
Venous Thromboembolism Prophylaxis in Gynecologic Oncology: A MITO-MaNGO Survey

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
- Hospitalized medical patients;
- Hospitalized surgical patients, preoperative and postoperative;
- Ambulatory outpatients on systemic therapy.
4.1. Hospitalized Medical Patients
4.2. Hospitalized Surgical Patients
4.3. Ambulatory Outpatients on Systemic Therapy
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lutsey, P.L.; Zakai, N.A. Epidemiology and prevention of venous thromboembolism. Nat. Rev. Cardiol. 2023, 20, 248–262. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.; Hangge, P.; Albadawi, H.; Wallace, A.; Shamoun, F.; Knuttien, M.G.; Naidu, S.; Oklu, R. Deep vein thrombosis: Pathogenesis, diagnosis, and medical management. Cardiovasc. Diagn. Ther. 2017, 7, S276–S284. [Google Scholar] [CrossRef] [PubMed]
- Guntupalli, S.R.; Spinosa, D.; Wethington, S.; Eskander, R.; Khorana, A.A. Prevention of venous thromboembolism in patients with cancer. BMJ 2023, 381, e072715. [Google Scholar] [CrossRef] [PubMed]
- Hohaus, S.; Bartolomei, F.; Cuccaro, A.; Maiolo, E.; Alma, E.; D’Alò, F.; Bellesi, S.; Rossi, E.; Stefano, V.D. Venous Thromboembolism in Lymphoma: Risk Stratification and Antithrombotic Prophylaxis. Cancers 2020, 12, 1291. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Lim, C.S.; Davies, A.H. Venous Thromboembolism in Gynecological Malignancy. Int. J. Gynecol. Cancer 2017, 27, 1970–1978. [Google Scholar] [CrossRef] [PubMed]
- Barber, E.L.; Clarke-Pearson, D.L. The limited utility of currently available venous thromboembolism risk assessment tools in gynecological oncology patients. Am. J. Obstet. Gynecol. 2016, 215, 445.e1–445.e9. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Matsumoto, K.; Tanaka, Y.O.; Akiyama, A.; Nakao, S.; Sakurai, M.; Ochi, H.; Onuki, M.; Minaguchi, T.; Sakurai, H.; et al. Incidence of venous thromboembolism before treatment in cervical cancer and the impact of management on venous thromboembolism after commencement of treatment. Thromb. Res. 2013, 131, e127–e132. [Google Scholar] [CrossRef]
- Rauh-Hain, J.A.; Hariton, E.; Clemmer, J.; Clark, R.M.; Hall, T.; Boruta, D.M.; Schorge, J.O.; Del Carmen, M.G. Incidence and Effects on Mortality of Venous Thromboembolism in Elderly Women with Endometrial Cancer. Obstet. Gynecol. 2015, 125, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, C.C.; Thomas, E.D.; Slaughter, K.N.; Farrell, R.; Ding, K.; Farris, R.E.; Lauer, J.K.; Perry, L.J.; McMeekin, D.S.; Moore, K.N. The survival detriment of venous thromboembolism with epithelial ovarian cancer. Gynecol. Oncol. 2014, 134, 73–77. [Google Scholar] [CrossRef]
- Lavikainen, L.I.; Guyatt, G.H.; Lee, Y.; Couban, R.J.; Luomaranta, A.L.; Sallinen, V.J.; Kalliala, I.E.J.; Karanicolas, P.J.; Cartwright, R.; Aaltonen, R.L.; et al. Systematic reviews of observational studies of Risk of Thrombosis and Bleeding in General and Gynecologic Surgery (ROTBIGGS): Introduction and methodology. Syst. Rev. 2021, 10, 264. [Google Scholar] [CrossRef]
- Ay, C.; Kamphuisen, P.W.; Agnelli, G. Antithrombotic therapy for prophylaxis and treatment of venous thromboembolism in patients with cancer: Review of the literature on current practice and emerging options. ESMO Open 2017, 2, e000188. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Anderson, F.A.; FitzGerald, G.; Decousus, H.; Pini, M.; Chong, B.H.; Zotz, R.B.; Bergmann, J.-F.; Tapson, V.; Froehlich, J.B.; et al. Predictive and Associative Models to Identify Hospitalized Medical Patients at Risk for VTE. Chest 2011, 140, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.J.; Greene, M.T.; Chopra, V.; Bernstein, S.J.; Hofer, T.P.; Flanders, S.A. Assessing the Caprini Score for Risk Assessment of Venous Thromboembolism in Hospitalized Medical Patients. Am. J. Med. 2016, 129, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Greene, M.T.; Spyropoulos, A.C.; Chopra, V.; Grant, P.J.; Kaatz, S.; Bernstein, S.J.; Flanders, S.A. Validation of Risk Assessment Models of Venous Thromboembolism in Hospitalized Medical Patients. Am. J. Med. 2016, 129, 1001.e9–1001.e18. [Google Scholar] [CrossRef] [PubMed]
- Pandor, A.; Tonkins, M.; Goodacre, S.; Sworn, K.; Clowes, M.; Griffin, X.L.; Holland, M.; Hunt, B.J.; De Wit, K.; Horner, D. Risk assessment models for venous thromboembolism in hospitalised adult patients: A systematic review. BMJ Open 2021, 11, e045672. [Google Scholar] [CrossRef] [PubMed]
- Gerotziafas, G.T.; Papageorgiou, L.; Salta, S.; Nikolopoulou, K.; Elalamy, I. Updated clinical models for VTE prediction in hospitalized medical patients. Thromb. Res. 2018, 164, S62–S69. [Google Scholar] [CrossRef] [PubMed]
- Streiff, M.B.; Holmstrom, B.; Angelini, D.; Ashrani, A.; Elshoury, A.; Fanikos, J.; Fertrin, K.Y.; Fogerty, A.E.; Gao, S.; Goldhaber, S.Z.; et al. Cancer-Associated Venous Thromboembolic Disease, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 15, 1181–1201. [Google Scholar] [PubMed]
- Falanga, A.; Ay, C.; Di Nisio, M.; Gerotziafas, G.; Jara-Palomares, L.; Langer, F.; Lecumberri, R.; Mandala, M.; Maraveyas, A.; Pabinger, I.; et al. Venous thromboembolism in cancer patients: ESMO Clinical Practice Guideline. Ann. Oncol. 2023, 34, 452–467. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Zhou, S.; Ma, X.; Jiang, S.; Xu, Y.; You, Y.; Qu, J.; Shang, H.; Lu, Y. Effectiveness of an artificial intelligence clinical assistant decision support system to improve the incidence of hospital-associated venous thromboembolism: A prospective, randomised controlled study. BMJ Open Qual. 2023, 12, e002267. [Google Scholar] [CrossRef]
- Ferroni, P.; Roselli, M.; Zanzotto, F.M.; Guadagni, F. Artificial intelligence for cancer-associated thrombosis risk assessment. Lancet Haematol. 2018, 5, e391. [Google Scholar] [CrossRef]
- Prevention of Venous Thromboembolism in Gynecologic Surgery: ACOG Practice Bulletin Summary, Number 232. Obstet. Gynecol. 2021, 138, 158–161. [CrossRef]
- Romano, F.; Di Lorenzo, G.; Stabile, G.; Mirandola, M.; Restaino, S.; Ianniello, P.; Mirenda, G.; Ricci, G. A Systematic Review of the Guidelines on Venous Thromboembolism Prophylaxis in Gynecologic Oncology. Cancers 2022, 14, 2439. [Google Scholar] [CrossRef] [PubMed]
- Gressel, G.M.; Marcus, J.Z.; Mullen, M.M.; Sinno, A.K. Direct oral anticoagulant use in gynecologic oncology: A Society of Gynecologic Oncology Clinical Practice Statement. Gynecol. Oncol. 2021, 160, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.T.; Maraveyas, A.; Beyer-Westendorf, J.; Lee, A.Y.Y.; Folkerts, K.; Abdelgawwad, K.; De Sanctis, Y.; Fatoba, S.; Bamber, L.; Bach, M.; et al. Patient-reported outcomes associated with changing to rivaroxaban for the treatment of cancer-associated venous thromboembolism—The COSIMO study. Thromb. Res. 2021, 206, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Guntupalli, S.R.; Brennecke, A.; Behbakht, K.; Tayebnejad, A.; Breed, C.A.; Babayan, L.M.; Cheng, G.; Ramzan, A.A.; Wheeler, L.J.; Corr, B.R.; et al. Safety and Efficacy of Apixaban vs Enoxaparin for Preventing Postoperative Venous Thromboembolism in Women Undergoing Surgery for Gynecologic Malignant Neoplasm: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e207410. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.-P.; Xiong, Y.-T.; Fan, Z.-Q.; Yan, L.-J.; Wang, J.-Y.; Gu, Z.-J. Efficacy of intermittent pneumatic compression for venous thromboembolism prophylaxis in patients undergoing gynecologic surgery: A systematic review and meta-analysis. Oncotarget 2017, 8, 20371–20379. [Google Scholar] [CrossRef] [PubMed]
- Amaragiri, S.V.; Lees, T. Elastic compression stockings for prevention of deep vein thrombosis. In Cochrane Database of Systematic Reviews; The Cochrane Collaboration, Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2000; p. CD001484. [Google Scholar]
- Prandoni, P.; Campello, E. Venous Thromboembolism in Cancer Patients Undergoing Chemotherapy: Risk Factors and Prevention. Semin. Thromb Hemost. 2021, 47, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Hasegawa, K.; Yoshino, K.; Murakami, R.; Hisamatsu, T.; Stone, R.L.; Previs, R.A.; Hansen, J.M.; Ikeda, Y.; Miyara, A.; et al. Venous thromboembolism, interleukin-6 and survival outcomes in patients with advanced ovarian clear cell carcinoma. Eur. J. Cancer 2015, 51, 1978–1988. [Google Scholar] [CrossRef] [PubMed]
- Black, K.A.; Ghosh, S.; Singh, N.; Chu, P.; Pin, S. Venous Thromboembolism in Patients Receiving Neoadjuvant Chemotherapy for Advanced Ovarian Cancer and Impact on Survival. J. Obstet. Gynaecol. Can. 2021, 43, 1380–1387. [Google Scholar] [CrossRef]
- Weeks, K.S.; Herbach, E.; McDonald, M.; Charlton, M.; Schweizer, M.L. Meta-Analysis of VTE Risk: Ovarian Cancer Patients by Stage, Histology, Cytoreduction, and Ascites at Diagnosis. Obstet. Gynecol. Int. 2020, 2020, 2374716. [Google Scholar] [CrossRef]
- Khorana, A.A.; Soff, G.A.; Kakkar, A.K.; Vadhan-Raj, S.; Riess, H.; Wun, T.; Streiff, M.B.; Garcia, D.A.; Liebman, H.A.; Belani, C.P.; et al. Rivaroxaban for Thromboprophylaxis in High-Risk Ambulatory Patients with Cancer. N. Engl. J. Med. 2019, 380, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, A.K.; Bauersachs, R.; Falanga, A.; Wong, J.; Kayani, G.; Kahney, A.; Hughes, R.; Levine, M. Fundamental Research in Oncology and Thrombosis 2 (FRONTLINE 2): A Follow-Up Survey. Oncologist 2020, 25, e1091–e1097. [Google Scholar] [CrossRef] [PubMed]
- Forgo, G.; Micieli, E.; Ageno, W.; Castellucci, L.A.; Cesarman-Maus, G.; Ddungu, H.; De Paula, E.V.; Dumantepe, M.; Guillermo Esposito, M.C.; Konstantinides, S.V.; et al. An update on the global use of risk assessment models and thromboprophylaxis in hospitalized patients with medical illnesses from the World Thrombosis Day steering committee: Systematic review and meta-analysis. J. Thromb. Haemost. 2022, 20, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.; Eichorn, A.; Alarcon, M.; McCullagh, L.; McGinn, T.; Spyropoulos, A.C. External Validation of the Risk Assessment Model of the International Medical Prevention Registry on Venous Thromboembolism (IMPROVE) for Medical Patients in a Tertiary Health System. J. Am. Heart Assoc. 2014, 3, e001152. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.A.; Molsberry, R.; Khan, S.S.; Linder, J.A.; Cameron, K.A.; Benson, A. Preventing venous thromboembolism in oncology practice: Use of risk assessment and anticoagulation prophylaxis. Res. Pract. Thromb. Haemost. 2020, 4, 1211–1215. [Google Scholar] [CrossRef] [PubMed]
- Moufarrij, S.; Sassine, D.; Basaran, D.; Jewell, E.L. Assessing the need for venous thromboembolism prophylaxis at the time of neoadjuvant chemotherapy for ovarian cancer: A literature review. Gynecol. Oncol. 2023, 170, 167–171. [Google Scholar] [CrossRef]
- Klaassen, Z.; Wallis, C.J.D.; Lavallée, L.T.; Violette, P.D. Perioperative venous thromboembolism prophylaxis in prostate cancer surgery. World J. Urol. 2020, 38, 593–600. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Answer | Percentage |
|---|---|---|
| 1. Age | ||
| <40 years old | 11 | 22% |
| >40 years old | 39 | 78% |
| 2. Specialty | ||
| Gynecologist | 25 | 50% |
| Oncologist | 25 | 50% |
| 3. Structure | ||
| Private hospital | 5 | 10% |
| Public hospital | 21 | 42% |
| University hospital | 22 | 44% |
| Outpatient setting | 2 | 4% |
| 4. How relevant do you perceive thromboembolic prophylaxis in gynecologic oncology? | ||
| Irrelevant | 1 | 2% |
| Averagely relevant | 8 | 16% |
| Highly relevant | 41 | 83% |
| 5. The center where you work has a standardized protocol for the management of thromboembolic prophylaxis in gynecologic oncology | ||
| No | 0 | 0% |
| Only for surgical prophylaxis | 22 | 44% |
| Only for prophylaxis to patients undergoing chemotherapy | 9 | 18% |
| For all patients | 19 | 38% |
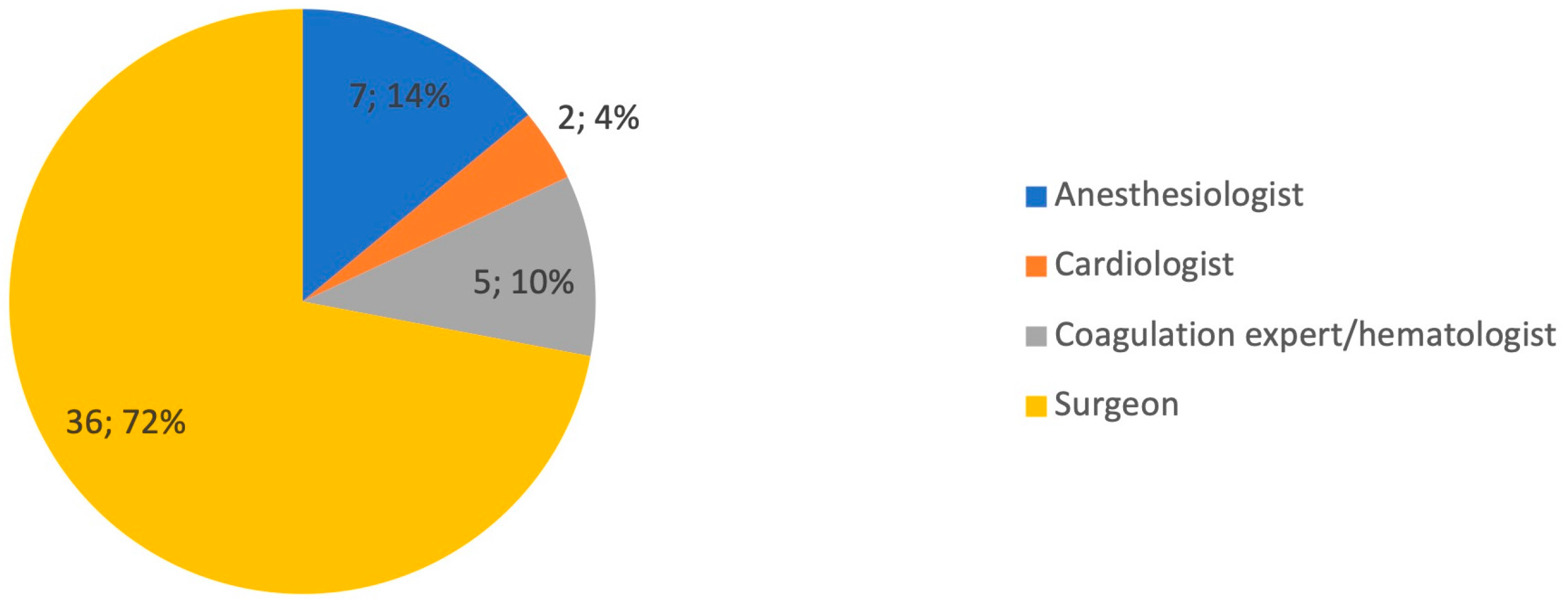
| 6. Who manages thromboembolic prophylaxis in patient undergoing gynecologic oncology surgery? | ||
| Surgeon | 36 | 72% |
| Anesthesiologist | 7 | 14% |
| Cardiologist | 2 | 4% |
| Coagulation expert/hematologist | 5 | 10% |
| 7. Who manages thromboembolic prophylaxis in patient undergoing chemotherapy for gynecologic malignancy? | ||
| Oncologist | 37 | 74% |
| Cardiologist | 3 | 6% |
| Coagulation expert/hematologist | 10 | 20% |
| 8. Do you use a thromboembolic risk assessment scale? | ||
| Yes | 13 | 26% |
| No | 5 | 10% |
| Only in high-risk cases | 32 | 64% |
| 9. If the answer is yes, which evaluation system scale do you prefer? | ||
| Caprini Score | 3 | 6% |
| Khorana Score | 3 | 6% |
| Wells Score | 1 | 2% |
| Regional guidelines | 6 | 12% |
| 10. State your level of knowledge of the following categories of drugs that may be used for thromboembolic prophylaxis | ||
| Direct oral anticoagulants (DOACs) | ||
| Poor | 6 | 12% |
| Medium | 34 | 68% |
| Good | 10 | 20% |
| Low-molecular-weight heparin | ||
| Poor | 1 | 2% |
| Medium | 4 | 8% |
| Good | 45 | 90% |
| Antiplatelets | ||
| Poor | 3 | 6% |
| Medium | 20 | 40% |
| Good | 27 | 54% |
| Dicumarolics | ||
| Poor | 15 | 30% |
| Medium | 20 | 40% |
| Good | 15 | 30% |
| 11. Are you aware of any interactions between drugs used for thromboembolism prophylaxis and antiblastic drugs? | ||
| Yes | 30 | 60% |
| No | 3 | 6% |
| Slightly | 17 | 34% |
| 12. Are you aware of hospital and territory prescribing regulations related to thromboembolic prophylaxis drugs? | ||
| Yes | 34 | 68% |
| No | 2 | 4% |
| Slightly | 14 | 28% |
| 13. Do you think the MITO/MaNGO research groups should further investigate this topic? | ||
| Yes | 50 | 100% |
| No | 0 | 0% |
| 14. Do you think a designated app can help you manage this matter? | ||
| Yes | 49 | 98% |
| No | 1 | 2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mongelli, M.; Lorusso, D.; Zanagnolo, V.; Pignata, S.; Colombo, N.; Cormio, G. Venous Thromboembolism Prophylaxis in Gynecologic Oncology: A MITO-MaNGO Survey. Diagnostics 2024, 14, 1159. https://doi.org/10.3390/diagnostics14111159
Mongelli M, Lorusso D, Zanagnolo V, Pignata S, Colombo N, Cormio G. Venous Thromboembolism Prophylaxis in Gynecologic Oncology: A MITO-MaNGO Survey. Diagnostics. 2024; 14(11):1159. https://doi.org/10.3390/diagnostics14111159
Chicago/Turabian StyleMongelli, Michele, Domenica Lorusso, Vanna Zanagnolo, Sandro Pignata, Nicoletta Colombo, and Gennaro Cormio. 2024. "Venous Thromboembolism Prophylaxis in Gynecologic Oncology: A MITO-MaNGO Survey" Diagnostics 14, no. 11: 1159. https://doi.org/10.3390/diagnostics14111159
APA StyleMongelli, M., Lorusso, D., Zanagnolo, V., Pignata, S., Colombo, N., & Cormio, G. (2024). Venous Thromboembolism Prophylaxis in Gynecologic Oncology: A MITO-MaNGO Survey. Diagnostics, 14(11), 1159. https://doi.org/10.3390/diagnostics14111159