

A Secondary Retrospective Analysis of the Predictive Value of Neutrophil-Reactive Intensity (NEUT-RI) in Septic and Non-Septic Patients in Intensive Care

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
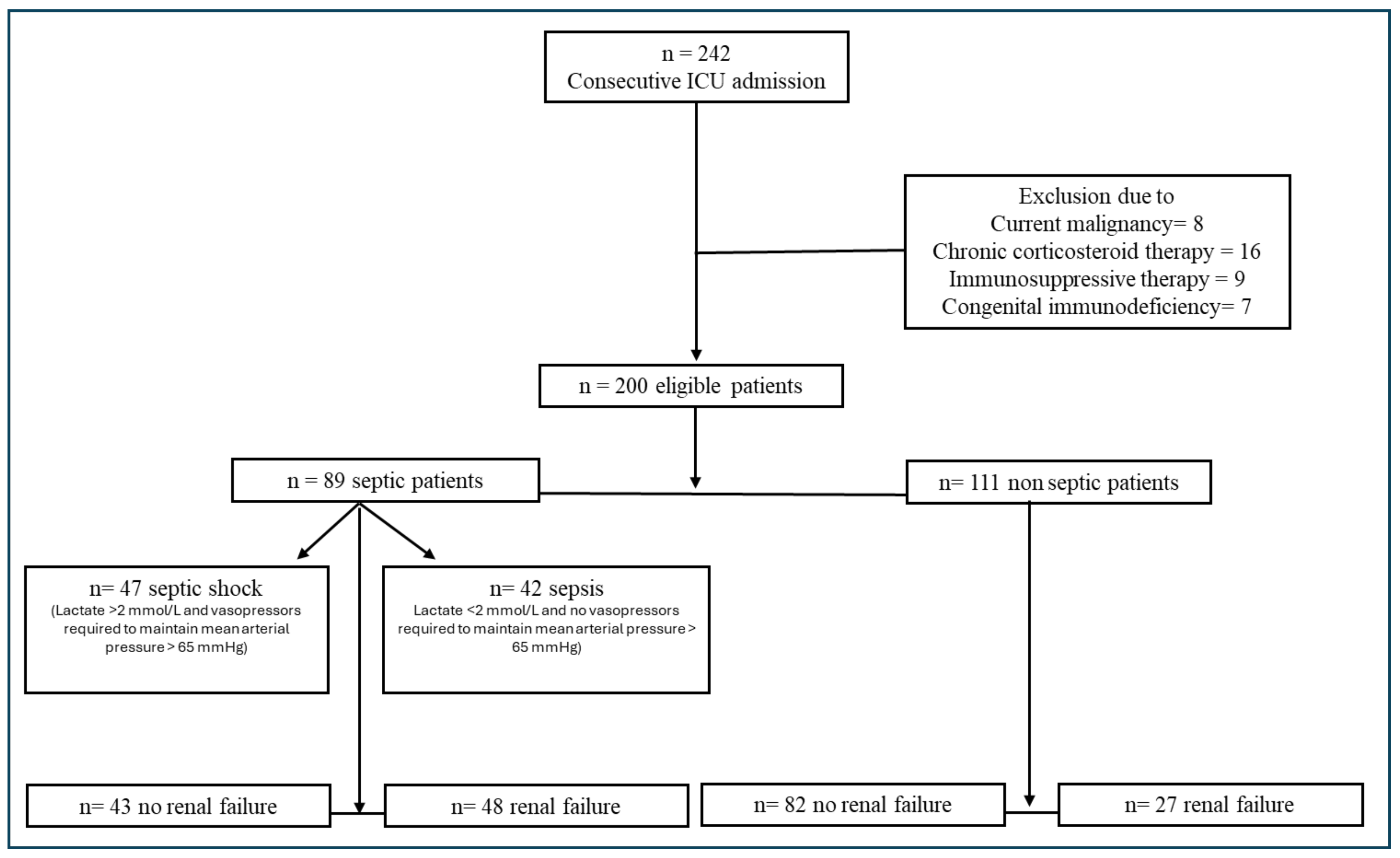
3. Results
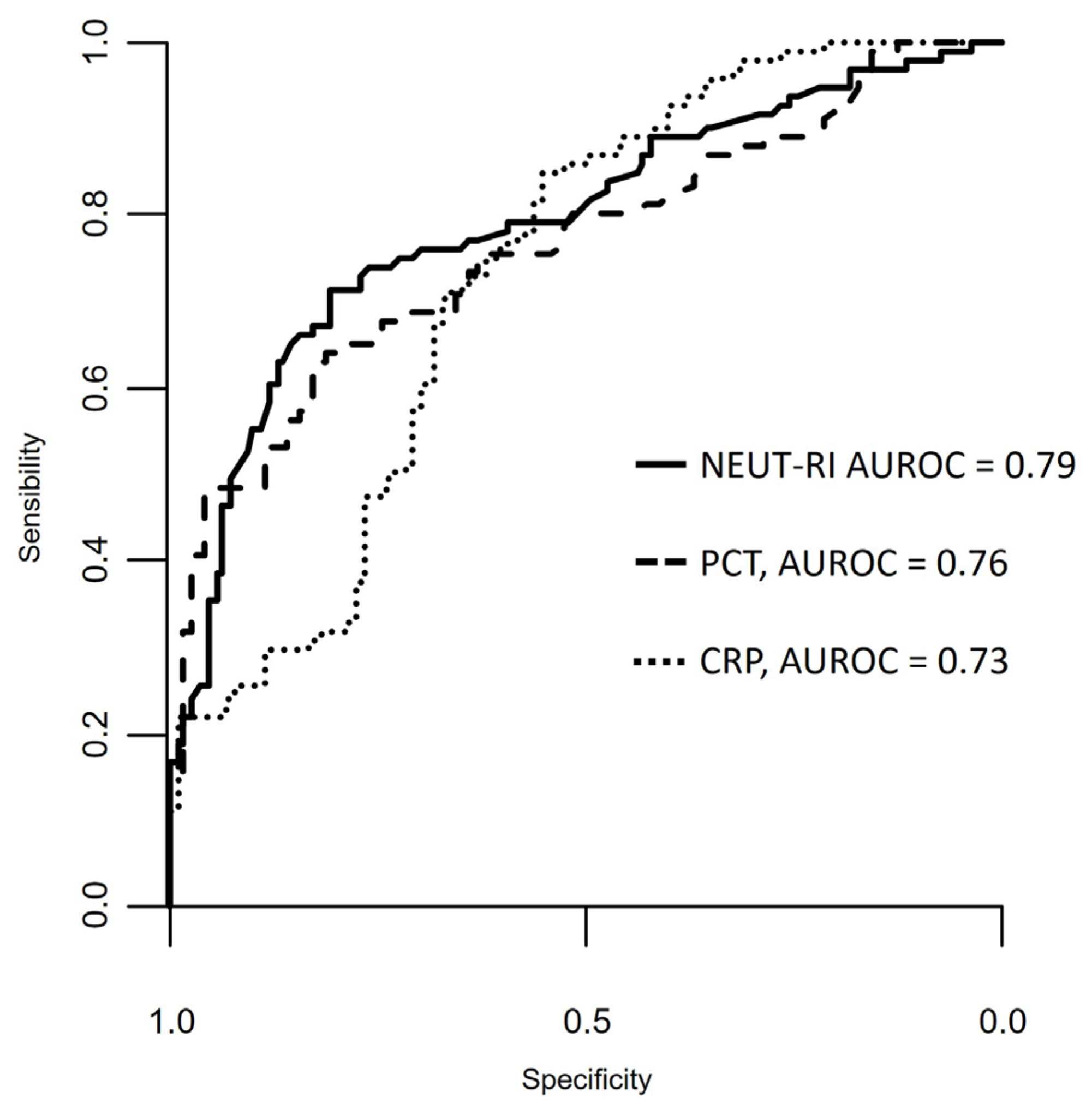
3.1. Inflammatory Parameters
3.2. Renal Failure and Inflammatory Parameters
3.3. 28-Day Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Ji, W.; Bo, L.; Bian, J. How to Improve the Care of Septic Patients Following “Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021”? J. Intensive Med. 2023, 3, 144–146. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA Score-Development, Utility and Challenges of Accurate Assessment in Clinical Trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Muteeb, G.; Rehman, M.T.; Shahwan, M.; Aatif, M. Origin of Antibiotics and Antibiotic Resistance, and Their Impacts on Drug Development: A Narrative Review. Pharmaceuticals 2023, 16, 1615. [Google Scholar] [CrossRef] [PubMed]
- Berild, D.; Mohseni, A.; My Diep, L.; Jensenius, M.; Holta Ringertz, S. Adjustment of antibiotic treatment according to the results of blood cultures leads to decreased antibiotic use and costs. J. Antimicrob. Chemother. 2006, 57, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Castelli, G.P.; Pognani, C.; Meisner, M.; Stuani, A.; Bellomi, D.; Sgarbi, L. Procalcitonin and C-Reactive Protein during Systemic Inflammatory Response Syndrome, Sepsis and Organ Dysfunction. Crit. Care 2004, 8, R234–R242. [Google Scholar] [CrossRef]
- Qu, R.; Hu, L.; Ling, Y.; Hou, Y.; Fang, H.; Zhang, H.; Liang, S.; He, Z.; Fang, M.; Li, J.; et al. C-Reactive Protein Concentration as a Risk Predictor of Mortality in Intensive Care Unit: A Multicenter, Prospective, Observational Study. BMC Anesthesiol. 2020, 20, 292. [Google Scholar] [CrossRef] [PubMed]
- de Werra, I.; Jaccard, C.; Corradin, S.B.; Chioléro, R.; Yersin, B.; Gallati, H.; Assicot, M.; Bohuon, C.; Baumgartner, J.D.; Glauser, M.P.; et al. Cytokines, Nitrite/Nitrate, Soluble Tumor Necrosis Factor Receptors, and Procalcitonin Concentrations: Comparisons in Patients with Septic Shock, Cardiogenic Shock, and Bacterial Pneumonia. Crit. Care Med. 1997, 25, 607–613. [Google Scholar] [CrossRef]
- Picod, A.; Morisson, L.; de Roquetaillade, C.; Sadoune, M.; Mebazaa, A.; Gayat, E.; Davison, B.A.; Cotter, G.; Chousterman, B.G. Systemic Inflammation Evaluated by Interleukin-6 or C-Reactive Protein in Critically Ill Patients: Results from the FROG-ICU Study. Front. Immunol. 2022, 13, 868348. [Google Scholar] [CrossRef]
- Wiedermann, F.J.; Kaneider, N.; Egger, P.; Tiefenthaler, W.; Wiedermann, C.J.; Lindner, K.H.; Schobersberger, W. Migration of Human Monocytes in Response to Procalcitonin. Crit. Care Med. 2002, 30, 1112–1117. [Google Scholar] [CrossRef] [PubMed]
- Wacker, C.; Prkno, A.; Brunkhorst, F.M.; Schlattmann, P. Procalcitonin as a Diagnostic Marker for Sepsis: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2013, 13, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Brunkhorst, F.M.; Wegscheider, K.; Forycki, Z.F.; Brunkhorst, R. Procalcitonin for Early Diagnosis and Differentiation of SIRS, Sepsis, Severe Sepsis, and Septic Shock. Intensive Care Med. 2000, 26 (Suppl. S2), S148–S152. [Google Scholar] [CrossRef] [PubMed]
- Urrechaga, E.; Bóveda, O.; Aguirre, U. Role of Leucocytes Cell Population Data in the Early Detection of Sepsis. J. Clin. Pathol. 2018, 71, 259–266. [Google Scholar] [CrossRef]
- Zhang, W.; Zhang, Z.; Pan, S.; Li, J.; Yang, Y.; Qi, H.; Xie, J.; Qu, J. The Clinical Value of Hematological Neutrophil and Monocyte Parameters in the Diagnosis and Identification of Sepsis. Ann. Transl. Med. 2021, 9, 1680. [Google Scholar] [CrossRef]
- Cornet, E.; Boubaya, M.; Troussard, X. Contribution of the New XN-1000 Parameters NEUT-RI and NEUT-WY for Managing Patients with Immature Granulocytes. Int. J. Lab. Hematol. 2015, 37, e123–e126. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Chang, J.; Kahng, J.; Park, H.; Jo, I.; Kim, Y.; Han, K. Development of a Novel Flow Cytometry-Based System for White Blood Cell Differential Counts: 10-Color LeukoDiff. Ann. Lab. Med. 2019, 39, 141–149. [Google Scholar] [CrossRef]
- Lee, J.; Gu, J.; Seo, J.E.; Kim, J.W.; Kim, H.K. Diagnostic and Prognostic Values of Neutrophil Reactivity Intensity (NEUT-RI) in Pediatric Systemic Inflammatory Response Syndrome and Sepsis. Ann. Clin. Lab. Sci. 2023, 53, 173–180. [Google Scholar]
- Mantovani, E.M.A.; Formenti, P.; Pastori, S.; Roccaforte, V.; Gotti, M.; Panella, R.; Galimberti, A.; Costagliola, R.; Vetrone, F.; Umbrello, M.; et al. The Potential Role of Neutrophil-Reactive Intensity (NEUT-RI) in the Diagnosis of Sepsis in Critically Ill Patients: A Retrospective Cohort Study. Diagnostics 2023, 13, 1781. [Google Scholar] [CrossRef]
- Finazzi, S.; Paci, G.; Antiga, L.; Brissy, O.; Carrara, G.; Crespi, D.; Csato, G.; Csomos, A.; Duek, O.; Facchinetti, S.; et al. PROSAFE: A European Endeavor to Improve Quality of Critical Care Medicine in Seven Countries. Minerva Anestesiol. 2020, 86, 1305–1320. [Google Scholar] [CrossRef]
- Levey, A.S. Defining AKD: The Spectrum of AKI, AKD, and CKD. Nephron 2022, 146, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Delano, M.J.; Ward, P.A. The Immune System’s Role in Sepsis Progression, Resolution and Long-Term Outcome. Immunol. Rev. 2016, 274, 330–353. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.A.; Selzman, C.H.; Cothren, C.; Sorensen, A.C.; Raeburn, C.D.; Harken, A.H. Diagnostic implications of C-reactive protein. Arch. Surg. 2003, 138, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Lelubre, C.; Anselin, S.; Zouaoui Boudjeltia, K.; Biston, P.; Piagnerelli, M. Interpretation of C-Reactive Protein Concentrations in Critically Ill Patients. Biomed. Res. Int. 2013, 2013, 124021. [Google Scholar] [CrossRef] [PubMed]
- Dinsdale, R.J.; Devi, A.; Hampson, P.; Wearn, C.M.; Bamford, A.L.; Hazeldine, J.; Bishop, J.; Ahmed, S.; Watson, C.; Lord, J.M.; et al. Changes in Novel Haematological Parameters Following Thermal Injury: A Prospective Observational Cohort Study. Sci. Rep. 2017, 7, 3211. [Google Scholar] [CrossRef] [PubMed]
- Doi, K. Role of Kidney Injury in Sepsis. J. Intensive Care 2016, 4, 17. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Kim, M.-J.; Ko, H.-J.; Lee, E.-J.; Kim, H.-R.; Jeon, J.-W.; Ham, Y.-R.; Na, K.-R.; Lee, K.-W.; Lee, S.-I.; et al. Diagnostic and Prognostic Roles of C-Reactive Protein, Procalcitonin, and Presepsin in Acute Kidney Injury Patients Initiating Continuous Renal Replacement Therapy. Diagnostics 2023, 13, 777. [Google Scholar] [CrossRef] [PubMed]
- Stuveling, E.M.; Hillege, H.L.; Bakker, S.J.L.; Gans, R.O.B.; De Jong, P.E.; De Zeeuw, D. C-Reactive Protein Is Associated with Renal Function Abnormalities in a Non-Diabetic Population. Kidney Int. 2003, 63, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.-L.; Xiao, Z.-H.; Yang, M.-Y.; Zhu, Y.-M. Diagnostic Value of Serum Procalcitonin in Patients with Chronic Renal Insufficiency: A Systematic Review and Meta-Analysis. Nephrol. Dial. Transplant. 2013, 28, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Steinbach, G.; Bölke, E.; Grünert, A.; Störck, M.; Orth, K. Procalcitonin in Patients with Acute and Chronic Renal Insufficiency. Wien. Klin. Wochenschr. 2004, 116, 849–853. [Google Scholar] [CrossRef]
- Vivas, M.C.; Villamarin Guerrero, H.F.; Tascon, A.J.; Valderrama-Aguirre, A. Plasma Interleukin-6 Levels Correlate with Survival in Patients with Bacterial Sepsis and Septic Shock. Interv. Med. Appl. Sci. 2021, 11, 224–230. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| A | B | |||||
|---|---|---|---|---|---|---|
| Septic (n = 89) | Non-Septic (n = 111) | p | Not Complicated Sepsis (n = 47) | Septic Shock (n = 42) | p | |
| Age | 73.00 [63.00–79.00] | 73.00 [56.00–79.00] | 0.454 | 74.00 [64.00–78.00] | 73.00 [62.75–79.75] | 0.808 |
| Male% | 48.4 | 52.3 | 0.679 | 59.6 | 35.7 | 0.042 |
| Creatinine | 1.57 [0.85–2.85] | 1.00 [0.77–1.39] | <0.001 | 1.16 [0.77–1.64] | 2.18 [1.67–3.67] | <0.001 |
| CRP | 20.79 [12.54–118.91] | 6.68 [1.54–21.70] | <0.001 | 18.79 [7.78–149.16] | 23.03 [17.97–87.09] | 0.7244 |
| PCT | 8.83 [0.82–45.88] | 0.48 [0.29–1.64] | <0.001 | 1.63 [0.40–12.09] | 32.59 [8.83–100.00] | <0.001 |
| NEUT-RI | 53.80 [49.65–59.05] | 48.00 [46.00–49.90] | <0.001 | 51.5 [47.80–56.30] | 56.20 [52.30–61.92] | 0.0054 |
| Septic | Non-Septic | |||||
|---|---|---|---|---|---|---|
| Renal Failure (n = 43) | Normal Renal Function (n = 48) | p | Renal Failure (n = 27) | Normal Renal Function (n = 82) | p | |
| Age | 73.00 [63.00–79.00] | 72.50 [63.50–77.50] | 0.443 | 78.00 [73.00–81.00] | 68.00 [53.25–77.00] | 0.004 |
| Male% | 37.2 | 58.3 | 0.071 | 51.9 | 52.4 | 1 |
| Creatinine | 2.81 [1.83–4.26] | 0.86 [0.74–1.28] | <0.001 | 1.60 [1.33–2.59] | 0.89 [0.68–1.19] | <0.001 |
| CRP | 25.53 [17.82–148.22] | 18.80 [7.35–103.27] | 0.164 | 13.45 [6.03–130.85] | 3.78 [1.05–18.59] | 0.003 |
| PCT | 32.23 [5.86–83.72] | 1.79 [0.39–13.04] | <0.001 | 1.15 [0.31–3.63] | 0.47 [0.28–1.21] | 0.193 |
| NEUT-RI | 55.10 [52.15–59.05] | 51.70 [47.82–58.65] | 0.101 | 47.90 [46.40–50.05] | 48.00 [45.85–49.88] | 0.886 |
| Septic | Non-Septic | |||||
|---|---|---|---|---|---|---|
| Alive (n = 78) | Dead (n = 11) | p | Alive (n = 95) | Dead (n = 16) | p | |
| CRP | 21.52 [11.48–137.89] | 19.06 [14.10–36.49] | 0.772 | 7.28 [1.88–21.70] | 1.06 [0.41–80.00] | 0.477 |
| PCT | 3.22 [0.59–32.32] | 39.56 [17.39–83.72] | 0.002 | 0.46 [0.28–1.21] | 0.72 [0.57–1.10] | 0.453 |
| NEUT-RI | 53.05 [48.90–57.22] | 58.80 [54.45–73.35] | 0.005 | 47.90 [45.80–49.82] | 45.60 [44.00–47.60] | 0.184 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Formenti, P.; Isidori, L.; Pastori, S.; Roccaforte, V.; Mantovani, E.A.; Iezzi, M.; Menozzi, A.; Panella, R.; Galimberti, A.; Brenna, G.; et al. A Secondary Retrospective Analysis of the Predictive Value of Neutrophil-Reactive Intensity (NEUT-RI) in Septic and Non-Septic Patients in Intensive Care. Diagnostics 2024, 14, 821. https://doi.org/10.3390/diagnostics14080821
Formenti P, Isidori L, Pastori S, Roccaforte V, Mantovani EA, Iezzi M, Menozzi A, Panella R, Galimberti A, Brenna G, et al. A Secondary Retrospective Analysis of the Predictive Value of Neutrophil-Reactive Intensity (NEUT-RI) in Septic and Non-Septic Patients in Intensive Care. Diagnostics. 2024; 14(8):821. https://doi.org/10.3390/diagnostics14080821
Chicago/Turabian StyleFormenti, Paolo, Letizia Isidori, Stefano Pastori, Vincenzo Roccaforte, Elena Alessandra Mantovani, Massimiliano Iezzi, Alessandro Menozzi, Rossella Panella, Andrea Galimberti, Giovanni Brenna, and et al. 2024. "A Secondary Retrospective Analysis of the Predictive Value of Neutrophil-Reactive Intensity (NEUT-RI) in Septic and Non-Septic Patients in Intensive Care" Diagnostics 14, no. 8: 821. https://doi.org/10.3390/diagnostics14080821