
A Multivariant Surrogate Virus Neutralization Test Demonstrates Distinct SARS-CoV-2-Specific Antibody Responses in People Living with HIV after a Fourth Monovalent mRNA Vaccination or an Omicron Breakthrough Infection

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Multivariant Surrogate Virus Neutralization Test
2.3. Statistical Analyses
3. Results
3.1. Antibody Levels in PWLH after Three Doses of mRNA Vaccines
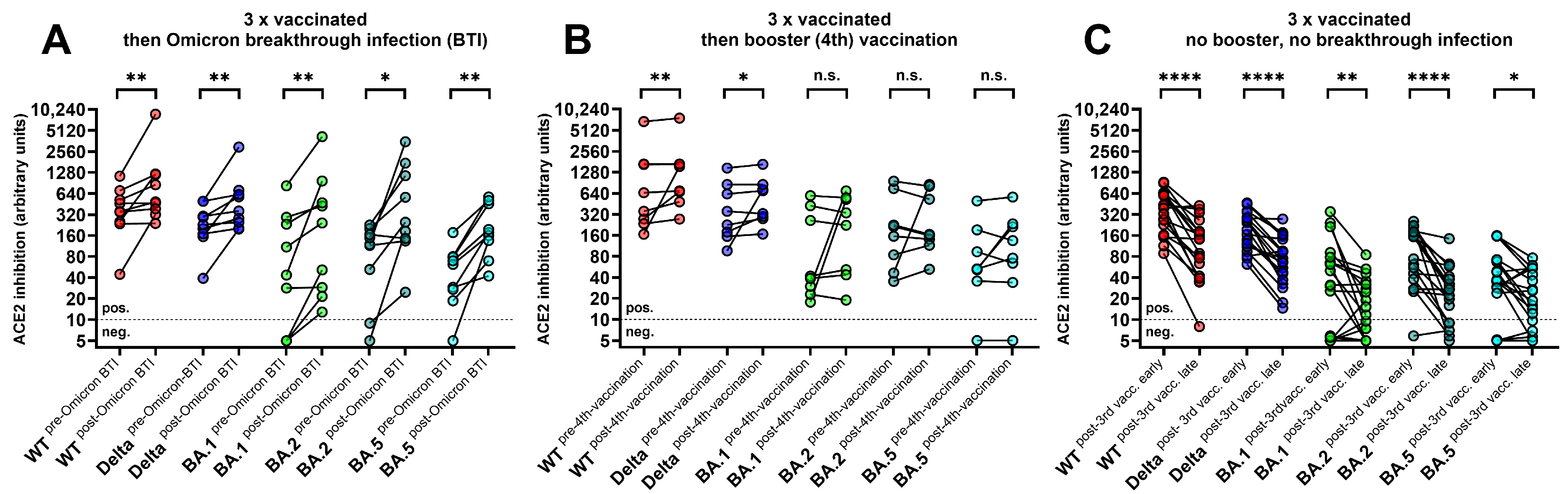
3.2. Levels of ACE2-RBD-Binding Inhibition after Booster Vaccination versus Omicron Breakthrough Infection
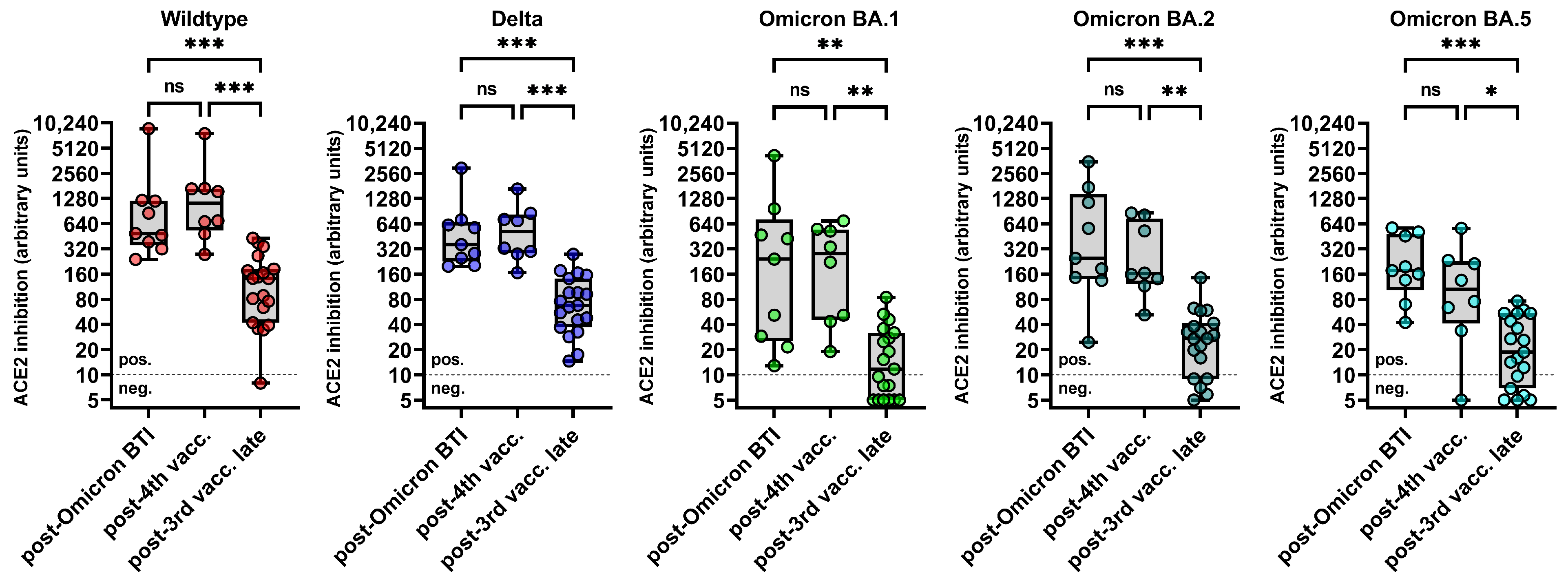
3.3. Levels of ACE2-RBD-Binding Inhibition for WT, Delta, Omicron BA.1, BA.2 and BA.5
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vicenti, I.; Basso, M.; Pirola, N.; Bragato, B.; Rossi, M.C.; Giobbia, M.; Pascoli, S.; Vinci, A.; Caputo, S.; Varasi, I.; et al. SARS-CoV-2 Neutralizing Antibodies to B.1 and to BA.5 Variant after Booster Dose of BNT162b2 Vaccine in HIV Patients COVID-Naive and on Successful Antiretroviral Therapy. Vaccines 2023, 11, 871. [Google Scholar] [CrossRef] [PubMed]
- Lapointe, H.R.; Mwimanzi, F.; Cheung, P.K.; Sang, Y.; Yaseen, F.; Speckmaier, S.; Barad, E.; Moran-Garcia, N.; Datwani, S.; Duncan, M.C.; et al. Antibody response durability following three-dose coronavirus disease 2019 vaccination in people with HIV receiving suppressive antiretroviral therapy. AIDS 2023, 37, 709–721. [Google Scholar] [CrossRef]
- Wei, J.; Matthews, P.C.; Stoesser, N.; Newton, J.N.; Diamond, I.; Studley, R.; Taylor, N.; Bell, J.I.; Farrar, J.; Kolenchery, J.; et al. Protection against SARS-CoV-2 Omicron BA.4/5 variant following booster vaccination or breakthrough infection in the UK. Nat. Commun. 2023, 14, 2799. [Google Scholar] [CrossRef] [PubMed]
- Perez-Saez, J.; Zaballa, M.E.; Lamour, J.; Yerly, S.; Dubos, R.; Courvoisier, D.S.; Villers, J.; Balavoine, J.F.; Pittet, D.; Kherad, O.; et al. Long term anti-SARS-CoV-2 antibody kinetics and correlate of protection against Omicron BA.1/BA.2 infection. Nat. Commun. 2023, 14, 3032. [Google Scholar] [CrossRef] [PubMed]
- Hertz, T.; Levy, S.; Ostrovsky, D.; Oppenheimer, H.; Zismanov, S.; Kuzmina, A.; Friedman, L.M.; Trifkovic, S.; Brice, D.; Chun-Yang, L.; et al. Correlates of protection for booster doses of the SARS-CoV-2 vaccine BNT162b2. Nat. Commun. 2023, 14, 4575. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.; Butta, G.M.; Donnici, L.; Bozzi, G.; Oggioni, M.; Bono, P.; Matera, M.; Consonni, D.; Ludovisi, S.; Muscatello, A.; et al. Anti-spike antibodies and neutralising antibody activity in people living with HIV vaccinated with COVID-19 mRNA-1273 vaccine: A prospective single-centre cohort study. Lancet Reg. Health Eur. 2022, 13, 100287. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.Y.; Hsiao, S.H.; Huang, C.G.; Chang, C.S.; Chen, G.Y.; Huang, Y.L.; Dutta, A.; Huang, C.T. Relatively preserved functional immune capacity with standard COVID-19 vaccine regimen in people living with HIV. Front. Immunol. 2023, 14, 1204314. [Google Scholar] [CrossRef] [PubMed]
- Heftdal, L.D.; Perez-Alos, L.; Hasselbalch, R.B.; Hansen, C.B.; Hamm, S.R.; Moller, D.L.; Pries-Heje, M.; Fogh, K.; Gerstoft, J.; Gronbaek, K.; et al. Humoral and cellular immune responses eleven months after the third dose of BNT162b2 an mRNA-based COVID-19 vaccine in people with HIV—A prospective observational cohort study. eBioMedicine 2023, 93, 104661. [Google Scholar] [CrossRef]
- Kling, K.D.; Janulis, P.; Demonbreun, A.R.; Sancilio, A.; Berzins, B.; Krueger, K.; Achenbach, C.; Price, R.; Sullivan, M.; Caputo, M.; et al. No difference in anti-spike antibody and surrogate viral neutralization following SARS-CoV-2 booster vaccination in persons with HIV compared to controls (CO-HIV Study). Front. Immunol. 2022, 13, 1048776. [Google Scholar] [CrossRef]
- Antinori, A.; Cicalini, S.; Meschi, S.; Bordoni, V.; Lorenzini, P.; Vergori, A.; Lanini, S.; De Pascale, L.; Matusali, G.; Mariotti, D.; et al. Humoral and Cellular Immune Response Elicited by mRNA Vaccination Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in People Living With Human Immunodeficiency Virus Receiving Antiretroviral Therapy Based on Current CD4 T-Lymphocyte Count. Clin. Infect. Dis. 2022, 75, e552–e563. [Google Scholar] [CrossRef]
- Hensley, K.S.; Jongkees, M.J.; Geers, D.; GeurtsvanKessel, C.H.; Mueller, Y.M.; Dalm, V.; Papageorgiou, G.; Steggink, H.; Gorska, A.; Bogers, S.; et al. Immunogenicity and reactogenicity of SARS-CoV-2 vaccines in people living with HIV in the Netherlands: A nationwide prospective cohort study. PLoS Med. 2022, 19, e1003979. [Google Scholar] [CrossRef] [PubMed]
- Verburgh, M.L.; van Pul, L.; Grobben, M.; Boyd, A.; Wit, F.; van Nuenen, A.C.; van Dort, K.A.; Tejjani, K.; van Rijswijk, J.; Bakker, M.; et al. Robust Vaccine-Induced as Well as Hybrid B- and T-Cell Immunity across SARS-CoV-2 Vaccine Platforms in People with HIV. Microbiol. Spectr. 2023, 11, e0115523. [Google Scholar] [CrossRef] [PubMed]
- Corma-Gomez, A.; Fernandez-Fuertes, M.; Vinuela, L.; Dominguez, C.; Santos, M.; Fuentes-Lopez, A.; Rojas, A.; Fernandez-Perez, N.; Martin-Carmona, J.; Serrano-Conde, E.; et al. Reduced neutralizing antibody response to SARS-CoV-2 vaccine booster dose in people living with HIV with severe immunosuppression. J. Med. Virol. 2023, 95, e28602. [Google Scholar] [CrossRef] [PubMed]
- Vergori, A.; Cozzi Lepri, A.; Cicalini, S.; Matusali, G.; Bordoni, V.; Lanini, S.; Meschi, S.; Iannazzo, R.; Mazzotta, V.; Colavita, F.; et al. Immunogenicity to COVID-19 mRNA vaccine third dose in people living with HIV. Nat. Commun. 2022, 13, 4922. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Cortes, L.F.; Saborido-Alconchel, A.; Trujillo-Rodriguez, M.; Serna-Gallego, A.; Llaves-Flores, S.; Munoz-Muela, E.; Perez-Santos, M.J.; Lozano, C.; Mejias-Trueba, M.; Roca, C.; et al. Humoral and cellular immunity to SARS-CoV-2 after vaccination with mRNA vaccines in PLWH with discordant immune response. Influence of the vaccine administered. Front. Immunol. 2023, 14, 1129753. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradnik, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.E.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484.e415. [Google Scholar] [CrossRef] [PubMed]
- Hachmann, N.P.; Miller, J.; Collier, A.Y.; Ventura, J.D.; Yu, J.; Rowe, M.; Bondzie, E.A.; Powers, O.; Surve, N.; Hall, K.; et al. Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5. N. Engl. J. Med. 2022, 387, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Medits, I.; Springer, D.N.; Graninger, M.; Camp, J.V.; Holtl, E.; Aberle, S.W.; Traugott, M.T.; Hoepler, W.; Deutsch, J.; Lammel, O.; et al. Different Neutralization Profiles After Primary SARS-CoV-2 Omicron BA.1 and BA.2 Infections. Front. Immunol. 2022, 13, 946318. [Google Scholar] [CrossRef]
- Rossler, A.; Netzl, A.; Knabl, L.; Schafer, H.; Wilks, S.H.; Bante, D.; Falkensammer, B.; Borena, W.; von Laer, D.; Smith, D.J.; et al. BA.2 and BA.5 omicron differ immunologically from both BA.1 omicron and pre-omicron variants. Nat. Commun. 2022, 13, 7701. [Google Scholar] [CrossRef]
- Vergori, A.; Matusali, G.; Lepri, A.C.; Cimini, E.; Fusto, M.; Colavita, F.; Gagliardini, R.; Notari, S.; Mazzotta, V.; Mariotti, D.; et al. Neutralizing activity and T-cell response after bivalent fifth dose of messenger RNA vaccine in people living with HIV. Int. J. Infect. Dis. 2023, 134, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.C.; Tiu, C.; Hu, Z.; Chen, V.C.W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2–spike protein–protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Springer, D.N.; Traugott, M.; Reuberger, E.; Kothbauer, K.B.; Borsodi, C.; Nageli, M.; Oelschlagel, T.; Kelani, H.; Lammel, O.; Deutsch, J.; et al. A Multivariant Surrogate Neutralization Assay Identifies Variant-Specific Neutralizing Antibody Profiles in Primary SARS-CoV-2 Omicron Infection. Diagnostics 2023, 13, 2278. [Google Scholar] [CrossRef] [PubMed]
- Zaballa, M.E.; Perez-Saez, J.; de Mestral, C.; Pullen, N.; Lamour, J.; Turelli, P.; Raclot, C.; Baysson, H.; Pennacchio, F.; Villers, J.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies and cross-variant neutralization capacity after the Omicron BA.2 wave in Geneva, Switzerland: A population-based study. Lancet Reg. Health Eur. 2023, 24, 100547. [Google Scholar] [CrossRef] [PubMed]
- Springer, D.N.; Höltl, E.; Prüger, K.; Puchhammer-Stöckl, E.; Aberle, J.H.; Stiasny, K.; Weseslindtner, L. Measuring Variant-Specific Neutralizing Antibody Profiles after Bivalent SARS-CoV-2 Vaccinations by a Multivariant Surrogate Virus Neutralization Microarray. Vaccines 2024, 12, 94. [Google Scholar] [CrossRef] [PubMed]
- Springer, D.N.; Reuberger, E.; Borsodi, C.; Puchhammer-Stöckl, E.; Weseslindtner, L. Comparison of anti-nucleocapsid antibody assays for the detection of SARS-CoV-2 Omicron vaccine breakthroughs after various intervals since the infection. J. Med. Virol. 2023, 95, e29229. [Google Scholar] [CrossRef]
- Vergori, A.; Cozzi-Lepri, A.; Matusali, G.; Colavita, F.; Cicalini, S.; Galli, P.; Garbuglia, A.R.; Fusto, M.; Puro, V.; Maggi, F.; et al. SARS-CoV-2 Omicron Variant Neutralization after Third Dose Vaccination in PLWH. Viruses 2022, 14, 1710. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Springer, D.N.; Daller, S.; Knappik, M.; Prüger, K.; Hartl, S.; Breyer-Kohansal, R.; Puchhammer-Stöckl, E.; Aberle, J.H.; Weseslindtner, L.; Breyer, M.K. A Multivariant Surrogate Virus Neutralization Test Demonstrates Distinct SARS-CoV-2-Specific Antibody Responses in People Living with HIV after a Fourth Monovalent mRNA Vaccination or an Omicron Breakthrough Infection. Diagnostics 2024, 14, 822. https://doi.org/10.3390/diagnostics14080822
Springer DN, Daller S, Knappik M, Prüger K, Hartl S, Breyer-Kohansal R, Puchhammer-Stöckl E, Aberle JH, Weseslindtner L, Breyer MK. A Multivariant Surrogate Virus Neutralization Test Demonstrates Distinct SARS-CoV-2-Specific Antibody Responses in People Living with HIV after a Fourth Monovalent mRNA Vaccination or an Omicron Breakthrough Infection. Diagnostics. 2024; 14(8):822. https://doi.org/10.3390/diagnostics14080822
Chicago/Turabian StyleSpringer, David Niklas, Simon Daller, Michael Knappik, Katja Prüger, Sylvia Hartl, Robab Breyer-Kohansal, Elisabeth Puchhammer-Stöckl, Judith Helene Aberle, Lukas Weseslindtner, and Marie Kathrin Breyer. 2024. "A Multivariant Surrogate Virus Neutralization Test Demonstrates Distinct SARS-CoV-2-Specific Antibody Responses in People Living with HIV after a Fourth Monovalent mRNA Vaccination or an Omicron Breakthrough Infection" Diagnostics 14, no. 8: 822. https://doi.org/10.3390/diagnostics14080822
APA StyleSpringer, D. N., Daller, S., Knappik, M., Prüger, K., Hartl, S., Breyer-Kohansal, R., Puchhammer-Stöckl, E., Aberle, J. H., Weseslindtner, L., & Breyer, M. K. (2024). A Multivariant Surrogate Virus Neutralization Test Demonstrates Distinct SARS-CoV-2-Specific Antibody Responses in People Living with HIV after a Fourth Monovalent mRNA Vaccination or an Omicron Breakthrough Infection. Diagnostics, 14(8), 822. https://doi.org/10.3390/diagnostics14080822