Abstract
Background: The lack of a clear answer regarding the efficacy of physiotherapy in the treatment of cubital tunnel syndrome (CuTS) has led to attempts to critically assess the scientific studies conducted to date. Materials and Methods: Two databases (MEDLINE via PubMed and PEDro) and Google Scholar were used to search for papers. The inclusion criteria were randomized controlled trials, case series, and case reports that evaluate the effects of physiotherapy in the treatment of patients with CuTS. Results: A total of 18 studies met the eligibility criteria, capturing a total of 425 participants. Seven papers were randomized controlled trials, three more described prospective studies without a control group, and eight papers contained case reports. An analysis of the literature evaluating the effectiveness of various forms of broadly defined physiotherapy indicates that their use can have a beneficial effect in reducing many subjective and objective symptoms and improving function. In the majority of papers included in this review, their authors indicated positive therapeutic effects. Only one randomized controlled trial reported no change following therapy. It can therefore be stated that the results of the research conducted so far are optimistic. However, only 7 of the 18 papers were randomized controlled trials, while 3 were prospective studies, and 8 papers were case studies, in which 23 people with CuTS were studied. Conclusions: The small number of randomized clinical trials and their considerable heterogeneity do not allow firm conclusions to be drawn about the effectiveness of physiotherapy in the conservative treatment of CuTS.
1. Introduction
Cubital tunnel syndrome (CuTS) is the second most common upper limb peripheral neuropathy in clinical practice after carpal tunnel syndrome [1,2]. The incidence of CuTS is estimated at an average of 21–24 cases per 100,000 patients per year [3] (2–6% in the general population) [4]. The typical clinical picture is characterized by sensory abnormalities in the early phase of the condition in the form of paresthesia and mild hypoesthesia, occurring paroxysmally and mainly related to the position of the elbow. Over time, sensory symptoms worsen, and motor disturbances gradually appear (weakness and atrophy of the intrinsic muscles of the hand) [5,6], which can lead to permanent sensory disturbances, paresis, and joint contractures [7]. McGowan identified three stages of CuTS related to the severity of symptoms, ranging from paroxysmal subjective sensory symptoms (Stage 1), significant sensory loss and weakness of the intrinsic muscles of the hand (Stage 2), to severe sensorimotor deficits with muscle atrophy (Stage 3) [8]. Failure to provide immediate and correct clinical diagnosis and appropriate timely treatment can result in significant impairment of hand function [9]. This, in turn, can have a significant impact on activities of daily living, work, and perceptions of overall quality of health, which is not only a medical problem but also a social and economic one [10].
The diagnosis of CuTS is based on the medical history, physical examination, electrophysiological assessment, and ultrasound examination [9]. However, with anatomical differences, a wide spectrum of symptoms, and the need to differentiate this problem from other neuropathies of the ulnar nerve, diagnosis often poses many problems [9]. Forms of CuTS are often divided into primary (idiopathic) and secondary (symptomatic) [11]. In the case of idiopathic CuTS, a specific morphological cause cannot be determined, making a correct diagnosis difficult [11]. In the secondary form, on the other hand, there are multiple causes (trauma, degenerative changes, cysts, ganglions, etc.) [1,12] and multiple sites of compression of the ulnar nerve (arcade of Struthers, the medial intermuscular septum, the medial epicondyle, the cubital tunnel, and the deep flexor-pronator aponeurosis) [13]. Such a variety of causes, sites of compression, and sometimes a lack of a tangible cause makes it significantly more difficult not only to diagnose but also to choose the most optimal form of therapy.
Both conservative and surgical approaches used in the treatment of CuTS [14]. Conservative treatment is recommended in mild to moderate forms of CuTS [6]. This usually includes pharmacological treatment [15,16], immobilization with elbow night splints [17], and education of the patient on how to change their habits at work and activities of daily living, with particular emphasis on avoiding prolonged elbow flexion [16]. Physiotherapy is also often implemented and includes manual therapy with neurodynamic techniques [18,19], short wave diathermy [20], low-level laser therapy [21], extracorporeal shock wave therapy [22], and even dry needling [23]. Unfortunately, as reported by Mezian et al. [9], conservative treatment of CuTS is based more on empirical experience than on a significant amount of high-quality scientific research. Surgical intervention is used in cases of advanced CuTS or when conservative treatment has failed. The most commonly used surgical methods are simple decompression [24], endoscopic techniques [25], medial epicondylectomy [26], or one of the anterior transposition methods: subcutaneous [27], intramuscular [28], or submuscular [29]. However, there are no scientific reports indicating that any of these techniques can produce better results than the others [30,31]. Palmer and Hughs emphasized that, to date, a ‘gold standard’ in the surgical treatment of CuTS has not been developed [1]. Therefore, there is a lack of scientifically supported treatments for CuTS. This concerns both surgical and conservative treatment, including physiotherapeutic management. Few randomized controlled trials have examined the effectiveness of physiotherapy in CuTS [19,20,21] and the results and conclusions fail to unequivocally demonstrate the beneficial effects of the various physiotherapy methods. Other studies are mostly case reports or case series with a low number of patients studied [18,22,23], which have shown an improvement in the patient’s condition but had a low level of reliability (they are not randomized controlled trials) and should therefore be approached with caution. To the best of our knowledge, there are no recommendations for the physiotherapeutic management of CuTS that are supported by strong scientific evidence. The lack of a clear answer regarding the efficacy of physiotherapy in the treatment of CuTS leads to the attempts to critically assess the scientific studies conducted to date on the use of various forms of physiotherapy in the conservative treatment of this neuropathy. This will help to identify areas that need such research and to deepen or extend the scientific research on the possibility of using different forms of physiotherapy in the conservative treatment of CuTS.
2. Materials and Methods
The literature review was conducted in December 2023. Two electronic databases (MEDLINE via PubMed and PEDro) and the Google Scholar search engine were used to search for papers. The search strategy for database papers was based on the use of key phrases and/or abbreviations, taking into account their respective English wording. The following terms were used: cubital tunnel syndrome, CuTS, physiotherapy, physical therapy, PT, electrostimulation, ES, ultrasound, US, magnet therapy, MT, shock wave therapy, RSW, shortwave diathermy, laser, neuromobilization, neurodynamic techniques, neurodynamic treatment, neurodynamic mobilization, nerve gliding exercises, neurodynamics, manual therapy, conservative treatment, and splitting.
Studies that met the following criteria were included in the review: (1) the participant had clinically and/or electrophysiologically diagnosed CuTS, and (2) any form of physical stimulus was used in the study. All papers were accepted regardless of the year of publication. The search was limited to papers published in English.
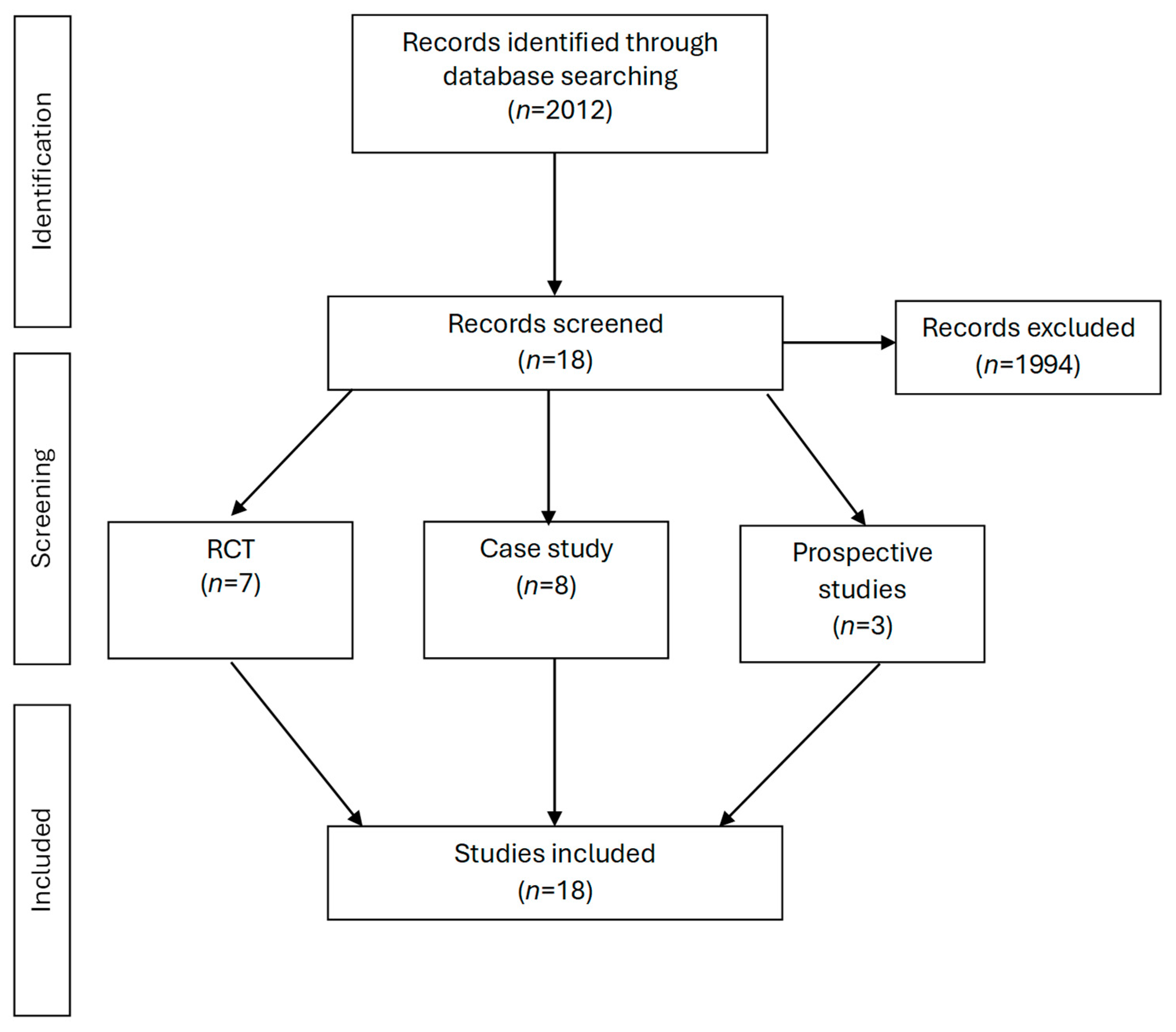
The titles and abstracts of the retrieved papers were analyzed to assess whether they met the inclusion criteria. Those that did not show relevance to the subject area studied were excluded, e.g., those that contain surgical treatment approaches. The bibliographies of the included papers were also analyzed to check whether other papers meeting the criteria had not been omitted (Figure 1).
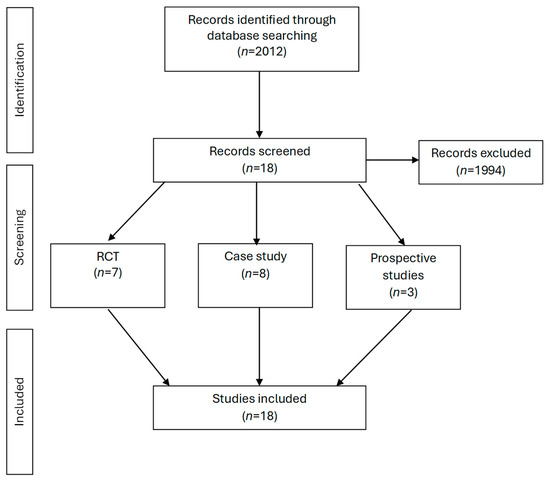
Figure 1.
Flow charts.
3. Results
Eighteen papers met the inclusion criteria [17,18,19,20,21,22,23,32,33,34,35,36,37,38,39,40,41,42]. Seven papers were randomized controlled trials [19,20,21,32,33,40,42] (Table 1), three more described prospective studies without a control group [17,37,39] (Table 2), and eight papers contained case reports [18,22,23,34,35,36,38,41] (Table 3). In six papers, the experiments were based on two comparison groups [20,21,32,33,40,42]; in one paper there were three groups [19]; three had no comparison groups [17,37,39]; and eight contained only case descriptions [18,22,23,34,35,36,38,41]. Participants were examined before the therapy in all the reviewed studies, and immediately after therapy in ten studies [20,21,32,34,35,36,37,38,39,42]. The long-term effects were assessed in thirteen studies [17,18,19,20,21,22,23,33,36,38,39,40,41] and at different follow-up times, ranging from two weeks to twelve months. In two studies, participants were assessed before each therapy session [18,23]. Also, two studies evaluated participants during the study [37,39]. In only one case, the study was double-blinded [20], one study was single-blinded [21], and two studies investigated the placebo effect [20,40]. There is no information in the other studies about their blinding [17,18,19,22,23,32,33,34,35,36,37,38,39,41,42].

Table 1.
Characteristics of randomized clinical trials (RCT).
Table 2.
Characteristics of papers describing prospective studies without a control group.
Table 3.
Characteristics of papers with case reports.
Seventeen papers had participants clinically and/or electrophysiologically diagnosed with CuTS, while one paper did not state how the diagnosis was made [42]. The number of participants ranged from 1 to 77. The age of the subjects was documented in seventeen papers [17,18,19,20,21,22,23,32,33,34,35,36,37,38,40,41,42] and ranged from seventeen to seventy-nine years. The interventions were described in men and women in nine papers [17,19,20,21,23,37,39,40,42], in women in four papers [18,32,34,35], and in men in three papers [33,36,41]. Two papers did not specify the gender of patients receiving treatment [22,38].
3.1. RCT Studies
In the manuscripts describing the randomized controlled trials, the most frequent assessments concerned pain severity (VAS) (five studies) [19,20,21,32,40] and grip strength (five studies) [19,20,21,32,42]. Four studies performed neurophysiological assessment (NCS) [19,21,33,40] while three assessed hand function using the DASH or QuickDASH questionnaires [20,32,40]. Three others used the Tinel’s test for assessment [20,21,32]. Assessment of activity (COMP) [19], neurological signs and symptoms [33], adduction of the little finger [19], pincer grip strength [32], muscle strength (MRC) [20], CuTS severity according to McGowan [40], quality of life using the SF-36 questionnaire [20], patient satisfaction [21], sensory threshold [21], neuropathy (SQUNE) [40], and neuromuscular ultrasound (NMUS) [40] were each used only once. Elbow night splinting [19,33,42], neurodynamic techniques [19,32,42], and ultrasound therapy [21,32,42] were evaluated in at least one of the four papers, either as the sole form of intervention [19,21,32,42] or as a component of the complex treatment applied [32,33,42]. Two studies used sham therapy to assess the effect of placebo on treatment [20,40]. The following physical stimuli were used in at least one study: short-wave diathermy [20], low-level laser [21], shock wave [40], and dry cupping [32]. Elements of treatment used in studies included strengthening exercises, autoneuromobilization, and co-contraction in one study [32], as well as patient education [19] and steroid injection [33]. Intra-group improvements, with no significant intergroup differences, were found in four studies [19,21,32,33], while intergroup differences after the interventions were observed in two papers [40,42], and one study found no changes in the parameters measured [20].
3.2. Prospective Studies
In the papers describing prospective studies without a control group, the following methods were used to assess the condition of the participants: two-point discrimination assessment [17,37,39], sensory threshold assessment based on Semmes–Weinstein monofilament [17,37], neurophysiological assessment (NCS) [17,37,39], Tinel’s sign [17,39], elbow flexion provocation test [39], measurements of grip strength and pinch grip strength [37,39], measurement of global muscle strength (MMT) [37], strength assessment of the first dorsal interosseous and flexor digitorum profundus to small finger [39], pain assessment (VAS) [17], assessment using the QDASH questionnaire [39], and SF-12 [39]. All of these papers described elbow night splinting as a form of intervention [17,37,39], and two additionally instructed participants on how to modify their activities of daily living [37,39]. Furthermore, a significant proportion of participants improved on all assessed parameters (73% to 100%) [17,37,39].
3.3. Case Studies
The case reports used a variety of methods to assess patients conditions, including pain severity score (VAS, NRS) [18,23,35,36,38], and measurements of grip strength [23,34,38] and pincer grip strength [38]. The sensory threshold was also assessed [38]. Provocative tests, such as elbow joint flexion [18,35,38], Tinel’s sign [18,34,38], the elevated arm stress test (EAST) [34], and the nerve provocation test [18,35,41] were carried out. Structural changes were assessed (PAM) [35] and a selective tissue tension test (STTT) was performed [35]. The DASH or QuickDASH questionnaires [22,38,41] were used to assess upper limb function, and, in one study, participants self-assessed neuropathic symptoms (S-LANSS) [41]. The global rating of change (GROC) [23,41] and patient-specific functional scale (PSFS) [23] were also employed. Furthermore, the severity of paresthesias [22,34], range of motion (ROM) [18,35], and functional status (NPQ) [18] were measured. Neurophysiological examination was performed in three cases (NCS) [18,22,36], and magnetic resonance imaging (MRI) [36] was conducted in one study. Neurodynamic techniques were used as treatment methods [18,38,41], and in one of the studies, it was performed by the patient [41]. Ultrasound therapy [38], shock wave [22], pulsed radiofrequency (PRF) [36], percutaneous electrical stimulation (PENS) [41], manual therapy [35], chiropractic therapy [34], dry needling [23], kinesiotaping [34], cold packs [38], and strengthening and resistance exercises [38] were also used. In all the studies cited, the authors achieved significant improvements and/or resolution of complaints [18,22,23,34,35,36,38,41].
4. Discussion
An analysis of the literature evaluating the effectiveness of various forms of broadly defined physiotherapy in the conservative treatment of CuTS indicates that their use can have a beneficial effect in reducing many subjective and objective symptoms and improving function. In the vast majority of papers included in this review (17/18), their authors indicated positive therapeutic effects [17,18,19,21,22,23,32,33,34,35,36,37,38,39,40,41,42]. Only one randomized controlled trial reported no change following therapy compared with a sham control group [20]. It can therefore be stated that the results of the research conducted so far are optimistic. However, it seems that the results obtained and the conclusions drawn from them should also be viewed critically. Only 7 of the 18 (39%) papers included in the review were randomized controlled trials [19,20,21,32,33,40,42], while 3 (17%) were prospective studies without a control group [17,37,39], and 8 (44%) papers were case studies [18,22,23,34,35,36,38,41], in which 23 people with CuTS were studied.
Randomized controlled trials have the lowest risk of bias, so they provide the most objective and reliable results. Most of the randomized controlled trials included in this review reported beneficial effects of the therapy (in 6/7 papers) [19,21,32,33,40,42]. However, it should be emphasized that in only four papers [19,21,33,40] the diagnosis of CuTS was based on medical history, orthopedic examination, and electrophysiological examination, which is considered a ‘gold standard’ in the diagnosis of compression syndromes [43]. In other studies, the diagnosis was based only on the medical history and orthopedic examination [20,32,42], which, of course, is very often sufficient in combination with an ultrasound examination, but, without an ultrasound and electrophysiological examination, other causes cannot be excluded, such as Guyon canal syndrome, cervical radiculopathy, or brachial plexopathy, which can produce similar symptoms [9]. Special attention should also be paid to the different methodologies used in all eligible randomized controlled trials. The majority of the papers assessed pain complaints (5/7 papers) [19,20,21,32,40], but although pain is the predominant symptom, it is not necessarily specific to CuTS. While several studies investigated muscle strength [19,20,21,32,42], function [20,32,40], and sensation [21], only one analyzed the overall quality of health [20]. The large spectrum of parameters studied makes it significantly more difficult to compare the results obtained from different studies. A similar observation can be made for the multitude of different physiotherapy interventions. In fact, different physiotherapy programs were used in each paper selected for review. In three out of seven papers [21,32,42], one of the groups used ultrasounds as one of the components of physiotherapy programs, and in two papers, it was used as the only form of therapy [21,42]. Also, in three papers, the common element of the physiotherapy program was neurodynamic techniques [19,32,42], but the other components of the physiotherapy program were different. Neurodynamic mobilizations to enhance ulnar nerve gliding include sliding techniques and, to a lesser extent, tensioning techniques. A sliding technique is an alternation of combined movements of (at least) two joints in which one movement loads the peripheral nervous system while the other movement simultaneously unloads the nervous system. These techniques facilitate nerve gliding without intensely challenging the nervous system. This process allows gliding to take place inside the nerve itself and between the surrounding tissues. The patient is in a supine position with a contralateral side bending position of the neck. External rotation is 90° abduction, and the shoulder is positioned in depression. The therapist executes passive forearm pronation and supination whereas the elbow is flexed to 90°. In the second step, the therapist pronates the forearm and conducts passive elbow flexion from 90° to 140° from the first position. Third, the therapist conducts shoulder depression from 90° to 120° of abduction, beginning from the final position obtained with the elbow in 90° flexion [18,32,42]. Also, in three papers, limb immobilization with a splint was used as the only therapy or as one of the components of a therapy program [19,33,42]. Other studies used short-wave diathermy [20], laser [21], shock wave [40], and strengthening exercises [32].
Benincá et al. [44] describe diathermy as the use of high-frequency electromagnetic currents to induce heat. It has many applications, such as producing tissue damage during surgery, hyperthermia treatment in oncology, and as a deep heating method in rehabilitation. The heating effects include pain relief, increased nerve conduction velocity, blood flow, local metabolism, tissue elasticity, and muscle relaxation. One form of diathermy used by physical therapists that achieves these effects is shortwave diathermy (SWD), which produces shortwave electric and magnetic fields in the tissue. SWD can be delivered by an inductive technique, in which the greatest amount of heat occurs in deep tissue, or by a capacitive technique, in which the greatest amount of heat occurs in superficial tissue. Inductive types of electrodes consist of a current flowing through a coiled cable that may be contained within drum or sleeve electrodes. Capacitive electrodes consist of two air plates or pad electrodes that allow for three arrangements: coplanar (electrodes placed side by side, tissues parallel to the current), anti-planar (electrodes on either side of the body part, tissues in series to the current), or longitudinal (electrodes placed at each end of the limb on opposite sides of the body part, tissues in series to the current). Each technique can be continuous (CSWD) or pulsed (PSWD), the continuous mode being used primarily for thermal effects, while the pulsed mode is used primarily for non-thermal effects.
Low-level laser therapy (LLLT) is described by Glazov et al. [45] as a light source treatment that may act via non-thermal or photochemical reactions in cells. It includes laser acupuncture, which involves focused irradiation at specific points, most commonly traditional acupuncture points, with a low-intensity laser. LLLT for pain relief in medicine remains controversial with claims that apparent efficacy is due to the placebo effect. Multiple mechanisms for LLLT analgesia may exist. There is experimental evidence suggesting that laser irradiation induces peripheral neural blockade, suppresses central synaptic activity, modulates neurotransmitters, reduces muscle spasm and interstitial oedema, and exerts anti-inflammatory effects.
Extracorporeal shock wave therapy (ESWT) was described by Yao et al. [46] as a non-invasive procedure in which acoustic waves are focused on targeted sites within the body to facilitate pain relief and healing. In general, ESWT is considered safe, non-invasive, easy to apply, and well tolerated by most patients, and so has been widely used for many musculoskeletal conditions over the last 25–30 years. Although the exact mechanisms for analgesic and functional effects are still incompletely understood, it is suggested that shock waves accelerate tissue regeneration, reduce calcification, and inhibit pain receptors.
This wide variation in the therapeutic programs in the randomized clinical trials conducted to date considerably complicates the comparison of study results. Therefore, the results obtained should be viewed with some caution. It should also be emphasized that only two out of seven randomized clinical trials performed a longitudinal evaluation of the effectiveness of the applied physiotherapy program [19,33], which indicated the achieved effects of the applied therapy were maintained after six months. The remaining five studies evaluated the effectiveness of the therapy program directly [32,42] or a maximum of 3 months [20,21,40] after its completion, so it cannot be assumed that the effects would be sustained over a longer period of time, and it seems that maintaining sustained improvements is most important from the point of view of its effectiveness.
In all three prospective studies without a control group included in this review, some improvements were obtained in patients with CuTS [17,37,39]. Improvements were documented in all participants in the first study [17], 88% of participants in the second [39], and 73% in the third [37]. Neurophysiological assessment was also performed in all studies, although subjects with normal nerve conduction who showed typical CuTS symptoms were also included [39]. Sensory threshold and discriminative sensation were assessed in two studies [17,37], while only discriminative sensation was assessed in one study [39], and pain intensity was assessed in one study [17]. Two out of three papers measured muscle strength [37,39], and one study evaluated the degree of disability [39] and general quality of health [39]. In all three studies, the main component of therapy was an elbow night splinting [17,37,39]. Two studies employed additionally provided instruction on changing habits during activities of daily living. All studies examined not only the effects immediately after the therapy but also the long-term effects one year later [17,37,39]. Although orthoses were used in all of these studies, unfortunately, the angle of flexion varied in each study (from the elbow in full extension to flexion up to 60°), which was not justified in any way. Unfortunately, the main limitation of all these studies was the lack of a control group. Therefore, it is impossible to verify whether the effects obtained result from the therapy used, spontaneous recovery, or the placebo effect.
Positive effects of the applied therapy were obtained in all case studies [18,22,23,34,35,36,38,41]. The studies reported a reduction in pain [18,22,23,36,38,41], improved function [18,22,23,38,41], increased muscle strength [23,34,38], and reduced symptoms in provocation tests [18,34,35,38]. Evaluation of therapeutic effects occurred immediately after therapy but in 6/8 papers also much later: 3 [22,36,41], 6 [18,23,36,41], and even 12 months [38,41] after the intervention. Unfortunately, the small number of study participants (23 people in all studies), the very large methodological variation, and the use of different physiotherapy programs require considerable caution in drawing conclusions about the effectiveness of the therapy used. The studies assessed pain [18,23,35,36,38], range of motion [18,35], sensation [38], muscle strength [34,38], and hand dexterity [22,38,41], conducted provocation tests [18,34,35,38]. Therapeutic interventions varied from neurodynamic techniques, spinal and rib manipulation [18], manual therapy [35], electric therapy [36,41], ultrasound [38], shock wave [22], and dry needling [23]. Dry needling as described by Gattie et al. [47] is a technique in which a fine needle is used to penetrate the skin, subcutaneous tissues, and muscle with the intention of mechanically disrupting the tissue without the use of an anesthetic. Dry needling is often used to treat myofascial trigger points (MTrPs), which are described as localized hypersensitive areas within a palpable taut band of muscle. These hypersensitive areas can be classified as active MTrPs when they elicit spontaneous pain and, on palpation, reproduce the pain known to the patient. Latent MTrPs do not elicit spontaneous pain and are painful only on palpation. Myofascial trigger points are commonly seen in patients with musculoskeletal pain. The physiologic mechanism underlying the action of dry needling remains to be elucidated. However, it has been suggested that dry needling may induce both local and central neural responses to restore homeostasis at the MTrP site, resulting in a reduction in both peripheral and central pain sensitivity. Centrally, dry needling may activate descending control mechanisms in the brain or spinal cord. Dry needling has been shown to immediately increase pressure pain threshold and range of motion, reduce muscle tension, and reduce pain in patients with musculoskeletal disorders.
The number of therapy sessions also varied and equaled 1 [36], 3 [41], 5 [18], or 11 [34]. Unfortunately, in the vast majority of these papers, the diagnosis of CuTS was based only on medical history and/or orthopedic examination [18,22,23,34,35,38,41], while electrophysiological examination was performed in only three cases [18,22,36], including one that was within normal values [18]. It is therefore difficult to confirm whether in all case studies the patients actually had CuTS or whether the symptoms had another cause. Also, in case study research, the lack of comparison with non-therapy cases may indicate that the effects obtained after therapy are the result of spontaneous recovery or a placebo effect. It should also be emphasized that case studies are subjected to a high risk of bias, and therefore the results obtained from the physiotherapy programs used should be approached with caution.
Techniques that may be useful in treating CuTS include interferential current (IFC), transcutaneous electrical nerve stimulation (TENS), neuromuscular electrical stimulation (NMES), and deep oscillation procedures. According to Rampazo and Liebano [48], IFC therapy involves the transcutaneous application of two medium-frequency alternating currents (>1 kHz to <10 kHz) out of phase to deliver current to deep tissues. For example, one of the alternating currents may have a fixed frequency of 4000 Hz, while the frequency of the other alternating current may be set between 4000 and 4250 Hz. The two medium-frequency currents “interfere” in the tissue and produce an amplitude-modulated low-frequency “beat” (0–250 Hz) which is the difference between the values of the two applied currents. IFC is an example of a pulse-modulated sinusoidal alternating current, also known as kilohertz alternating current, and is reportedly more comfortable, reaches deeper tissues, and produces greater muscle torque than low-frequency pulsed currents. There are several parameters that can be adjusted in IFC devices, including the carrier frequency, amplitude modulated frequency, sweep frequency, sweep mode or swing pattern (slope), application type (bipolar or quadripolar application), and application time and intensity.
Mokhtari et al. [49] describe TENS as a noninvasive pain relief technique that activates peripheral nerves by delivering electrical impulses to the intact skin surface, which can modulate the transmission of nerve impulses by inhibiting presynaptic nociceptive information. In practice, TENS can be implemented using different stimulus parameters in terms of frequency, intensity, and electrode placement. Since TENS with different stimulus parameters can activate different populations of nerve fibers, this technique can be divided into different types, including conventional TENS (low intensity and high frequency), acupuncture-like TENS (high intensity and low frequency), and intensive TENS (high intensity and high frequency).
As described by Doucet et al. [50], neuromuscular electrical stimulation, used interchangeably with electrical stimulation (ES), is typically delivered at higher frequencies (20–50 Hz) with the express purpose of producing tetany and muscle contraction that can be used for “functional” purposes. The frequencies of electrical stimulation used can vary widely depending on the goals of the task or intervention, but most clinical regimens use patterns of 20–50 Hz to achieve optimal results. To avoid fatigue or discomfort, a constant low-frequency stimulation that produces a smooth contraction at low force levels is typically used. Electrical stimulation devices deliver pulses in waveforms that are often represented by geometric shapes such as a square, spike, or sine wave. Controversy regarding optimal electrode placement is common in the literature, with most debates centering on whether the muscle belly or the motor point is the preferred location. Program duration has ranged from 30 min once a day to an hour in each session three times daily. The total treatment period ranged from 2 weeks to 3 months.
Deep Oscillation (DO), as described by Villalba-Meneses et al. [51], is a patented manual therapy that produces mechanical vibrations in the skin and deep tissues. This device uses repeated electrostatic oscillations to relieve the pain and swelling of a specific area by moving the swelling through the lymphatic system. DO therapy builds up a pulsating electrostatic field of low intensity (100–400 V; 150 μA) and low frequency (5–250 Hz) between the hand applicator and the affected tissue. Its low-frequency electrostatic field produces a throbbing effect in the underlying tissues that improves wound healing and anti-inflammatory effects, stimulates lymphatic flow, stimulates collagen production, and cell regeneration, and ensures more blood reaches the affected area. Both the patient and the physical therapist are connected to the deep oscillation device, which serves as a source of tension with high internal resistance. The impulse of the voltage produces an electrostatic attraction on the tissue and rhythmic frictions are generated when massaging the oedema. These rhythmic frictions result in oscillations of the local tissue (skin, conductive tissue, subcutaneous adipose tissue, muscles, blood, and lymphatic vessels) and increase the vascular circulation of the area concerned. Each session of deep oscillation therapy follows a rigorous clinical protocol. In most medical trials, therapy begins with 15 min of conventional manual lymphatic drainage. Later, the DO equipment is used for 10 min at 200–250 Hz in the area to be treated, and oscillations of 85 Hz are administered for 10 min to finish. The physiological effects of deep oscillation therapy in the treatment of low back pain will depend on the frequency and intensity applied. Clinical studies have reported that DO therapy restores mobility between fibers, repairs affected tissue, exerts anti-inflammatory effects, reduces oedema, improves drainage channels, and accelerates wound healing.
It must be emphasized that, from the broader perspective, studies to date on the effectiveness of physiotherapy in the conservative treatment of CuTS have found beneficial effects, although no clear far-reaching conclusions can be drawn at this stage. This is mainly due to the small number of randomized clinical trials, the significant methodological discrepancies regarding both the diagnosis of CuTS and the parameters studied, and the significant variety of therapeutic programs used. Therefore, high-quality randomized controlled trials evaluating the effectiveness of different physiotherapy measures in the conservative treatment of CuTS are needed. Due to the frequent occurrence of CuTS, case studies do not seem to be relevant. Since positive therapeutic effects were documented in most of the papers included in this review, similar therapeutic programs based on manual therapy incorporating neurodynamic techniques, ultrasound therapy, low-level laser, or other measures that had a beneficial effect on the patient’s condition could be used in further studies. It would also be advisable to conduct studies with blinding of participants and investigators.
This critical review of studies evaluating the effectiveness of physiotherapy in the conservative treatment of CuTS has some limitations. Only two databases and the Google Scholar search engine were used to search for papers for the review. This was limited to English-language papers only, so other valuable studies might have been likely omitted, especially randomized controlled trials that have evaluated the effectiveness of physiotherapy in the conservative treatment of CuTS. Another limitation is that we have only managed to cover a limited number of the existing physiotherapy procedures with positive effects on CuTS.
5. Conclusions
A review of studies to date evaluating the effectiveness of physiotherapy in the conservative treatment of CuTS leads to the conclusion that beneficial therapeutic effects were achieved in the majority of these studies. The small number of randomized clinical trials and their considerable heterogeneity do not allow firm conclusions to be drawn about the effectiveness of physiotherapy in the conservative treatment of CuTS.
6. Future Directions
High-quality randomized controlled trials evaluating the effectiveness of different physiotherapy programs in the conservative treatment of CuTS are needed.
Author Contributions
Conceptualization, M.W. and T.W.; methodology, M.W., T.W. and R.G.; formal analysis, M.W. and T.W.; investigation, M.W., T.W. and R.G.; resources, M.W., R.G. and T.W.; data curation, M.W. and T.W.; writing—original draft preparation, M.W.; writing—review and editing, M.W., T.W. and R.G.; visualization, M.W.; supervision, T.W. and R.G.; project administration, T.W.; funding acquisition, T.W. and M.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available upon request.
Conflicts of Interest
Author Michał Wieczorek was employed by the company The Health Center in Mikołów Ltd. The remaining author declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
References
- Palmer, B.A.; Hughes, T.B. Cubital Tunnel Syndrome. J. Hand Surg. Am. 2010, 35, 153–163. [Google Scholar] [CrossRef]
- Arle, J.E.; Zager, E.L. Surgical Treatment of Common Entrapment Neuropathies in the Upper Limbs. Muscle Nerve 2000, 23, 1160–1174. [Google Scholar] [CrossRef] [PubMed]
- Cambon-Binder, A. Ulnar Neuropathy at the Elbow. Orthop. Traumatol. Surg. Res. 2021, 107, 102754. [Google Scholar] [CrossRef] [PubMed]
- An, T.W.; Evanoff, B.A.; Boyer, M.I.; Osei, D.A. The Prevalence of Cubital Tunnel Syndrome: A Cross-Sectional Study in a U.S. Metropolitan Cohort. J. Bone Jt. Surg. Am. Vol. 2017, 99, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Elhassan, B.; Steinmann, S.P. Entrapment Neuropathy of the Ulnar Nerve. J. Am. Acad. Orthop. Surg. 2007, 15, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Kooner, S.; Cinats, D.; Kwong, C.; Matthewson, G.; Dhaliwal, G. Conservative Treatment of Cubital Tunnel Syndrome: A Systematic Review. Orthop. Rev. 2019, 11, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Staples, J.R.; Calfee, R. Cubital Tunnel Syndrome: Current Concepts. J. Am. Acad. Orthop. Surg. 2017, 25, e215–e224. [Google Scholar] [CrossRef] [PubMed]
- McGowan, A.J. The Results of Transposition of the Ulnar Nerve for Traumatic Ulnar Neuritis. J. Bone Jt. Surg. Br. 1950, 32, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Mezian, K.; Jačisko, J.; Kaiser, R.; Machač, S.; Steyerová, P.; Sobotová, K.; Angerová, Y.; Naňka, O. Ulnar Neuropathy at the Elbow: From Ultrasound Scanning to Treatment. Front. Neurol. 2021, 12, 661441. [Google Scholar] [CrossRef]
- Juratli, S.M.; Nayan, M.; Fulton-Kehoe, D.; Robinson, L.R.; Franklin, G.M. A Population-Based Study of Ulnar Neuropathy at the Elbow in Washington State Workers’ Compensation. Am. J. Ind. Med. 2010, 53, 1242–1251. [Google Scholar] [CrossRef]
- Sunderland, S. Nerves and Nerve Injuries; Churchill Livingstone: Edinburgh, UK; London, UK; New York, NY, USA, 1978. [Google Scholar]
- Assmus, H.; Antoniadis, G.; Bischoff, C.; Hoffmann, R.; Martini, A.K.; Preiler, P.; Scheglmann, K.; Schwerdtfeger, K.; Wessels, K.D.; Wüstner-Hofmann, M. Cubital Tunnel Syndrome a Review and Management Guidelines. Zentralbl. Neurochir. 2011, 72, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, N.; Honmo, J.; Tsujino, A.; Nisiura, Y. Electrodiagnosis in Entrapment Neuropathy by the Arcade of Struthers. Clin. Orthop. Relat. Res. 2000, 378, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Cutts, S. Cubital Tunnel Syndrome. Postgrad. Med. J. 2007, 83, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Shin, R.; Ring, D. The Ulnar Nerve in Elbow Trauma. J. Bone Jt. Surg. 2007, 89, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Alblas, C.L.; van Kasteel, V.; Jellema, K. Injection with Corticosteroids (Ultrasound Guided) in Patients with an Ulnar Neuropathy at the Elbow, Feasibility Study. Eur. J. Neurol. 2012, 19, 1582–1584. [Google Scholar] [CrossRef] [PubMed]
- Seror, P. Treatment of With Nerve Splint Palsy at the Elbow with a Night Splint. J Bone Jt. Surg Br. 1993, 75, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Coppieters, M.W.; Bartholomeeusen, K.E.; Stappaerts, K.H. Incorporating Nerve-Gliding Techniques in the Conservative Treatment of Cubital Tunnel Syndrome. J. Manip. Physiol. Ther. 2004, 27, 560–568. [Google Scholar] [CrossRef]
- Svernlöv, B.; Larsson, M.; Rehn, K.; Adolfsson, L. Conservative Treatment of the Cubital Tunnel Syndrome. J. Hand Surg. 2009, 34, 201–207. [Google Scholar] [CrossRef]
- Bilgin Badur, N.; Unlu Ozkan, F.; Aktas, I. Efficacy of Shortwave Diathermy in Ulnar Nerve Entrapment at the Elbow: A Double-Blind Randomized Controlled Clinical Trial. Clin. Rehabil. 2020, 34, 1048–1055. [Google Scholar] [CrossRef]
- Ozkan, F.U.; Saygı, E.K.; Senol, S.; Kapcı, S.; Aydeniz, B.; Aktaş, İ.; Gozke, E. New Treatment Alternatives in the Ulnar Neuropathy at the Elbow: Ultrasound and Low-Level Laser Therapy. Acta Neurol. Belg. 2015, 115, 355–360. [Google Scholar] [CrossRef]
- Shen, Y.P.; Wu, Y.Y.; Chu, H.Y.; Li, T.Y.; Chen, L.C.; Wu, Y.T. Extracorporeal Shock Wave Therapy in Cubital Tunnel Syndrome: A Pilot Study. Neurol. Asia 2018, 23, 233–238. [Google Scholar]
- Anandkumar, S.; Manivasagam, M. Effect of Dry Needling on Cubital Tunnel Syndrome: Three Case Reports. Physiother. Theory Pract. 2019, 35, 363–372. [Google Scholar] [CrossRef]
- Waugh, R.P.; Zlotolow, D.A. In Situ Decompression of the Ulnar Nerve at the Cubital Tunnel. Hand Clin. 2007, 23, 319–327. [Google Scholar] [CrossRef]
- Tsai, T.-M.; Chen, I.-C.; Majd, M.E.; Lim, B.-H. Cubital Tunnel Release with Endoscopic Assistance: Results of a New Technique. J. Hand Surg. Am. 1999, 24, 21–29. [Google Scholar] [CrossRef]
- King, T. The Treatment of Traumatic Ulnar Neuritis; Mobilization of the Ulnar Nerve at the Elbow by Removal of the Medial Epicondyle and Adjacent Bone. Aust. N. Z. J. Surg. 1950, 20, 33–42. [Google Scholar] [CrossRef]
- Catalano, L.W.; Barron, O.A. Anterior Subcutaneous Transposition of the Ulnar Nerve. Hand Clin. 2007, 23, 339–344. [Google Scholar] [CrossRef]
- Kleinman, W.B.; Bishop, A.T. Anterior Intramuscular Transposition of the Ulnar Nerve. J. Hand Surg. Am. 1989, 14, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Leffert, R.D. Anterior Submuscular Transposition of the Ulnar Nerves by the Learmonth Technique. J. Hand Surg. Am. 1982, 7, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Zlowodzki, M.; Chan, S.; Bhandari, M.; Kalliainen, L.; Schubert, W. Anterior Transposition Compared with Simple Decompression for Treatment of Cubital Tunnel Syndrome. J. Bone Jt. Surg.-Am. Vol. 2007, 89, 2591–2598. [Google Scholar] [CrossRef] [PubMed]
- Bartels, R.H.M.A.; Verhagen, W.I.M.; van der Wilt, G.J.; Meulstee, J.; van Rossum, L.G.M.; Grotenhuis, J.A. Prospective Randomized Controlled Study Comparing Simple Decompression versus Anterior Subcutaneous Transposition for Idiopathic Neuropathy of the Ulnar Nerve at the Elbow: Part 1. Neurosurgery 2005, 56, 522–530. [Google Scholar] [CrossRef]
- Galal, D.O.S.M.G.; Abdelmageed, S.M.; Elserty, N.; Helmy, A.M. Effect of Dry Cupping Therapy with Neurodynamic Mobilization on Pain Intensity, Muscle Strength and Functional Abilities in Patients with Cubital Tunnel Syndrome: A Randomized Clinical Trial. Turk. J. Physiother. Rehabil. 2021, 32, 8689–8697. [Google Scholar]
- Hong, C.Z.; Long, H.A.; Kanakamedala, R.V.; Chang, Y.M.; Yates, L. Splinting and Local Steroid Injection for the Treatment of Ulnar Neuropathy at the Elbow: Clinical and Electrophysiological Evaluation. Arch. Phys. Med. Rehabil. 1996, 77, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Illes, J.D.; Johnson, T.L. Chiropractic Management of a Patient with Ulnar Nerve Compression Symptoms: A Case Report. J. Chiropr. Med. 2013, 12, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kearns, G.; Wang, S. Medical Diagnosis of Cubital Tunnel Syndrome Ameliorated with Thrust Manipulation of the Elbow and Carpals. J. Man. Manip. Ther. 2012, 20, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.; Jeong, D.; Choo, Y.J.; Chang, M.C. Management of Neuropathic Pain Induced by Cubital Tunnel Syndrome Using Pulsed Radiofrequency Two Case Reports. Medicine 2019, 98, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Nakamichi, K.; Tachibana, S.; Ida, M.; Yamamoto, S. Patient Education for the Treatment of Ulnar Neuropathy at the Elbow. Arch. Phys. Med. Rehabil. 2009, 90, 1839–1845. [Google Scholar] [CrossRef] [PubMed]
- Oskay, D.; Meriç, A.; Kirdi, N.; Firat, T.; Ayhan, Ç.; Leblebicioǧlu, G. Neurodynamic Mobilization in the Conservative Treatment of Cubital Tunnel Syndrome: Long-Term Follow-Up of 7 Cases. J. Manip. Physiol. Ther. 2010, 33, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.M.; Calfee, R.P.; Gelberman, R.H.; Goldfarb, C.A. Outcomes of Rigid Night Splinting and Activity Modification in the Treatment of Cubital Tunnel Syndrome. J. Hand Surg. Am. 2013, 38, 1125–1130.e1. [Google Scholar] [CrossRef]
- Alashkar, D.S.; Hablas, S. Therapeutic Potentials of Radial Shock Wave in Cubital Tunnel Syndrome. Egypt. J. Hosp. Med. 2023, 91, 5212–5218. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Arias-Buría, J.L.; El Bachiri, Y.R.; Plaza-Manzano, G.; Cleland, J.A. Ultrasound-Guided Percutaneous Electrical Stimulation for a Patient with Cubital Tunnel Syndrome: A Case Report with a One-Year Follow-Up. Physiother. Theory Pract. 2022, 38, 1564–1569. [Google Scholar] [CrossRef]
- Gaber, M.; El_dein, M. Ultrasound versus Nerve Gliding on Hand Grip Strength in Cubital Tunnel Syndrome. Egypt. J. Phys. Ther. 2021, 5, 1–5. [Google Scholar] [CrossRef]
- Johnson, E.W. Diagnosis of Carpal Tunnel Syndrome the Gold Standard. Am. J. Phys. Med. Rehabil. 1993, 72, 1. [Google Scholar] [CrossRef] [PubMed]
- Benincá, I.L.; de Estéfani, D.; Pereira de Souza, S.; Weisshahn, N.K.; Haupenthal, A. Tissue Heating in Different Short Wave Diathermy Methods: A Systematic Review and Narrative Synthesis. J. Bodyw. Mov. Ther. 2021, 28, 298–310. [Google Scholar] [CrossRef]
- Glazov, G.; Yelland, M.; Emery, J. Low-Level Laser Therapy for Chronic Non-Specific Low Back Pain: A Meta-Analysis of Randomised Controlled Trials. Acupunct. Med. 2016, 34, 328–341. [Google Scholar] [CrossRef]
- Yao, G.; Chen, J.; Duan, Y.; Chen, X. Efficacy of Extracorporeal Shock Wave Therapy for Lateral Epicondylitis: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 2064781. [Google Scholar] [CrossRef]
- Gattie, E.; Cleland, J.A.; Snodgrass, S. The Effectiveness of Trigger Point Dry Needling for Musculoskeletal Conditions by Physical Therapists: A Systematic Review and Meta-Analysis. J. Orthop. Sports Phys. Ther. 2017, 47, 133–149. [Google Scholar] [CrossRef]
- Rampazo, É.P.; Liebano, R.E. Analgesic Effects of Interferential Current Therapy: A Narrative Review. Medicina 2022, 58, 141. [Google Scholar] [CrossRef]
- Mokhtari, T.; Ren, Q.; Li, N.; Wang, F.; Bi, Y.; Hu, L. Transcutaneous Electrical Nerve Stimulation in Relieving Neuropathic Pain: Basic Mechanisms and Clinical Applications. Curr. Pain Headache Rep. 2020, 24, 14. [Google Scholar] [CrossRef] [PubMed]
- Doucet, B.M.; Lam, A.; Griffin, L. Neuromuscular Electrical Stimulation for Skeletal Muscle Function. Yale J. Biol. Med. 2012, 85, 201–215. [Google Scholar]
- Villalba-Meneses, F.; Chaglla-Monge, K.; Almeida-Galárraga, D.; Cadena-Morejón, C.; Moreno-Calvo, A.; Marín, J.; Marín, J.J. Evaluation of Deep Oscillation Therapy for the Treatment of Lumbar Pain Syndrome Using Motion Capture Systems: A Systematic Review. J. Bodyw. Mov. Ther. 2024, 38, 180–190. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).