
Development and Validation of an Ultrasonography-Based Machine Learning Model for Predicting Outcomes of Bruxism Treatments

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Outcome Variables
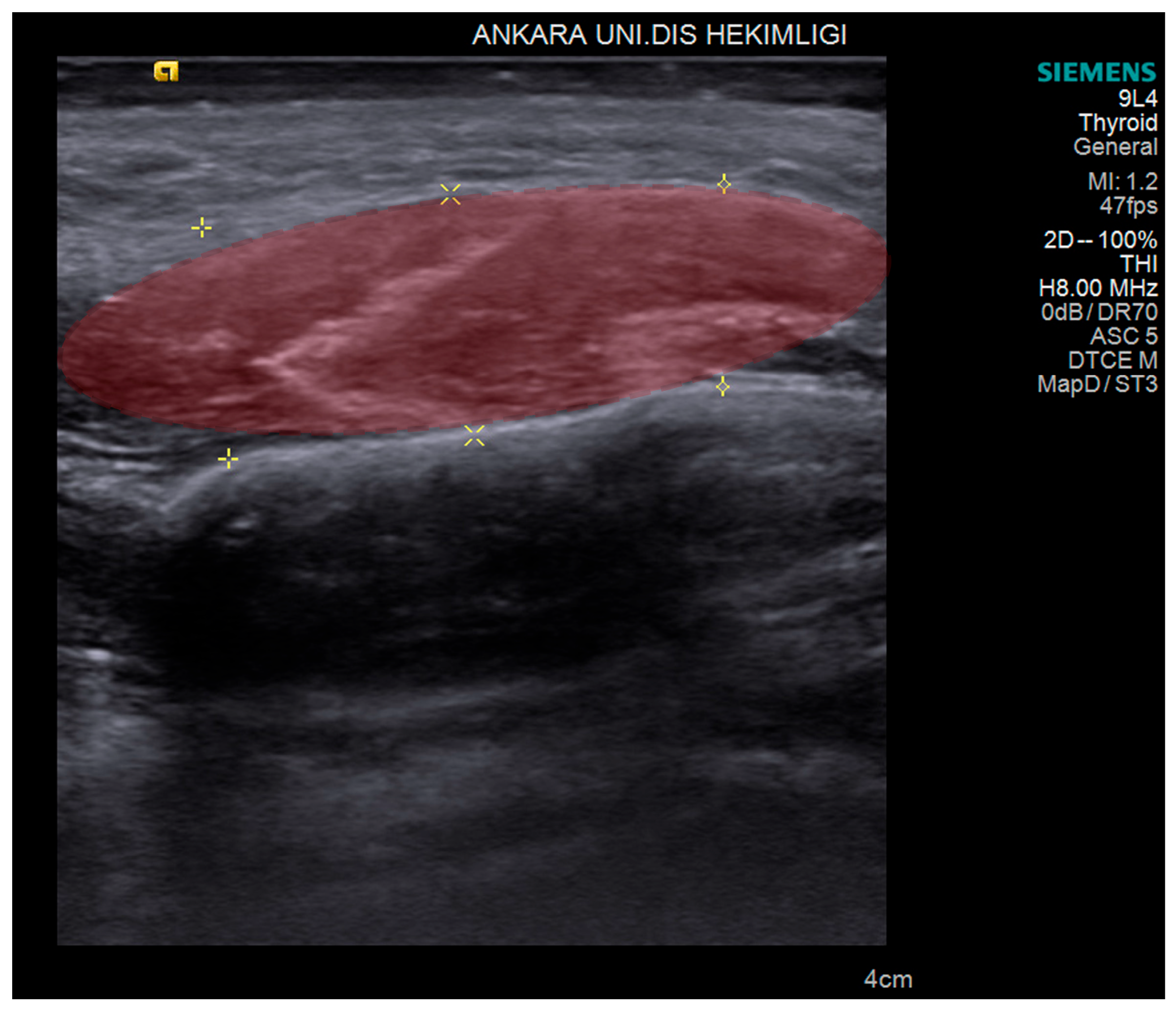
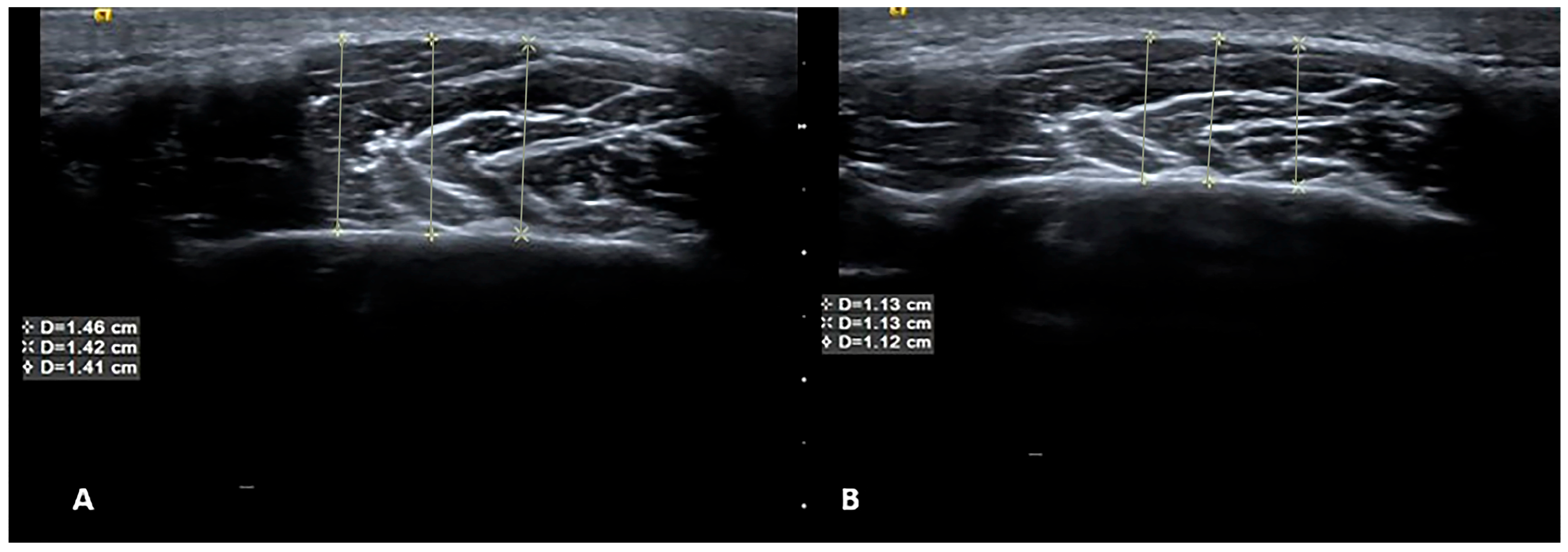
2.2. USG Imaging
2.3. USG Image Segmentation
2.4. Treatment Protocols of Patients
2.5. Radiomics Evaluation
2.6. Feature Extraction
2.7. Consensus Clustering
2.8. Statistical and Machine Learning Analysis
3. Results
3.1. Machine Learning and Radiomics Results
- Ibp-2D_firstorder_variance;
- Exponential_glszm_ZoneVariance;
- Wavelet-LLL_firstorder_variance;
- Wavelet_HLH_glszm_SmallAreaHighGrayLevelEmphasis;
- Wavelet_LLH_glszm_SmalldepedneceHighGrayLevelEmphasis;
- Ibp-2D_firstorder_10percentile.
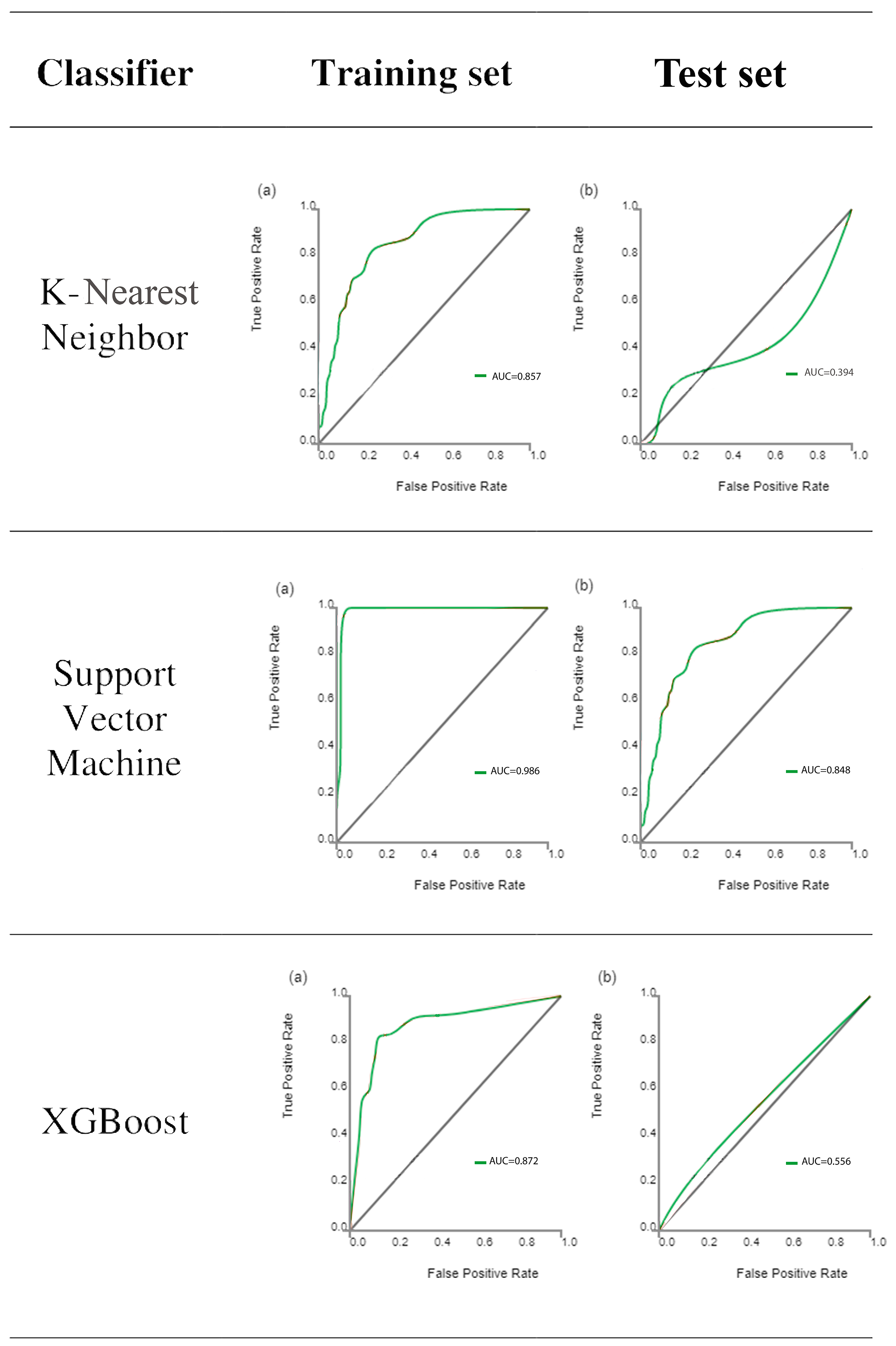
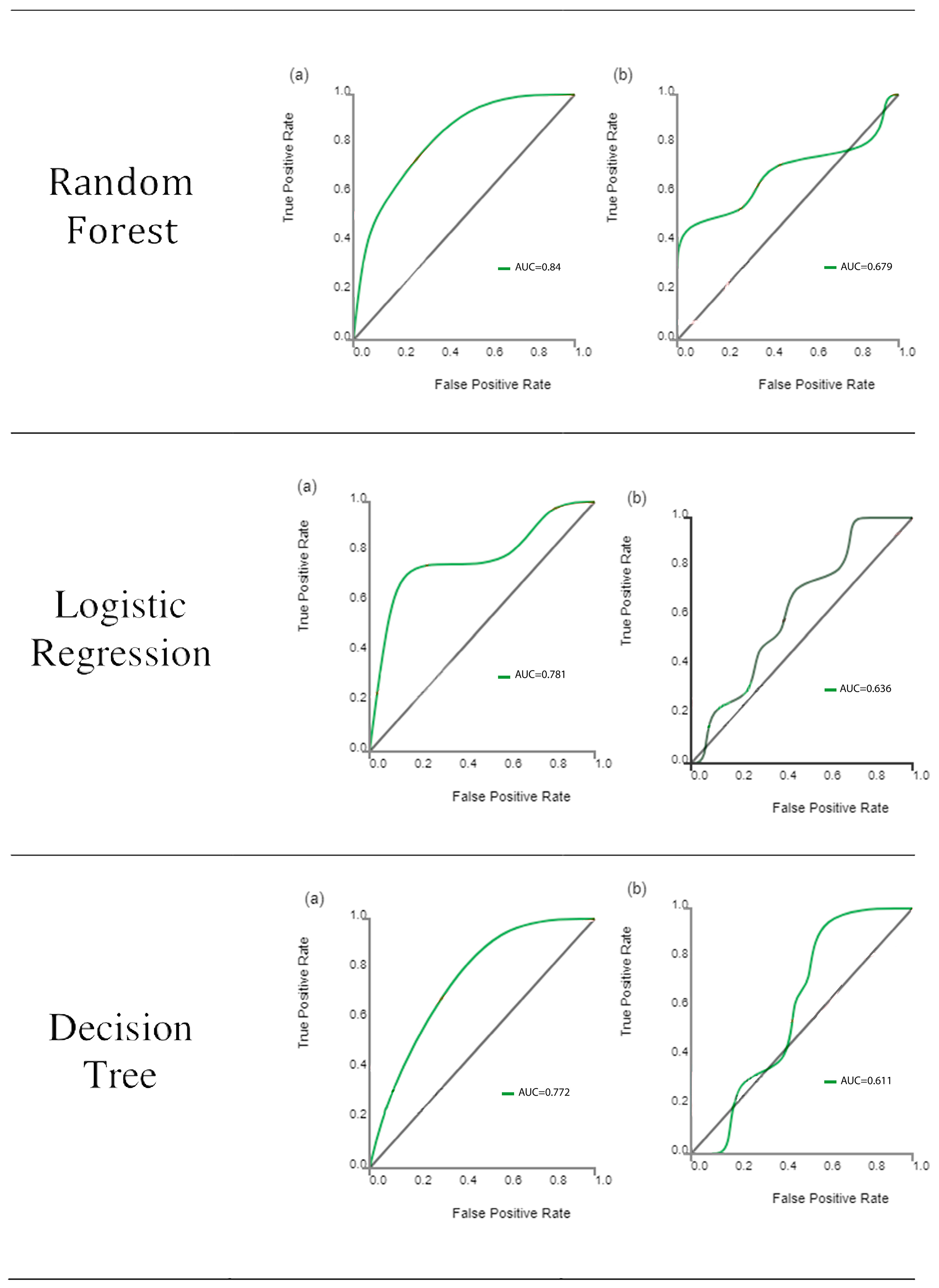
3.2. Diagnostic Performance of Machine Learning Using Six Supervised Learning Classifiers
3.3. Predictive Performance of Models for All Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Silva, A.; Peña-Durán, C.; Tobar-Reyes, J.; Frugone-Zambra, R. Sleep and awake bruxism in adults and its relationship with temporomandibular disorders: A systematic review from 2003 to 2014. Acta Odontol. Scand. 2017, 75, 36–58. [Google Scholar] [CrossRef]
- Yalcin, E.D.; Ozturk, E.M.A. Ultrasonographic evaluation of the effect of splint therapy on masseter muscle and blood flow in patients with bruxism. CRANIO® 2022, 1–9. [Google Scholar] [CrossRef]
- Orhan, K.; Yazici, G.; Kolsuz, M.E.; Kafa, N.; Bayrakdar, I.S.; Çelik, Ö. An artificial intelligence hypothetical approach for masseter muscle segmentation on ultrasonography in patients with bruxism. J. Adv. Oral Res. 2021, 12, 206–213. [Google Scholar] [CrossRef]
- Ariji, Y.; Gotoh, A.; Hiraiwa, Y.; Kise, Y.; Nakayama, M.; Nishiyama, W.; Sakuma, S.; Kurita, K.; Ariji, E. Sonographic elastography for evaluation of masseter muscle hardness. Oral Radiol. 2013, 29, 64–69. [Google Scholar] [CrossRef]
- Brattain, L.J.; Telfer, B.A.; Dhyani, M.; Grajo, J.R.; Samir, A.E. Machine learning for medical ultrasound: Status, methods, and future opportunities. Abdom. Radiol. 2018, 43, 786–799. [Google Scholar] [CrossRef]
- Chartrand, G.; Cheng, P.M.; Vorontsov, E.; Drozdzal, M.; Turcotte, S.; Pal, C.J.; Kadoury, S.; Tang, A. Deep learning: A primer for radiologists. Radiographics 2017, 37, 2113–2131. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.D.; Golan, D.; Hanna, S.A.; Ramachandran, M. Artificial intelligence, machine learning and the evolution of healthcare: A bright future or cause for concern? Bone Jt. Res. 2018, 7, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Shamout, F.; Zhu, T.; Clifton, D.A. Machine learning for clinical outcome prediction. IEEE Rev. Biomed. Eng. 2020, 14, 116–126. [Google Scholar] [CrossRef]
- Bishop, C.M.; Nasrabadi, N.M. Pattern Recognition and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2006; Volume 4. [Google Scholar]
- Lo Casto, A.; Spartivento, G.; Benfante, V.; Di Raimondo, R.; Ali, M.; Di Raimondo, D.; Tuttolomondo, A.; Stefano, A.; Yezzi, A.; Comelli, A.; et al. Artificial Intelligence for Classifying the Relationship between Impacted Third Molar and Mandibular Canal on Panoramic Radiographs. Life 2023, 13, 1441. [Google Scholar] [CrossRef]
- Serindere, G.; Bilgili, E.; Yesil, C.; Ozveren, N. Evaluation of maxillary sinusitis from panoramic radiographs and cone-beam computed tomographic images using a convolutional neural network. Imaging Sci. Dent. 2022, 52, 187. [Google Scholar] [CrossRef]
- Önder, M.; Evli, C.; Türk, E.; Kazan, O.; Bayrakdar, İ.Ş.; Çelik, Ö.; Costa, A.L.F.; Gomes, J.P.P.; Ogawa, C.M.; Jagtap, R. Deep-learning-based automatic segmentation of parotid gland on computed tomography images. Diagnostics 2023, 13, 581. [Google Scholar] [CrossRef]
- Tan, Y.; Schwartz, L.H.; Zhao, B. Segmentation of lung lesions on CT scans using watershed, active contours, and Markov random field. Med. Phys. 2013, 40, 043502. [Google Scholar] [CrossRef]
- Panth, K.M.; Leijenaar, R.T.; Carvalho, S.; Lieuwes, N.G.; Yaromina, A.; Dubois, L.; Lambin, P. Is there a causal relationship between genetic changes and radiomics-based image features? An in vivo preclinical experiment with doxycycline inducible GADD34 tumor cells. Radiother. Oncol. 2015, 116, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Petrella, F.; Buscarino, V.; De Maria, F.; Raimondi, S.; Barberis, M.; Fumagalli, C.; Spitaleri, G.; Rampinelli, C.; De Marinis, F.; et al. CT radiogenomic characterization of EGFR, K-RAS, and ALK mutations in non-small cell lung cancer. Eur. Radiol. 2016, 26, 32–42. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef]
- Shen, J. Log-Linear Regression. In Encyclopedia of Database Systems; Liu, L., ÖZsu, M.T., Eds.; Springer: Boston, MA, USA, 2009; pp. 1660–1661. [Google Scholar]
- Cavallo, P.; Carpinelli, L.; Savarese, G. Perceived stress and bruxism in university students. BMC Res. Notes 2016, 9, 514. [Google Scholar] [CrossRef] [PubMed]
- Nomura, K.; Vitti, M.; Oliveira, A.S.; Chaves, T.C.; Semprini, M.; Siéssere, S.; Hallak, J.E.; Regalo, S.C. Use of the Fonseca’s questionnaire to assess the prevalence and severity of temporomandibular disorders in Brazilian dental undergraduates. Braz. Dent. J. 2007, 18, 163–167. [Google Scholar] [CrossRef]
- Chang, P.H.; Chen, Y.J.; Chang, K.V.; Wu, W.T.; Özçakar, L. Ultrasound measurements of superficial and deep masticatory muscles in various postures: Reliability and influencers. Sci. Rep. 2020, 10, 14357. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Paradowska-Stolarz, A.; Wieckiewicz, W. Psychosocial aspects of bruxism: The most paramount factor influencing teeth grinding. BioMed Res. Int. 2014, 2014, 469187. [Google Scholar] [CrossRef]
- Dharmadhikari, S.; Romito, L.M.; Dzemidzic, M.; Dydak, U.; Xu, J.; Bodkin, C.L.; Manchanda, S.; Byrd, K.E. GABA and glutamate levels in occlusal splint-wearing males with possible bruxism. Arch. Oral Biol. 2015, 60, 1021–1029. [Google Scholar] [CrossRef]
- Coutinho, E.N.; Santos, K.P.R.D.; Ferreira, E.H.B. Association between self-reported sleep bruxism and temporomandibular disorder in undergraduate students from Brazil. CRANIO® 2018, 38, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Volkan-Yazici, M.; Kolsuz, M.E.; Kafa, N.; Yazici, G.; Evli, C.; Orhan, K. Comparison of Kinesio Taping and manual therapy in the treatment of patients with bruxism using shear-wave elastography—A randomised clinical trial. Int. J. Clin. Pract. 2021, 75, e14902. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Burges, C.J. Some notes on applied mathematics for machine learning. In Summer School on Machine Learning; Springer: Berlin/Heidelberg, Germany, 2003; pp. 21–40. [Google Scholar]
- Monti, S.; Tamayo, P.; Mesirov, J.P.; Golub, T.R. Consensus clustering: A resampling-based method for class discovery and visualization of gene expression microarray data. Mach. Learn. 2003, 52, 91–118. [Google Scholar] [CrossRef]
- Power, M.; Fell, G.; Wright, M. Principles for high-quality, high-value testing. BMJ Evid.-Based Med. 2013, 18, 5–10. [Google Scholar] [CrossRef]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and reproducibility of radiomic features: A systematic review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1143–1158. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Pierce, L.A.; Zhang, Y.; Pipavath, S.N.J.; Randolph, T.W.; Lastwika, K.J.; Lampe, P.D.; Houghton, A.M.; Liu, H.; Xia, L.; et al. Comparison of prediction models with radiological semantic features and radiomics in lung cancer diagnosis of the pulmonary nodules: A case-control study. Eur. Radiol. 2019, 29, 6100–6108. [Google Scholar] [CrossRef]
- Hawkins, S.; Wang, H.; Liu, Y.; Garcia, A.; Stringfield, O.; Krewer, H.; Li, Q.; Cherezov, D.; Gatenby, R.A.; Balagurunathan, Y.; et al. Predicting malignant nodules from screening CT scans. J. Thorac. Oncol. 2016, 11, 2120–2128. [Google Scholar] [CrossRef]
- Zhou, H.; Jin, Y.; Dai, L.; Zhang, M.; Qiu, Y.; Wang, K.; Tian, J.; Zheng, J. Differential diagnosis of benign and malignant thyroid nodules using deep learning radiomics of thyroid ultrasound images. Eur. J. Radiol. 2020, 127, 108992. [Google Scholar] [CrossRef]
- Bhatia, K.S.; Lam, A.C.; Pang, S.W.; Wang, D.; Ahuja, A.T. Feasibility study of texture analysis using ultrasound shear wave elastography to predict malignancy in thyroid nodules. Ultrasound Med. Biol. 2016, 42, 1671–1680. [Google Scholar] [CrossRef]
- Park, V.Y.; Lee, E.; Lee, H.S.; Kim, H.J.; Yoon, J.; Son, J.; Song, K.; Moon, H.J.; Yoon, J.H.; Kim, G.R.; et al. Combining radiomics with ultrasound-based risk stratification systems for thyroid nodules: An approach for improving performance. Eur. Radiol. 2021, 31, 2405–2413. [Google Scholar] [CrossRef]
- Zhang, B.; Tian, J.; Pei, S.; Chen, Y.; He, X.; Dong, Y.; Zhang, L.; Mo, X.; Huang, W.; Cong, S.; et al. Machine learning–assisted system for thyroid nodule diagnosis. Thyroid 2019, 29, 858–867. [Google Scholar] [CrossRef]
- Lee, S.E.; Han, K.; Kwak, J.Y.; Lee, E.; Kim, E.K. Radiomics of US texture features in differential diagnosis between triple-negative breast cancer and fibroadenoma. Sci. Rep. 2018, 8, 13546. [Google Scholar] [CrossRef]
- Wijntjes, J.; van Alfen, N. Muscle ultrasound: Present state and future opportunities. Muscle Nerve 2021, 63, 455–466. [Google Scholar] [CrossRef]
- Chen, W.; Li, Y.; Dyer, B.A.; Feng, X.; Rao, S.; Benedict, S.H.; Chen, Q.; Rong, Y. Deep learning vs. atlas-based models for fast auto-segmentation of the masticatory muscles on head and neck CT images. Radiat. Oncol. 2020, 15, 176. [Google Scholar] [CrossRef]
- Keser, G.; Bayrakdar, I.S.; Pekiner, F.N.; Çelik, Ö.; Orhan, K. A Deep Learning Approach for Masseter Muscle Segmentation on Ultrasonography. J. Ultrason. 2022, 22, e204–e208. [Google Scholar] [CrossRef]
- Saleh, A.; Laradji, I.H.; Lammie, C.; Vazquez, D.; Flavell, C.A.; Azghadi, M.R. A Deep Learning Localization Method for Measuring Abdominal Muscle Dimensions in Ultrasound Images. IEEE J. Biomed. Health Inf. 2021, 25, 3865–3873. [Google Scholar] [CrossRef]
- Qin, H.; Wu, Y.Q.; Lin, P.; Gao, R.Z.; Li, X.; Wang, X.R.; Chen, G.; He, Y.; Yang, H. Ultrasound Image-Based Radiomics: An Innovative Method to Identify Primary Tumorous Sources of Liver Metastases. J. Ultrasound Med. 2021, 40, 1229–1244. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.Y.; Jiang, Z.Y.; Fu, T.T.; Wang, Q.M.; Zhu, Y.L.; Dai, M.; Wang, W.P.; Yu, J.H.; Ding, H. Transfer learning radiomics based on multimodal ultrasound imaging for staging liver fibrosis. Eur. Radiol. 2020, 30, 2973–2983. [Google Scholar] [CrossRef]
- D'Souza, J.C.; Sultan, L.R.; Hunt, S.J.; Schultz, S.M.; Brice, A.K.; Wood, A.K.W.; Sehgal, C.M. B-mode ultrasound for the assessment of hepatic fibrosis: A quantitative multiparametric analysis for a radiomics approach. Sci. Rep. 2019, 9, 8708. [Google Scholar] [CrossRef]
- Wang, J.; Guo, L.; Shi, X.; Pan, W.; Bai, Y.; Ai, H. Real-time elastography with a novel quantitative technology for assessment of liver fibrosis in chronic hepatitis B. Eur. J. Radiol. 2012, 81, e31–e36. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiomics Group | Associated Filter | Radiomics Features |
|---|---|---|
| First-order statistics | None | Energy, total energy, entropy, minimum, 10 percentile, 90 percentile, maximum, mean, median, interquartile range, range, mean absolute deviation, robust mean absolute deviation, root mean square, standard deviation, skewness, kurtosis, variance |
| Shape | None | Volume, surface area, surface volume ratio, spherical disproportion, maximum 3D diameter, maximum 2d diameter column, maximum 2d diameter row, elongation |
| Texture features | GLCM | Autocorrelation, average intensity, cluster prominence, cluster shade, cluster tendency, contrast, difference average, difference entropy, difference variance, dissimilarity, entropy, sum average, sum entropy, sum variance, sum squares |
| Texture features | GLSZM | Large area emphasis, gray level non uniformity, size zone non uniformity, gray level variance, zone entropy, high gray level zone emphasis, small area high gray level emphasis, large area high gray level emphasis |
| Texture features | GLRLM | Gray level non uniformity, run length non uniformity, gray level variance, run entropy, high gray level run emphasis, short run high gray level emphasis, long run high level emphasis |
| Classifiers | AUC | 95% CI | Sensitivity | Specificity |
|---|---|---|---|---|
| kNN | 0.857 | 0.68–1.00 | 0.95 | 0.42 |
| SVM | 0.986 | 0.85–1.00 | 0.98 | 0.64 |
| XGBoost | 0.872 | 0.71–1.00 | 0.9 | 0.58 |
| RF | 0.84 | 0.74–0.96 | 0.98 | 0.14 |
| LR | 0.781 | 0.64–0.92 | 0.93 | 0.25 |
| DT | 0.772 | 0.64–0.91 | 0.92 | 0.29 |
| Classifiers | AUC | 95% CI | Sensitivity | Specificity |
|---|---|---|---|---|
| kNN | 0.394 | 0.31–0.48 | 0.91 | 0.31 |
| SVM | 0.848 | 0.58–1.00 | 0.93 | 0.85 |
| XGBoost | 0.556 | 0.58–0.58 | 1.00 | 0.33 |
| RF | 0.679 | 0.68–0.68 | 1.00 | 0 |
| LR | 0.636 | 0.64–0.64 | 1.00 | 0 |
| DT | 0.611 | 0.27–0.97 | 0.91 | 0.33 |
| Indicators | kNN | SVM | XGBoost | RF | LR | DT | |
|---|---|---|---|---|---|---|---|
| 1 | Precision | 0.84 | 0.91 | 0.88 | 0.81 | 0.80 | 0.83 |
| Recall | 0.95 | 0.98 | 0.90 | 0.98 | 0.93 | 0.92 | |
| F1-score | 0.89 | 0.95 | 0.89 | 0.89 | 0.86 | 0.88 | |
| Support | 40 | 40 | 40 | 40 | 40 | 40 | |
| 2 | Precision | 0.71 | 0.90 | 0.64 | 0.67 | 0.50 | 0.50 |
| Recall | 0.42 | 0.64 | 0.58 | 0.14 | 0.25 | 0.29 | |
| F1-score | 0.53 | 0.75 | 0.61 | 0.24 | 0.33 | 0.36 | |
| Support | 12 | 12 | 12 | 14 | 53 | 12 |
| Indicators | kNN | SVM | XGBoost | RF | LR | DT | |
|---|---|---|---|---|---|---|---|
| 1 | Precision | 0.77 | 0.85 | 0.81 | 0.79 | 0.78 | 0.81 |
| Recall | 0.91 | 1.00 | 0.93 | 1.00 | 1.00 | 0.93 | |
| F1-score | 0.83 | 0.92 | 0.87 | 0.88 | 0.88 | 0.87 | |
| Support | 11 | 11 | 11 | 11 | 14 | 11 | |
| 2 | Precision | 0.00 | 1.00 | 0.50 | 0.00 | 0.00 | 0.50 |
| Recall | 0.00 | 0.33 | 0.25 | 0.00 | 0.00 | 0.25 | |
| F1-score | 0.00 | 0.50 | 0.33 | 0.00 | 0.00 | 0.33 | |
| Support | 3 | 3 | 3 | 3 | 4 | 2 | |
| Cumulative | Precision | 0.77 | 0.85 | 0.79 | 0.79 | 0.79 | 0.81 |
| Recall | 0.91 | 1.00 | 0.95 | 0.95 | 0.93 | 0.91 | |
| F1-score | 0.83 | 0.91 | 0.84 | 0.83 | 0.88 | 0.87 | |
| Support | 11 | 11 | 11 | 11 | 11 | 11 |
| Selected Features | SVMR Coefficients | p-Value | |
|---|---|---|---|
| Patient reduction | Clinical model | ||
| Age | −0.582 | ||
| Gender | 0.510 | ||
| Maximum mouth opening | 0.760 | ||
| Pain (Vas score) | 0.620 | ||
| Pain on palpation | −0.120 | 0.016 † | |
| Treatment type (KTMT) | 0.510 | 0.02 † | |
| Treatment type (MT) | 0.510 | 0.03 † | |
| Treatment type (BT-A) | −0.059 | ||
| Sleep quality index | 0.448 | ||
| Radiomic model | |||
| Ibp-2D_firstorder_variance | −0.880 | 0.04 † | |
| Ibp-2D_firstorder_10percentile | −0.330 | 0.02 † | |
| Exponential_glszm_ZoneVariance | 0.442 | ||
| Wavelet_LLH_glszm_SmalldepedneceHighGrayLevelEmphasis | 0.650 | ||
| Wavelet_HLH_glszm_SmallAreaHighGrayLevelEmphasis | 0.152 | 0.03 † | |
| Wavelet-LLL_firstorder_variance | 0.065 | 0.03 † | |
| 0.442 | |||
| Combined model | |||
| Age * | −0.109 | ||
| Gender * | 0.335 | ||
| Treatment type (KTMT) * | 0.079 | 0.021 † | |
| Treatment type (MT) * | 0.218 | 0.02 † | |
| Treatment type (BT-A) * | 0.046 | 0.018 † | |
| Pain on palpation * | −0.110 | 0.02 † | |
| Ibp-2D_firstorder_variance * | 0.280 | ||
| Ibp-2D_firstorder_10percentile * | 0.228 | ||
| Exponential_glszm_ZoneVariance * | 0.091 | 0.03 † | |
| Wavelet_LLH_glszm_SmalldepedneceHighGrayLevelEmphasis * | 0.333 | 0.02 † | |
| Wavelet_HLH_glszm_SmallAreaHighGrayLevelEmphasis * | 0.541 | 0.02 † | |
| Wavelet-LLL_firstorder_variance * | 0.440 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orhan, K.; Yazici, G.; Önder, M.; Evli, C.; Volkan-Yazici, M.; Kolsuz, M.E.; Bağış, N.; Kafa, N.; Gönüldaş, F. Development and Validation of an Ultrasonography-Based Machine Learning Model for Predicting Outcomes of Bruxism Treatments. Diagnostics 2024, 14, 1158. https://doi.org/10.3390/diagnostics14111158
Orhan K, Yazici G, Önder M, Evli C, Volkan-Yazici M, Kolsuz ME, Bağış N, Kafa N, Gönüldaş F. Development and Validation of an Ultrasonography-Based Machine Learning Model for Predicting Outcomes of Bruxism Treatments. Diagnostics. 2024; 14(11):1158. https://doi.org/10.3390/diagnostics14111158
Chicago/Turabian StyleOrhan, Kaan, Gokhan Yazici, Merve Önder, Cengiz Evli, Melek Volkan-Yazici, Mehmet Eray Kolsuz, Nilsun Bağış, Nihan Kafa, and Fehmi Gönüldaş. 2024. "Development and Validation of an Ultrasonography-Based Machine Learning Model for Predicting Outcomes of Bruxism Treatments" Diagnostics 14, no. 11: 1158. https://doi.org/10.3390/diagnostics14111158
APA StyleOrhan, K., Yazici, G., Önder, M., Evli, C., Volkan-Yazici, M., Kolsuz, M. E., Bağış, N., Kafa, N., & Gönüldaş, F. (2024). Development and Validation of an Ultrasonography-Based Machine Learning Model for Predicting Outcomes of Bruxism Treatments. Diagnostics, 14(11), 1158. https://doi.org/10.3390/diagnostics14111158