

Prevalence of Septate Uterus in a Large Population of Women of Reproductive Age: Comparison of ASRM 2016 and 2021, ESHRE/ESGE, and CUME Diagnostic Criteria: A Prospective Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
- women aged 18 to 45 years old;
- asymptomatic or complaining of pelvic pain, uterine bleeding, or vaginal discharge;
- no virgo intacta (for allowing transvaginal ultrasound);
- previous hysterectomy for any reason;
- past or current history of gynecological cancer;
- previous metroplasty with uterine septum resection;
- menopause established.
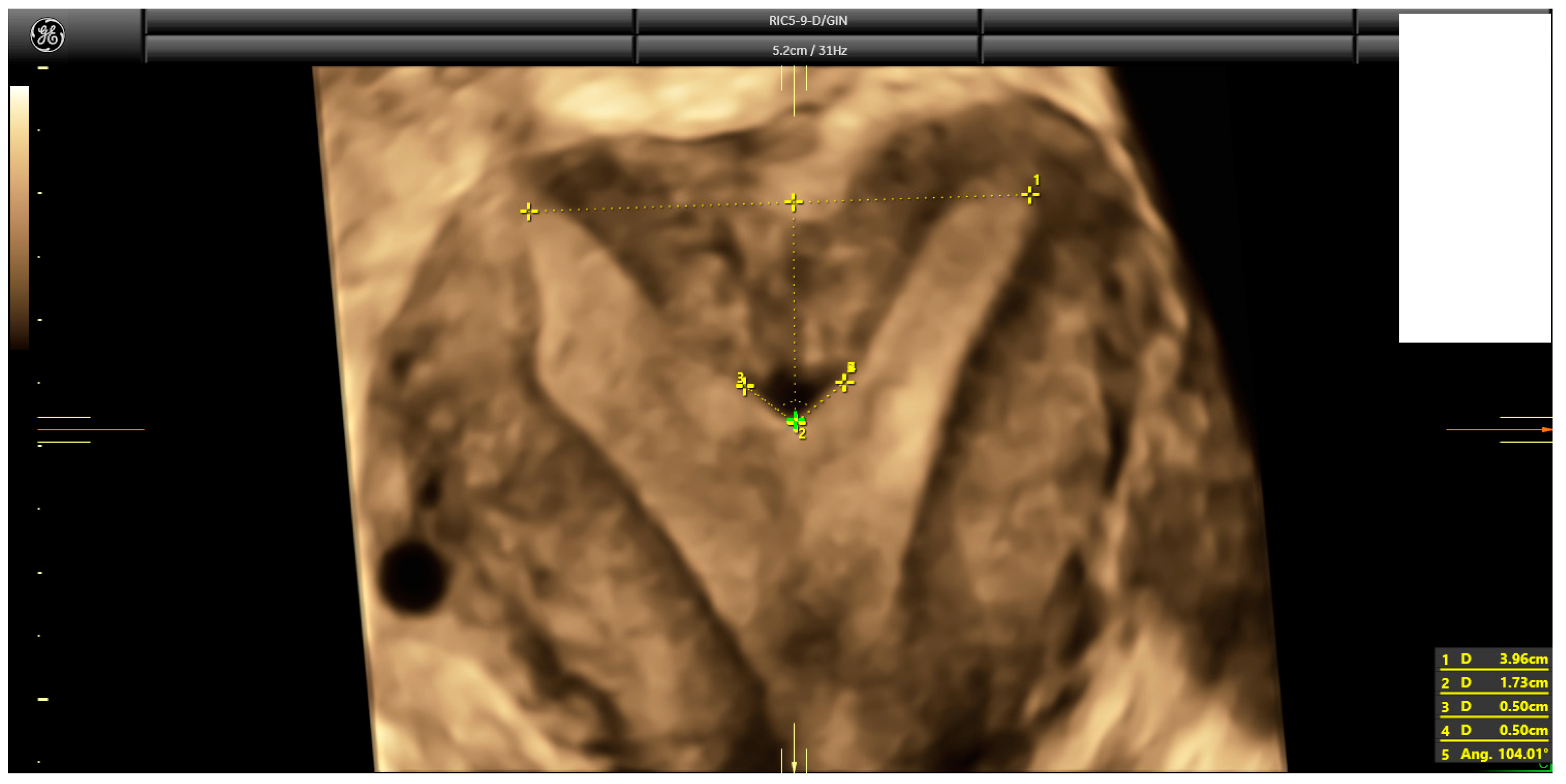
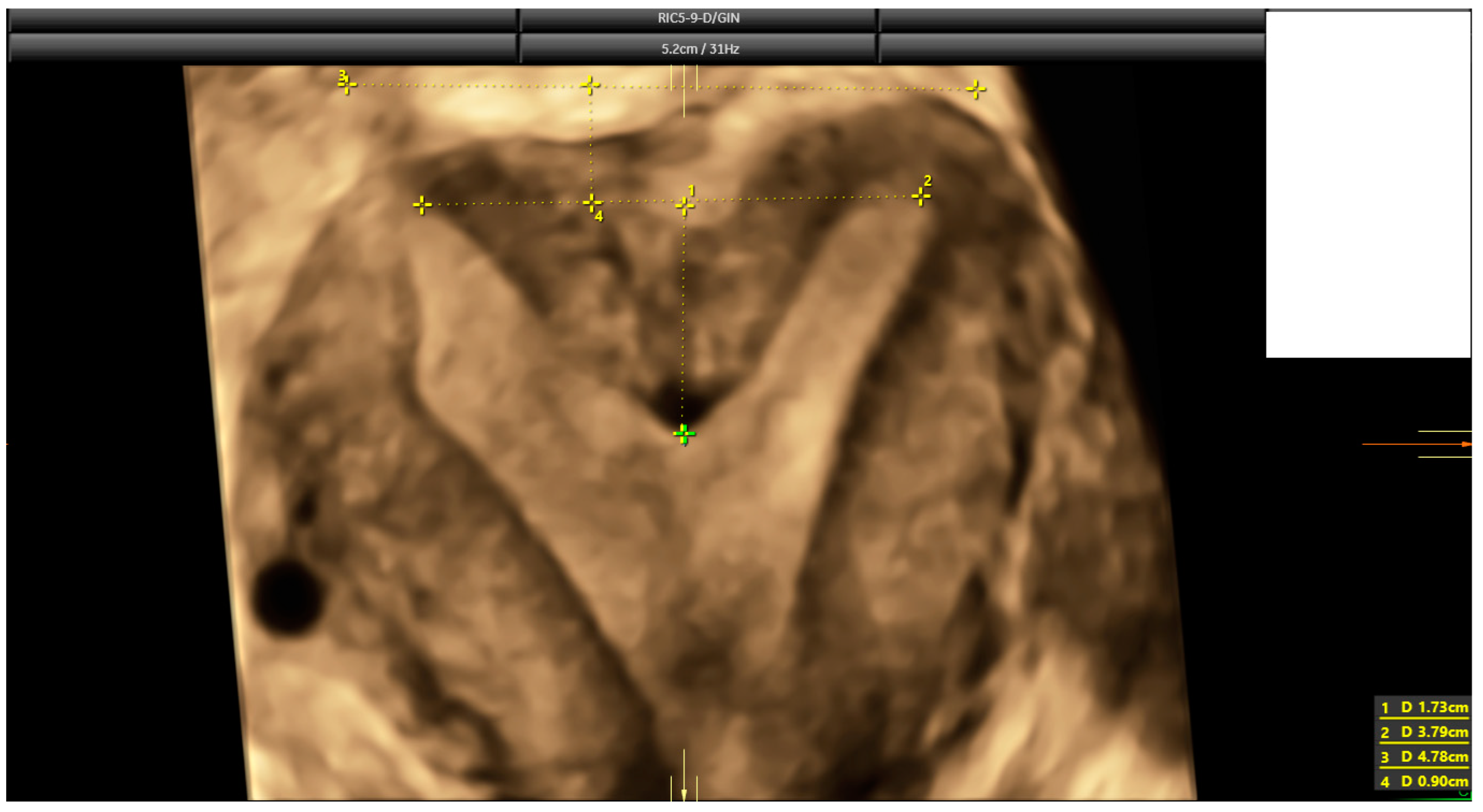
2.3. Ultrasound Evaluation
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
4. Discussion
4.1. Summary of Findings
4.2. Interpretation of Findings
4.3. Strengths and Limitations
4.4. Future Research Agenda
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akhtar, M.A.; Saravelos, S.H.; Li, T.C.; Jayaprakasan, K.; Royal College of Obstetricians and Gynaecologists. Reproductive Implications and Management of Congenital Uterine Anomalies: Scientific Impact Paper No. 62 November 2019. BJOG Int. J. Obstet. Gynaecol. 2020, 127, e1–e13. [Google Scholar] [CrossRef] [PubMed]
- Passos, I.M.P.E.; Britto, R.L. Diagnosis and treatment of müllerian malformations. Taiwan J. Obstet. Gynecol. 2020, 59, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.Y.; Jayaprakasan, K.; Zamora, J.; Thornton, J.G.; Raine-Fenning, N.; Coomarasamy, A. The prevalence of congenital uterine anomalies in unselected and high-risk populations: A systematic review. Hum. Reprod. Update 2011, 17, 761–771. [Google Scholar] [CrossRef] [PubMed]
- The American Fertility Society. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil. Steril. 1988, 49, 944–955. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Gordts, S.; Di Spiezio Sardo, A.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.C.; Tanos, V.; Brölmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef]
- Oppelt, P.; Renner, S.P.; Brucker, S.; Strissel, P.L.; Strick, R.; Oppelt, P.G.; Doerr, H.G.; Schott, G.E.; Hucke, J.; Wallwiener, D.; et al. The VCUAM (Vagina Cervix Uterus Adnex-associated Malformation) classification: A new classification for genital malformations. Fertil. Steril. 2005, 84, 1493–1497. [Google Scholar] [CrossRef]
- Acién, P.; Acién, M.I. The history of female genital tract malformation classifications and proposal of an updated system. Hum. Reprod. Update 2011, 17, 693–705. [Google Scholar] [CrossRef]
- Salim, R.; Woelfer, B.; Backos, M.; Regan, L.; Jurkovic, D. Reproducibility of three-dimensional ultrasound diagnosis of congenital uterine anomalies. Ultrasound Obstet. Gynecol. 2003, 21, 578–582. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Practice Committee of the American Society for Reproductive Medicine. Uterine septum: A guideline. Fertil. Steril. 2016, 106, 530–540. [Google Scholar] [CrossRef]
- Pfeifer, S.M.; Attaran, M.; Goldstein, J.; Lindheim, S.R.; Petrozza, J.C.; Rackow, B.W.; Siegelman, E.; Troiano, R.; Winter, T.; Zuckerman, A.; et al. ASRM müllerian anomalies classification 2021. Fertil. Steril. 2021, 116, 1238–1252. [Google Scholar] [CrossRef]
- Ludwin, A.; Tudorache, S.; Martins, W.P. ASRM Müllerian Anomalies Classification 2021: A critical review. Ultrasound Obstet. Gynecol. 2022, 60, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Grimbizis, G.F.; Di Spiezio Sardo, A.; Saravelos, S.H.; Gordts, S.; Exacoustos, C.; Van Schoubroeck, D.; Bermejo, C.; Amso, N.N.; Nargund, G.; Timmerman, D.; et al. The Thessaloniki ESHRE/ESGE consensus on diagnosis of female genital anomalies. Hum. Reprod. 2016, 31, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Detti, L.; Peregrin-Alvarez, I.; Roman, R.A.; Levi D’Ancona, R.; Gordon, J.C.; Christiansen, M.E. A comparison of four systems for uterine septum diagnosis and indication for surgical correction. Minerva Obstet. Gynecol. 2021, 73, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Ludwin, A.; Martins, W.P.; Bhagavath, B.; Lindheim, S.R. Overdiagnosis, overdetection, and overdefinition of the septate uterus: Reexamination of the ASRM and ESHRE-ESGE criteria is urgently needed. Fertil. Steril. 2019, 112, 448–449. [Google Scholar] [CrossRef]
- Ludwin, A.; Martins, W.P.; Nastri, C.O.; Ludwin, I.; Coelho Neto, M.A.; Leitão, V.M.; Acién, M.; Alcazar, J.L.; Benacerraf, B.; Condous, G.; et al. Congenital Uterine Malformation by Experts (CUME): Better criteria for distinguishing between normal/arcuate and septate uterus? Ultrasound Obstet. Gynecol. 2018, 51, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Ludwin, A.; Ludwin, I.; Coelho Neto, M.A.; Nastri, C.O.; Bhagavath, B.; Lindheim, S.R.; Martins, W.P. Septate uterus according to ESHRE/ESGE, ASRM and CUME definitions: Association with infertility and miscarriage, cost and warnings for women and healthcare systems. Ultrasound Obstet. Gynecol. 2019, 54, 800–814. [Google Scholar] [CrossRef]
- Heinonen, P.K. Distribution of female genital tract anomalies in two classifications. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 141–146. [Google Scholar] [CrossRef]
- Knez, J.; Saridogan, E.; Van Den Bosch, T.; Mavrelos, D.; Ambler, G.; Jurkovic, D. ESHRE/ESGE female genital tract anomalies classification system-the potential impact of discarding arcuate uterus on clinical practice. Hum. Reprod. 2018, 33, 600–606. [Google Scholar] [CrossRef]
- Schöller, D.; Hölting, M.; Stefanescu, D.; Burow, H.; Schönfisch, B.; Rall, K.; Taran, F.; Grimbizis, G.F.; Di Spiezio Sardo, A.; Brucker, S.Y. Female genital tract congenital malformations and the applicability of the ESHRE/ESGE classification: A systematic retrospective analysis of 920 patients. Arch. Gynecol. Obstet. 2018, 297, 1473–1481. [Google Scholar] [CrossRef]
- Ouyang, Y.; Yi, Y.; Gong, F.; Lin, G.; Li, X. ESHRE-ESGE versus ASRM classification in the diagnosis of septate uterus: A retrospective study. Arch. Gynecol. Obstet. 2018, 298, 845–850. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Royo, P.; Alcázar, J.L. Three-dimensional power Doppler assessment of uterine vascularization in women with primary dysmenorrhea. J. Ultrasound. Med. 2008, 27, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Ludwin, A.; Martins, W.P. Correct measurements of uterine fundal internal indentation depth and angle: An important but overlooked issue for precise diagnosis of uterine anomalies. Ultrasound Obstet. Gynecol. 2021, 58, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Harmsen, M.J.; Van den Bosch, T.; de Leeuw, R.A.; Dueholm, M.; Exacoustos, C.; Valentin, L.; Hehenkamp, W.J.K.; Groenman, F.; De Bruyn, C.; Rasmussen, C.; et al. Consensus on revised definitions of Morphological Uterus Sonographic Assessment (MUSA) features of adenomyosis: Results of modified Delphi procedure. Ultrasound Obstet. Gynecol. 2022, 60, 118–131. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, C.; Castro, M.; Carriles, I.; Arriba, M.; Lapresa, V.; Alcazar, J.L. Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Using Three Different Classifications: An Interobserver and Intraobserver Agreement Study. Rev. Bras. Ginecol. Obs. 2021, 43, 911–918. [Google Scholar] [CrossRef]
- Bhagavath, B.; Ellie, G.; Griffiths, K.M.; Winter, T.; Alur-Gupta, S.; Richardson, C.; Lindheim, S.R. Uterine Malformations: An Update of Diagnosis, Management, and Outcomes. Obstet. Gynecol. Surv. 2017, 72, 377–392. [Google Scholar] [CrossRef]
- Saravelos, S.H.; Cocksedge, K.A.; Li, T.C. Prevalence and diagnosis of congenital uterine anomalies in women with reproductive failure: A critical appraisal. Hum. Reprod. Update 2008, 14, 415–429. [Google Scholar] [CrossRef]
- Ludwin, A.; Ludwin, I. Comparison of the ESHRE-ESGE and ASRM classifications of Müllerian duct anomalies in everyday practice. Hum. Reprod. 2015, 30, 569–580. [Google Scholar] [CrossRef]
- Rikken, J.F.W.; Kowalik, C.R.; Emanuel, M.H.; Bongers, M.Y.; Spinder, T.; Jansen, F.W.; Mulders, A.G.M.G.J.; Padmehr, R.; Clark, T.J.; van Vliet, H.A.; et al. Septum resection versus expectant management in women with a septate uterus: An international multicentre open-label randomized controlled trial. Hum. Reprod. 2021, 36, 1260–1267. [Google Scholar] [CrossRef]
- Kowalik, C.R.; Goddijn, M.; Emanuel, M.H.; Bongers, M.; Spinder, T.; de Kruif, J.H.; Mol, B.W.; Heineman, M.J. Metroplasty versus expectant management for women with recurrent miscarriage and a septate uterus. Cochrane Database Syst. Rev. 2011, CD008576. [Google Scholar] [CrossRef]
- Valle, R.F.; Ekpo, G.E. Hysteroscopic metroplasty for the septate uterus: Review and meta-analysis. J Minim Invasive Gynecol. 2013, 20, 22–42. [Google Scholar] [CrossRef] [PubMed]
- Noventa, M.; Spagnol, G.; Marchetti, M.; Saccardi, C.; Bonaldo, G.; Laganà, A.S.; Cavallin, F.; Andrisani, A.; Ambrosini, G.; Vitale, S.G.; et al. Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes—A Systematic Review and Meta-Analysis of Observational Research. J. Clin. Med. 2022, 11, 3290. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhang, M.; Sun, P.; Jiang, J.J.; Yan, L. Pregnancy and Adverse Obstetric Outcomes After Hysteroscopic Resection: A Systematic Review and Meta-Analysis. Front. Surg. 2022, 9, 889696. [Google Scholar] [CrossRef] [PubMed]
- Carrera, M.; Pérez Millan, F.; Alcázar, J.L.; Alonso, L.; Caballero, M.; Carugno, J.; Dominguez, J.A.; Moratalla, E. Effect of Hysteroscopic Metroplasty on Reproductive Outcomes in Women with Septate Uterus: Systematic Review and Meta-Analysis. J. Minim. Invasive Gynecol. 2022, 29, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wang, L.; Wang, B.; Shen, H.; Wu, J.; He, J.; Liu, A.; Wang, Y.; Zhang, X.; Ma, B. Reproductive outcomes of natural pregnancy after hysteroscopic septum resection in patients with a septate uterus: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2023, 5, 100762. [Google Scholar] [CrossRef] [PubMed]
- Joshi, B.; Kaushal, A.; Suri, V.; Gainder, S.; Choudhary, N.; Jamwal, S.; Sharma, S. Prevalence and Pregnancy Outcome of Mullerian Anomalies in Infertile Women: A Retrospective Study. J. Hum. Reprod. Sci. 2021, 14, 431–435. [Google Scholar]
- Russo, C.; Conway, F.; Siciliano, T.; Selntigia, A.; Martire, G.F.; Soreca, G.; Ticconi, C.; Exacoustos, C. 3D transvaginal ultrasound diagnosis of uterine septa according to different classifications: Are there other measurements that correlate to reproductive outcome in small indentation length? Facts Views Vis. Obgyn 2022, 14, 129–138. [Google Scholar] [CrossRef]
- Galusiano, M.; Gulino, F.A.; Incognito, G.G.; Cimino, M.; Dalisi, V.; Di Stefano, A.; D’Urso, V.; Cannone, F.; Martire, F.G.; Palumbo, M. Role of hysteroscopy in infertility: The eternal dilemma. Clin. Exp. Obstet. Gynecol. 2023, 50, 99. [Google Scholar] [CrossRef]
- Abuzeid, O.; LaChance, J.; Zaghmout, O.; Corrado, J.; Hebert, J.; Ashraf, M.; Abuzeid, M.I. The role of diagnostic hysteroscopy in diagnosis of incomplete uterine septum/significant arcuate uterine anomaly in infertile patients in the era of transvaginal 3D ultrasound scan. Middle East Fertil. Soc. J. 2020, 25, 1. [Google Scholar] [CrossRef]
- Lin, Y.; Liu, M.; He, S.; Yang, M.; Wu, Q. The effectiveness of uterine parametrics measured by three-dimensional transvaginal sonography in the diagnosis of uterine cavity distortions. Ann. Transl. Med. 2020, 8, 1486. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age * | 35.0 years (8.1) | Range: 18–45 |
| Gravidity † | 1.0 (2.0) | Range: 0–10 |
| Parity † | 0.0 (1.0) | Range: 0–6 |
| Miscarriage † | 0.0 (0.0) | Range: 0–6 |
| Termination of pregnancy † | 0.0 (0.0) | Range: 0–2 |
| Parameter | ||
|---|---|---|
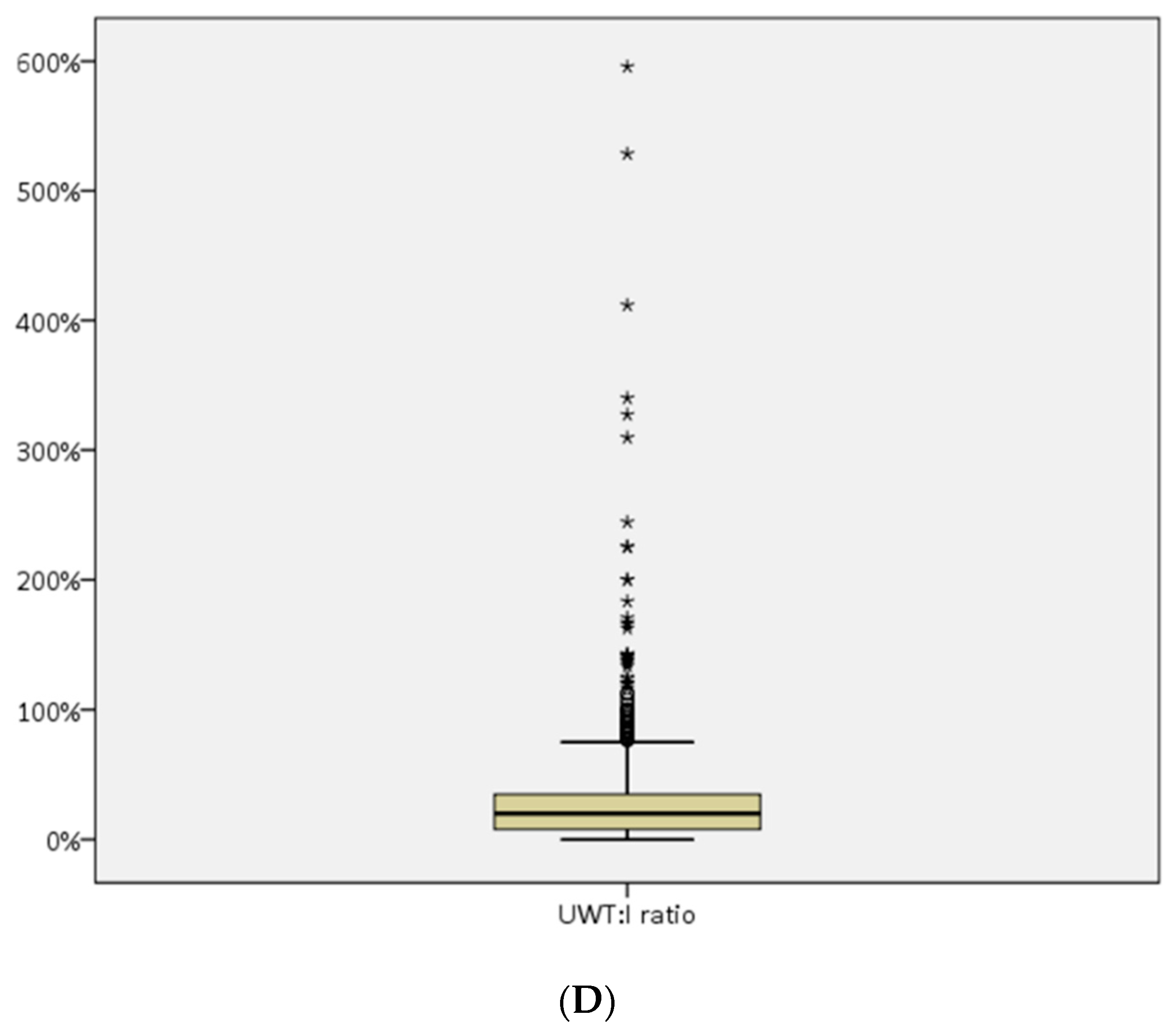
| Indentation length * | 2.0 mm (2.3) | Range: 0–37 mm |
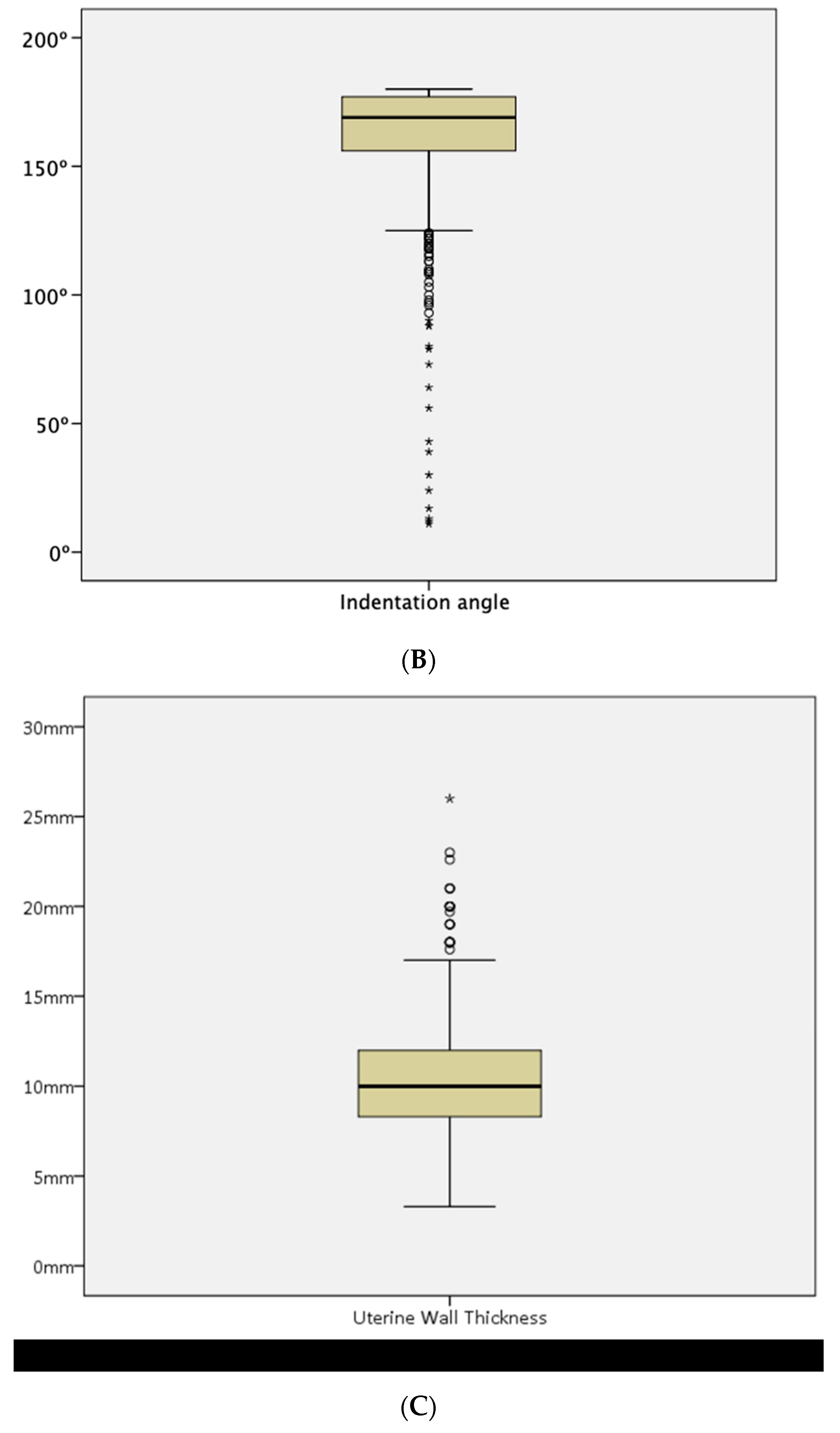
| Uterine Wall thickness * | 10.0 mm (3.7) | Range: 3.3–26.0 mm |
| Indentation angle * | 169° (21.0) | Range: 0–180° |
| I:WT ratio * | 20% (27.0) | Range: 1–596% |
| ESHER-ESGE Septate | ESHRE-ESGE No Septate | Total | |
|---|---|---|---|
| CUME septate | 23 | 0 | 23 |
| CUME no septate | 109 | 845 | 954 |
| 2016-ASRM septate | 9 | 0 | 9 |
| 2016-ASRM gray zone | 9 | 0 | 9 |
| 2016-ASRM no septate | 114 | 845 | 959 |
| 2021-ASRM septate | 14 | 0 | 14 |
| 2021-ASRM gray zone | 11 | 0 | 11 |
| 2021-ASRM no septate | 107 | 845 | 952 |
| 2016-ASRM Septate | 2016-ASRM Grey Zone | 2016-ASRM No Septate | Total | |
|---|---|---|---|---|
| CUME septate | 9 | 7 | 7 | 23 |
| CUME no septate | 0 | 2 | 952 | 954 |
| 2021-ASRM septate | 9 | 5 | 0 | 14 |
| 2021-ASRM gray zone | 0 | 4 | 7 | 11 |
| 2021-ASRM no septate | 0 | 0 | 952 | 952 |
| 2021-ASRM Septate | 2021-ASRM Grey Zone | 2021-ASRM No Septate | Total | |
|---|---|---|---|---|
| CUME septate | 14 | 9 | 0 | 23 |
| CUME no septate | 0 | 2 | 952 | 954 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carriles, I.; Brotons, I.; Errasti, T.; Ruiz-Zambrana, A.; Ludwin, A.; Alcazar, J.L. Prevalence of Septate Uterus in a Large Population of Women of Reproductive Age: Comparison of ASRM 2016 and 2021, ESHRE/ESGE, and CUME Diagnostic Criteria: A Prospective Study. Diagnostics 2024, 14, 2019. https://doi.org/10.3390/diagnostics14182019
Carriles I, Brotons I, Errasti T, Ruiz-Zambrana A, Ludwin A, Alcazar JL. Prevalence of Septate Uterus in a Large Population of Women of Reproductive Age: Comparison of ASRM 2016 and 2021, ESHRE/ESGE, and CUME Diagnostic Criteria: A Prospective Study. Diagnostics. 2024; 14(18):2019. https://doi.org/10.3390/diagnostics14182019
Chicago/Turabian StyleCarriles, Isabel, Isabel Brotons, Tania Errasti, Alvaro Ruiz-Zambrana, Artur Ludwin, and Juan Luis Alcazar. 2024. "Prevalence of Septate Uterus in a Large Population of Women of Reproductive Age: Comparison of ASRM 2016 and 2021, ESHRE/ESGE, and CUME Diagnostic Criteria: A Prospective Study" Diagnostics 14, no. 18: 2019. https://doi.org/10.3390/diagnostics14182019