
Risk Factors for Immune Checkpoint Inhibitor-Induced Liver Injury and the Significance of Liver Biopsy

 , ,
, ,
Abstract
1. Introduction
2. Subjects and Methods
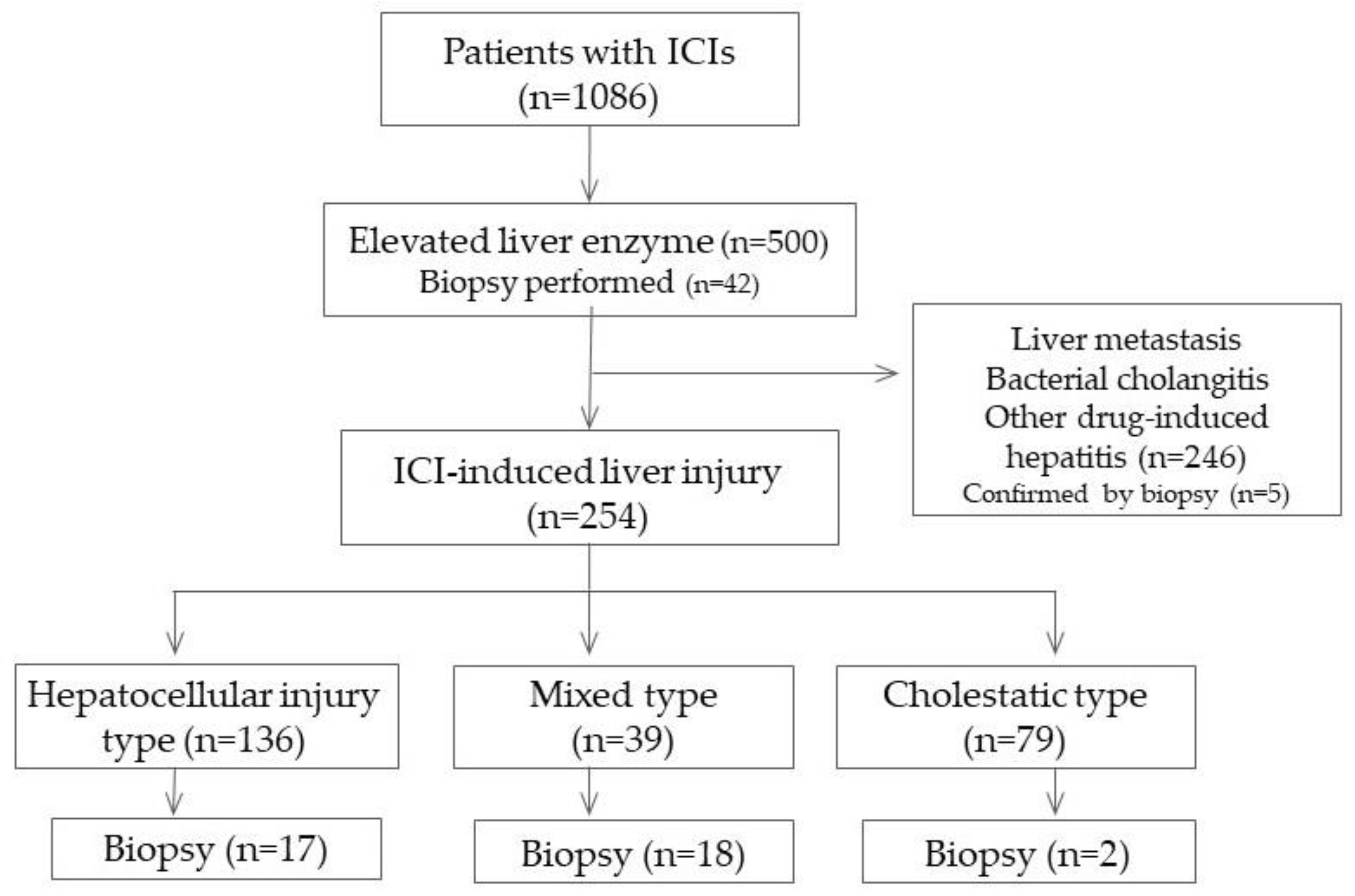
2.1. Accumulation of Cases
2.2. Diagnostic Criteria
2.3. Statistical Analysis
3. Results
3.1. Patient Background
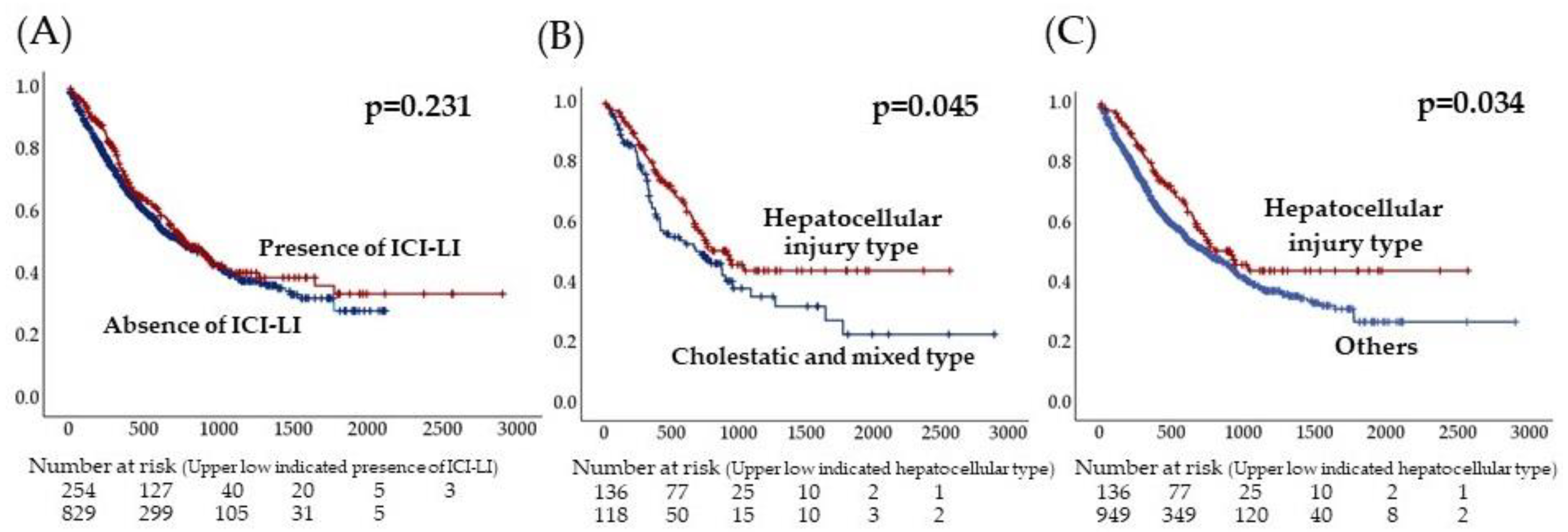
3.2. Clinical Characteristics of Patients with ICI-Induced LI
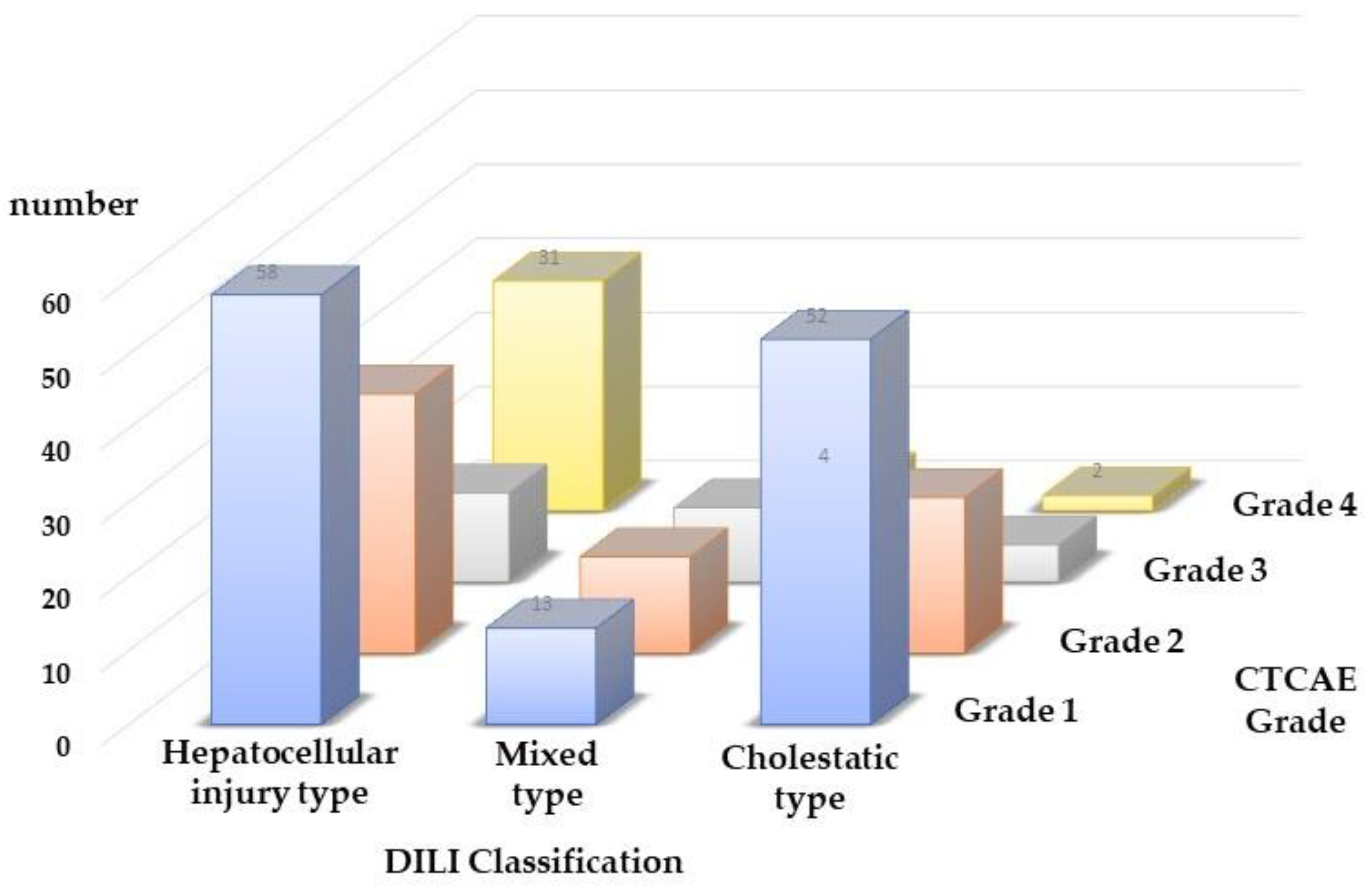
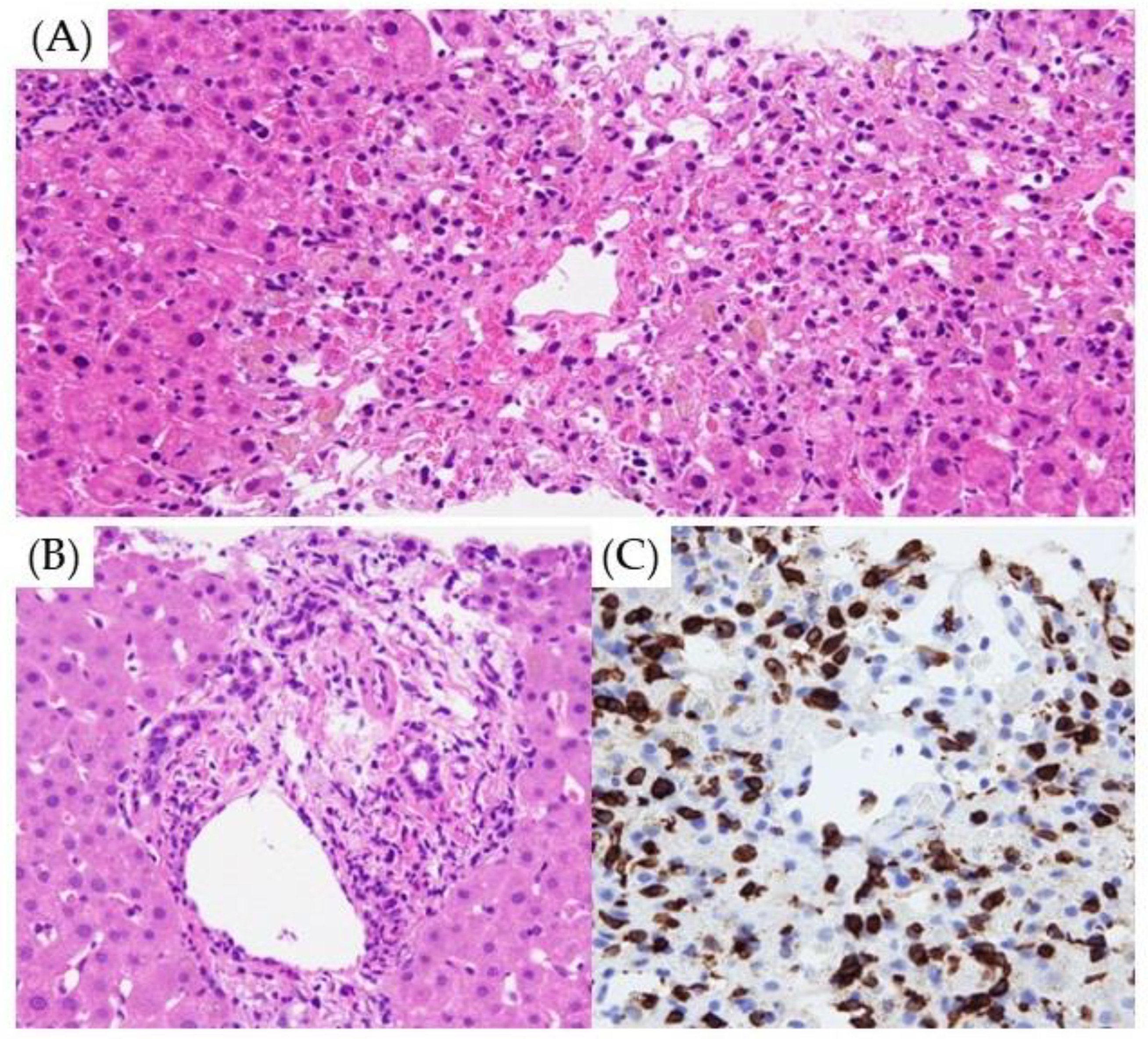
3.3. Type of ICI-Induced LI and Pathological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Michot, J.M.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related Adverse Events with Immune Checkpoint Blockade: A Comprehensive Review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef]
- De Martin, E.; Michot, J.M.; Papouin, B.; Champiat, S.; Mateus, C.; Lambotte, O.; Roche, B.; Antonini, T.M.; Coilly, A.; Laghouati, S.; et al. Characterization of Liver Injury Induced by Cancer Immunotherapy Using Immune Checkpoint Inhibitors. J. Hepatol. 2018, 68, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Hellmann, M.D. Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 1165. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chavez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Mariette, X.; Prat, A.; Suárez-Almazor, M.E. Immune-related Adverse Events of Checkpoint Inhibitors. Nat. Rev. Dis. Primers 2020, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; Clinical Practice Guideline Panel: Chair; Panel Members; EASL Governing Board Representative. EASL Clinical Practice Guidelines: Drug-induced liver injury. J. Hepatol. 2019, 70, 1222–1261. [Google Scholar] [CrossRef] [PubMed]
- Daetwyler, E.; Wallrabenstein, T.; König, D.; Cappelli, L.C.; Naidoo, J.; Zippelius, A.; Läubli, H. Corticosteroid-resistant immune-related adverse events: A systematic review. J. Immunother. Cancer 2024, 12, e007409. [Google Scholar] [CrossRef] [PubMed]
- Danan, G.; Teschke, R. RUCAM in drug and herb induced liver injury: The update. Int. J. Mol. Sci. 2015, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Clinton, J.W.; Kiparizoska, S.; Aggarwal, S.; Woo, S.; Davis, W.; Lewis, J.H. Drug-induced liver injury: Highlights and controversies in the recent literature. Drug Saf. 2021, 44, 1125–1149. [Google Scholar] [CrossRef] [PubMed]
- Benichou, C.; Danan, G.; Flahault, A. Causality assessment of adverse reactions to drugs—II. An original model for validation of drug causality assessment methods: Case reports with positive rechallenge. J. Clin. Epidemiol. 1993, 46, 1331–1336. [Google Scholar] [CrossRef]
- Danan, G.; Benichou, C. Causality assessment of adverse reactions to drugs—I. A novel method based on the conclusions of international consensus meetings: Application to drug-induced liver injuries. J. Clin. Epidemiol. 1993, 46, 1323–1330. [Google Scholar] [CrossRef]
- Ito, T.; Ishigami, M.; Yamamoto, T.; Mizuno, K.; Yamamoto, K.; Imai, N.; Ishizu, Y.; Honda, T.; Kawashima, H.; Yasuda, S.; et al. Clinical course of liver injury induced by immune checkpoint inhibitors in patients with advanced malignancies. Hepatol. Int. 2021, 15, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Madjar, K.; Mohindra, R.; Durán-Pacheco, G.; Rasul, R.; Essioux, L.; Maiya, V.; Chandler, G.S. Baseline risk factors associated with immune related adverse events and atezolizumab. Front. Oncol. 2023, 13, 1138305. [Google Scholar] [CrossRef] [PubMed]
- Kitagataya, T.; Suda, G.; Nagashima, K.; Katsurada, T.; Yamamoto, K.; Kimura, M.; Maehara, O.; Yamada, R.; Shigesawa, T.; Suzuki, K.; et al. Prevalence, clinical course, and predictive factors of immune checkpoint inhibitor monotherapy-associated hepatitis in Japan. J. Gastroenterol. Hepatol. 2020, 35, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Miah, A.; Tinoco, G.; Zhao, S.; Wei, L.; Johns, A.; Patel, S.; Li, M.; Grogan, M.; Lopez, G.; Husain, M.; et al. Immune checkpoint inhibitor-induced hepatitis injury: Risk factors, outcomes, and impact on survival. J. Cancer Res. Clin. Oncol. 2023, 149, 2235–2242. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.S.; Bergmann, O.M.; Björnsson, H.K.; Kvaran, R.B.; Olafsson, S. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology 2013, 144, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Bonkovsky, H.L.; Fontana, R.; Lee, W.; Stolz, A.; Talwalkar, J.; Reddy, K.R.; Watkins, P.B.; Navarro, V.; Barnhart, H.; et al. Features and outcomes of 899 patients with drug-induced liver injury: The DILIN prospective study. Gastroenterology 2015, 148, 1340–1352.e7. [Google Scholar] [CrossRef] [PubMed]
- Lucena, M.I.; Andrade, R.J.; Kaplowitz, N.; García-Cortes, M.; Fernández, M.C.; Romero-Gomez, M.; Bruguera, M.; Hallal, H.; Robles-Diaz, M.; Rodriguez-González, J.F.; et al. Phenotypic characterization of idiosyncratic drug-induced liver injury: The influence of age and sex. Hepatology 2009, 49, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- De Velasco, G.; Je, Y.; Bossé, D.; Awad, M.M.; Ott, P.A.; Moreira, R.B.; Schutz, F.; Bellmunt, J.; Sonpavde, G.P.; Hodi, F.S.; et al. Comprehensive Meta-analysis of Key Immune-Related Adverse Events from CTLA-4 and PD-1/PD-L1 Inhibitors in Cancer Patients. Cancer Immunol. Res. 2017, 5, 312–318. [Google Scholar] [CrossRef]
- Yamamoto, A.; Yano, Y.; Ueda, Y.; Yasutomi, E.; Hatazawa, Y.; Hayashi, H.; Yoshida, R.; Asaji, N.; Shiomi, Y.; Tobimatsu, K.; et al. Clinical features of immune-mediated hepatotoxicity induced by immune checkpoint inhibitors in patients with cancers. J. Cancer Res. Clin. Oncol. 2021, 147, 1747–1756. [Google Scholar] [CrossRef]
- Yoshikawa, Y.; Imamura, M.; Yamauchi, M.; Hayes, C.N.; Aikata, H.; Okamoto, W.; Miyata, Y.; Okada, M.; Hattori, N.; Sugiyama, K.; et al. Prevalence of immune-related adverse events and anti-tumor efficacy following immune checkpoint inhibitor therapy in Japanese patients with various solid tumors. BMC Cancer 2022, 22, 1232. [Google Scholar] [CrossRef]
- Diehl, A.; Yarchoan, M.; Hopkins, A.; Jaffee, E.; Grossman, S.A. Relationships between lymphocyte counts and treatment-related toxicities and clinical responses in patients with solid tumors treated with PD-1 checkpoint inhibitors. Oncotarget 2017, 8, 114268–114280. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Morooka, H.; Ito, T.; Ishigami, M.; Mizuno, K.; Yokoyama, S.; Yamamoto, K.; Imai, N.; Ishizu, Y.; Honda, T.; et al. Clustering using unsupervised machine learning to stratify the risk of immune-related liver injury. J. Gastroenterol. Hepatol. 2023, 38, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, K.; Ito, T.; Ishigami, M.; Ishizu, Y.; Kuzuya, T.; Honda, T.; Kawashima, H.; Inukai, Y.; Toyoda, H.; Yokota, K.; et al. Real world data of liver injury induced by immune checkpoint inhibitors in Japanese patients with advanced malignancies. J. Gastroenterol. 2020, 55, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Papouin, B.; Mussini, C.; De Martin, E.; Guettier, C. Hepatic and Digestive Adverse Events of Immune Checkpoint Inhibitors (Anti-CTLA-4 and Anti-PD-1/pd-L1): A Clinico-Pathological Review. Ann. Pathol. 2018, 38, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Okuno, T.; Nakashima, K.; Mitarai, Y.; Kataoka, M.; Tobita, H.; Nagase, M.; Isobe, T.; Tsubata, Y. Immune checkpoint inhibitor (ICI)-induced hepatitis diagnosed by liver biopsy followed by ICI-free chemotherapy leading to therapeutic effect: A case of lung cancer treatment. Respir. Med. Case. Rep. 2022, 40, 101773. [Google Scholar] [CrossRef] [PubMed]
- Imoto, K.; Kohjima, M.; Hioki, T.; Kurashige, T.; Kurokawa, M.; Tashiro, S.; Suzuki, H.; Kuwano, A.; Tanaka, M.; Okada, S.; et al. Clinical Features of Liver Injury Induced by Immune Checkpoint Inhibitors in Japanese Patients. Can. J. Gastroenterol. Hepatol. 2019, 2019, 6391712. [Google Scholar] [CrossRef] [PubMed]
- Hsiehchen, D.; Naqash, A.R.; Espinoza, M.; Von Itzstein, M.S.; Cortellini, A.; Ricciuti, B.; Owen, D.H.; Laharwal, M.; Toi, Y.; Burke, M.; et al. Association between immune-related adverse event timing and treatment outcomes. Oncoimmunology 2022, 11, 2017162. [Google Scholar] [CrossRef]
- Ng, K.Y.Y.; Tan, S.H.; Tan, J.J.E.; Tay, D.S.H.; Lee, A.W.X.; Ang, A.J.S.; Wong, L.W.J.; Choo, S.P.; Tai, D.W.M.; Lee, J.J.X. Impact of Immune-Related Adverse Events on Efficacy of Immune Checkpoint Inhibitors in Patients with Advanced Hepatocellular Carcinoma. Liver Cancer 2022, 11, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.M.; Xiong, H.F.; Chen, X.P.; Zhang, Z.W.; Zhu, L.P.; Wu, B. Correlation between immune-related adverse events and long-term outcomes in pembrolizumab-treated patients with unresectable hepatocellular carcinoma: A retrospective study. World. J. Gastrointest. Oncol. 2023, 15, 689–699. [Google Scholar] [CrossRef]
- Weber, J.S.; Kähler, K.; Hauschild, A. Management of immune-related adverse events and kinetics of response with ipilimumab. J. Clin. Oncol. 2012, 30, 2691–2697. [Google Scholar] [CrossRef]
- Wang, L.L.; Patel, G.; Chiesa-Fuxench, Z.C.; McGettigan, S.; Schuchter, L.; Mitchell, T.C.; Ming, M.E.; Chu, E.Y. Timing of onset of adverse cutaneous reactions associated with programmed cell death protein 1 inhibitor therapy. JAMA Dermatol. 2018, 154, 1057–1061. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Akamatsu, H.; Murakami, E.; Sasaki, S.; Kanai, K.; Hayata, A.; Tokudome, N.; Akamatsu, K.; Koh, Y.; Ueda, H.; et al. Correlation between immune-related adverse events and efficacy in non-small cell lung cancer treated with nivolumab. Lung Cancer 2018, 115, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Spain, L.; Diem, S.; Larkin, J. Management of toxicities of immune checkpoint inhibitors. Cancer Treat. Rev. 2016, 44, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.S.; Hodi, S.F.; Wolchok, J.D.; Topalian, S.L.; Schadendorf, D.; Larkin, J.; Sznol, M.; Long, G.V.; Li, H.; Waxman, I.M.; et al. Safety profile of nivolumab monotherapy: A pooled analysis of patients with advanced melanoma. J. Clin. Oncol. 2017, 35, 785–792. [Google Scholar] [CrossRef]
- Ghisoni, E.; Wicky, A.; Bouchaab, H.; Imbimbo, M.; Delyon, J.; Gautron Moura, B.; Gérard, C.L.; Latifyan, S.; Özdemir, B.C.; Caikovski, M.; et al. Late-onset and long-lasting immune-related adverse events from immune checkpoint-inhibitors: An overlooked aspect in immunotherapy. Eur. J. Cancer 2021, 149, 153–164. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade 0 (n = 830) | Grade 1 (n = 123) | Grade 2 (n = 69) | Grade 3 (n = 26) | Grade 4 (n = 37) | |
|---|---|---|---|---|---|
| Age | 70 (21–89) | 69 (35–85) | 69 (28–87) | 70 (50–82) | 69 (30–79) |
| Sex (male) | 631 (76%) | 93 (76%) | 49 (71%) | 19 (76%) | 24 (65%) |
| BMI | 22.0 ± 3.5 | 22.7 ± 4.1 | 21.9 ± 4.0 | 21.8 ± 3.7 | 22.3 ± 4.5 |
| ICI treatment details | |||||
| PD-1 | 562 | 96 | 50 | 15 | 23 |
| Anti-PDL-1 | 207 | 22 | 12 | 7 | 5 |
| Anti-CTLA-4 | 10 | 0 | 1 | 0 | 2 |
| Combination | 51 | 5 | 5 | 4 | 7 |
| Laboratory data before therapy | |||||
| WBC (/mm3) | 5950 (2000–67,500) | 6000 (2200–14,500) | 6250 (2800–19,400) | 6650 (3800–17,600) | 6600 (3100–14,900) |
| Lymphocytes (/mm3) | 1186 (160–5133) | 1265 (213–3802) | 1396 (216–4462) | 1006 (306–2229) | 1239 (512–4042) |
| AST (IU/L) | 20 (6–247) | 22 (12–56) | 22 (11–83) | 24 (11–127) | 21 (9–76) |
| ALT (IU/L) | 15 (2–221) | 16 (6–56) | 21 (7–91) | 24 (7–180) | 18 (8–80) |
| γGTP (IU/L) | 31 (2–1101) | 30 (8–277) | 32 (10–342) | 39.5 (15–154) | 36 (12–346) |
| ALP (IU/L) | 89 (10–1391) | 84 (10–431) | 84 (41–347) | 93 (10–376) | 99.5 (10–353) |
| Maximum value | |||||
| AST (IU/L) | 43.0 (16–80) | 84 (31–199) | 205 (82–357) | 510 (178–1269) | |
| ALT (IU/L) | 47.0 (13–78) | 101 (22–186) | 228 (102–392) | 630 (184–2458) | |
| ALP (IU/L) | 120.0 (31–823) | 131 (35–768) | 300 (71–1462) | 288 (106–981) | |
| γGTP (IU/L) | 67.5 (13–1075) | 142 (10–1113) | 291 (24–997) | 346 (48–1780) | |
| T-Bil (mg/dL) | 0.8 (0.2–2.8) | 0.9 (0.4–4.5) | 1.0 (0.4–3.1) | 1.5 (0.6–14.3) | |
| Treatment period (days) | 85 (1–1714) | 159 (1–2675) | 148 (1–1034) | 86.5 (1–2024) | 43 (1–1018) |
| ORR | 271 (35%) | 52 (43%) | 31 (47%) | 9 (35%) | 7 (19%) |
| DCR | 421 (55%) | 83 (69%) | 44 (67%) | 13 (50%) | 26 (70%) |
| Steroid therapy | 14 (11%) | 9 (13%) | 15 (58%) | 22 (59%) |
| ICI-LI Presence (n = 254) | ICI-LI Absence (n = 830) | p | |
|---|---|---|---|
| Age (years) | 69 (28–87) | 70 (21–91) | 0.226 |
| Sex (male/female) | 185/69 | 631/199 | 0.313 |
| PS | 0.69 ± 0.67 | 0.76 ± 0.67 | 0.150 |
| BMI (kg/m2) | 22.3 ± 4.1 | 22.0 ± 3.5 | 0.311 |
| Lung cancer | 84 | 274 | 0.901 |
| Urethral cancer | 71 | 208 | 0.363 |
| Cervical cancer | 41 | 116 | 0.494 |
| Malignant melanoma | 33 | 58 | 0.019 * |
| Esophageal cancer | 8 | 42 | 0.148 |
| Intestinal cancer | 10 | 42 | 0.401 |
| Hepatocellular carcinoma | 5 | 50 | 0.002 * |
| Liver involvement | 26 (19%) | 158 (19%) | 0.849 |
| ICI treatment details | |||
| PD-1 | 183 (72%) | 564 (68%) | 0.146 |
| Anti-PDL-1 | 46 (18%) | 208 (25%) | 0.017 * |
| Anti-CTLA-4 | 25 (1%) | 83 (1%) | 0.976 |
| Combination | 20 (8%) | 50 (6%) | 0.270 |
| Laboratory data before therapy | |||
| WBC (/mm3) | 6400 (2200–19,400) | 5950 (2000–67,500) | 0.383 |
| Neutrocyte count (/mm3) | 4216 (795–15,714) | 3946 (288–55,350) | 0.580 |
| Lymphocyte count (/mm3) | 1290 (213–4462) | 1186 (160–5133) | 0.010 * |
| NLR | 3.19 (0.64–31.43) | 3.30 (0.19–43.50) | 0.251 |
| AST (IU/L) | 22 (9–127) | 20 (6–247) | 0.194 |
| ALT (IU/L) | 18 (6–180) | 15 (2–221) | 0.241 |
| ALP (IU/L) | 88 (10–431) | 89 (12–1391) | 0.018 * |
| γGTP (IU/L) | 32 (8–346) | 31 (2–1101) | 0.003 * |
| CRP (mg/dL) | 0.46 (0.1–17.3) | 0.43 (0.1–27.7) | 0.145 |
| ORR | 102 (40%) | 291 (35%) | 0.204 |
| DCR | 170 (67%) | 457 (55%) | <0.001 * |
| ICI treatment period (days) | 131 (1–2675) | 85 (1–1714) | 0.009 |
| Hepatocellular Injury Type (n = 136) | Cholestatic and Mixed Type (n = 118) | p | |
|---|---|---|---|
| Age (years) | 69 (35–87) | 69.5 (28–85) | 0.866 |
| Sex (male/female) | 98/38 | 87/31 | 0.766 |
| BMI (kg/m2) | 22.4 ± 4.1 | 22.1 ± 4.1 | 0.339 |
| ICI treatment details | |||
| PD-1 | 102 (75%) | 81 (69%) | 0.331 |
| Anti-PDL-1 | 22 (16%) | 24 (20%) | 0.395 |
| Anti-CTLA-4 | 1 (1%) | 12 (1%) | 0.642 |
| Combination | 10 (7%) | 11 (9%) | 0.575 |
| Liver involvement | 26 (19%) | 21 (18%) | 0.787 |
| Laboratory data before therapy | |||
| WBC (/mm3) | 6450 (2700–19,400) | 6250 (2200–14,500) | 0.026 * |
| Neutrocyte count (/mm3) | 4216 (1290–15,714) | 4234 (795–11,310) | 0.181 |
| Lymphocyte count (/mm3) | 1334 (213–4462) | 1247 (216–3165) | 0.003 * |
| NLR | 3.01 (0.81–12.00) | 3.46 (0.64–31.43) | 0.177 |
| AST (IU/L) | 21 (10–127) | 23 (9–83) | 0.836 |
| ALT (IU/L) | 17 (6–180) | 18 (7–91) | 0.750 |
| ALP (IU/L) | 80 (10–210) | 98 (12–431) | <0.001 * |
| γGTP (IU/L) | 30 (10–346) | 37 (8–342) | 0.015 * |
| Maximum value | |||
| AST (IU/L) | 64 (16–1269) | 62 (22–509) | <0.001 * |
| ALT (IU/L) | 86 (26–2458) | 64 (13–836) | <0.001 * |
| ALP (IU/L) | 104 (31–648) | 221 (113–1462) | <0.001 * |
| γGTP (IU/L) | 85 (10–1780) | 167 (22–1113) | <0.001 * |
| ORR | 57 (42%) | 44 (37%) | 0.419 |
| DCR | 94 (69%) | 76 (64%) | 0.372 |
| ICI treatment period (days) | 128 (1–2185) | 134 (1–2675) | 0.664 |
| Steroid therapy | 35 (26%) | 25 (21%) | 0.394 |
| Treatment continued/re-treatment | 97 (71%) | 87 (74%) | 0.673 |
| p | HR | 95%CI | |
|---|---|---|---|
| Malignant melanoma | 0.041 * | 1.945 | 1.029–3.677 |
| Liver cancer | 0.061 | ||
| Anti-PD-1 antibody | 0.163 | ||
| ALP | 0.007 * | 0.991 | 0.984–0.997 |
| γGTP | 0.056 | ||
| Lymphocyte count | 0.013 * | 1.000 | 1.000–1.001 |
| Histological Findings | DILI Classification | p | ||
|---|---|---|---|---|
| Hepatocellular Injury Type (n = 17) | Mixed Type (n = 18) | Cholestatic Type (n = 2) | ||
| Centrilobular hepatitis | 13 (76%) * | 5 (28%) * | 0 (0%) | 0.005 * |
| Spotty/focal necrosis | 14 (82%) * | 8 (44%) * | 2 (100%) | 0.020 * |
| Pigmented macrophage | 6 (35%) | 4 (22%) | 0 (0%) | n.s. |
| Granuloma | 1 (6%) | 4 (22%) | 0 (0%) | n.s. |
| Councilman body | 9 (53%) | 5 (28%) | 1 (50%) | n.s. |
| Ballooning | 5 (29%) | 3 (17%) | 0 (0%) | n.s. |
| Emperiporesis | 5 (29%) | 3 (17%) | 0 (0%) | n.s. |
| Interface hepatitis | 4 (24%) * | 11 (61%) * | 2 (100%) | 0.028 * |
| Portal inflammation | 4 (24%) * | 14 (78%) * | 2 (100%) | 0.002 * |
| Fibrosis of portal tract | 5 (29%) | 6 (33%) | 0 (0%) | n.s. |
| Eosinophil infiltration | 6 (35%) | 9 (50%) | 2 (100%) | n.s. |
| Ductular reaction | 2 (12%) * | 8 (44%) * | 2 (100%) | 0.032 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawano, M.; Yano, Y.; Yamamoto, A.; Yasutomi, E.; Inoue, Y.; Kitadai, J.; Yoshida, R.; Matsuura, T.; Shiomi, Y.; Ueda, Y.; et al. Risk Factors for Immune Checkpoint Inhibitor-Induced Liver Injury and the Significance of Liver Biopsy. Diagnostics 2024, 14, 815. https://doi.org/10.3390/diagnostics14080815
Kawano M, Yano Y, Yamamoto A, Yasutomi E, Inoue Y, Kitadai J, Yoshida R, Matsuura T, Shiomi Y, Ueda Y, et al. Risk Factors for Immune Checkpoint Inhibitor-Induced Liver Injury and the Significance of Liver Biopsy. Diagnostics. 2024; 14(8):815. https://doi.org/10.3390/diagnostics14080815
Chicago/Turabian StyleKawano, Miki, Yoshihiko Yano, Atsushi Yamamoto, Eiichiro Yasutomi, Yuta Inoue, Jun Kitadai, Ryutaro Yoshida, Takanori Matsuura, Yuuki Shiomi, Yoshihide Ueda, and et al. 2024. "Risk Factors for Immune Checkpoint Inhibitor-Induced Liver Injury and the Significance of Liver Biopsy" Diagnostics 14, no. 8: 815. https://doi.org/10.3390/diagnostics14080815
APA StyleKawano, M., Yano, Y., Yamamoto, A., Yasutomi, E., Inoue, Y., Kitadai, J., Yoshida, R., Matsuura, T., Shiomi, Y., Ueda, Y., & Kodama, Y. (2024). Risk Factors for Immune Checkpoint Inhibitor-Induced Liver Injury and the Significance of Liver Biopsy. Diagnostics, 14(8), 815. https://doi.org/10.3390/diagnostics14080815