
The Value of C-Reactive Protein and Peritoneal Cytokines as Early Predictors of Anastomotic Leak after Colorectal Surgery

 , , ,
, , ,
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Sample Collection
2.3. Statistics
3. Results
3.1. Patient Characteristics
3.2. CRP Levels in Serum
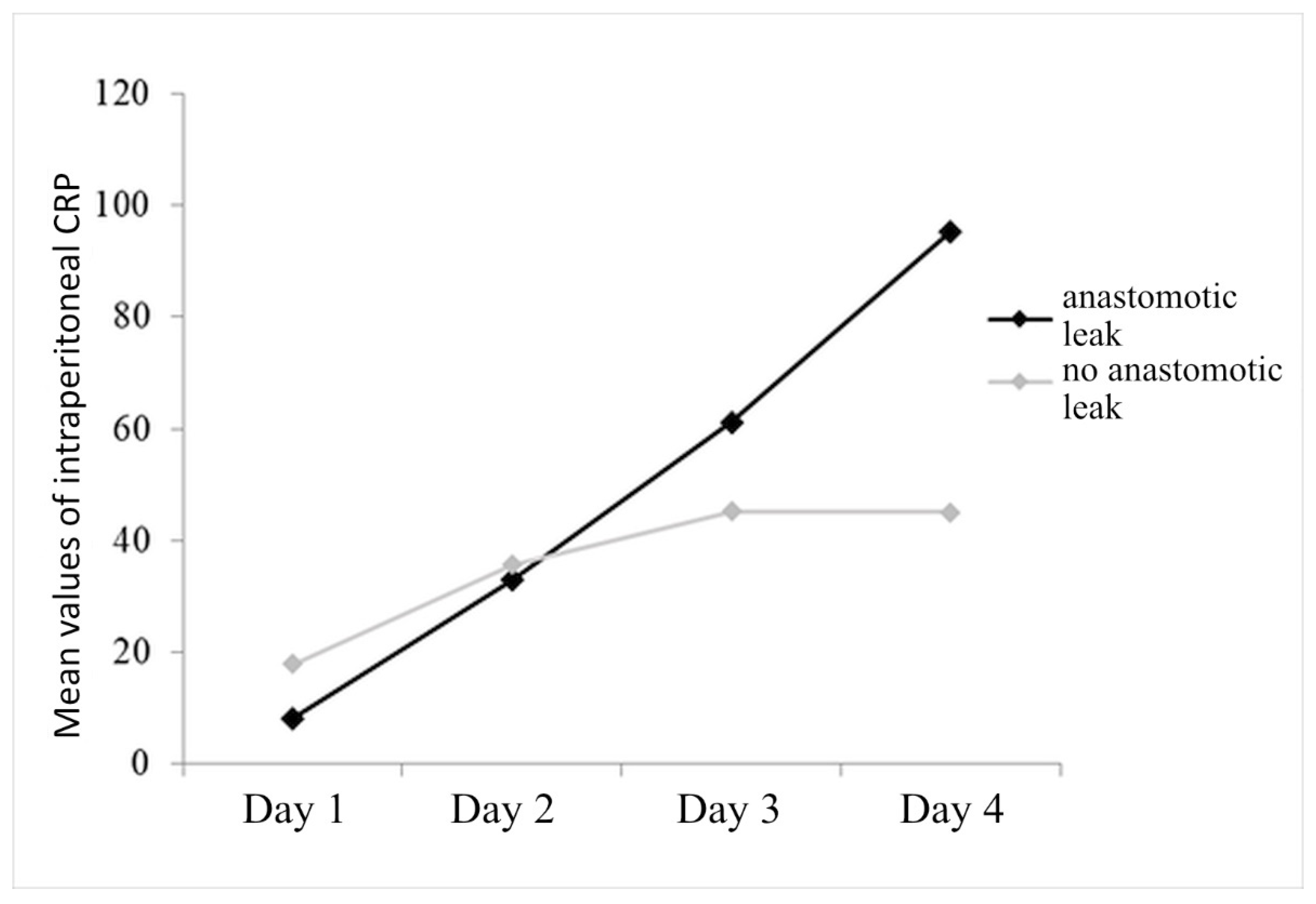
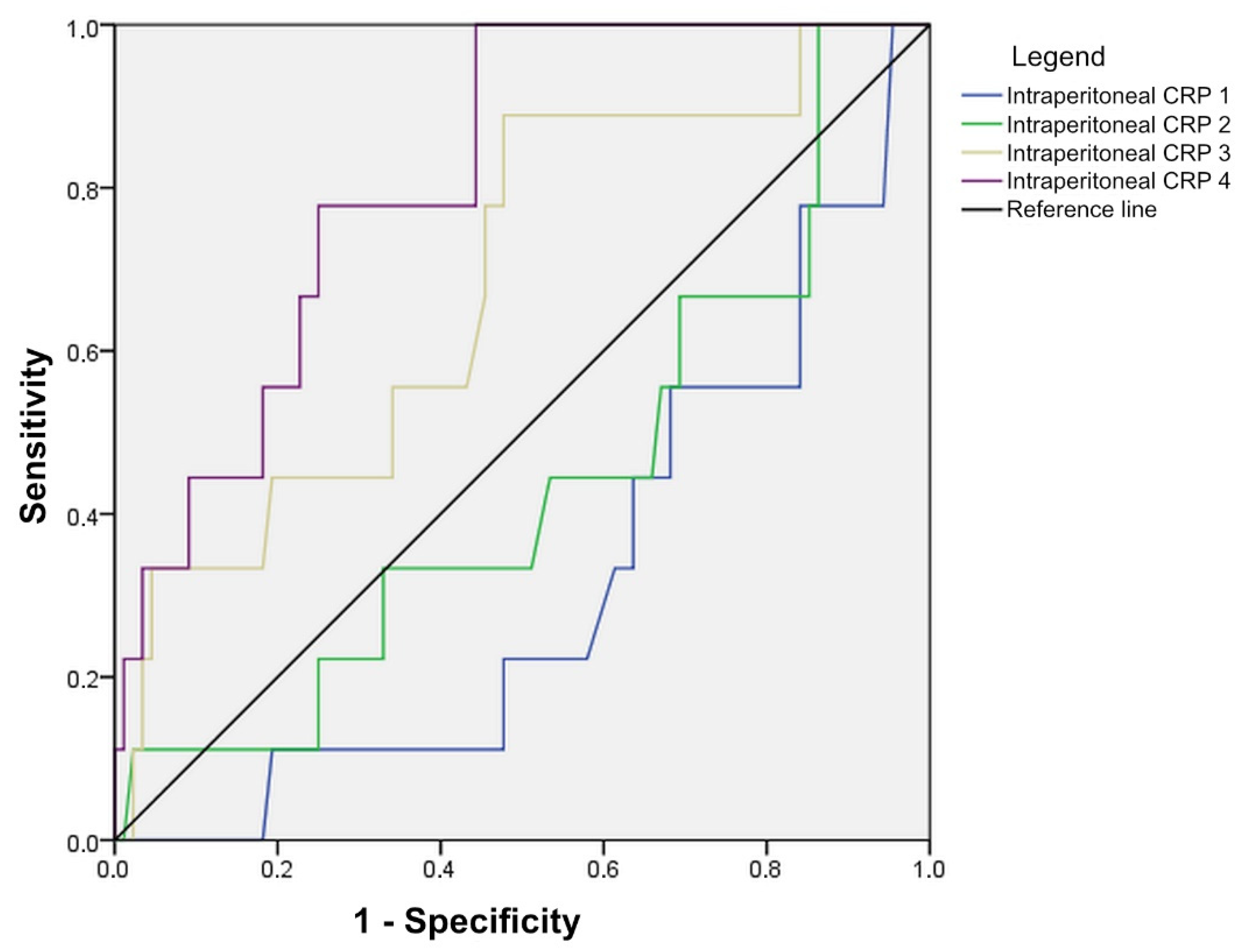
3.3. CRP Levels in Peritoneal Fluid
3.4. IL-6 Levels in Peritoneal Fluid
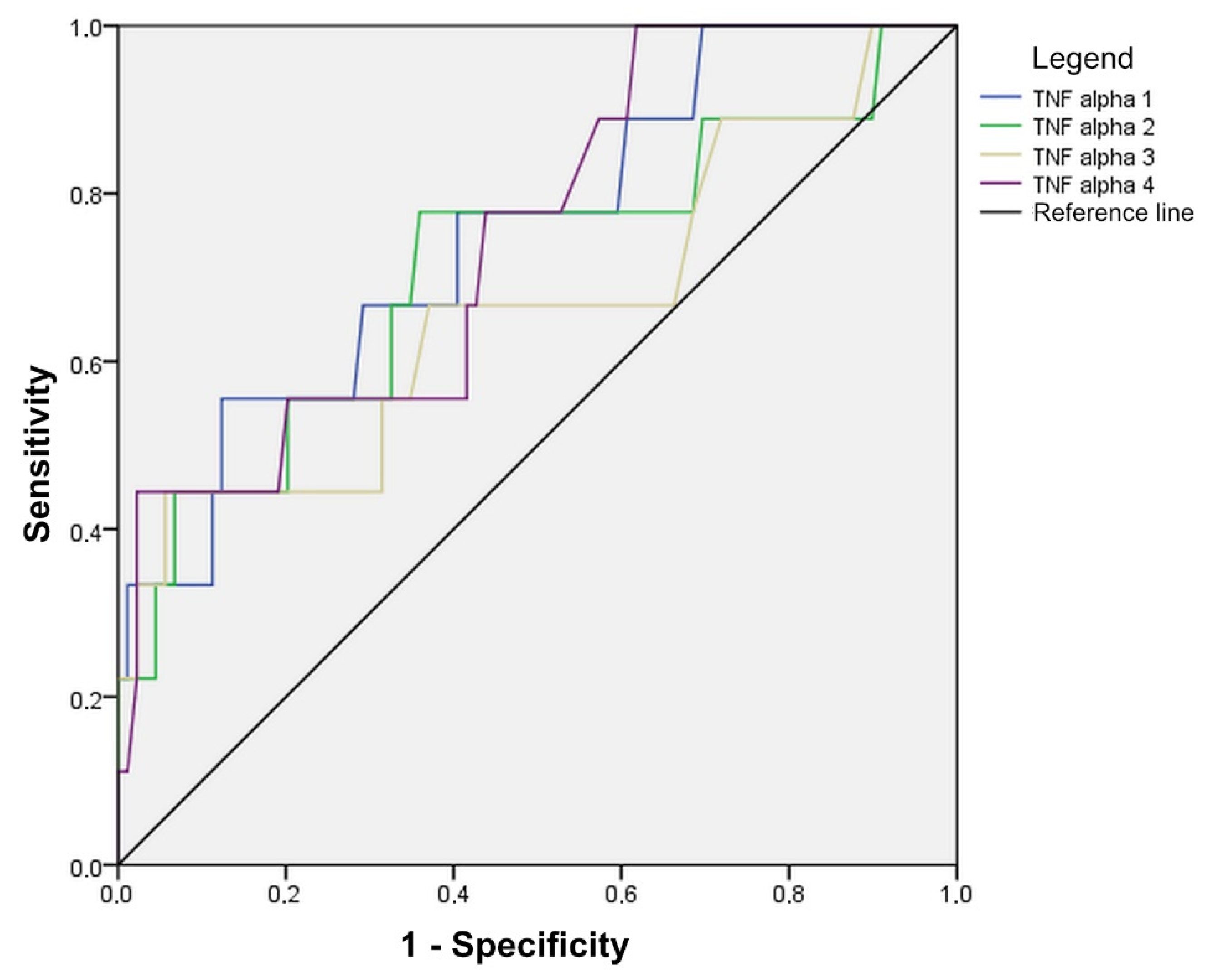
3.5. TNF-Alpha in Peritoneal Fluid
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hyman, N.; Manchester, T.L.; Osler, T.; Burns, B.; Cataldo, P.A. Anastomotic Leaks After Intestinal Anastomosis: It’s Later Than You Think. Ann. Surg. 2007, 245, 254–258. [Google Scholar] [CrossRef]
- Kingham, T.P.; Pachter, H.L. Colonic anastomotic leak: Risk factors, diagnosis, and treatment. J. Am. Coll. Surg. 2009, 208, 269–278. [Google Scholar] [CrossRef]
- Park, J.S.; Choi, G.S.; Kim, S.H.; Kim, H.R.; Kim, N.K.; Lee, K.Y.; Kang, S.B.; Kim, J.Y.; Lee, K.Y.; Kim, B.C.; et al. Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: The Korean laparoscopic colorectal surgery study group. Ann. Surg. 2013, 257, 665–671. [Google Scholar] [CrossRef]
- Wallace, B.; Schuepbach, F.; Gaukel, S.; Marwan, A.I.; Staerkle, R.F.; Vuille-Dit-Bille, R.N. Evidence according to Cochrane Systematic Reviews on Alterable Risk Factors for Anastomotic Leakage in Colorectal Surgery. Gastroenterol. Res. Pract. 2020, 2020, 9057963. [Google Scholar] [CrossRef]
- Matthiessen, P.; Hallböök, O.; Andersson, M.; Rutegård, J.; Sjödahl, R. Risk factors for anastomotic leakage after anterior resection of the rectum. Color. Dis. 2004, 6, 462–469. [Google Scholar] [CrossRef]
- Veyrie, N.; Ata, T.; Muscari, F.; Couchard, A.-C.; Msika, S.; Hay, J.-M.; Fingerhut, A.; Dziri, C. Anastomotic leakage after elective right versus left colectomy for cancer: Prevalence and independent risk factors. J. Am. Coll. Surg. 2007, 205, 785–793. [Google Scholar] [CrossRef]
- Golda, T.; Lazzara, C.; Zerpa, C.; Sobrino, L.; Fico, V.; Kreisler, E.; Biondo, S. Risk factors for ileocolic anastomosis dehiscence; a cohort study. Am. J. Surg. 2020, 220, 170–177. [Google Scholar] [CrossRef]
- Park, J.S.; Huh, J.W.; Park, Y.A.; Cho, Y.B.; Yun, S.H.; Kim, H.C.; Lee, W.Y. Risk Factors of Anastomotic Leakage and Long-Term Survival After Colorectal Surgery. Medicine 2016, 95, e2890. [Google Scholar] [CrossRef]
- Wu, Z.; van de Haar, R.C.J.; Sparreboom, C.L.; Boersema, G.S.A.; Li, Z.; Ji, J.; Jeekel, J.; Lange, J.F. Is the intraoperative air leak test effective in the prevention of colorectal anastomotic leakage? A systematic review and meta-analysis. Int. J. Color. Dis. 2016, 31, 1409–1417. [Google Scholar] [CrossRef]
- Jessen, M.; Nerstrøm, M.; Wilbek, T.E.; Roepstorff, S.; Rasmussen, M.S.; Krarup, P.-M. Risk factors for clinical anastomotic leakage after right hemicolectomy. Int. J. Color. Dis. 2016, 31, 1619–1624. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef]
- Dietz, D.W.; Bailey, H.R. Postoperative complications. In ASCRS Textbook of Colon and Rectal Surgery; Church, J.M., Beck, D.E., Wolff, B.G., Fleshman, J.W., Pemberton, J.H., Eds.; Springer: New York, NY, USA, 2006; p. 141. [Google Scholar]
- Rullier, E.; Laurent, C.; Garrelon, J.L.; Michel, P.; Saric, J.; Parneix, M. Risk factors for anastomotic leakage after resection of rectal cancer. Br. J. Surg. 1998, 85, 355–358. [Google Scholar] [CrossRef]
- Bakker, I.S.; Grossmann, I.; Henneman, D.; Havenga, K.; Wiggers, T. Risk factors for anastomotic leakage and leak-related mortality after colonic cancer surgery in a nationwide audit. Br. J. Surg. 2014, 101, 424–432. [Google Scholar] [CrossRef]
- den Dulk, M.; Noter, S.L.; Hendriks, E.R.; Brouwers, M.; van der Vlies, C.; Oostenbroek, R.; Menon, A.; Steup, W.; van de Velde, C. Improved diagnosis and treatment of anastomotic leakage after colorectal surgery. Eur. J. Surg. Oncol. 2009, 35, 420–426. [Google Scholar] [CrossRef]
- Marres, C.C.M.; van de Ven, A.W.H.; Leijssen, L.G.J.; Verbeek, P.C.M.; Bemelman, W.A.; Buskens, C.J. Colorectal anastomotic leak: Delay in reintervention after false-negative computed tomography scan is a reason for concern. Tech. Coloproctol. 2017, 21, 709–714. [Google Scholar] [CrossRef]
- Finnerty, C.C.; Mabvuure, N.T.; Ali, A.; Kozar, R.A.; Herndon, D.N. The Surgically Induced Stress Response. JPEN J. Parenter. Enter. Nutr. 2013, 37, 21S–29S. [Google Scholar] [CrossRef]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef]
- Singh, P.P.; Zeng, I.S.; Srinivasa, S.; Lemanu, D.P.; Connolly, A.B.; Hill, A.G. Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak after colorectal surgery. Br. J. Surg. 2014, 101, 339–346. [Google Scholar] [CrossRef]
- Daams, F.; Wu, Z.; Lahaye, M.J.; Jeekel, J.; Lange, J.F. Prediction and diagnosis of colorectal anastomotic leakage: A systematic review of literature. World J. Gastrointest. Surg. 2014, 6, 14–26. [Google Scholar] [CrossRef]
- Sparreboom, C.L.; Wu, Z.; Dereci, A.; Boersema, G.S.A.; Menon, A.G.; Ji, J.; Kleinrensink, G.-J.; Lange, J.F. Cytokines as Early Markers of Colorectal Anastomotic Leakage: A Systematic Review and Meta-Analysis. Gastroenterol. Res. Pract. 2016, 2016, 3786418. [Google Scholar] [CrossRef]
- Cini, C.; Wolthuis, A.; D’Hoore, A. Peritoneal fluid cytokines and matrix metalloproteinases as early markers of anastomotic leakage in colorectal anastomosis: A literature review and meta-analysis. Color. Dis. 2013, 15, 1070–1077. [Google Scholar] [CrossRef]
- Villegas Coronado, L.; Lopez-Navarro, J.; Chavez-Bermudez, D.; Gonzalez-Jimenez, I.; Chao-Zhou, L.; Gonzalez-Bojorquez, D. Peritoneal and Serum or Plasma Interleukin-6 as Early Biomarkers for Colorectal Anastomotic Leakage after Colorectal Surgery in Patients with Colorectal Cancer: A Systematic Review and Meta-Analysis. Surg. Gastroenterol. Oncol. 2023, 28, 125. [Google Scholar] [CrossRef]
- Mari, G.; Crippa, J.; Costanzi, A.; Mazzola, M.; Rossi, M.; Maggioni, D. ERAS Protocol Reduces IL-6 Secretion in Colorectal Laparoscopic Surgery: Results From a Randomized Clinical Trial. Surg. Laparosc. Endosc. Percutan Tech. 2016, 26, 444–448. [Google Scholar] [CrossRef]
- Mouliou, D.S. C-Reactive Protein: Pathophysiology, Diagnosis, False Test Results and a Novel Diagnostic Algorithm for Clinicians. Diseases 2023, 11, 132. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | (%) | ||
|---|---|---|---|
| Gender | Male | 56 | (56.0) |
| Female | 44 | (44.0) | |
| Age (years) | <60 | 29 | (29.0) |
| 60–79 | 49 | (49.0) | |
| 80+ | 22 | (22.0) | |
| Localisation | Rectum | 32 | (32.0) |
| Left colon | 38 | (38.0) | |
| Right colon | 30 | (30.0) | |
| Cut-Off Value | Sensitivity | Specificity | AUC | 95% CI | p | |
|---|---|---|---|---|---|---|
| Serum CRP 1 | 125.50 | 60.0 | 65.2 | 0.690 | 0.540–0.839 | 0.062 |
| Serum CRP 2 | 162.05 | 80.0 | 73.0 | 0.800 | 0.684–0.916 | 0.003 |
| Serum CRP 3 | 169.90 | 77.8 | 79.9 | 0.853 | 0.733–0.972 | 0.001 |
| Serum CRP 4 | 149.00 | 77.8 | 84.3 | 0.888 | 0.791–0.984 | <0.001 |
| Cut-Off Value | Sensitivity | Specificity | AUC | 95% CI | p | |
|---|---|---|---|---|---|---|
| Peritoneal CRP 1 | 9.05 | 40.0 | 36.0 | 0.313 | 0.148–0.479 | 0.066 |
| Peritoneal CRP 2 | 31.60 | 40.0 | 43.3 | 0.437 | 0.238–0.636 | 0.534 |
| Peritoneal CRP 3 | 41.15 | 55.6 | 57.8 | 0.687 | 0.511–0.864 | 0.065 |
| Peritoneal CRP 4 | 56.65 | 77.8 | 75.6 | 0.815 | 0.697–0.933 | 0.002 |
| Cut-Off Value | Sensitivity | Specificity | AUC | 95% CI | p | |
|---|---|---|---|---|---|---|
| Interleukin-6 1 | 42,150 | 70.0 | 67.8 | 0.782 | 0.671–0.893 | 0.005 |
| Interleukin-6 2 | 26,250 | 60.0 | 61.1 | 0.614 | 0.445–0.783 | 0.263 |
| Interleukin-6 3 | 13,300 | 55.6 | 56.7 | 0.669 | 0.455–0.883 | 0.097 |
| Interleukin-6 4 | 10,800 | 55.6 | 62.2 | 0.662 | 0.476–0.848 | 0.111 |
| Cut-Off Value | Sensitivity | Specificity | AUC | 95% CI | p | |
|---|---|---|---|---|---|---|
| TNF-alpha 1 | 78.00 | 70.0 | 66.7 | 0.749 | 0.577–0.920 | 0.014 |
| TNF-alpha 2 | 58.50 | 70.0 | 66.7 | 0.708 | 0.504–0.912 | 0.040 |
| TNF-alpha 3 | 45.50 | 66.7 | 62.2 | 0.662 | 0.441–0.881 | 0.109 |
| TNF-alpha 4 | 48.50 | 55.6 | 57.8 | 0.746 | 0.580–0.911 | 0.015 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mužina, D.; Kopljar, M.; Bilić, Z.; Davidović, B.L.; Glavčić, G.; Janković, S.; Mačkić, M. The Value of C-Reactive Protein and Peritoneal Cytokines as Early Predictors of Anastomotic Leak after Colorectal Surgery. Diagnostics 2024, 14, 2101. https://doi.org/10.3390/diagnostics14182101
Mužina D, Kopljar M, Bilić Z, Davidović BL, Glavčić G, Janković S, Mačkić M. The Value of C-Reactive Protein and Peritoneal Cytokines as Early Predictors of Anastomotic Leak after Colorectal Surgery. Diagnostics. 2024; 14(18):2101. https://doi.org/10.3390/diagnostics14182101
Chicago/Turabian StyleMužina, Dubravka, Mario Kopljar, Zdenko Bilić, Blaženka Ladika Davidović, Goran Glavčić, Suzana Janković, and Monika Mačkić. 2024. "The Value of C-Reactive Protein and Peritoneal Cytokines as Early Predictors of Anastomotic Leak after Colorectal Surgery" Diagnostics 14, no. 18: 2101. https://doi.org/10.3390/diagnostics14182101
APA StyleMužina, D., Kopljar, M., Bilić, Z., Davidović, B. L., Glavčić, G., Janković, S., & Mačkić, M. (2024). The Value of C-Reactive Protein and Peritoneal Cytokines as Early Predictors of Anastomotic Leak after Colorectal Surgery. Diagnostics, 14(18), 2101. https://doi.org/10.3390/diagnostics14182101