
Carbohydrate Antigen 125 (CA 125): A Novel Biomarker in Acute Heart Failure
 , ,
, ,
Abstract
1. Introduction
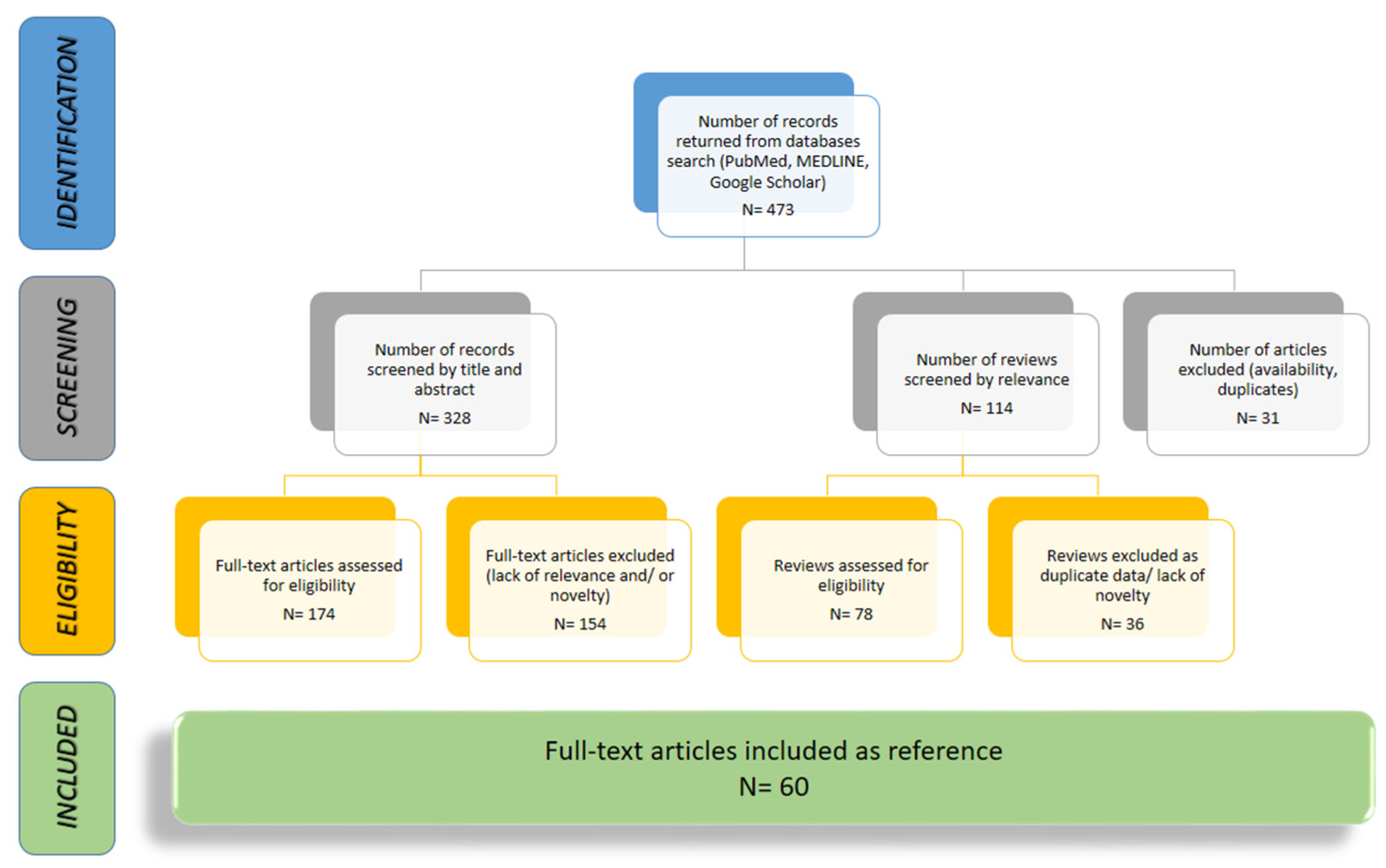
2. Methodology
3. Results
3.1. CA 125 and Congestion in Heart Failure
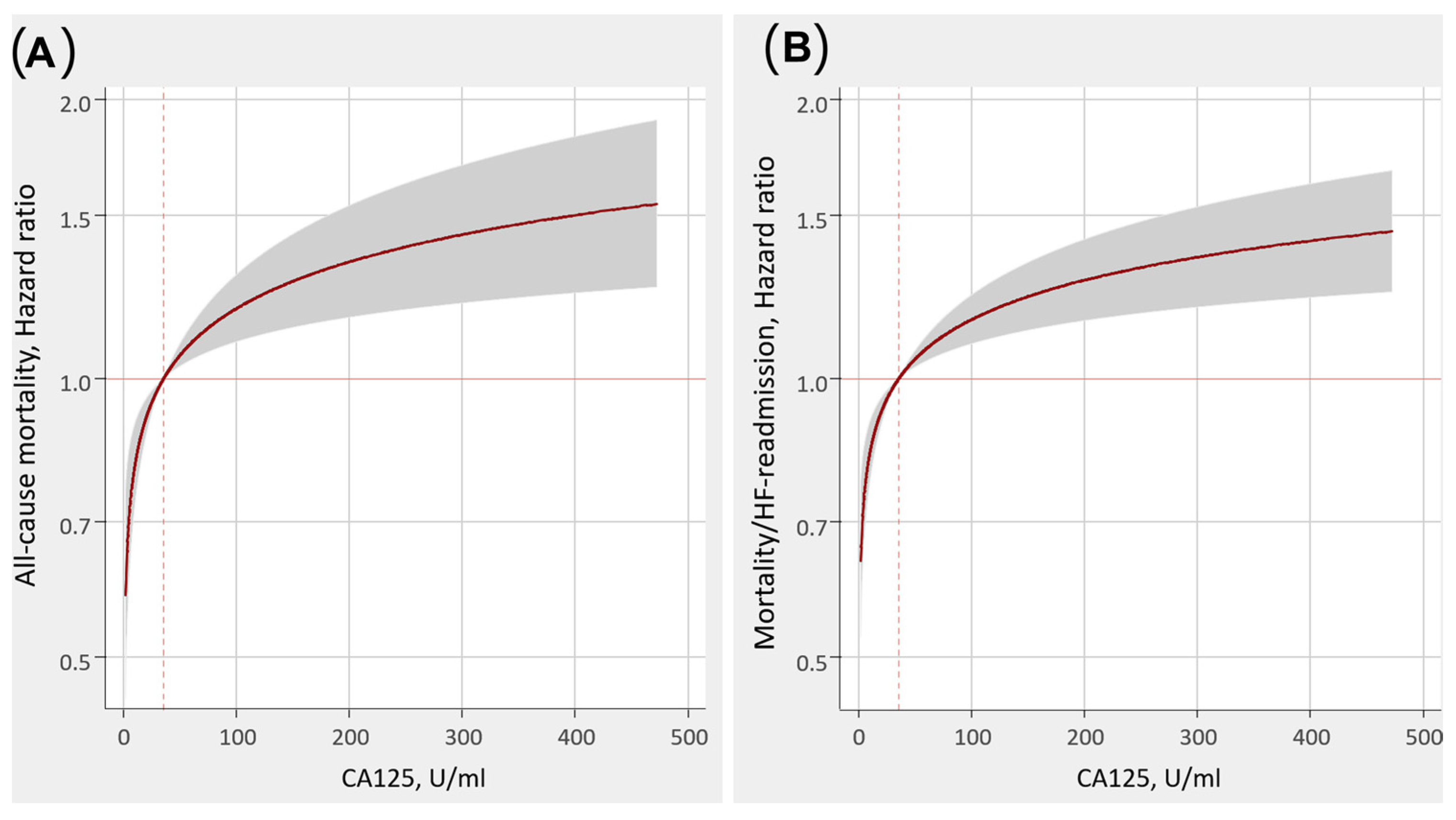
3.2. CA 125 and Risk Stratification in Heart Failure
3.3. CA 125 Use in Guiding Heart Failure Therapy
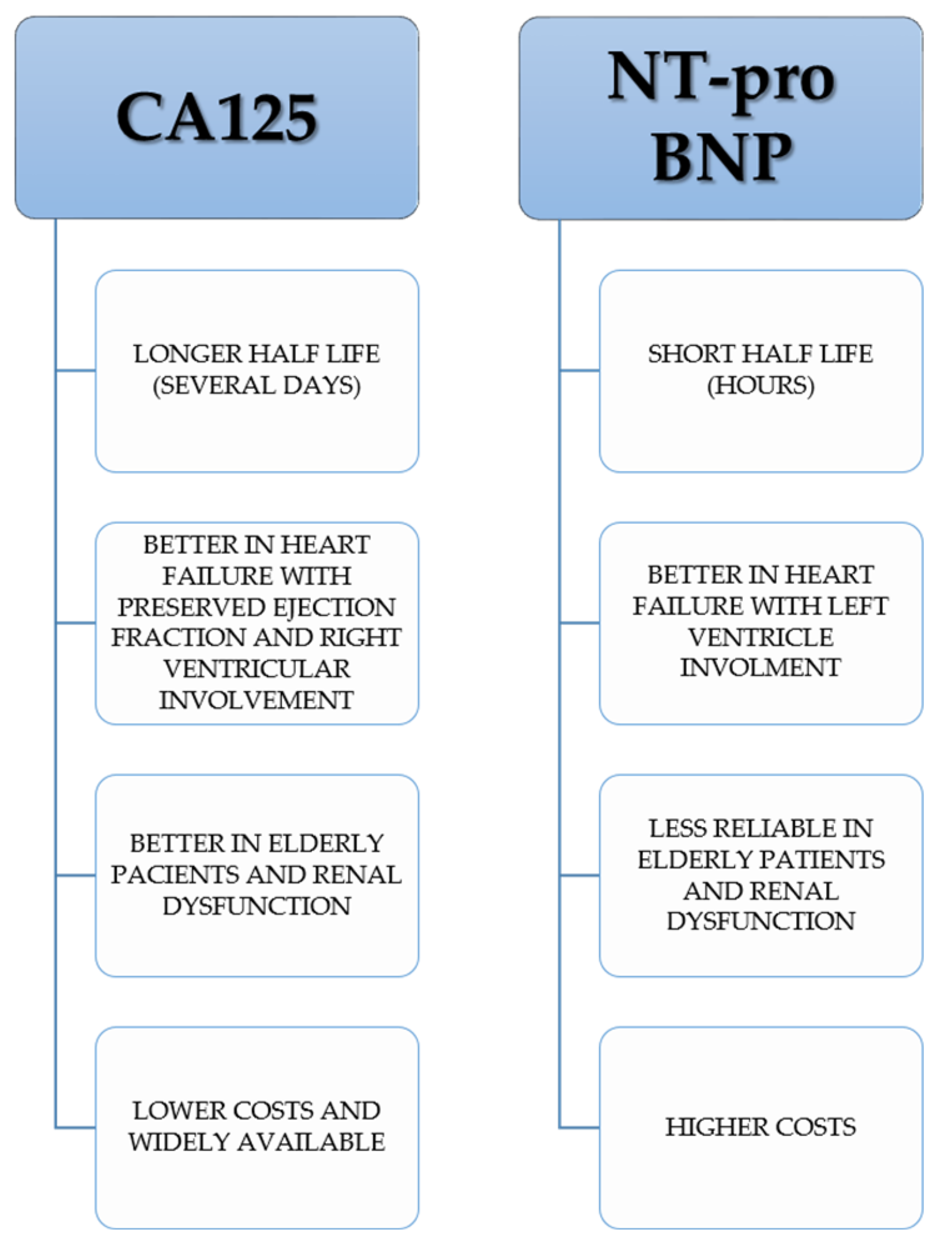
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hollenberg, S.M.; Warner Stevenson, L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Peterson, P.N.; et al. 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized with Heart Failure: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2019, 74, 1966–2011, Erratum in: J. Am. Coll. Cardiol. 2020, 75, 132. . [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.K.; Pocock, S.J.; McMurray, J.J.; Granger, C.B.; Michelson, E.L.; Östergren, J.; Pfeffer, M.A.; Solomon, S.D.; Swedberg, K.; Yusuf, S. Analysing recurrent hospitalizations in heart failure: A review of statistical methodology, with application to CHARM-Preserved. Eur. J. Heart Fail. 2014, 16, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Zhang, P.; Hu, H. Serum Levels of Hcy, sST2 and CA-125 in CHF Patients and Their Correlation with Cardiac Function Classification. Heart Surg. Forum. 2023, 26, E449–E454. [Google Scholar] [CrossRef] [PubMed]
- Pandhi, P.; Ter Maaten, J.M.; Anker, S.D.; Ng, L.L.; Metra, M.; Samani, N.J.; Lang, C.C.; Dickstein, K.; de Boer, R.A.; van Veldhuisen, D.J.; et al. Pathophysiologic Processes and Novel Biomarkers Associated with Congestion in Heart Failure. JACC Heart Fail. 2022, 10, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Santas, E.; Palau, P.; Bayés-Ge, A.; Núñez, J. The emerging role of carbohydrate antigen 125 in heart failure. Biomark. Med. 2020, 14, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.; Zhang, Z.; Fan, Q. Carbohydrate antigen 125 in congestive heart failure: Ready for clinical application? Front. Oncol. 2023, 13, 1161723. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Chen, J.; Liu, Y.; Zhang, K.; Wang, J.; Huang, H. New mechanism of elevated CA125 in heart failure: The mechanical stress and inflammatory stimuli initiate CA125 synthesis. Med. Hypotheses 2012, 79, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Zang, R.; Lu, Z.; Zhang, G.; Huang, J.; Liu, C.; Wang, Z.; Mao, S.; Che, Y.; Wang, X.; et al. ERO1L promotes IL6/sIL6R signaling and regulates MUC16 expression to promote CA125 secretion and the metastasis of lung cancer cells. Cell Death Dis. 2020, 11, 853. [Google Scholar] [CrossRef] [PubMed]
- Scholler, N.; Urban, N. CA125 in ovarian cancer. Biomark. Med. 2007, 1, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, K.O.; Yin, B.W. Synthesis and secretion of the ovarian cancer antigen CA 125 by the human cancer cell line NIH:OVCAR-3. Tumour Biol. 2001, 22, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Bottoni, P.; Scatena, R. The Role of CA 125 as Tumor Marker: Biochemical and Clinical Aspects. Adv. Exp. Med. Biol. 2015, 867, 229–244. [Google Scholar] [CrossRef] [PubMed]
- Miralles, C.; Orea, M.; España, P.; Provencio, M.; Sánchez, A.; Cantos, B.; Cubedo, R.; Carcereny, E.; Bonilla, F.; Gea, T. Cancer antigen 125 associated with multiple benign and malignant pathologies. Ann. Surg. Oncol. 2003, 10, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Miñana, G.; Núñez, E.; Chorro, F.J.; Bodí, V.; Sanchis, J. Clinical utility of antigen carbohydrate 125 in heart failure. Heart Fail. Rev. 2014, 19, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Llàcer, P.; Bayés-Genís, A.; Núñez, J. Carbohydrate antigen 125 in heart failure. New era in the monitoring and control of treatment. Med. Clin. 2019, 152, 266–273, (In English, Spanish). [Google Scholar] [CrossRef] [PubMed]
- Topalak, O.; Saygili, U.; Soyturk, M.; Karaca, N.; Batur, Y.; Uslu, T.; Erten, O. Serum, pleural effusion, and ascites CA-125 levels in ovarian cancer and nonovarian benign and malignant diseases: A comparative study. Gynecol. Oncol. 2002, 85, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Zeillemaker, A.M.; Verbrugh, H.A.; Hoynck van Papendrecht, A.A.; Leguit, P. CA 125 secretion by peritoneal mesothelial cells. J. Clin. Pathol. 1994, 47, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Bulska-Będkowska, W.; Chełmecka, E.; Owczarek, A.J.; Mizia-Stec, K.; Witek, A.; Szybalska, A.; Grodzicki, T.; Olszanecka-Glinianowicz, M.; Chudek, J. CA125 as a Marker of Heart Failure in the Older Women: Population-Based Analysis. J. Clin. Med. 2019, 8, 607. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Rabinovich, G.A.; Sandino, J.; Mainar, L.; Palau, P.; Santas, E.; Villanueva, M.P.; Núñez, E.; Bodí, V.; Chorro, F.J.; et al. Prognostic value of the interaction between galectin-3 and antigen carbohydrate 125 in acute heart failure. PLoS ONE 2015, 10, e0122360. [Google Scholar] [CrossRef] [PubMed]
- Nägele, H.; Bahlo, M.; Klapdor, R.; Schaeperkoetter, D.; Rödiger, W. CA 125 and its relation to cardiac function. Am. Heart J. 1999, 137, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Núñez, E.; Consuegra, L.; Sanchis, J.; Bodí, V.; Martínez-Brotons, A.; Bertomeu-González, V.; Robles, R.; Bosch, M.J.; Fácila, L.; et al. Carbohydrate antigen 125: An emerging prognostic risk factor in acute heart failure? Heart 2007, 93, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Miñana, G.; González, M.; Garcia-Ramón, R.; Sanchis, J.; Bodí, V.; Núñez, E.; Chorro, F.J.; Llàcer, A.; Miguel, A. Antigen carbohydrate 125 in heart failure: Not just a surrogate for serosal effusions? Int J Cardiol. 2011, 146, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Miñana, G.; Núñez, J.; Sanchis, J.; Bodí, V.; Núñez, E.; Llàcer, A. CA125 and immunoinflammatory activity in acute heart failure. Int. J. Cardiol. 2010, 145, 547–548. [Google Scholar] [CrossRef] [PubMed]
- Colombo, P.C.; Onat, D.; Harxhi, A.; Demmer, R.T.; Hayashi, Y.; Jelic, S.; LeJemtel, T.H.; Bucciarelli, L.; Kebschull, M.; Papapanou, P.; et al. Peripheral venous congestion causes inflammation, neurohormonal, and endothelial cell activation. Eur. Heart J. 2014, 35, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.P.; Kakkar, R.; McCarthy, C.P.; Januzzi, J.L., Jr. Inflammation in Heart Failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 1324–1340. [Google Scholar] [CrossRef] [PubMed]
- Duman, D.; Palit, F.; Simsek, E.; Bilgehan, K. Serum carbohydrate antigen 125 levels in advanced heart failure: Relation to B-type natriuretic peptide and left atrial volume. Eur. J. Heart Fail. 2008, 10, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Kouris, N.T.; Zacharos, I.D.; Kontogianni, D.D.; Goranitou, G.S.; Sifaki, M.D.; Grassos, H.E.; Kalkandi, E.M.; Babalis, D.K. The significance of CA125 levels in patients with chronic congestive heart failure. Correlation with clinical and echocardiographic parameters. Eur. J. Heart Fail. 2005, 7, 199–203. [Google Scholar] [CrossRef] [PubMed]
- D’Aloia, A.; Faggiano, P.; Aurigemma, G.; Bontempi, L.; Ruggeri, G.; Metra, M.; Nodari, S.; Dei Cas, L. Serum levels of carbohydrate antigen 125 in patients with chronic heart failure: Relation to clinical severity, hemodynamic and Doppler echocardiographic abnormalities, and short-term prognosis. J. Am. Coll. Cardiol. 2003, 41, 1805–1811. [Google Scholar] [CrossRef] [PubMed]
- Vizzardi, E.; D’Aloia, A.; Curnis, A.; Dei Cas, L. Carbohydrate antigen 125: A new biomarker in heart failure. Cardiol. Rev. 2013, 21, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Llàcer, P.; García-Blas, S.; Bonanad, C.; Ventura, S.; Núñez, J.M.; Sánchez, R.; Fácila, L.; de la Espriella, R.; Vaquer, J.M.; et al. CA125-Guided Diuretic Treatment Versus Usual Care in Patients with Acute Heart Failure and Renal Dysfunction. Am. J. Med. 2020, 133, 370–380.e4. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Bayés-Genís, A.; Revuelta-López, E.; Ter Maaten, J.M.; Miñana, G.; Barallat, J.; Cserkóová, A.; Bodi, V.; Fernández-Cisnal, A.; Núñez, E.; et al. Clinical Role of CA125 in Worsening Heart Failure: A BIOSTAT-CHF Study Subanalysis. JACC Heart Fail. 2020, 8, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Kumric, M.; Kurir, T.T.; Bozic, J.; Glavas, D.; Saric, T.; Marcelius, B.; D’Amario, D.; Borovac, J.A. Carbohydrate Antigen 125: A Biomarker at the Crossroads of Congestion and Inflammation in Heart Failure. Card. Fail. Rev. 2021, 7, e19. [Google Scholar] [CrossRef] [PubMed]
- Miñana, G.; de la Espriella, R.; Mollar, A.; Santas, E.; Núñez, E.; Valero, E.; Bodí, V.; Chorro, F.J.; Fernández-Cisnal, A.; Martí-Cervera, J.; et al. Factors associated with plasma antigen carbohydrate 125 and amino-terminal pro-B-type natriuretic peptide concentrations in acute heart failure. Eur. Heart J. Acute Cardiovasc. Care. 2020, 9, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Sanchis, J.; Bodí, V.; Fonarow, G.C.; Núñez, E.; Bertomeu-González, V.; Miñana, G.; Consuegra, L.; Bosch, M.J.; Carratalá, A.; et al. Improvement in risk stratification with the combination of the tumour marker antigen carbohydrate 125 and brain natriuretic peptide in patients with acute heart failure. Eur. Heart J. 2010, 31, 1752–1763. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Bayés-Genís, A.; Revuelta-López, E.; Miñana, G.; Santas, E.; Ter Maaten, J.M.; de la Espriella, R.; Carratalá, A.; Lorenzo, M.; Palau, P.; et al. Optimal carbohydrate antigen 125 cutpoint for identifying low-risk patients after admission for acute heart failure. Rev. Esp. Cardiol. 2022, 75, 316–324, (In English, Spanish). [Google Scholar] [CrossRef] [PubMed]
- Seo, T.; Ikeda, Y.; Onaka, H.; Hayashi, T.; Kawaguchi, K.; Kotake, C.; Toda, T.; Kobayashi, K. Usefulness of serum CA125 measurement for monitoring pericardial effusion. Jpn. Circ. J. 1993, 57, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Falcão, F.J.A.; Oliveira, F.R.A.; Cantarelli, F.; Cantarelli, R.; Brito-Júnior, P.; Lemos, H.; Silva, P.; Camboim, I.; Freire, M.C.; Carvalho, O.; et al. Carbohydrate antigen 125 predicts pulmonary congestion in patients with ST-segment elevation myocardial infarction. Braz. J. Med. Biol. Res. 2019, 52, e9124. [Google Scholar] [CrossRef] [PubMed]
- Falcão, F.; Oliveira, F.; Cantarelli, F.; Cantarelli, R.; Brito Júnior, P.; Lemos, H.; Silva, P.; Camboim, I.; Freire, M.C.; Carvalho, O.; et al. Carbohydrate antigen 125 for mortality risk prediction following acute myocardial infarction. Sci. Rep. 2020, 10, 11016. [Google Scholar] [CrossRef] [PubMed]
- Bobeica, C.; Niculet, E.; Tatu, A.L.; Craescu, M.; Vata, D.; Statescu, L.; Iancu, A.V.; Musat, C.L.; Draganescu, M.L.; Onisor, C.; et al. Old and new therapeutic strategies in systemic sclerosis (Review). Exp. Ther. Med. 2022, 23, 134. [Google Scholar] [CrossRef] [PubMed]
- Miñana Escrivá, G.; Núñez, J.; Sanchis, J.; Bodi, V.; Núñez, E.; Chorro, F.J.; Llàcer, A. Mediciones seriadas de antígeno carbohidrato 125 tras un ingreso por insuficiencia cardiaca aguda y riesgo de reingreso precoz [Carbohydrate antigen 125 serial measurements after an admission for acute heart failure and risk of early readmission]. Med. Clin. 2012, 139, 479–486. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Núñez, E.; Bayés-Genís, A.; Fonarow, G.C.; Miñana, G.; Bodí, V.; Pascual-Figal, D.; Santas, E.; Garcia-Blas, S.; Chorro, F.J.; et al. Long-term serial kinetics of N-terminal pro B-type natriuretic peptide and carbohydrate antigen 125 for mortality risk prediction following acute heart failure. Eur. Heart J. Acute Cardiovasc. Care. 2017, 6, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Li, K.H.C.; Gong, M.; Li, G.; Baranchuk, A.; Liu, T.; Wong, M.C.S.; Jesuthasan, A.; Lai, R.W.C.; Lai, J.C.L.; Lee, A.P.W.; et al. International Health Informatics Study (IHIS) Network. Cancer antigen-125 and outcomes in acute heart failure: A systematic review and meta-analysis. Heart Asia 2018, 10, e011044. [Google Scholar] [CrossRef] [PubMed]
- Soler, M.; Miñana, G.; Santas, E.; Núñez, E.; de la Espriella, R.; Valero, E.; Bodí, V.; Chorro, F.J.; Fernández-Cisnal, A.; D’Ascoli, G.; et al. CA125 outperforms NT-proBNP in acute heart failure with severe tricuspid regurgitation. Int. J. Cardiol. 2020, 308, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Llàcer, P.; Gallardo, M.Á.; Palau, P.; Moreno, M.C.; Castillo, C.; Fernández, C.; de la Espriella, R.; Mollar, A.; Santas, E.; Miñana, G.; et al. Comparison between CA125 and NT-proBNP for evaluating congestion in acute heart failure. Med. Clin. 2021, 156, 589–594, (In English, Spanish). [Google Scholar] [CrossRef] [PubMed]
- Núñez-Marín, G.; de la Espriella, R.; Santas, E.; Lorenzo, M.; Miñana, G.; Núñez, E.; Bodí, V.; González, M.; Górriz, J.L.; Bonanad, C.; et al. CA125 but not NT-proBNP predicts the presence of a congestive intrarenal venous flow in patients with acute heart failure. Eur. Heart J. Acute Cardiovasc. Care. 2021, 10, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.B.; Zorlu, A.; Tandogan, I. Plasma CA-125 level is related to both sides of the heart: A retrospective analysis. Int. J. Cardiol. 2011, 149, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Oprea, V.D.; Marinescu, M.; Rișcă Popazu, C.; Sârbu, F.; Onose, G.; Romila, A. Cardiovascular Comorbidities in Relation to the Functional Status and Vitamin D Levels in Elderly Patients with Dementia. Diagnostics. 2022, 12, 2994. [Google Scholar] [CrossRef] [PubMed]
- Menghoum, N.; Badii, M.C.; Deltombe, M.; Lejeune, S.; Roy, C.; Vancraeynest, D.; Pasquet, A.; Gerber, B.L.; Horman, S.; Gruson, D.; et al. Carbohydrate antigen 125: A useful marker of congestion, fibrosis, and prognosis in heart failure with preserved ejection fraction. ESC Heart Fail. 2024. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.L.; Hung, T.C.; Lai, Y.H.; Lu, C.S.; Wu, Y.J.; Yeh, H.I. Beyond malignancy: The role of carbohydrate antigen 125 in heart failure. Biomark. Res. 2013, 1, 25. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.Y.; Yang, D.H.; Cho, H.J.; Kim, N.K.; Kim, C.Y.; Son, J.; Roh, J.H.; Jang, S.Y.; Bae, M.H.; Lee, J.H.; et al. Serum levels of carbohydrate antigen 125 in combination with N-terminal pro-brain natriuretic peptide in patients with acute decompensated heart failure. Korean J. Intern. Med. 2019, 34, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Llàcer, P.; Bertomeu-González, V.; Bosch, M.J.; Merlos, P.; García-Blas, S.; Montagud, V.; Bodí, V.; Bertomeu-Martínez, V.; Pedrosa, V.; et al. CHANCE-HF Investigators. Carbohydrate Antigen-125-Guided Therapy in Acute Heart Failure: CHANCE-HF: A Randomized Study. JACC Heart Fail. 2016, 4, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, M.; Palau, P.; Llàcer, P.; Domínguez, E.; Ventura, B.; Núñez, G.; Miñana, G.; Solsona, J.; Santas, E.; De La Espriella, R.; et al. Clinical utility of antigen carbohydrate 125 for planning the optimal length of stay in acute heart failure. Eur. J. Intern. Med. 2021, 92, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Miñana, G.; de la Espriella, R.; Palau, P.; Llácer, P.; Núñez, E.; Santas, E.; Valero, E.; Lorenzo, M.; Núñez, G.; Bodí, V.; et al. Carbohydrate antigen 125 and risk of heart failure readmissions in patients with heart failure and preserved ejection fraction. Sci. Rep. 2022, 12, 1344. [Google Scholar] [CrossRef] [PubMed]
- Docherty, K.F.; McDowell, K.; Welsh, P.; Osmanska, J.; Anand, I.; de Boer, R.A.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; O’Meara, E.; et al. Association of Carbohydrate Antigen 125 on the Response to Dapagliflozin in Patients with Heart Failure. J. Am. Coll. Cardiol. 2023, 82, 142–157. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Llàcer, P.; Núñez, E.; Ventura, S.; Bonanad, C.; Bodí, V.; Miñana, G.; Santas, E.; Mascarell, B.; Fonarow, G.C.; et al. Antigen carbohydrate 125 and creatinine on admission for prediction of renal function response following loop diuretic administration in acute heart failure. Int. J. Cardiol. 2014, 174, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Núñez, E.; Miñana, G.; Bodí, V.; Fonarow, G.C.; Bertomeu-González, V.; Palau, P.; Merlos, P.; Ventura, S.; Chorro, F.J.; et al. Differential mortality association of loop diuretic dosage according to blood urea nitrogen and carbohydrate antigen 125 following a hospitalization for acute heart failure. Eur. J. Heart Fail. 2012, 14, 974–984. [Google Scholar] [CrossRef]
- Ordu, S.; Ozhan, H.; Alemdar, R.; Aydin, M.; Caglar, O.; Yuksel, H.; Kandis, H. Carbohydrate antigen-125 and N-terminal pro-brain natriuretic peptide levels: Compared in heart-failure prognostication. Tex. Heart Inst. J. 2012, 39, 30–35. [Google Scholar]
- de la Espriella-Juan, R.; Núñez, E.; Sanchis, J.; Bayés-Genis, A.; Núñez, J. Carbohydrate Antigen-125 in Heart Failure: An Overlooked Biomarker of Congestion. JACC Heart Fail. 2018, 6, 441–442. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; de la Espriella, R.; Miñana, G.; Santas, E.; Llácer, P.; Núñez, E.; Palau, P.; Bodí, V.; Chorro, F.J.; Sanchis, J.; et al. Antigen carbohydrate 125 as a biomarker in heart failure: A narrative review. Eur. J. Heart Fail. 2021, 23, 1445–1457. [Google Scholar] [CrossRef] [PubMed]
- Sikaris, K.A. CA125—A test with a change of heart. Heart Lung Circ. 2011, 20, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Wu, M.; Huang, M.; Zhuo, X.; Weng, Y.; Chen, X. Carbohydrate antigen 125 combined with N-terminal pro-B-type natriuretic peptide in the prediction of acute heart failure following ST-elevation myocardial infarction. Medicine 2022, 101, e32129. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Number of Patients | Results |
|---|---|---|---|
| D’Aloia et al. [27] | 2003 | 286 | CA 125 > 35 U/mL—increased risk of death/repeated hospitalization at 6 months follow-up |
| Hung et al. [48] | 2012 | 158 | In acute heart failure patients with preserved ejection fraction CA 125 levels > 17.29 U/mL correlated with increased readmissions |
| Nunez et al. CHANCE-HF TRIAL [50] | 2016 | 380 | CA-125-guided therapy superior to standard of care therapy in terms of reducing 1 year risk of death/readmissions |
| Li et al. [41] | 2018 | 8401 | Increased CA 125 levels linked to higher incidence of death/readmission for acute heart failure |
| Nunez et al. BIOSTAT—CHF TRIAL [30] | 2020 | 2516 | CA 125 high levels correlated with 1 year risk of all cause mortality |
| Soler et al. [42] | 2020 | 2961 | Higher CA 125 levels in patients with high mortality risk |
| Lorenzo et al. [51] | 2021 | 1387 | Higher levels of CA-125 in patients with AHF may identify the need for a prolonged hospitalization |
| Minana et al. [52] | 2022 | 4812 | CA 125 positively associated with heart failure readmission risk |
| Docherty et al. [53] | 2023 | 3123 | Elevated CA 125 levels were an independent predictor of the risk of worsening heart failure or cardiovascular death |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marinescu, M.C.; Oprea, V.D.; Munteanu, S.N.; Nechita, A.; Tutunaru, D.; Nechita, L.C.; Romila, A. Carbohydrate Antigen 125 (CA 125): A Novel Biomarker in Acute Heart Failure. Diagnostics 2024, 14, 795. https://doi.org/10.3390/diagnostics14080795
Marinescu MC, Oprea VD, Munteanu SN, Nechita A, Tutunaru D, Nechita LC, Romila A. Carbohydrate Antigen 125 (CA 125): A Novel Biomarker in Acute Heart Failure. Diagnostics. 2024; 14(8):795. https://doi.org/10.3390/diagnostics14080795
Chicago/Turabian StyleMarinescu, Mihai Cristian, Violeta Diana Oprea, Sorina Nicoleta Munteanu, Aurel Nechita, Dana Tutunaru, Luiza Camelia Nechita, and Aurelia Romila. 2024. "Carbohydrate Antigen 125 (CA 125): A Novel Biomarker in Acute Heart Failure" Diagnostics 14, no. 8: 795. https://doi.org/10.3390/diagnostics14080795
APA StyleMarinescu, M. C., Oprea, V. D., Munteanu, S. N., Nechita, A., Tutunaru, D., Nechita, L. C., & Romila, A. (2024). Carbohydrate Antigen 125 (CA 125): A Novel Biomarker in Acute Heart Failure. Diagnostics, 14(8), 795. https://doi.org/10.3390/diagnostics14080795