
Comparative Analysis of Vascular Calcification Risk Factors in Pre-Hemodialysis and Prevalent Hemodialysis Adult Patients: Insights into Calcification Biomarker Associations and Implications for Intervention Strategies in Chronic Kidney Disease
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biochemical Analyses
2.2. Calcification Assessment
2.3. Statistical Analysis
3. Results
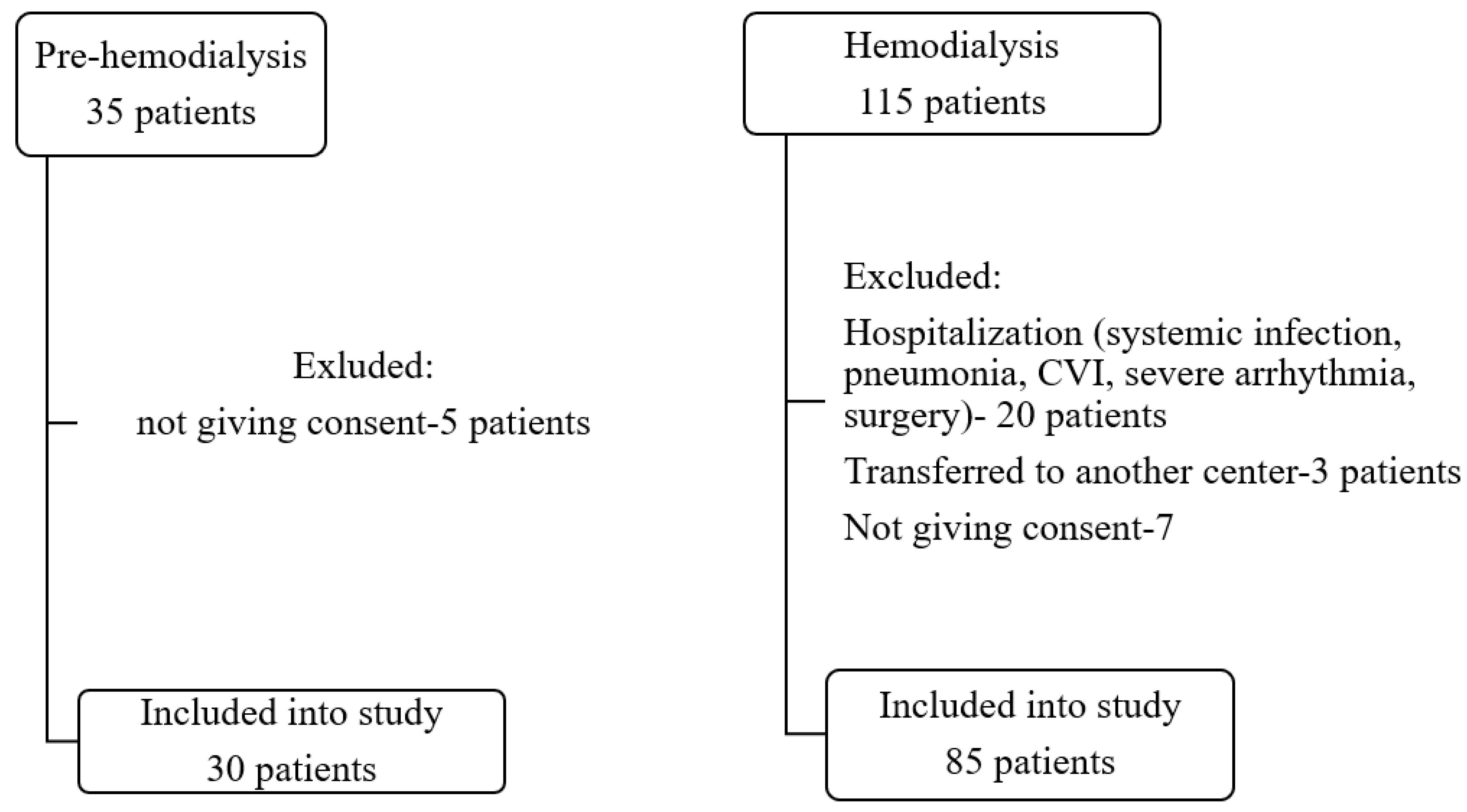
3.1. Study Population
3.2. Laboratory Analyses
3.3. Predictors of Vascular Calcification in Studied Groups
4. Discussion
4.1. Association of Biomarkers and Vascular Calcification in Pre-HD and HD Group of Patients
4.2. Other Risk Factors for VC in Pre-HD and HD Group of Patients
4.3. Significance and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ortiz, A.; Covic, A.; Fliser, D.; Fouque, D.; Goldsmith, D.; Kanbay, M.; Mallamaci, F.; Massy, Z.A.; Rossignol, P.; Vanholder, R.; et al. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet 2014, 383, 1831–1843. [Google Scholar] [CrossRef] [PubMed]
- Budoff, M.-J.; Rader, D.-J.; Reilly, M.-P.; Mohler, E.-R., 3rd; Lash, J.; Yang, W.; Rosen, L.; Glenn, M.; Teal, V.; Feldman, H.-I.; et al. Relationship of estimated GFR and coronary artery calcification in the CRIC (Chronic Renal Insufficiency Cohort) Study. Am. J. Kidney Dis. 2011, 58, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Kestenbaum, B.R.; Adeney, K.-L.; de Boer, I.-H.; Ix, J.-H.; Shlipak, M.-G.; Siscovick, D.-S. Incidence and progression of coronary calcification in chronic kidney disease: The Multi-Ethnic Study of Atherosclerosis. Kidney Int. 2009, 76, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Schlieper, G.; Schurgers, L.; Brandenburg, V.; Reutlings-Perger, C.; Floege, J. Vascular calcification in chronic kidney disease: An update. Nephrol. Dial. Transplant. 2016, 31, 31–39. [Google Scholar] [CrossRef] [PubMed]
- London, G.-M.; Marchais, S.J.; Guérin, A.-P.; Métivier, F. Arteriosclerosis, vascular calcifications and cardiovascular disease in uremia. Curr. Opin. Nephrol. Hypertens. 2005, 14, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Gungor, O.; Kocyigit, I.; Yilmaz, M.-I.; Sezer, S. Role of vascular calcification inhibitors in preventing vascular dysfunction and mortality in hemodialysis patients. Semin. Dial. 2018, 31, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M. Update on fibroblast growth factor 23 in chronic kidney disease. Kidney Int. 2012, 82, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Kakani, E.; Elyamny, M.; Ayach, T.; El-Husseini, A. Pathogenesis and management of vascular calcification in CKD and dialysis patients. Semin. Dial. 2019, 32, 553–561. [Google Scholar] [CrossRef]
- Werida, R.H.; Abou-Madawy, S.; Abdelsalam, M.; Helmy, M.W. Omega 3 fatty acids effect on the vascular calcification biomarkers fetuin A and osteoprotegerin in hemodialysis patients. Clin. Exp. Med. 2022, 22, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Caluwé, R.; Pyfferoen, L.; De Boeck, K.; De Vriese, A.S. The effects of vitamin K supplementation and vitamin K antagonists on progression of vascular calcification: Ongoing randomized controlled trials. Clin. Kidney J. 2016, 9, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Di Lullo, L.; Tripepi, G.; Ronco, C.; D’Arrigo, G.; Barbera, V.; Russo, D.; Di Iorio, B.R.; Uguccioni, M.; Paoletti, E.; Ravera, M.; et al. Cardiac valve calcification and use of anticoagulants: Preliminary observation of a potentially modifiable risk factor. Int. J. Cardiol. 2019, 278, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Hamano, T.; Obi, Y.; Monden, C.; Oka, T.; Yamaguchi, S.; Matsui, I.; Hashimoto, N.; Matsumoto, A.; Shimada, K.; et al. A Randomized Trial of Magnesium Oxide and Oral Carbon Adsorbent for Coronary Artery Calcification in Predialysis CKD. J. Am. Soc. Nephrol. 2019, 30, 1073–1085. [Google Scholar] [CrossRef] [PubMed]
- Ketteler, M.; Block, G.-A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.-A.; McCann, L.; Moe, S.-M.; Shroff, R.; Tonelli, M.-A.; Toussaint, N.-D.; et al. Executive summary of the 2017 KDIGO chronic kidney disease-mineral and bone disorder (CKD-MBD) guideline update: What’s changed and why it matters. Kidney Int. 2017, 92, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De-Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W.; Wagner, C.L. Normal serum vitamin D levels. N. Engl. J. Med. 2005, 352, 515–516. [Google Scholar] [CrossRef] [PubMed]
- Adragao, T.; Pires, A.; Lucas, C.; Birne, R.; Magalhaes, L.; Gonçalves, M.; Negrao, A.-P. A simple vascularcalcification score predicts cardiovascular risk in haemodialysis patients. Nephrol. Dial. Transpl. 2004, 19, 1480–1488. [Google Scholar] [CrossRef] [PubMed]
- Gorriz, J.-L.; Molina, P.; Cerveron, M.-J.; Vila, R.; Bover, J.; Nieto, J.; Barril, G.; Martínez-Castelao, A.; Fernández, E.; Escudero, V.; et al. Vascular calcification in patients with nondialysis CKD over 3 years. Clin. J. Am. Soc. Nephrol. 2015, 10, 654–666. [Google Scholar] [CrossRef] [PubMed]
- Damjanovic, T.; Djuric, Z.; Markovic, N.; Dimkovic, S.; Radojicic, Z.; Dimkovic, N. Screening of vascular calcifications in patients with end-stage renal diseases. Gen. Physiol. Biophys. 2009, 28, 277–283. [Google Scholar] [PubMed]
- Zhang, H.; Li, G.; Yu, X.; Yang, J.; Jiang, A.; Cheng, H.; Fu, J.; Liang, X.; Liu, J.; Lou, J.; et al. China Dialysis Calcification Study Group. Progression of Vascular Calcification and Clinical Outcomes in Patients Receiving Maintenance Dialysis. JAMA Netw. Open 2023, 6, e2310909. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Nayeri, H.; Nasri, H. Association of fetuin-A with kidney disease; a review on current concepts and new data. J. Nephropharmacol. 2019, 8, e14. [Google Scholar] [CrossRef]
- Ketteler, M.; Bongartz, P.; Westenfeld, R.; Wildberger, J.-E.; Mahnken, A.-H.; Böhm, R.; Metzger, T.; Wanner, C.; Jahnen-Dechent, W.; Floege, J. Association of low fetuin-A (AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: A cross-sectional study. Lancet 2003, 361, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Ulutas, O.; Taskapan, M.-C.; Dogan, A.; Baysal, T.; Taskapan, H. Vascular calcification is not related to serum fetuin-A and osteopontin levels in hemodialysis patients. Int. Urol. Nephrol. 2018, 50, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.-R.; Olauson, H.; Witasp, A.; Haarhaus, M.; Brandenburg, V.; Wernerson, A.; Lindholm, B.; Söderberg, M.; Wennberg, L.; Nordfors, L.; et al. Increased circulating sclerostin levels in end-stage renal disease predict biopsy-verified vascular medial calcification and coronary artery calcification. Kidney Int. 2015, 88, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Claes, K.-J.; Viaene, L.; Heye, S.; Meijers, B.; d’Haese, P.; Evenepoel, P. Sclerostin: Another vascular calcification inhibitor? J. Clin. Endocrinol. Metab. 2013, 98, 3221–3228. [Google Scholar] [CrossRef]
- Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.-H.; Scialla, J.; Wahl, P.; Gutiérrez, O.-M.; Steigerwalt, S.; He, J.; et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011, 305, 2432–2439. [Google Scholar] [CrossRef] [PubMed]
- Nasrallah, M.-M.; El-Shehaby, A.-R.; Salem, M.-M.; Osman, N.-A.; El Sheikh, E.; Sharaf, E.-l.; Din, U.-A. Fibroblast growth factor-23 (FGF-23) is indepenently correlated to aortic calcification in haemodialysis patients. Nephrol. Dial. Transplant. 2010, 25, 2679–2685. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, L.; Liabeuf, S.; Renard, C.; Lenglet, A.; Lemke, H.-D.; Choukroun, G.; Drueke, T.-B.; Massy, Z.-A.; European Uremic Toxin (EUTox) Work Group. FGF-23 is independently associated with vascular calcification but not bone mineral density in patients at various CKD stages. Osteoporos. Int. 2012, 23, 2017–2025. [Google Scholar] [CrossRef] [PubMed]
- Baralić, M.; Brković, V.; Stojanov, V.; Stanković, S.; Lalić, N.; Đurić, P.; Đukanović, L.; Kašiković, M.; Petrović, M.; Petrović, M.; et al. Dual Roles of the Mineral Metabolism Disorders Biomarkers in Prevalent Hemodilysis Patients: In Renal Bone Disease and in Vascular Calcification. J. Med. Biochem. 2019, 38, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Scialla, J.-J.; Lau, W.-L.; Reilly, M.-P.; Isakova, T.; Yang, H.-Y.; Crouthamel, M.-H.; Chavkin, N.-W.; Rahman, M.; Wahl, P.; Amaral, A.-P.; et al. Chronic Renal Insufficiency Cohort Study Investigators. Fibroblast growth factor 23 is not associated with and does not induce arterial calcification. Kidney Int. 2013, 83, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Souberbielle, J.C.; Roth, H.; Fouque, D.P. Parathyroid hormone measurement in CKD. Kidney Int. 2010, 77, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Cannata-Andia, J.-B.; Rodriguez, G.-M.; Gomez, A.-C. Osteoporosis and adynamic bone in chronic kidney disease. J. Nephrol. 2013, 26, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Barreto, F.C.; Barreto, D.V.; Moysés, R.M.; Neves, K.R.; Canziani, M.E.; Draibe, S.A.; Jorgetti, V.; Carvalho, A.B. K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease in hemodialysis patients. Kidney Int. 2008, 73, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Ureña, P.; De Vernejoul, M.C. Circulating biochemical markers of bone remodeling in uremic patients. Kidney Int. 1999, 55, 2141–2156. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.; Towler, D.A. Arterial calcification and bone physiology: Role of the bone-vascular axis. Nat. Rev. Endocrinol. 2012, 8, 529–543. [Google Scholar] [CrossRef] [PubMed]
- Hernandes, F.R.; Canziani, M.E.; Barreto, F.C.; Santos, R.O.; Moreira, V.M.; Rochitte, C.E.; Carvalho, A.B. The shift from high to low turnover bone disease after parathyroidectomy is associated with the progression of vascular calcification in hemodialysis patients: A 12-month follow-up study. PLoS ONE 2017, 12, e0174811. [Google Scholar] [CrossRef] [PubMed]
- London, G.M.; Marty, C.; Marchais, S.J.; Guerin, A.P.; Metivier, F.; de Vernejoul, M.C. Arterial calcifications and bone histomorphometry in end-stage renal disease. J. Am. Soc. Nephrol. 2004, 15, 1943–1951. [Google Scholar] [CrossRef] [PubMed]
- Adragao, T.; Ferreira, A.; Frazao, J.M.; Papoila, A.L.; Pinto, I.; Monier-Faugere, M.C.; Malluche, H.H. Higher mineralized bone volume is associated with a lower plain X-Ray vascular calcification score in hemodialysis patients. PLoS ONE 2017, 12, e0179868. [Google Scholar] [CrossRef] [PubMed]
- Persy, V.; D’Haese, P. Vascular calcification and bone disease: The calcification paradox. Trends Mol. Med. 2009, 15, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Drüeke, T.B. Hyperparathyroidism in Chronic Kidney Disease. [Updated 18 October 2021]. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/sites/books/NBK278975/ (accessed on 11 February 2024).
- Bisson, S.K.; Ung, R.V.; Mac-Way, F. Role of the Wnt/β-Catenin Pathway in Renal Osteodystrophy. Int. J. Endocrinol. 2018, 2018, 5893514. [Google Scholar] [CrossRef] [PubMed]
- Pietrzyk, B.; Wyskida, K.; Ficek, J.; Kolonko, A.; Ficek, R.; Więcek, A.; Olszanecka-Glinianowicz, M.; Chudek, J. Relationship between plasma levels of sclerostin, calcium-phosphate disturbances, established markers of bone turnover, and inflammation in haemodialysis patients. Int. Urol. Nephrol. 2019, 51, 519–526. [Google Scholar] [CrossRef]
- Wu, P.-Y.; Lee, S.-Y.; Chang, K.-V.; Chao, C.-T.; Huang, J.-W. Gender-Related Differences in Chronic Kidney Disease-Associated Vascular Calcification Risk and Potential Risk Mediators: A Scoping Review. Healthcare 2021, 9, 979. [Google Scholar] [CrossRef] [PubMed]
- Becs, G.; Zarjou, A.; Agarwal, A.; Kovács, K.É.; Becs, Á.; Nyitrai, M.; Balogh, E.; Bányai, E.; Eaton, J.W.; Arosio, P.; et al. Pharmacological induction of ferritin prevents osteoblastic transformation of smooth muscle cells. J. Cell. Mol. Med. 2016, 20, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.C.; Liu, W.C.; Zheng, C.M.; Zheng, J.Q.; Yen, T.H.; Lu, K.C. Role of Vitamin D in Uremic Vascular Calcification. BioMed Res. Int. 2017, 2017, 2803579. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.; Akizawa, T.; Bavanandan, S.; Hamano, T.; Liew, A.; Lu, K.C.; Lumlertgul, D.; Oh, K.H.; Zhao, M.H.; Ka-Shun Fung, S.; et al. 2017 Kidney Disease: Improving Global Outcomes (KDIGO) Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update Implementation: Asia Summit Conference Report. Kidney Int. Rep. 2019, 4, 1523–1537. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pre-HD (N = 30) | HD (N = 85) | p | |
|---|---|---|---|
| Demographics | |||
| Age, years | 66.7 ± 14.96 | 57.72 ± 13.07 | 0.023 |
| Sex, m/f | 19/11 | 40/45 | 0.141 |
| Underlying kidney disease: (%) | |||
| GN | 3 (10) | 15 (17.6) | 0.394 |
| Nephroangiosclerosis | 6 (20) | 14 (16.5) | 0.779 |
| ADPKD | 2 (6.7) | 8 (9.4) | 1.000 |
| T2DM | 5 (9.4) | 8 (9.4) | 0.442 |
| Nephrolithiasis | 1 (3.3) | 12 (14.1) | 0.178 |
| Others | 13 (43.3) | 28 (32.9) | 0.376 |
| Co-morbidities, yes (%) | |||
| T2DM | 4 (13.3) | 14 (16.4) | 0.778 |
| Hypertension | 27 (90) | 65 (76.7) | 0.029 |
| CVD | 14 (46.7) | 34 (34.1) | 0.527 |
| CVI | 2 (6.7) | 10 (10.6) | 0.728 |
| tumor | 1 (3.3) | 8 (8.2) | 0.442 |
| Treatment, no (%) | |||
| ESA | 7 (23.3) | 36 (64.3) | 0.080 |
| Phosphate binder | 21 (70) | 80 (94.1) | 0.001 |
| Alpha D3 | 9 (30) | 25 (29.4) | 1.000 |
| Antihypertensive | 16 (53.3) | 62 (72.9) | 0.068 |
| VC score, no (%) | |||
| 0 | 16 (53.3) | 36 (42.35) | 0.393 |
| 1–2 | 4 (13.3) | 18 (21.2) | 0.384 |
| ≥3 | 10 (33.3) | 31 (37.47) | 0.756 |
| ≥6 (8) | 1 (0) | 15 (6) | 0.030 |
| Pre-HD (N = 30) | HD (N = 85) | p | |
|---|---|---|---|
| Cholesterol, mmol/L | 4.83 ± 1.32 | 4.59 ± 1.24 | 0.109 |
| Triglyceride, mmol/L | 1.4 (0.8) | 1.65 (1.2–2.8) | 0.804 |
| Hemoglobin, g/L | 106 (96.7–114.5) | 108 (101.5–116.5) | 0.384 |
| Glycaemia, mmol/L | 5.2 (4.7–5.55) | 4.9 (4.2–6.05) | 0.663 |
| Creatinine, µmol/L | 552.5 (318–731.2) | 808 (705.5–915) | 0.000 |
| Urea, mmol/L | 23.4 (14.2–32.95) | 21.0 (17.9–26.0) | 0.327 |
| Urate, µmol/L | 386.70 ± 99.1 | 362.1 ± 88.9 | 0.201 |
| Sodium, mmol/L | 139.87 ± 3.96 | 137.86 ± 2.98 | 0.022 |
| Potassium, mmol/L | 4.85 ± 0.80 | 5.29 ± 0.69 | 0.008 |
| Calcium, mmol/L | 2.16 (2.05–2.28) | 2.19 (2.1–2.31) | 0.541 |
| Phosphate, mmol/L | 1.53 (1.1–1.8) | 1.65 (1.3–2.03) | 0.247 |
| Ferritin, µg/L | 84.3 (50.75–231.87) | 355 (131.7–490.1) | 0.000 |
| Alkaline phosphatase, IU/L | 73.5 (61.5–99.2) | 87 (60–109) | 0.304 |
| Ln (iPTH), pg/mL | 4.97 ± 1.0 | 4.61 ± 1.37 | 0.279 |
| <100 * | 11 (36.6%) | 36 (42.3%) | |
| 25(OH)D, ng/mL | 24.7 (46.22) | 27.5 (19.2–48.05) | 0.879 |
| <29 * (deficiency + insufficiency) | 19 (64.28) | 45 (53.6%) | |
| Ln (Fetuin A), ng/mL | 6.24 ± 0.25 | 5.85 ± 0.43 | 0.001 |
| Ln (Sclerostin), pg/mL | 8.12 ± 0.36 | 7.54 ± 0.91 | 0.012 |
| Ln (FGF 23), pg/mL | 5.01 ± 0.75 | 6.48 ± 1.11 | 0.000 |
| Pre HD Group | HD Group | p | |||
|---|---|---|---|---|---|
| 1 VC + | 2 VC Neg | 3 VC + | 4 VC Neg | ||
| Number | 14 | 16 | 49 | 36 | |
| Age, years | 71.7 ± 7.96 | 62.5 ± 18.98 | 58.66 ± 13.24 | 56.43 ± 13.07 | 1 vs. 3, 4, p < 0.001 |
| Sex, m/f | 12/2 | 7/9 | 23/26 | 17/19 | 1 vs. 2, 3, 4, p < 0.02 |
| ESA, yes/no | 2/12 | 5/11 | 20/29 | 16/20 | 1 vs. 4, p = 0.05 |
| Phosphate binder, yes/no | 9/5 | 12/4 | 47/2 | 33/3 | 1 vs. 3, 4, p < 0.03 2 vs. 3, p = 0.028 |
| Phosphate, mmol/L | 1.57 ± 0.68 | 1.51 ± 0.33 | 1.54 ± 0.38 | 1.87 ± 0.52 | 4 vs. 2, 3, p < 0.018 |
| Phosphate range, mmol/L <1.0 1.0–1.8 ≥1.9 | 2 8 4 * | 2 12 2 * | 2 37 a 10 b,* | 0 18 a 18 b,* | a p = 0.020 b p= 0.005 * 2 + 4 vs. 1 + 3, p = 0.057 |
| Ln(FGF 23), pg/mL | 6.31 (5.98–6.40) | 6.26 (6.14–6.30) | 5.83 (5.62–6.17) | 5.95 (5.46–6.10) | 2 vs. 3, 4, p < 0.0001 1 vs. 3, 4, p < 0.004 |
| Ln(Fetuin A), ng/mL | 4.67 (4.17–5.57) | 5.13 (4.31–5.60) | 6.92 (5.91–7.31) | 7.16 (5.85–7.31) | 1 vs. 3, 4, p = 0.001 2 vs. 3, 4, p < 0.003 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Variables | Standardized Coefficients (95% CI) | p | Standardized Coefficients (95% CI) | p |
| Ln (Fetuin A), ng/mL | −0.249 (−7.037–−1.858) | 0.120 | −0.701 (−0.030–−0.024) | 0.001 |
| Ln (Sclerostin), pg/mL | 0.590 (1.364–5.651) | 0.003 | 0.970 (4.222–5.764) | 0.001 |
| Ln (FGF 23), pg/mL | 0.343 (−0.233–2.277) | 0.103 | ||
| Gender | −0.409 (−3.101–−0.229) | 0.025 | −1.607 (−8.128–−6.803) | 0.000 |
| Age | 0.309 (−0.008–0.089) | 0.096 | 1.269 (0.148–0.177) | 0.000 |
| Diagnosis | −0.137 (−0.526–0.249) | 0.471 | ||
| Hemoglobin, g/L | −0.489 (−0.123–0.002) | 0.057 | ||
| s-creatinine, µmol/L | −0.023 (−0.004–0.004) | 0.935 | ||
| s-urea, mmol/L | −0.238 (−0.139–0.056) | 0.391 | ||
| s-urate, µmol/L | 0.010 (−0.007–0.007) | 0.963 | ||
| s-calcium, mmol/L | −0.075 (−6.067–4.848) | 0.812 | ||
| s-phosphate, mmol/L | 0.012 (−1.866–1.957) | 0.961 | ||
| Alk. Phosphatase, IU/L | 0.085 (−0.014–0.020) | 0.681 | ||
| Ln (iPTH), pg/mL | −0.456 (−0.005–0.004) | 0.030 | ||
| Ferritin, µg/L | −0.241 (−0.012–0.003) | 0.083 | −0.252 (−0.007–−0.002) | 0.014 |
| Phosphate binder | −0.097 (−2.060–0.788) | 0.612 | ||
| Vit D treatment | −0.177 (−2.247–0.796) | 0.104 | −0.187 (−1.259–−0.274) | 0.022 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Variables | Standardized Coefficient (95% CI) | p | Standardized Coefficient (95% CI) | p |
| Ferritin, µg/L | 0.014 (−0.002–0.002) | 0.934 | ||
| (Ln) Fetuin A, ng/mL | −0.238 (−4.446–1.331) | 0.280 | ||
| (Ln) Sclerostin, pg/mL | 0.322 (0.333–2.247) | 0.102 | 0.902 (1.967–3.542) | 0.001 |
| (Ln) FGF 23, pg/mL | −0.105 (−0.407–0.003) | 0.109 | 0.593 (1.216–2.568) | 0.001 |
| Gender, male | 0.089 (−0.911–1.862) | 0.495 | ||
| Age | −0.008 (−0.106–0.102) | 0.971 | ||
| dialysis vintage, months | −0.018 (−0.009–0.008) | 0.892 | ||
| Diagnosis | 0.195 (−0.296–0.776) | 0.359 | ||
| s-cholesterol, mmol/L | 0.697 (−0.005–2.640) | 0.051 | ||
| Hemoglobin, g/L | −0.286 (−0.146–0.025) | 0.156 | ||
| s-creatinine, µmol/L | 0.065 (−0.002–0.004) | 0.618 | ||
| s-urea, mmol/L | 0.565 (−0.001–0.491) | 0.051 | 0.446 (0.069–0.318) | 0.004 |
| s-urate, µmol/L | −0.066 (−0.010–0.006) | 0.614 | ||
| s-calcium, mmol/L | 0.019 (−3.817–4.42) | 0.884 | ||
| s-phosphate, mmol/L | 0.035 (−0.976–1.247) | 0.807 | ||
| Alk. Phosphatase, IU/L | −0.046 (−0.018–0.013) | 0.727 | ||
| (Ln) iPTH, pg/mL | −0.080 (−0.419–−0.246) | 0.058 | −0.895 (−1.049–−0.008) | 0.001 |
| Phosphate binder | 0.013 (−3.051–3.384) | 0.918 | ||
| Vit. D treatment | 0.118 (−0.837–2.246) | 0.364 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrović, M.; Brković, V.; Baralić, M.; Marić, I.; Petković, N.; Stanković, S.; Lalić, N.; Stanisavljević, D.; Đukanović, L.; Ležaić, V. Comparative Analysis of Vascular Calcification Risk Factors in Pre-Hemodialysis and Prevalent Hemodialysis Adult Patients: Insights into Calcification Biomarker Associations and Implications for Intervention Strategies in Chronic Kidney Disease. Diagnostics 2024, 14, 824. https://doi.org/10.3390/diagnostics14080824
Petrović M, Brković V, Baralić M, Marić I, Petković N, Stanković S, Lalić N, Stanisavljević D, Đukanović L, Ležaić V. Comparative Analysis of Vascular Calcification Risk Factors in Pre-Hemodialysis and Prevalent Hemodialysis Adult Patients: Insights into Calcification Biomarker Associations and Implications for Intervention Strategies in Chronic Kidney Disease. Diagnostics. 2024; 14(8):824. https://doi.org/10.3390/diagnostics14080824
Chicago/Turabian StylePetrović, Marko, Voin Brković, Marko Baralić, Ivko Marić, Nenad Petković, Sanja Stanković, Nataša Lalić, Dejana Stanisavljević, Ljubica Đukanović, and Višnja Ležaić. 2024. "Comparative Analysis of Vascular Calcification Risk Factors in Pre-Hemodialysis and Prevalent Hemodialysis Adult Patients: Insights into Calcification Biomarker Associations and Implications for Intervention Strategies in Chronic Kidney Disease" Diagnostics 14, no. 8: 824. https://doi.org/10.3390/diagnostics14080824