | 0.0 | 2.00 | 3.0 | 5.00 | ||||||||
| Chronic Disease | 0.356 | <0.001 * | 0.307 | <0.001 * | 0.224 | 0.007 * | 0.418 | <0.001 * | ||||||||
| ⠀⠀Yes | 3.0 | 3.00 | 1.0 | 2.00 | 1.0 | 3.00 | 5.0 | 7.00 | ||||||||
| ⠀⠀No | 1.0 | 4.00 | 0.0 | 1.00 | 0.0 | 2.00 | 3.0 | 6.00 | ||||||||
| Exposure to COVID-19 | 0.38 | <0.001 * | 0.196 | 0.017 * | 0.311 | <0.001 * | 0.394 | <0.001 * | ||||||||
| ⠀⠀Yes | 3.0 | 4.50 | 1.0 | 3.00 | 1.0 | 4.00 | 6.0 | 9.50 | ||||||||
| ⠀⠀No | 2.0 | 3.00 | 0.0 | 2.00 | 0.0 | 2.00 | 3.0 | 5.00 | ||||||||
| Vaccination for COVID-19 | 0.235 | 0.008 * | 0.162 | 0.048 * | 0.221 | 0.008 * | 0.266 | 0.003 * | ||||||||
| ⠀⠀Yes | 2.0 | 4.00 | 0.0 | 2.00 | 0.0 | 2.00 | 4.0 | 6.00 | ||||||||
| ⠀⠀No | 3.0 | 3.00 | 1.0 | 3.00 | 1.0 | 4.00 | 4.0 | 9.00 | ||||||||
| Type of Vaccine | 0.306 | 0.003 ** | 0.236 | 0.399 | <0.001 ** | 0.387 | <0.001 ** | |||||||||
| ⠀⠀Sinovac™ | 2.0 a | 4.00 | 0.0 a | 2.00 | 0.021 ** | 1.0 a | 3.00 | 4.0 a | 7.00 | |||||||
| ⠀⠀Biontech™ | 1.0 a | 4.00 | 0.0 ab | 2.00 | 0.0 a | 2.00 | 4.0 a | 6.00 | ||||||||
| ⠀⠀Both * | 1.0 b | 2.00 | 0.0 b | 1.00 | 0.0 b | 1.00 | 2.0 b | 5.00 | ||||||||
| Hesitancy to Vaccinate for COVID-19 | 1.589 | <0.001 * | 1.634 | <0.001 * | 1.492 | 0.004 * | 1.605 | <0.001 * | ||||||||
| ⠀⠀Yes | 3.0 | 3.00 | 1.0 | 3.00 | 1.0 | 3.00 | 5.0 | 8.00 | ||||||||
| ⠀⠀No | 1.0 | 4.00 | 0.0 | 1.00 | 0.0 | 2.00 | 3.0 | 6.00 | ||||||||
| Belief in Efficacy of Vaccination for COVID-19 | 0.171 | <0.001 ** | 0.279 | <0.001 ** | 0.273 | <0.001 ** | 0.238 | <0.001 ** | ||||||||
| ⠀⠀Yes | 1.0 a | 4.00 | 0.0 a | 1.00 | 0.0 a | 2.00 | 3.0 a | 7.00 | ||||||||
| ⠀⠀No | 3.0 b | 3.00 | 1.5 b | 4.00 | 3.0 b | 5.00 | 7.0 b | 11.0 | ||||||||
| ⠀⠀No idea | 2.0 b | 3.00 | 1.0 b | 3.00 | 1.0 c | 3.00 | 4.5 c | 7.00 | ||||||||
| Variables [Median (IQR)] [Mean and SD] | CAS-SF | ES | p | |||
|---|---|---|---|---|---|---|
| Median | IQR | Mean | SD | |||
| Group | ||||||
| ⠀⠀HCC | 0.0 | 0.0 | 0.64 | 1.64 | 0.22 | 0.002 * |
| ⠀⠀Non-HCC | 0.0 | 1.0 | 0.61 | 1.00 | ||
| Gender | 0.246 | 0.001 * | ||||
| ⠀⠀Female | 0.0 | 1.0 | 0.86 | 1.52 | ||
| ⠀⠀Male | 0.0 | 1.0 | 0.55 | 1.30 | ||
| Chronic Disease | 0.214 | 0.003 * | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.77 | 1.38 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.54 | 1.35 | ||
| Exposure to COVID-19 | 0.071 | 0.325 * | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.90 | 1.96 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.55 | 1.11 | ||
| Need for Hospitalization Due to COVID-19 | 0.146 | 0.351 * | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.97 | 2.46 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.87 | 1.77 | ||
| Vaccination for COVID-19 | 0.054 | 0.458 * | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.65 | 1.39 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.56 | 1.25 | ||
| COVID-19 Vaccination Dose | 0.119 | 0.760 ** | ||||
| ⠀⠀1 dose | 0.0 | 1.0 | 0.72 | 1.62 | ||
| ⠀⠀2 doses | 0.0 | 1.0 | 0.64 | 1.36 | ||
| ⠀⠀3 doses | 0.0 | 1.0 | 0.63 | 1.38 | ||
| Type of vaccine | 0.093 | 0.573 ** | ||||
| ⠀⠀Sinovac™ | 0.0 | 1.0 | 0.70 | 1.52 | ||
| ⠀⠀Biontech™ | 0.0 | 1.0 | 0.58 | 1.37 | ||
| ⠀⠀Both | 0.0 | 1.0 | 0.62 | 1.17 | ||
| Postvaccination COVID-19 Exposure | 0.194 | 0.015 * | ||||
| ⠀⠀Yes | 0.0 | 2.0 | 1.16 | 2.07 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.59 | 1.30 | ||
| Hesitancy to Vaccinate for COVID-19 | 0.239 | 0.001 * | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.87 | 1.62 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.53 | 1.24 | ||
| Belief in the Efficacy of COVID-19 Vaccines | 0.234 | 0.013 ** | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.56 | 1.30 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.94 | 1.67 | ||
| ⠀⠀No idea | 0.0 | 1.0 | 0.77 | 1.46 | ||
| Approval of Mandatory Vaccination for COVID-19 | 0.11 | 0.173 ** | ||||
| ⠀⠀Yes | 0.0 | 1.0 | 0.50 | 1.06 | ||
| ⠀⠀No | 0.0 | 1.0 | 0.74 | 1.25 | ||
| ⠀⠀No idea | 0.0 | 1.0 | 0.83 | 1.82 | ||
| DASS-21 Stress | DASS-21 Anxiety | DASS-21 Depression | CAS-SF | DASS-21 Total | ||
|---|---|---|---|---|---|---|
| α | ||||||
| DASS-21 Stress (7 items) | r | 1.000 | 0.823 | |||
| p | ----- | |||||
| α | 0.766 | |||||
| DASS-21 Anxiety (7 items) | r | 0.499 | 1.000 | |||
| p | <0.001 | ----- | ||||
| α | ----- | 0.776 | ||||
| DASS-21 Depression (7 items) | r | 0.504 | 0.513 | 1.000 | ||
| p | <0.001 | <0.001 | ----- | |||
| α | ----- | ----- | 0.859 | |||
| CAS-SF (5 items) | r | 0.148 | 0.292 | 0.325 | 1.000 | |
| p | 0.001 | <0.001 | <0.001 | ----- | ||
| α | ----- | ----- | ----- | 0.783 |
| Variables | Categories | IRR | 95% CI | p |
|---|---|---|---|---|
| Group | [1: HCC; 2: Non-HCC] | 1.26 | 1.01–1.52 | 0.031 |
| Age | - | 1.01 | 1.01–1.03 | 0.008 |
| Gender | [1: Female; 2: Male] | 1.29 | 1.04–1.69 | 0.036 |
| Educational Level | 1.00 | 0.91–1.11 | 0.969 | |
| Monthly Income | [1: Poor; 2: Moderate; 3: Good] | 1.19 | 1.00–1.47 | 0.069 |
| Smoking | [1: Yes; 2: No] | 1.19 | 0.95–1.64 | 0.186 |
| Chronic Disease | [1: Yes; 2: No] | 1.65 | 1.39–2.08 | <0.001 |
| COVID-19 Exposure | [1: Yes; 2: No] | 1.63 | 1.35–2.13 | <0.001 |
| Vaccination for COVID-19 | [1: Yes; 2: No] | 1.50 | 1.11–1.87 | 0.002 |
| Variables | Categories | IRR | 95% CI | p |
|---|---|---|---|---|
| Group | [1: HCC; 2: Non-HCC] | 1.33 | 0.95–2.27 | 0.160 |
| Age | - | 1.00 | 0.98–1.02 | 0.728 |
| Gender | [1: Female; 2: Male] | 1.75 | 1.22–3.22 | 0.014 |
| Educational Level | 1.09 | 0.89–1.29 | 0.348 | |
| Monthly Income | [1: Poor; 2: Moderate; 3: Good] | 1.36 | 1.00–2.12 | 0.090 |
| Smoking | [1: Yes; 2: No] | 1.15 | 0.77–2.38 | 0.579 |
| Chronic Disease | [1: Yes; 2: No] | 1.38 | 1.00–2.27 | 0.107 |
| COVID-19 Exposure | [1: Yes; 2: No] | 1.51 | 1.07–2.63 | 0.048 |
| Vaccination for COVID-19 | [1: Yes; 2: No] | 1.09 | 0.72–1.39 | 0.731 |
| Variables | Importance |
|---|---|
| Exposure to COVID-19 | 0.269 |
| Group | 0.187 |
| Belief in the Efficacy of the COVID-19 Vaccine | 0.179 |
| Hesitancy to Vaccinate for COVID-19 | 0.141 |
| Chronic Disease | 0.127 |
| Vaccination for COVID-19 | 0.071 |
| Gender | 0.026 |
| Variables | Importance |
|---|---|
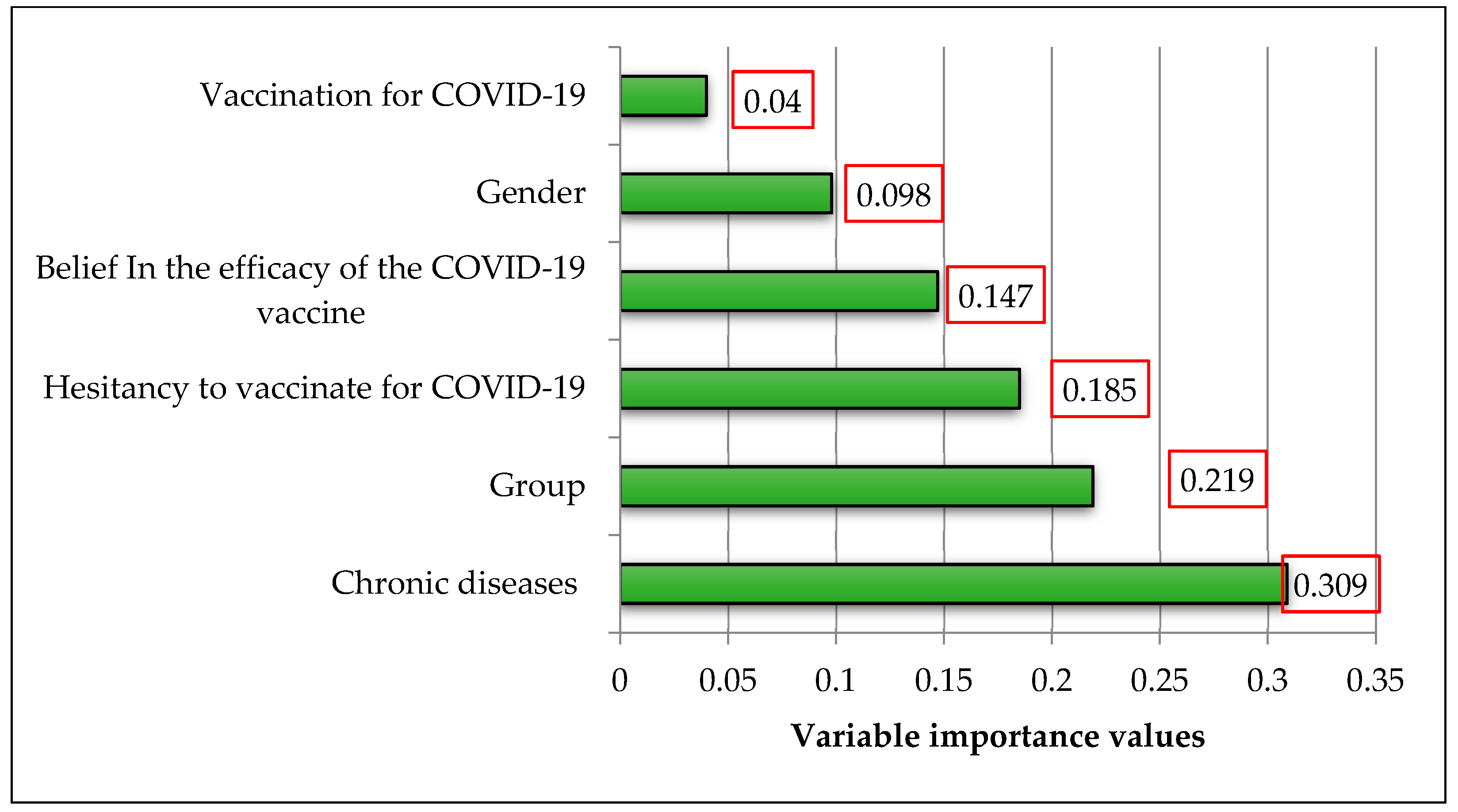
| Chronic Disease | 0.309 |
| Group | 0.219 |
| Hesitancy to Vaccinate for COVID-19 | 0.185 |
| Belief in the Efficacy of the COVID-19 Vaccine | 0.147 |
| Gender | 0.098 |
| Vaccination for COVID-19 | 0.040 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbulut, S.; Kucukakcali, Z.; Saritas, H.; Bozkir, C.; Tamer, M.; Akyuz, M.; Bagci, N.; Unsal, S.; Akbulut, M.S.; Sahin, T.T.; et al. Effect of the COVID-19 Pandemic on the Psychological Health of Patients Who Underwent Liver Transplantation Due to Hepatocellular Carcinoma. Diagnostics 2023, 13, 1410. https://doi.org/10.3390/diagnostics13081410
Akbulut S, Kucukakcali Z, Saritas H, Bozkir C, Tamer M, Akyuz M, Bagci N, Unsal S, Akbulut MS, Sahin TT, et al. Effect of the COVID-19 Pandemic on the Psychological Health of Patients Who Underwent Liver Transplantation Due to Hepatocellular Carcinoma. Diagnostics. 2023; 13(8):1410. https://doi.org/10.3390/diagnostics13081410
Chicago/Turabian StyleAkbulut, Sami, Zeynep Kucukakcali, Hasan Saritas, Cigdem Bozkir, Murat Tamer, Musap Akyuz, Nazlican Bagci, Selver Unsal, Mehmet Serdar Akbulut, Tevfik Tolga Sahin, and et al. 2023. "Effect of the COVID-19 Pandemic on the Psychological Health of Patients Who Underwent Liver Transplantation Due to Hepatocellular Carcinoma" Diagnostics 13, no. 8: 1410. https://doi.org/10.3390/diagnostics13081410