
Anatomical Location of the Vesical Branches of the Inferior Hypogastric Plexus in Human Cadavers

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Material
2.2. Gross Post-Mortem or Open Intra-Operative Abdominal Approach
2.3. Manual Laparoscopic or Robot-Assisted Laparoscopic Approach
2.4. Histological Assessment of Nerve Branches
2.5. Statistics
3. Results
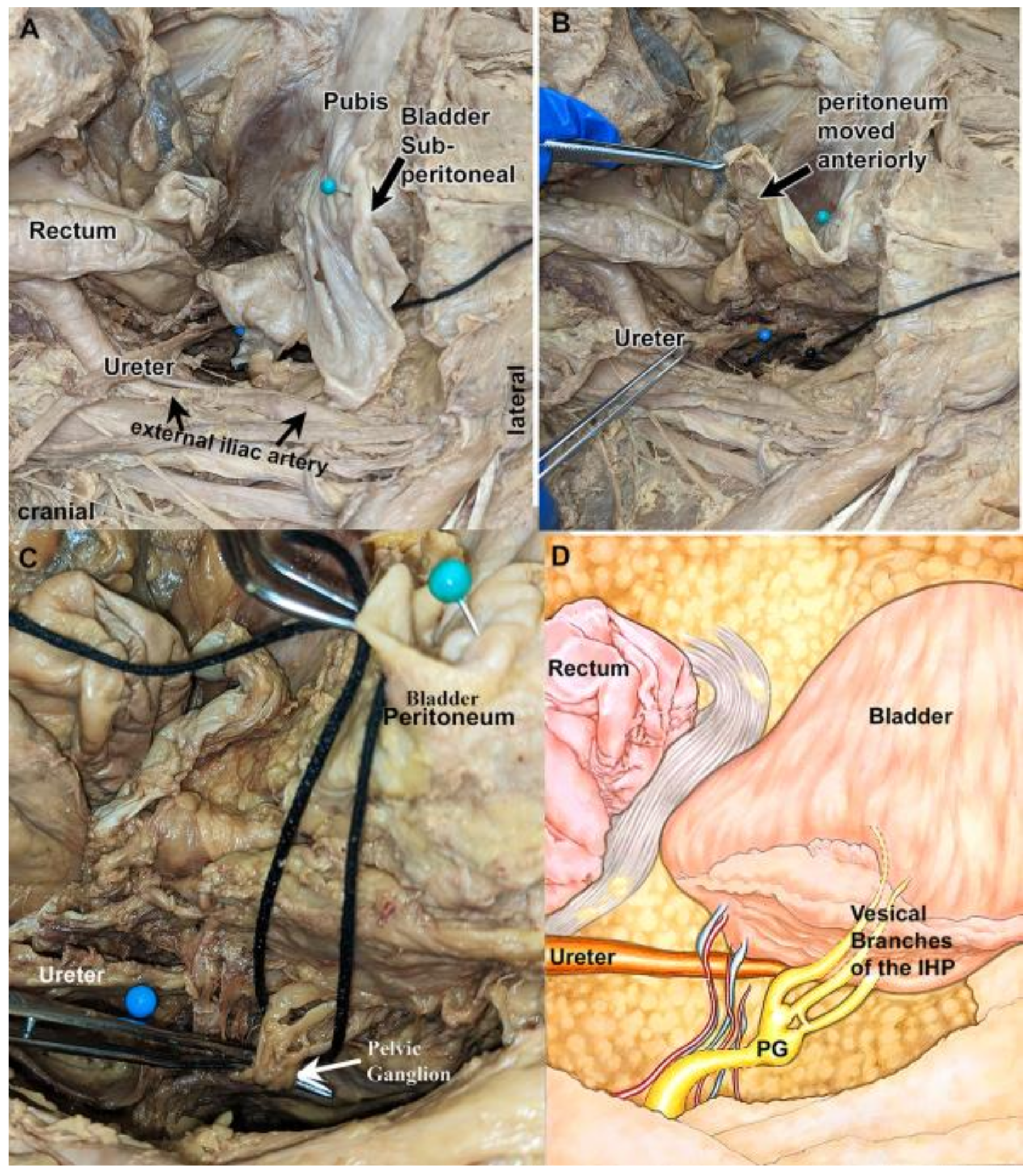
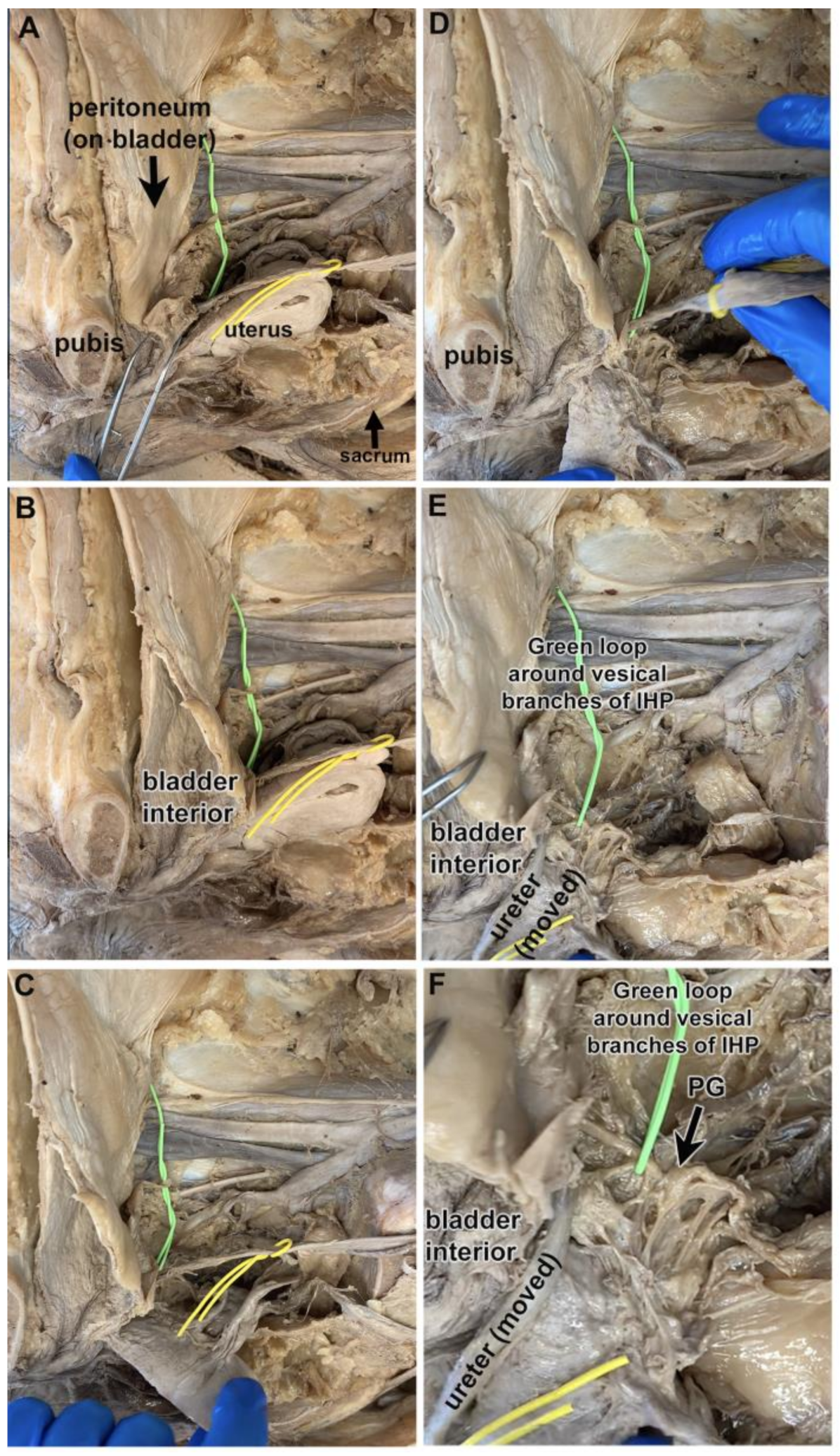
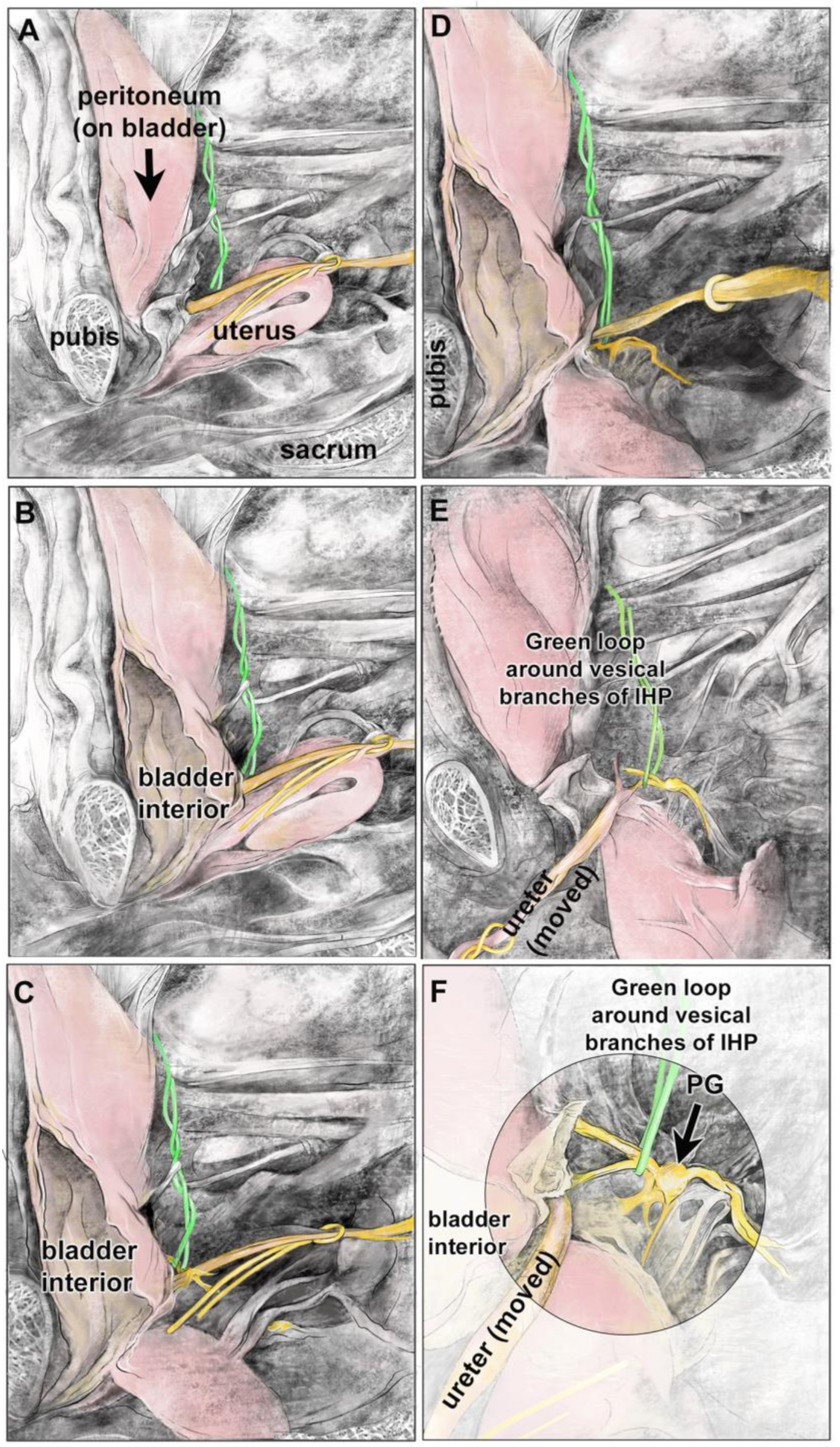
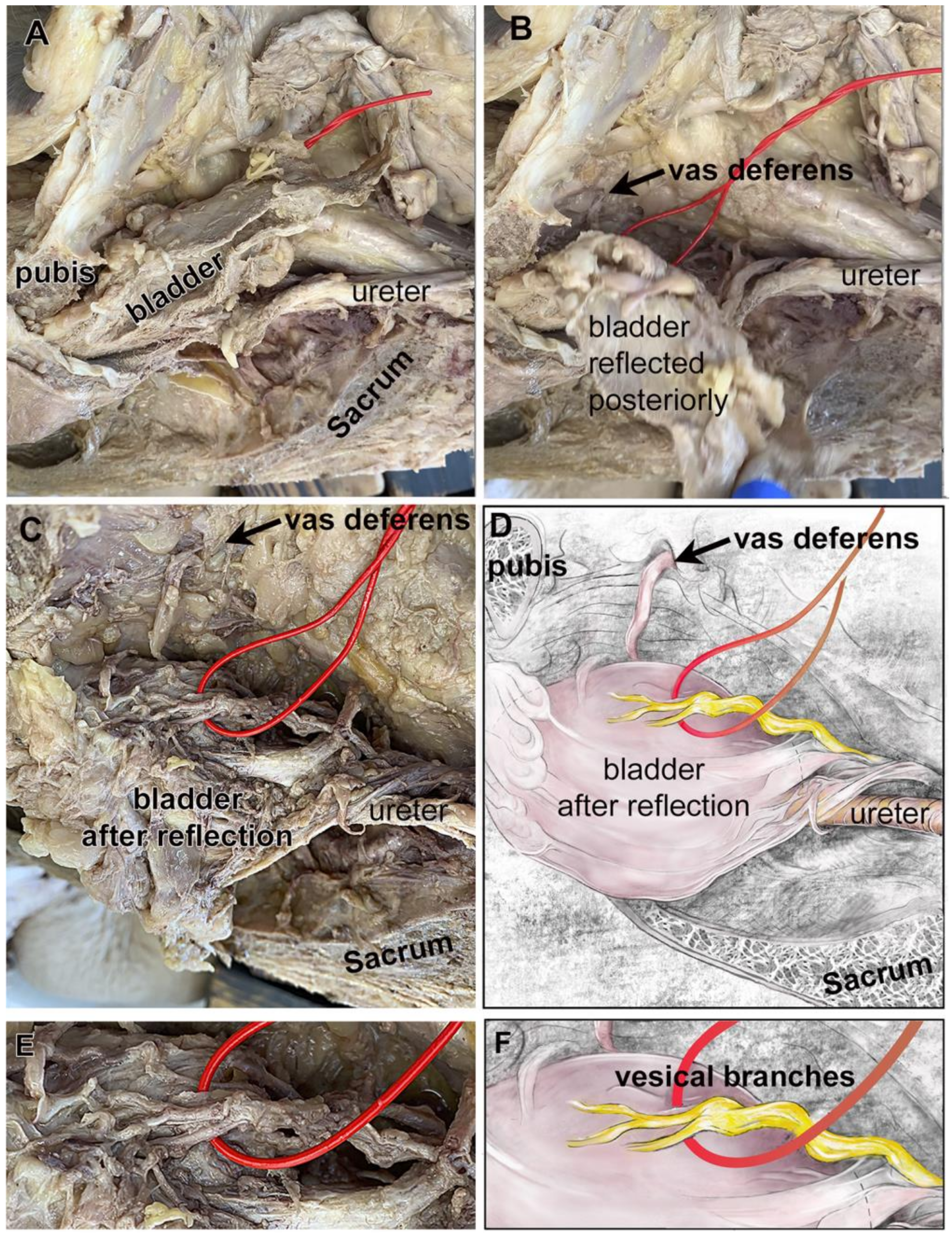
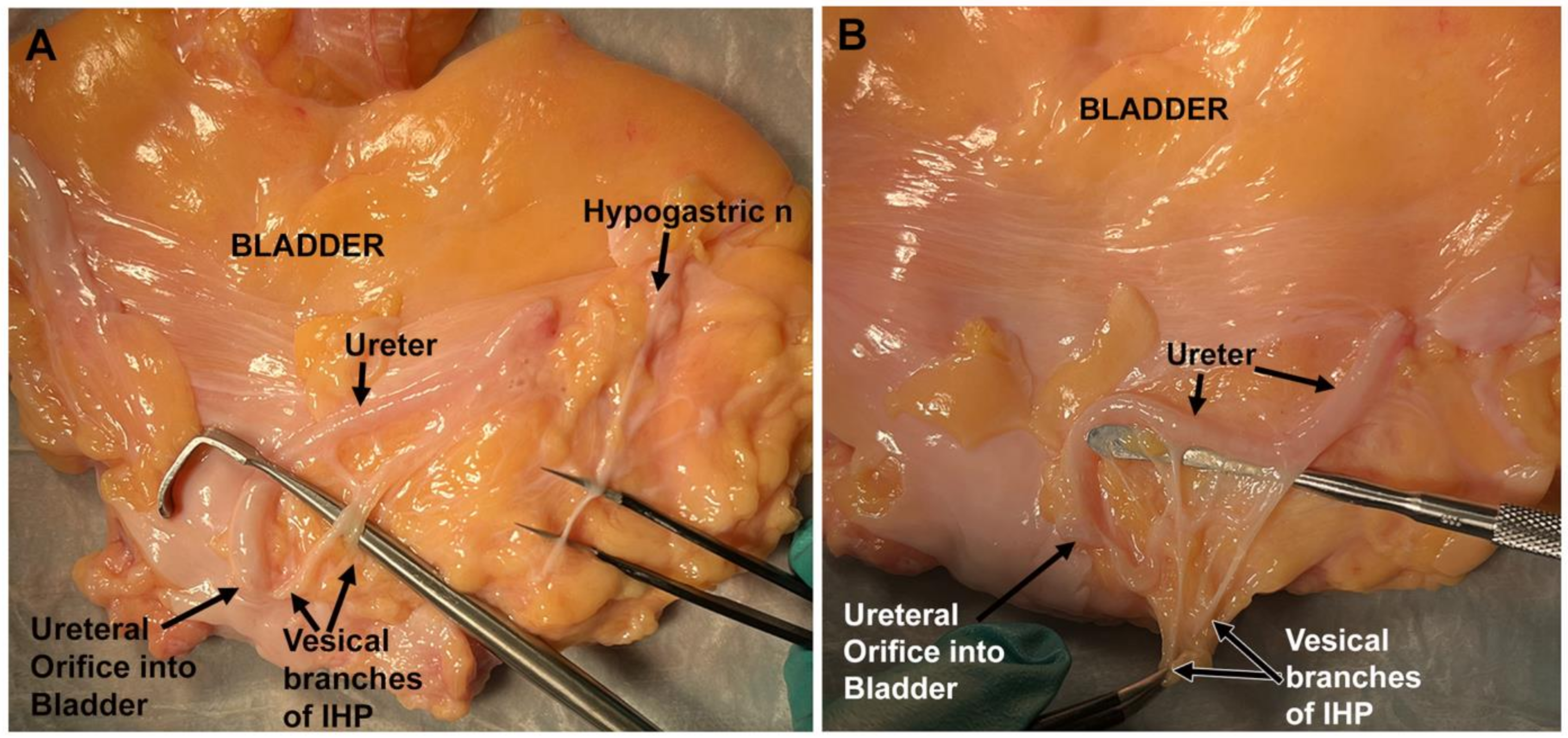
3.1. Vesical Nerves and Pelvic Ganglia Were Typically Located Posterolateral to the Ureteral Orifice
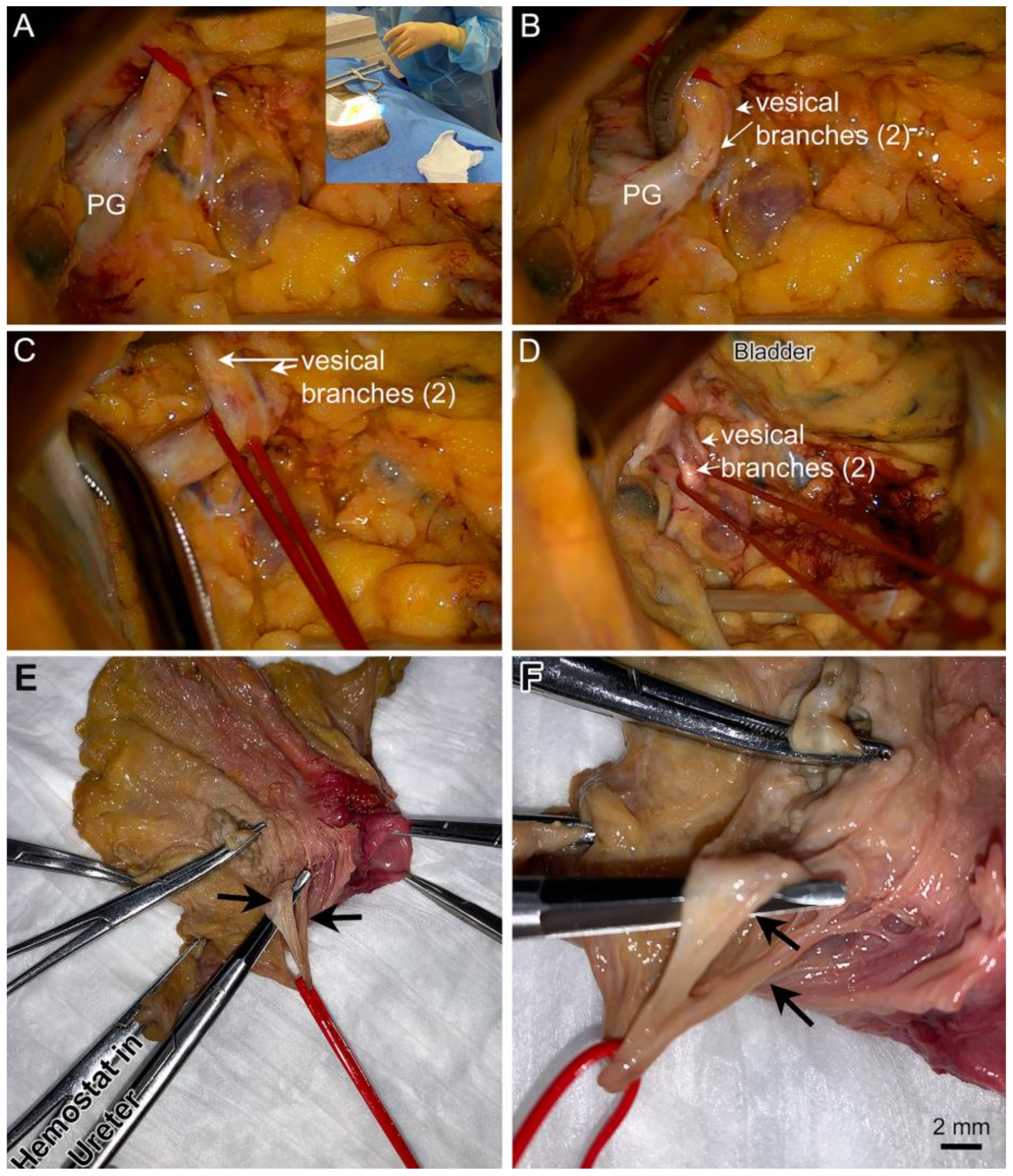
3.2. Most Cadavers Had Two Vesical Nerve Branches of the IHP
3.3. Vesical Branches of the IHP Typically Arose Distally from a Grossly Visible Pelvic Ganglion Located near the Ureteral Orifice
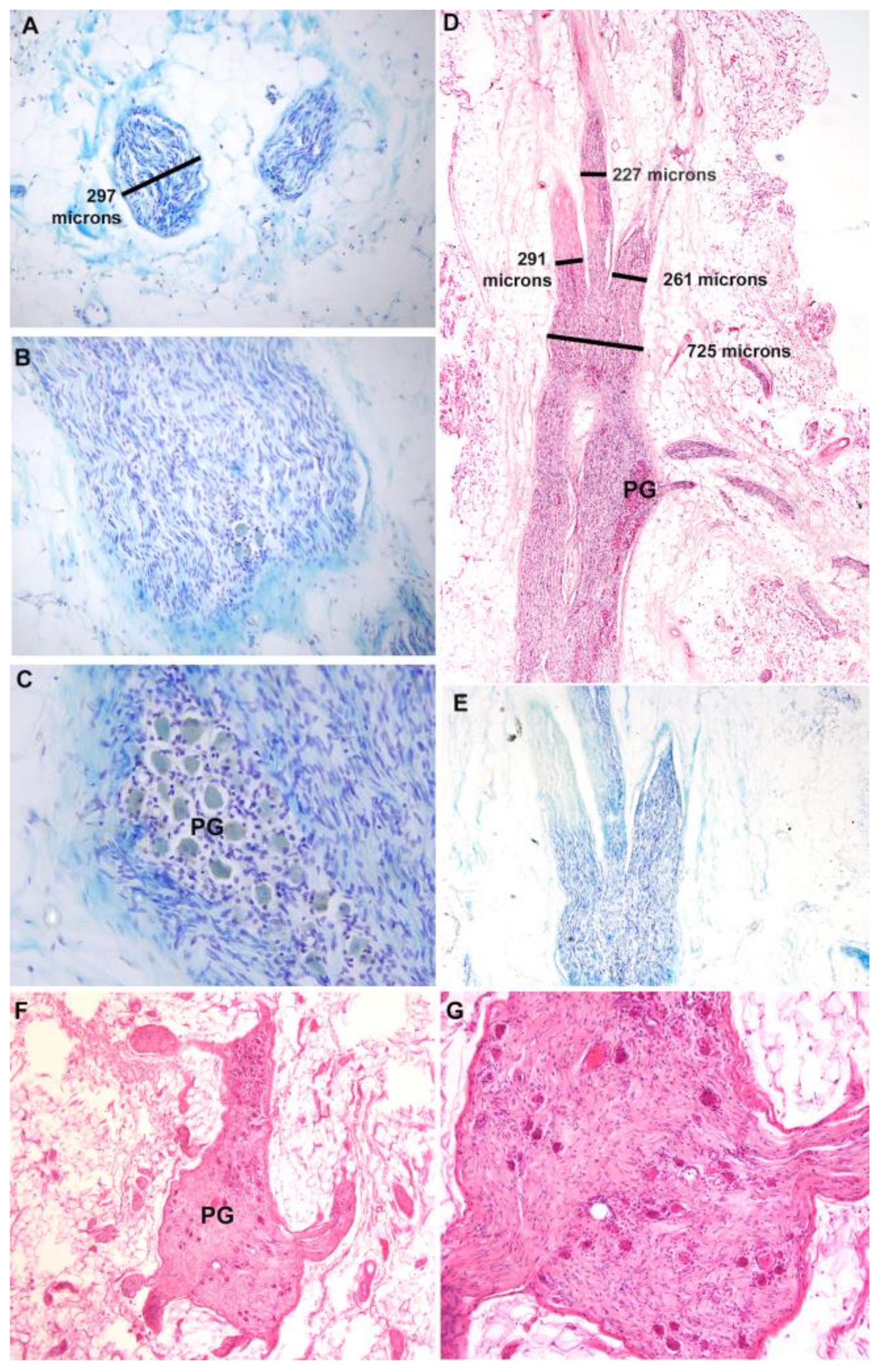
3.4. Histological Assessment of Vesical Branches and Pelvic Ganglion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taweel, W.A.; Seyam, R. Neurogenic bladder in spinal cord injury patients. Res. Rep. Urol. 2015, 7, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.D. Targeting recovery: Priorities of the spinal cord-injured population. J. Neurotrauma 2004, 21, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Nadelhaft, I.; de Groat, W.C. The distribution of visceral primary afferents from the pelvic nerve to Lissauer’s tract and the spinal gray matter and its relationship to the sacral parasympathetic nucleus. J. Comp. Neurol. 1981, 201, 415–440. [Google Scholar] [CrossRef] [PubMed]
- Rothlisberger, R.; Aurore, V.; Boemke, S.; Bangerter, H.; Bergmann, M.; Thalmann, G.N.; Djonov, V. The anatomy of the male inferior hypogastric plexus: What should we know for nerve sparing surgery. Clin. Anat. 2018, 31, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Mauroy, B.; Demondion, X.; Bizet, B.; Claret, A.; Mestdagh, P.; Hurt, C. The female inferior hypogastric (=pelvic) plexus: Anatomical and radiological description of the plexus and its afferences—Applications to pelvic surgery. Surg. Radiol. Anat. 2007, 29, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Stupart, D.; Pickles, K.; Briggs, C. Anatomy of the vesicovaginal fascia and its relation to branches of the inferior hypogastric plexus. Clin. Anat. 2022, 35, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I.; Wedel, T.; Pape, J.; Possover, M.; Dhanawat, J. Review: Pelvic nerves—From anatomy and physiology to clinical applications. Transl. Neurosci. 2021, 12, 362–378. [Google Scholar] [CrossRef] [PubMed]
- Sekiyama, K.; Fujii, S.; Mandai, M. Anatomical location of the surgically identifiable bladder branch of the inferior hypogastric plexus for nerve-sparing radical hysterectomy. Gynecol. Oncol. Rep. 2023, 46, 101152. [Google Scholar] [CrossRef]
- Goidescu, O.C.; Dogaru, I.A.; Enyedi, M.; Enciu, O.; Mutu, D.G.; Filipoiu, F.M. The Pelvic and Sacral Splanchnic Nerves—Identification by Dissection, Trajectory. Maedica 2022, 17, 571–575. [Google Scholar] [CrossRef]
- Kostov, S.; Kornovski, Y.; Yordanov, A.; Watrowski, R.; Slavchev, S.; Ivanova, Y.; Ganev, T.; Yalcin, H.; Selcuk, I. Surgical Anatomy and Dissection of the Hypogastric Plexus in Nerve-Sparing Radical Hysterectomy. Diagnostics 2023, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Goidescu, O.C.; Dogaru, I.A.; Badea, T.G.; Enyedi, M.; Enciu, O.; Gheoca Mutu, D.E.; Filipoiu, F.M. The distribution of the inferior hypogastric plexus in female pelvis. J. Med. Life 2022, 15, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.M.; Barbe, M.F.; Albo, M.E.; Lai, H.H.; Ruggieri, M.R., Sr. Anatomical feasibility of performing intercostal and ilioinguinal nerve to pelvic nerve transfer: A possible technique to restore lower urinary tract innervation. J. Neurosurg. Spine 2012, 17, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.M.; Barbe, M.F.; Albo, M.E.; Ruggieri, M.R., Sr. Anatomical feasibility of performing a nerve transfer from the femoral branch to bilateral pelvic nerves in a cadaver: A potential method to restore bladder function following proximal spinal cord injury. J. Neurosurg. Spine 2013, 18, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Floyd, K.; McMahon, S.B.; Morrison, J.F. Inhibitory interactions between the colonic and vesical branches of the pelvic nerve in the cat [proceedings]. J. Physiol. 1979, 290, 50P–51P. [Google Scholar] [PubMed]
- Lee, Y.H.; Kim, M.K.; Moon, H.Y.; Chong, G.O.; Lee, H.J.; Lee, Y.S.; Park, J.Y.; Lee, C.H.; Baek, M.C.; Hong, D.G. Proteomic Analysis of Pelvic Autonomic Nerve in Nerve-sparing Radical Hysterectomy for Cervical Carcinoma. Cancer Genom. Proteom. 2018, 15, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Jia, J.; Xiao, Y.; Kang, L.; Cui, H. Anatomical basis of female pelvic cavity for nerve sparing radical hysterectomy. Surg. Radiol. Anat. 2015, 37, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, M.M.; Alsaid, B.; Droupy, S.; Ripoche, J.; Benoit, G.; Adalian, P.; Brunet, C.; Piercecchi-Marti, M.D.; Prudhomme, M. Anatomical basis of the coordination between smooth and striated urethral and anal sphincters: Loops of regulation between inferior hypogastric plexus and pudendal nerve. Immuno-histological study with 3D reconstruction. Surg. Radiol. Anat. 2016, 38, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Mauroy, B.; Bizet, B.; Bonnal, J.L.; Crombet, T.; Duburcq, T.; Hurt, C. Systematization of the vesical and uterovaginal efferences of the female inferior hypogastric plexus (pelvic): Applications to pelvic surgery on women patients. Surg. Radiol. Anat. 2007, 29, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Z.; Masuko, S. Target specific organization and neuron types of the dog pelvic ganglia: A retrograde-tracing and immunohistochemical study. Arch. Histol. Cytol. 2001, 64, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Ragionieri, L.; Botti, M.; Gazza, F.; Sorteni, C.; Chiocchetti, R.; Clavenzani, P.; Minelli, L.B.; Panu, R. Localization of peripheral autonomic neurons innervating the boar urinary bladder trigone and neurochemical features of the sympathetic component. Eur. J. Histochem. 2013, 57, e16. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Amaya, S.M.; Barbe, M.F.; Brown, J.M.; Lamarre, N.S.; Braverman, A.S.; Massicotte, V.S.; Ruggieri, M.R., Sr. Bladder reinnervation using a primarily motor donor nerve (femoral nerve branches) is functionally superior to using a primarily sensory donor nerve (genitofemoral nerve). J. Urol. 2015, 193, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, M.R.; Braverman, A.S.; D’Andrea, L.; McCarthy, J.; Barbe, M.F. Functional reinnervation of the canine bladder after spinal root transection and immediate somatic nerve transfer. J. Neurotrauma 2008, 25, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, E.; Porreca, D.S.; Braverman, A.S.; Holt-Bright, L.; Frara, N.A.; Brown, J.M.; Johnston, B.R.; Bazarek, S.F.; Hilliard, B.A.; Mazzei, M.; et al. Nerve transfer for restoration of lower motor neuron-lesioned bladder, urethral and anal sphincter function. Part 4: Effectiveness of the motor reinnervation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.R.; Bazarek, S.; Sten, M.; McIntyre, B.S.; Fine, N.; De, E.J.B.; McGovern, F.; Lemos, N.; Ruggieri, M.R.; Barbe, M.F.; et al. Restoring bladder function using motor and sensory nerve transfers: A cadaveric feasibility study. J. Neurosurg. Spine 2023, 38, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Wang, S.; Li, P.; Xue, Y.; Wang, H. Transplantation of obturator nerve to repair pelvic splanchnic nerve in the treatment of urination disorder caused by traumatic sacral plexus injury. Chin. J. Orthop. 2019, 5, 278–283. [Google Scholar]
- Aurore, V.; Rothlisberger, R.; Boemke, N.; Hlushchuk, R.; Bangerter, H.; Bergmann, M.; Imboden, S.; Mueller, M.D.; Eppler, E.; Djonov, V. Anatomy of the female pelvic nerves: A macroscopic study of the hypogastric plexus and their relations and variations. J. Anat. 2020, 237, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Ripperda, C.M.; Jackson, L.A.; Phelan, J.N.; Carrick, K.S.; Corton, M.M. Anatomic relationships of the pelvic autonomic nervous system in female cadavers: Clinical applications to pelvic surgery. Am. J. Obstet. Gynecol. 2017, 216, 388.e1–388.e7. [Google Scholar] [CrossRef]
- Zakhari, A.; Mabrouk, M.; Raimondo, D.; Mastronardi, M.; Seracchioli, R.; Mattei, B.; Papillon-Smith, J.; Solnik, M.J.; Murji, A.; Lemos, N. Keep Your Landmarks Close and the Hypogastric Nerve Closer: An Approach to Nerve-sparing Endometriosis Surgery. J. Minim. Invasive Gynecol. 2020, 27, 813–814. [Google Scholar] [CrossRef] [PubMed]
- Puntambekar, S.P.; Venkateswaran, S.; Naidu, S.; Parulekar, M.; Patil, M.; Inampudi, S.; Chitale, M.; Bharambe, S.; Puntambekar, A.; Manerikar, K.; et al. Endometriosis Resection Using Nerve Sparing Versus Non-nerve Sparing Surgical Techniques. J. Obstet. Gynaecol. India 2023, 73, 421–427. [Google Scholar] [CrossRef] [PubMed]
- U.S. Health and Human Services. Guidance Regarding Methods for De-identification of Protected Health Information in Accordance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. Health Information Privacy 2022. Available online: https://www.hhs.gov/hipaa/for-professionals/privacy/special-topics/de-identification/index.html (accessed on 26 March 2024).
- U.S. Department of Health and Human Services. Exemptions (2018 Requirements). Office for Human Research Protection 2018. Available online: https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/common-rule-subpart-a-46104/index.html (accessed on 26 March 2024).
- National Institute of Health. Definition of Human Subjects Research. Policy & Compliance, Human Subjects Research—Home Page 2019. Available online: https://grants.nih.gov/policy/humansubjects.htm (accessed on 2 December 2019).
- Liao, P.Y.; Wang, Z.G. Thiel-embalming technique: Investigation of possible modification in embalming tissue as evaluation model for radiofrequency ablation. J. Biomed. Res. 2019, 33, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Lemos, N.; Souza, C.; Marques, R.M.; Kamergorodsky, G.; Schor, E.; Girao, M.J. Laparoscopic anatomy of the autonomic nerves of the pelvis and the concept of nerve-sparing surgery by direct visualization of autonomic nerve bundles. Fertil. Steril. 2015, 104, e11–e12. [Google Scholar] [CrossRef] [PubMed]
- Carriel, V.; Campos, A.; Alaminos, M.; Raimondo, S.; Geuna, S. Staining Methods for Normal and Regenerative Myelin in the Nervous System. Methods Mol. Biol. 2017, 1560, 207–218. [Google Scholar] [CrossRef] [PubMed]
- National Spinal Cord Injury Statistical Center. Spinal Cord Injury Facts and Figures at a Glance. Available online: www.nscisc.uab.edu (accessed on 13 June 2023).
- Simpson, L.A.; Eng, J.J.; Hsieh, J.T.; Wolfe, D.L.; Spinal Cord Injury Rehabilitation Evidence Scire Research, T. The health and life priorities of individuals with spinal cord injury: A systematic review. J. Neurotrauma 2012, 29, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Amaya, S.M.; Barbe, M.F.; de Groat, W.C.; Brown, J.M.; Tuite, G.F.; Corcos, J.; Fecho, S.B.; Braverman, A.S.; Ruggieri, M.R., Sr. Neural reconstruction methods of restoring bladder function. Nat. Rev. Urol. 2015, 12, 100–118. [Google Scholar] [CrossRef] [PubMed]
- Livshits, A.; Catz, A.; Folman, Y.; Witz, M.; Livshits, V.; Baskov, A.; Gepstein, R. Reinnervation of the neurogenic bladder in the late period of the spinal cord trauma. Spinal Cord 2004, 42, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Koopman, J.E.; Duraku, L.S.; de Jong, T.; de Vries, R.B.M.; Michiel Zuidam, J.; Hundepool, C.A. A systematic review and meta-analysis on the use of fibrin glue in peripheral nerve repair: Can we just glue it? J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 1018–1033. [Google Scholar] [CrossRef] [PubMed]
- Sameem, M.; Wood, T.J.; Bain, J.R. A systematic review on the use of fibrin glue for peripheral nerve repair. Plast. Reconstr. Surg. 2011, 127, 2381–2390. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.Z.; Chang, J.; Hawasli, A.; Wilson, T.J.; Yang, L. Motor Nerve Transfers: A Comprehensive Review. Neurosurgery 2016, 78, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.B.; Murray, P.M. Heterotopic nerve transfers: Recent trends with expanding indication. J. Hand Surg. 2007, 32, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Cosma, S.; Ferraioli, D.; Carosso, A.; Ceccaroni, M.; Benedetto, C. A Fascial Reinterpretation of the Classical Female Pelvic Surgical Anatomy: Seeing Things from a Different Angle. J. Minim. Invasive Gynecol. 2021, 28, 940–941. [Google Scholar] [CrossRef] [PubMed]
- Cosma, S.; Ferraioli, D.; Mitidieri, M.; Ceccaroni, M.; Zola, P.; Micheletti, L.; Benedetto, C. A simplified fascial model of pelvic anatomical surgery: Going beyond parametrium-centered surgical anatomy. Anat. Sci. Int. 2021, 96, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Bae, J.W.; Han, M.; Cho, Y.J.; Park, J.W.; Oh, S.R.; Kim, S.J.; Choe, S.Y.; Yun, J.H.; Lee, Y. Efficacy of nerve-sparing radical hysterectomy vs. conventional radical hysterectomy in early-stage cervical cancer: A systematic review and meta-analysis. Mol. Clin. Oncol. 2020, 12, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Furuya, K.; Kawada, M.; Kinugasa, Y.; Omote, K.; Namiki, A.; Uchiyama, E.; Murakami, G. Human pelvic extramural ganglion cells: A semiquantitative and immunohistochemical study. Surg. Radiol. Anat. 2006, 28, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Morino, M.; Rimonda, R.; Allaix, M.E.; Giraudo, G.; Garrone, C. Ultrasonic versus standard electric dissection in laparoscopic colorectal surgery: A prospective randomized clinical trial. Ann. Surg. 2005, 242, 897–901, discussion 901. [Google Scholar] [CrossRef] [PubMed]
- Verlinden, T.J.M.; Lamers, W.H.; Herrler, A.; Kohler, S.E. The differences in the anatomy of the thoracolumbar and sacral autonomic outflow are quantitative. Clin. Auton. Res. 2024, 34, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Kinugasa, Y.; Arakawa, T.; Murakami, G.; Fujimiya, M.; Sugihara, K. Nerve supply to the internal anal sphincter differs from that to the distal rectum: An immunohistochemical study of cadavers. Int. J. Colorectal. Dis. 2014, 29, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, A.; Kawada, M.; Murakami, G.; Hisasue, S.; Tsukamoto, T.; Fujisawa, M. Interindividual variation in distribution of extramural ganglion cells in the male pelvis: A semi-quantitative and immunohistochemical study concerning nerve-sparing pelvic surgery. Eur. Urol. 2005, 48, 46–52, discussion 52. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.S.; Jen, P.Y.; Gosling, J.A. Immunohistochemical characteristics of human paraganglion cells and sensory corpuscles associated with the urinary bladder. A developmental study in the male fetus, neonate and infant. J. Anat. 1998, 192 Pt 3, 407–415. [Google Scholar] [CrossRef]
- Jen, P.Y.; Dixon, J.S.; Gosling, J.A. Co-localisation of tyrosine hydroxylase, nitric oxide synthase and neuropeptides in neurons of the human postnatal male pelvic ganglia. J. Auton. Nerv. Syst. 1996, 59, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Exemption_Infographic_v8_508c_1-15-2020. 2020. Available online: https://grants.nih.gov/sites/default/files/exemption_infographic_v8_508c_1-15-2020.pdf (accessed on 13 June 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cadaver Number | Vesical Branch(es) and PG Location Relative to Ureteral Orifice | # Vesical Branches of the IHP | Distance of PG to Ureteral Orifice (mm) | PG Diameter (mm) | ||||
|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | Right | Left | |
| 1 | Posterolateral | NA | 2 | NA | 6.19 | NA | 3.94 | NA |
| 2 | Posterolateral | Posterolateral | 2 | NA | 10 | NA | 2 | NA |
| 3 | Posterolateral | NA | 3 | NA | 18 | NA | 8 | NA |
| 4 | Posterolateral | Posterolateral | 3 | 2 | 0.4 | 6 | 5 | 4.5 |
| 5 | Posterolateral | Lateral (3.6 cm cranially on ureter) | 2 | 4 | 2 | 5 | 3.50 | 4.20 |
| 6 | NA | Lateral (overlying ureter) | NA | 4 | NA | 5 | NA | 4.5 mm |
| 7 | Posterolateral | Posterolateral | 3 | 3 (2 large, 1 small) | 5 | 10 | 1 mm: several grouped ganglia | 2 |
| 8 | Posterolateral | Posterolateral | 2 from PG; 2 non-ganglionic derived branches | 1 | 1 | 13 | 3.5 | 2 and 2.3 |
| 9 | Overlying (on ureteral entrance) | Overlying (on ureteral entrance) | 2 (1 large, 1 very small) | 3 | 0 | 0 | 3 | 3.4 |
| 10 | Posterolateral | NA | 2 | NA | 2 | NA | 2 | NA |
| 11 | Posterolateral | Posterior (near colon) | 2 | 2 | 5 | 15 | 3 | 3.3 |
| 12 | NA (none remaining) | Main: posterolateral; 2nd: anterior to ureter | NA | 1 from main ganglion | NA | Both 2 | NA | 3.1 |
| 13 | Posterolateral | Posterolateral | 2 | 2 | 2 | 12 | 30 (excluded) | 2 |
| 14 | NA | Overlying | NA | 2 | NA | 0 | NA | 2.5 |
| 15 | NA | Overlying | NA | 2 | NA | 0 | NA | 2 |
| 16 | NA | Anterolateral | NA | 4 (1 large, 1 medium, and 2 small) | NA | 7 | NA | 10.5 |
| 17 | Posterolateral | NA | 2 | NA | 5 | NA | 5.5 | NA |
| 18 | NA | NA | NA | NA | NA | NA | NA | NA |
| 19 | Posterolateral | Posterolateral | 4 | 2 | 11 | 12 | 3.5 | 3 |
| 20 | Posterolateral | NA | 2 | NA | NA | NA | 3 | NA |
| 21 | Posterolateral | Posterolateral | 2 | 2 | NA | NA | 8.5 | 6 |
| 22 | Immediately posterior | Posterolateral | 3 | 2 | 0.4 | 6 mm | NA | NA |
| 23 | Posterolateral | Posterolateral | 2 | 2 | NA | NA | 3 | 4 |
| 24 | Posterolateral | Posterolateral | 3 | 2 | NA | NA | 2.5 | 3 |
| 25 | Posterolateral | NA | 2 | NA | NA | NA | 6 | NA |
| 26 | Posterolateral | NA | 2 (1 large, 1 small) | NA | NA | NA | 2.1 | NA |
| 27 | Posterolateral | NA | 2 | NA | NA | NA | NA | |
| 28 | NA | NA | 2 | 2 | NA | NA | NA | NA |
| 29 | Posterolateral | 1 | 3 | 2 | 2 | 1.5 | ||
| 30 | Posterolateral | Posterolateral | 2 | 2.5 | NA | 1.5 | NA | |
| Mean ± SD by side | 22/23 (96%) right sides showed posterolateral location | 7/19 (63%) left sides showed a posterolateral location | 2.3 ± 0.6 | 2.4 ± 0.9 | 7.44 ± 7.02 mm | 6.75 ± 5.17 mm | 3.94 ± 2.14 mm | 3.75 ± 2.28 mm |
| Overall ± SD | 29/42 (69%) cadaveric sides showed a posterolateral location for vesical branches | 2.33 ± 0.72 | 7.11 ± 6.11 | 3.8 ± 2.05 | ||||
| # Vesical Branches from Right PG | # Vesical Branches from Left PG | Right PG Location Relative to Ureteral Orifice | Right PG: Distance to Ureteral Orifice | Left PG Location Relative to Ureteral Orifice | Left PG: Distance to Ureteral Orifice | Right PG Diameter | Left PG Diameter | |
|---|---|---|---|---|---|---|---|---|
| Female n = 18 | 2.4 ± 0.6 | 2.1 ± 0.7 | 14/15 posterolateral | 7.9 ± 7.3 mm | 10/14 posterolateral | 7.9 ± 5.3 mm | 3.5 ± 1.8 mm | 3.2 ± 1.3 mm |
| Male n = 11 | 2.1 ± 0.4 | 3.0 ± 1.4 | 6/7 posterolateral | 6.2 ± 7.0 mm | 2/5 posterolateral | 3.5 ± 3.1 mm | 4.7 ± 2.2 mm | 5.4 ± 3.5 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Day, E.P.; Johnston, B.R.; Bazarek, S.F.; Brown, J.M.; Lemos, N.; Gibson, E.I.; Hurban, H.N.; Fecho, S.B.; Holt-Bright, L.; Eun, D.D.; et al. Anatomical Location of the Vesical Branches of the Inferior Hypogastric Plexus in Human Cadavers. Diagnostics 2024, 14, 794. https://doi.org/10.3390/diagnostics14080794
Day EP, Johnston BR, Bazarek SF, Brown JM, Lemos N, Gibson EI, Hurban HN, Fecho SB, Holt-Bright L, Eun DD, et al. Anatomical Location of the Vesical Branches of the Inferior Hypogastric Plexus in Human Cadavers. Diagnostics. 2024; 14(8):794. https://doi.org/10.3390/diagnostics14080794
Chicago/Turabian StyleDay, Emily P., Benjamin R. Johnston, Stanley F. Bazarek, Justin M. Brown, Nucelio Lemos, Eve I. Gibson, Helaina N. Hurban, Susan B. Fecho, Lewis Holt-Bright, Daniel D. Eun, and et al. 2024. "Anatomical Location of the Vesical Branches of the Inferior Hypogastric Plexus in Human Cadavers" Diagnostics 14, no. 8: 794. https://doi.org/10.3390/diagnostics14080794
APA StyleDay, E. P., Johnston, B. R., Bazarek, S. F., Brown, J. M., Lemos, N., Gibson, E. I., Hurban, H. N., Fecho, S. B., Holt-Bright, L., Eun, D. D., Pontari, M. A., De, E. J., McGovern, F. J., Ruggieri, M. R., & Barbe, M. F. (2024). Anatomical Location of the Vesical Branches of the Inferior Hypogastric Plexus in Human Cadavers. Diagnostics, 14(8), 794. https://doi.org/10.3390/diagnostics14080794