Abstract
Respiratory viral infections have been found to have a negative impact on neurological functions, potentially leading to significant neurological impairment. The SARS-CoV-2 virus has precipitated a worldwide pandemic, posing a substantial threat to human lives. Growing evidence suggests that SARS-CoV-2 may severely affect the CNS and respiratory system. The current prevalence of clinical neurological issues associated with SARS-CoV-2 has raised significant concerns. However, there needs to be a more comprehensive understanding of the specific pathways by which SARS-CoV-2 enters the nervous system. Based on the available evidence, this review focuses on the clinical neurological manifestations of SARS-CoV-2 and the possible mechanisms by which SARS-CoV-2 invades the brain.
1. Introduction
Respiratory diseases resulting from viral agents pose a significant challenge to public health. Such conditions annually contribute to elevated levels of illness and death, particularly among vulnerable populations such as youngsters, older adults, and individuals with compromised immune systems [1]. The primary viral agents responsible for respiratory diseases include coronavirus (CoV), influenza virus (IV), human respiratory syncytial virus (hRSV, orthopneumoviruses), and human metapneumovirus (hMPV, metapneumoviruses) [2]. The primary transmission mode for these viruses is through direct contact with contaminated objects or inhalation of suspended droplets [3,4].
All of these viruses share the common characteristic of being able to cause bronchiolitis and pneumonia, resulting in a significant number of hospitalizations during each winter season [5,6]. In addition to the seasonal viruses that affect the respiratory system, new strains of these viruses periodically spread among people, resulting in epidemics or even pandemics. Typically, these viruses belong to the RNA viral group, including influenza A subtypes and strains of human coronaviruses. These viruses exist within an animal reservoir and can traverse the species barrier, adapting to and infecting a new host [2,7]. The most recent emerging virus, known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV2), was discovered in December 2019 in a person residing in the Chinese city of Wuhan. This person showed severe pneumonia symptoms. The World Health Organization (WHO) officially designated the illness as COVID-19 and labeled it a worldwide pandemic of significant concern [2].
The similarity between SARS-CoV-2 and coronaviruses found in bats and pangolins exceeds 90%, indicating a significant capacity for cross-species transmission [8]. The virus has a spherical morphology similar to other coronaviruses (CoVs) [9,10], measuring around 100 nm in diameter. It is classified as a single-stranded positive-sense RNA virus. It consists of four kinds of proteins: membrane (M) glycoprotein, spike (S) glycoprotein, envelope (E) glycoprotein, and nucleocapsid (N) protein [11]. Research revealed that the SARS-CoV-2 virus can attach to the angiotensin-converting enzyme 2 (ACE2) receptors. This binding process occurs in the presence of a protein called S protein and requires the involvement of the transmembrane protein serine protease 2 (TMPRSS2). Consequently, cells that express ACE2 receptors become vulnerable to viral infection [12,13].
It is essential to acknowledge that, besides impacting the airways, this newly developing virus can also have severe consequences for various other areas of the human body, such as the central nervous system (CNS). As a result, there is a potential escalation in susceptibility to neurological illnesses and neurodegenerative conditions [1,14]. The invasion of the CNS and its resulting pathology have been extensively investigated in infections caused by various viruses, including Japanese encephalitis virus (JEV), measles virus (MV), human immunodeficiency virus (HIV), and Varicella-Zoster virus (VZV), among others [15]. A growing interest exists in enhancing our understanding of the characteristics and mechanisms associated with neurological manifestations [16,17]. Patients with severe respiratory illnesses exhibit various clinical signs associated with neurological abnormalities, as outlined in Table 1.
Following the discovery of the first COVID-19 case in Wuhan, SARS-CoV-2 spread quickly worldwide and infected many people; according to WHO data, the global count of clinically confirmed COVID-19 cases exceeds 163 million, with a death toll of almost 3.3 million. Initially, COVID-19 was characterized as a respiratory disease presenting symptoms such as fever, tiredness, dyspnea, cough, and abnormal chest X-ray findings [18,19]. Additionally, many COVID-19 patients experience neurological symptoms such as ataxia, headaches, myalgia, drowsiness, hypogeusia, and hyposmia during infection [20,21,22]. SARS-CoV-2 has been extensively investigated as a causative agent for numerous neurological disorders [23].
However, the mechanisms by which SARS-CoV-2 impacts the CNS still need to be fully understood. This paper comprehensively analyses previously recorded CNS and PNS diseases associated with SARS-CoV-2. Additionally, we explore the various probable pathways of neuroinvasiveness, aiming to enhance neurologists’ understanding of the influence of SARS-CoV-2 on the CNS. This understanding will aid in diagnosing and developing appropriate treatment strategies for COVID-19.

Table 1.
Neurologic manifestations associated with severe viral respiratory infections.
Table 1.
Neurologic manifestations associated with severe viral respiratory infections.
| Respiratory Viruses | Virus Overview | Neurological Complications | Ref. |
|---|---|---|---|
| Human Coronaviruses (SARS-CoV1, MERS-CoV, SARS-CoV2) |
|
| [24,25,26,27,28,29,30,31,32,33] |
| Influenza A Viruses (H1N1, H3N2, H5N1, H7N7) |
|
| [34,35,36,37,38,39] |
| Human Respiratory Syncytial Virus/Orthopneumovirus |
|
| [37,40] |
| Human Metapneumovirus |
|
| [41,42,43] |
No matter what manifestations or damage in the CNS, neurologically impaired functions need to be restored. Clinical reports of novel neurorestorative treatments have recently improved the neurological processes of patients with CNS diseases and damage [44,45,46,47,48].
2. Respiratory Virus Transmission Routes to the Nervous System
The CNS serves as the primary regulatory entity of the human body and, therefore, requires specific measures to safeguard it against internal and external threats [49,50]. Hence, despite being closely related to the surrounding environment, the CNS is predominantly shielded from unrestricted infiltration of harmful substances, infections, and circulating antibodies in the bloodstream. This safeguarding is accomplished through the presence of the blood–brain barrier (BBB) and the blood–cerebrospinal fluid barrier (BCSFB), which are situated in the choroid plexus located within the brain’s ventricles [51]. BBB maintenance is ensured through tight junctions connecting the endothelial cells of cerebral microvessels, the astrocytic end feet, pericytes, and the extracellular matrix [51]. However, it has been noted that specific respiratory viruses possessing neurotropic characteristics can disturb the tight junctions of the BBB and ultimately invade the cells inside the CNS.
Moreover, it has been observed that these viruses can get past the BBB by directly infecting endothelial cells and pericytes through endocytic vesicles, a mechanism commonly referred to as transcytosis. An alternative method of accessing the CNS is the “Trojan horse approach”. This approach involves the exploitation of neurotropic viruses, which can cross the BBB by employing infected monocytes or macrophages, commonly referred to as hematogenous routes [52,53]. The section below will examine SARS-CoV-2’s various transmission routes and their mechanisms.
3. Coronavirus
The Coronaviridae family comprises a group of RNA viruses initially identified in the 1960s from individuals exhibiting symptoms of upper respiratory tract infections [54]. Human variants of coronavirus (HCoV), specifically alphacoronavirus and betacoronavirus, are prevalent globally and typically manifest with the characteristic symptoms of HCoV, such as rhinitis, pharyngitis, laryngitis, bronchitis, and otitis [55]. In 2002, a novel strain of coronavirus known as Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) was discovered. This particular strain was found to have originated from bats. It was transmitted to humans through an intermediate reservoir via zoonotic transmission [56], and in contrast to the usual Human Coronavirus (HCoV) strains, SARS-CoV exhibited an exceptionally high level of virulence. This was further exacerbated by acute respiratory distress syndrome (ARDS), multiple organ dysfunction syndrome, and a mortality rate reaching up to 10% in affected individuals [56,57]. Due to zoonotic transmission, the Middle East Respiratory Syndrome Coronavirus (MERS-CoV), a new coronavirus, was discovered in 2012. A 35% fatality rate has been noted for this specific coronavirus strain, which is linked to the emergence of severe respiratory symptoms [58]. In 2019, a novel coronavirus strain, SARS-CoV-2, was identified. The viral pathogen has undergone rapid dissemination, resulting in the emergence of a pandemic outbreak at the beginning of 2020. The virus exhibits a significant degree of homology with the SARS-CoV and is responsible for developing severe and often fatal pneumonia known as COVID-19. The clinical manifestations of this disease closely resemble those observed in cases of SARS-CoV and MERS-CoV [59].
3.1. How SARS-CoV-2 Infections Affect the CNS
The Neuronal Pathway
The neuronal pathway serves as an essential pathway for neurotropic viruses to gain access to the central nervous system (CNS). Viruses have the ability to disseminate through the infection of sensory or motor nerve endings, employing retrograde or anterograde neural transport systems supported by motor proteins such as dynein and kinesins [53]. Olfactory neuron transport is an example of a neuronal pathway [2,60]. In the peripheral nervous system (PNS), the olfactory nerve is the primary pathway through which the SARS-CoV-2 virus infiltrates the CNS. This is primarily attributed to the higher presence of transmembrane protein serine protease 2 (TMPRSS2) and angiotensin-converting enzyme 2 (ACE2) within the olfactory epithelium cells. These proteins facilitate viral binding and accumulation [61,62,63,64]. The olfactory nerve can be classified as a CNS conduction loop rather than a typical nerve, as it establishes direct contact with the brain (Figure 1) [65,66]. The olfactory mucosa in the nasal cavity consists of neurons, basal cells, epithelial cilia, and Bowman’s glands [67,68]. The nasal cavity contains a unique neuroepithelium specialized for olfaction, characterized by sustentacular cells that primarily make up the apical surface [69]. Support cells were found to have high amounts of TMPRSS2 and ACE2 [70], demonstrating their susceptibility to SARS-CoV-2 infection [71].
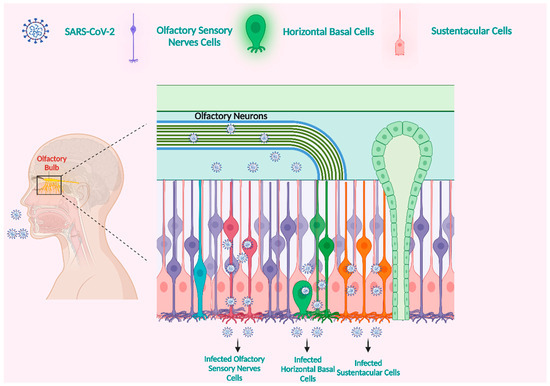
Figure 1.
The olfactory nerve is a potential entry point for SARS-CoV-2 into the brain. The ACE2 receptor is involved in SARS-CoV-2 infection of the olfactory mucosa. Horizontal basal cells with the ACE2 receptor are everywhere across the olfactory epithelium. Infection with SARS-CoV-2 is likely due to the expression of ACE2 in human horizontal basal cells. Horizontal basal cells can develop into olfactory neurons. We propose that horizontal basal cells infected with SARS-CoV-2 can develop into infected olfactory neurons. These infected olfactory neurons have synaptic connections with olfactory bulb (OB) neurons. The central nervous system (CNS) could subsequently become infected. The OB is connected to numerous regions of the brain. This facilitates the spread of the virus to multiple brain regions quickly. Created with BioRender.com (https://app.biorender.com/illustrations/64901c58f8f3b377cd55200b, accessed on 28 August 2023).
In addition to the olfactory nerve, it has been suggested that SARS-CoV-2 may utilize other possible peripheral nerves, such as the nasopharyngeal nerves, trigeminal, and vagus, to access the brain. From an anatomical perspective, the vagus nerve is a component of the digestive nervous system and establishes connections with digestive pathways that exhibit heightened levels of NRP1 and ACE2 expression. ACE2 and TMPRRSS2 are found in intestinal enteric neurons and glia, suggesting their vulnerability to SARS-CoV-2 [72]. The gut–brain connection is significant in developing CNS diseases [73]. A comprehensive analysis of 42 individuals diagnosed with COVID-19 revealed that around 66.67% of the mentioned patients exhibited the presence of SARS-CoV-2 RNA in their stools [74]. In an experimental setting, it was demonstrated that SARS-CoV-2 can infect the epithelial cells of the human intestines [75]. Therefore, it is reasonable to conclude that enterocytes infected with SARS-CoV-2 may potentially disseminate to neuronal and glial cells within the enteric nervous system, ultimately leading to the invasion of the central nervous system via the vagus nerve [61,76].
3.2. Hematogenous Route
The hematogenous pathway is a potential path through which SARS-CoV-2 may gain access to the brain, as it involves circulating the virus within the bloodstream [1,2]. In this circumstance, the blood–brain barrier (BBB) is a frequently utilized pathway for disseminating the virus to the central nervous system (CNS). SARS-CoV-2 infiltrates the central nervous system (CNS) via the hematogenous pathway by employing two distinct mechanisms. Firstly, it infects vascular endothelial cells, allowing them to pass through the BBB. Secondly, it triggers inflammatory responses that lead to the disruption of the BBB.
3.2.1. SARS-CoV-2 Infection of Vascular Endothelial Cells and Crossing the BBB
Available reports show that the inflammation and disruption of epithelial barrier cells facilitate the virus’s ability to infiltrate the lymphatic vessels and circulatory system, subsequently leading to its dissemination to different organs, including the brain [23]. The autopsy of lung tissue from five patients who tested positive for COVID-19 showed the presence of viral proteins within the lungs’ capillaries. Furthermore, infection with the SARS-CoV-2 virus resulted in the death of endothelial cells and damage to the capillaries [77]. Although the incidence of SARS-CoV-2 detection in blood samples of COVID-19 patients remains relatively low, it does imply the potential for viral dissemination within the bloodstream and subsequent involvement of various organs, including the brain [78]. Upon entering the bloodstream, the virus can quickly infect the endothelial cells within the vasculature. This is facilitated by the presence of ACE2, TMPRSS2, and NRP1 expressions [79]. Additionally, a comprehensive examination of the postmortem analysis of a patient with COVID-19 revealed the presence of viral particles within both neural and capillary endothelial tissues of the frontal cortex. This indicates that the virus can enter the brain by infiltrating endothelial cells in the vascular system (Figure 2) [80]. Moreover, a laboratory study conducted using human blood vessel organelles revealed the invasion and replication of SARS-CoV-2. This finding supports the understanding of how infected brain endothelial cells facilitate the entry of blood-borne viruses into the brain [81]. The brain microvascular endothelial cells (BMVECs) represent a significant constituent of the BBB. The primary role of the BBB is to safeguard the brain by impeding the hematogenous infiltration of infections and toxic compounds into the CNS [82]. As a result, the virus must get past the BBB and subsequently infect the brain via the hematogenous pathway.
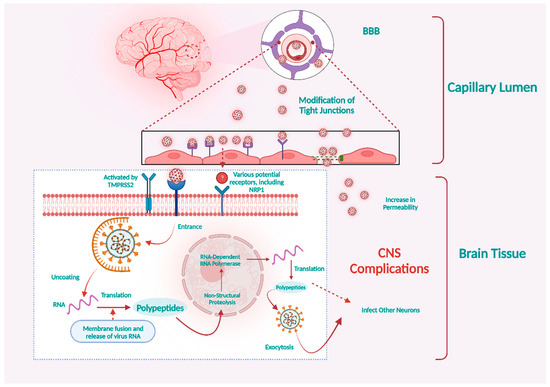
Figure 2.
SARS-CoV-2 may infect vascular endothelial cells via the ACE2 or NRP1 receptors. Viral particles in the bloodstream can contaminate and replicate inside brain microvascular endothelial cells, allowing them to cross the BBB. Infection of neurons by SARS-CoV-2 and increased permeability of the BBB may account for COVID-19’s severe neurological manifestations. Created with BioRender.com (https://app.biorender.com/illustrations/64cb6825bac8184af357a74a, accessed on 28 August 2023).
The choroid plexus demonstrated more excellent permeability in the blood–cerebrospinal fluid barrier than the BBB. Additionally, it was observed that the choroid plexus expressed ACE2 and TMPRSS2 [72], suggesting that it could serve as an alternative pathway for the invasion of the CNS by the virus.
Based on a study performed on a human choroid plexus model, it was observed that SARS-CoV-2 not only exhibited infectivity towards choroid plexus cells but also resulted in the disruption of the blood–cerebrospinal fluid barrier. This disruption presents an additional pathway for the virus to gain access to the brain [83].
3.2.2. Immune Cells Initiate Cytokine Secretion in Response to SARS-CoV-2
The presence of a viral infection can lead to immune responses that have the potential to induce damage to the nervous system. It is noteworthy to mention that SARS-CoV-2 possesses the capability to infect immune cells, potentially leading to subsequent invasion of the CNS. The activation of different immune cells, such as neutrophils, macrophages/monocytes, T cells, and natural killer cells, has been observed in response to SARS-CoV-2. The immune cells that have been activated can eliminate the virus by releasing cytokines such as interferon (IFN), interleukin (IL), tumor necrosis factor (TNF), and chemokines [84,85,86,87,88]. Under typical biological conditions, it is observed that pro-inflammatory factors and immune cells can establish a positive feedback cycle, thereby contributing to the maintenance of cytokine balance [84,89]. However, it is essential to note that infection with SARS-CoV-2 has been observed to elicit an exaggerated immune response in specific individuals. This immune response can initiate a systemic inflammatory response characterized by cytokine storms (Figure 3). Consequently, the primary consequence of this inflammatory cascade is the infliction of damage to blood vessels [90,91]. Cytokine storms have distinct effects on BBB permeability, which may allow the virus or infected immune cells to reach the brain and induce associated CNS symptoms [92,93].
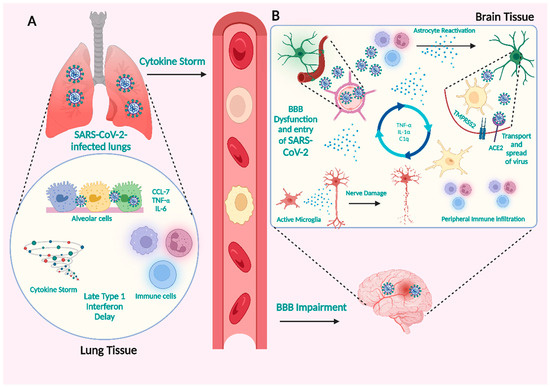
Figure 3.
SARS-CoV-2 infection can result in increased peripheral immunological responses, which can lead to BBB disruption. (A) Cytokine storms with high BBB permeability may allow viruses or infected immune cells to enter the brain. (B) Potential CNS pathogenic processes generated by COVID-19-induced severe peripheral hyperinflammation. In COVID-19, infected immune cells penetrate the brain and produce cytokines that trigger glial cells, causing them to create pro-inflammatory cytokines, resulting in severe neurological symptoms. Created with BioRender.com (https://app.biorender.com/illustrations/64eb7c1e6661a54a2025c481, accessed on 28 August 2023).
Previous studies have demonstrated that macrophages and peripheral lymphocytes, once infected, play a crucial role in facilitating the spread of the infection through the BBB, meninges, and choroid plexus [90,94]. According to reports, SARS-CoV-2 has predominantly infected human monocytes, while MERS-CoV has been observed to infect both T cells and monocytes. In the meantime, it has been established that SARS-CoV-2 can infect dendritic cells. Nevertheless, it was observed that both monocytes and macrophages exhibited a small level of ACE2 expression. This suggests an unidentified mechanism that potentially mediates the communication between the host’s natural immune system and SARS-CoV-2. The precise method through which SARS-CoV-2 contaminates immune cells is still not fully understood.
3.3. Expression of Essential Viral Infection Factors in the Nervous System
It is widely acknowledged that SARS-CoV-2 enters cells by utilizing ACE2 [12,21] with the involvement of TMPRSS2 [62,70], primarily due to the significant expression of these proteins in the pulmonary region. Moreover, extensive research suggests that the expression of both ACE2 and TMPRSS2 is also observed in the brain but at lower tiers. According to early immunohistochemistry research conducted by Lazartigue and colleagues, it was shown that ACE2 is present in the nerve cells of rat brains rather than the cells called glia [95]. Additionally, it has been determined that ACE2 plays a crucial role in regulating blood pressure and developing disorders related to the autonomic nervous system.
The investigation of human ACE2 mutant mice and brain organoids demonstrated that SARS-CoV-2 could infiltrate neurons and subsequently induce necrosis [96,97,98]. Furthermore, it is worth noting that the spike protein of SARS-CoV-2 can potentially engage with ACE2 receptors present in the endothelial cells of capillaries. This interaction raises the possibility that the virus could cause harm to the blood–brain barrier and gain access to the central nervous system by targeting the vascular system [99]. In addition to ACE2 and TMPRSS2, SARS-CoV-2 can invade other receptors or proteins, as shown in Table 2. Currently, the distribution of ACE2 is primarily determined by the analysis of mRNA data. However, it is essential to note that mRNA analysis does not fully capture the fully functional ACE2 protein distribution. Consequently, it is vitally necessary to conduct several immunohistochemical characterization studies.
Table 2.
SARS-CoV-2 infection-related receptors or proteins in the CNS.
4. Vascular Endothelial Growth Factor Cause Inflammation
Vascular endothelial growth factor (VEGF) displays a widespread distribution within the CNS [115]. Its primary function is to regulate the processes of angiogenesis, proliferation of endothelial cells, and permeability of blood vessels [32]. Furthermore, the interaction between SARS-CoV-2 and ACE2 can activate the renin–angiotensin system, a pathway implicated in the inflammatory response (Figure 4). This activation subsequently facilitates the production of VEGF using the binding between angiotensin II (AngII) and angiotensin II type 1 receptor (AT1R). In reality, VEGF increases angiogenesis in brain disorders and damages the BBB by causing inflammatory reactions [116].
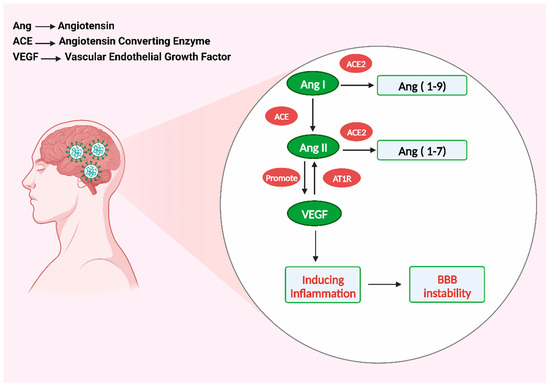
Figure 4.
VEGF-induced inflammation damages the blood–brain barrier. Created with BioRender.com (https://app.biorender.com/illustrations/64e6045bf2e116b8a7af2194, accessed on 28 August 2023).
Angiogenesis is generally accompanied by inflammation, which causes an increase in vascular permeability and the recruitment of inflammatory cells [116]. The ACE2 enzyme plays a crucial role in the catalytic process of converting Ang I and Ang II, Ang I to Ang 1-9 and Ang II to Ang 1-7, respectively [117,118]. When the SARS-CoV-2 virus interacts with ACE2, it can deactivate this enzyme, which may cause an increase in the activation of the ACE/AngII/AT1R axis, subsequently leading to the excessive synthesis of AngII. The positive feedback of Ang II stimulated the growth of ACE2 in the brain infected with SARS-CoV-2. VEGF, in turn, boosts Ang II, resulting in a cycle that releases pro-inflammatory cytokines such as TNF-, IL-1, IL-6, IL-8, and ICAM-1 [119]. Furthermore, interleukin-6 (IL-6) is an important inflammatory cytokine mediator linked to the severity of COVID-19 symptoms. It can be used as an indicator of COVID-19 severity [87,120].
5. Neurologic Symptoms of SARS-CoV-2 Infection
According to available data, the capability of SARS-CoV-2 to infect the neurological system is becoming more apparent. Case reports and retrospective cohort studies have been the primary sources of information regarding neurological symptoms of SARS-CoV-2 infection. China has conducted the first retrospective investigation on neurological symptoms [28,121,122]. Among the study group of 214 individuals diagnosed with COVID-19, it was observed that 78 patients, or 36.4% of the study, displayed neurological symptoms. The study revealed that individuals had acute cerebrovascular disease, impaired consciousness, skeletal muscle injury, and neurological symptoms, including dizziness, headache, nausea, blurred vision, tinnitus, fatigue, decreased taste sensation, and reduced sense of smell [123] (Figure 5). One of the symptoms of COVID-19 is headache, with a frequency of 6–13% [109,124,125,126,127]. It frequently occurs with other symptoms like fever and cough; thus, it is not an isolated symptom. Hyposmia and hypogeusia were noted as symptoms observed in individuals diagnosed with COVID-19, with reported prevalence rates varying from approximately 5% [28,128] to as high as 70% [129] or even exceeding 79% [130,131]. The data presented in this study indicate that specific findings may possess prognostic relevance in predicting the possibility of serious neurological problems. However, further research needs to be done in prospective studies to assess the diagnostic significance of neurological symptoms. This would greatly facilitate the early identification of patients at risk for neurological complications.
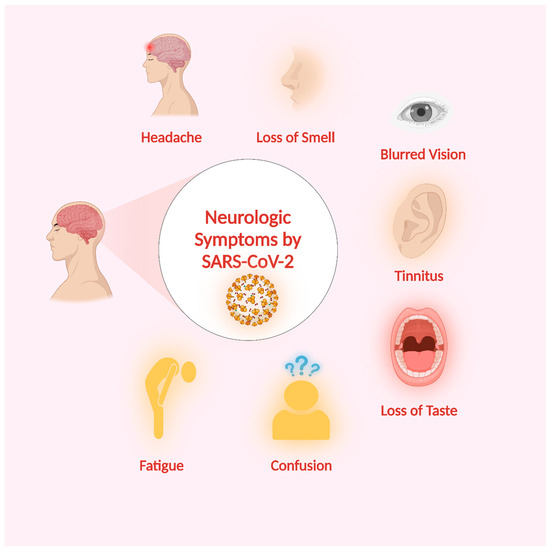
Figure 5.
SARS-CoV-2-related neurological symptoms. Created with BioRender.com (https://app.biorender.com/illustrations/649345fe5442443eead4ecc9, accessed on 28 August 2023).
6. SARS-CoV-2-Related Disorders of the Nervous System
The possible neurological diseases induced by SARS-CoV-2 fall into three broad categories: (a) the neurological adverse effects of associated pulmonary and systemic disorders, such as cerebrovascular disease; (b) the virus directly infiltrates the CNS, resulting in encephalitis; and (c) possible immune-mediated conditions following an infection, like Guillain–Barre syndrome (GBS) and other demyelinating diseases (Figure 6).
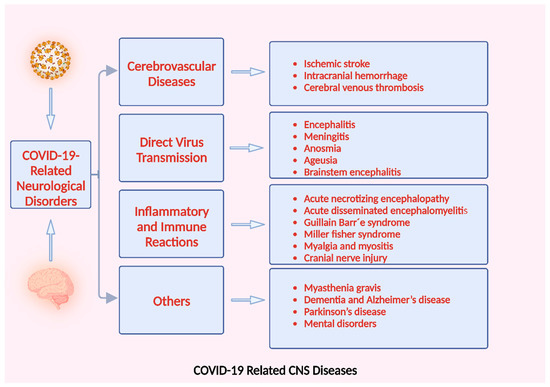
Figure 6.
CNS diseases associated with COVID-19. Created with BioRender.com (https://app.biorender.com/illustrations/6494a0a2b6f253735e3e3b2a, accessed on 28 August 2023).
6.1. Cerebrovascular Disease
Cerebrovascular disease is a group of diseases that affect the vessels that carry blood to the brain and induce brain tissue injury due to disruptions in cerebral blood circulation [132]. The virus replication within the pulmonary tissue induces extensive alveolar and interstitial inflammatory fluids and the production of hyaline membranes. This will result in abnormal alveolar exchanges of gases, hypoxia of the CNS, an increase in the anaerobic breakdown of brain tissue, the onset of edema between cells, blockage of cerebral circulation, resulting in ischemia of cerebral circulation, and gradual deterioration of brain function as the pressure in the brain rises [120,133,134,135]. It can also cause acute cerebrovascular disorders like cerebral venous thrombosis, hemorrhage, and ischemic stroke (Figure 7).
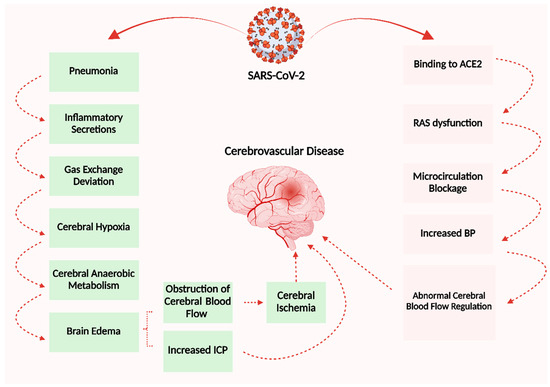
Figure 7.
This schematic diagram illustrates the pathophysiological mechanisms underlying cerebrovascular disease resulting from SARS-CoV-2. Created with BioRender.com (https://app.biorender.com/illustrations/64e779e77fc48876a30e4ac2, accessed on 25 August 2023).
Ischemic stroke is associated with many different viruses [136]. Stroke risk is increased even though the infection is often localized to the periphery and there is no evidence of the virus in the CNS. In these situations, systemic immunological activation is assumed to be the primary pathogenic mechanism. Combined with the accompanying hypercoagulability or endothelial dysfunction, this may result in vascular damage or the development of thromboemboli [137,138]. In such cases, the pathogenic mechanism of stroke may be easier to explain; however, CNS invasion does not rule out a role for systemic immune activation in stroke pathogenesis (Figure 8).
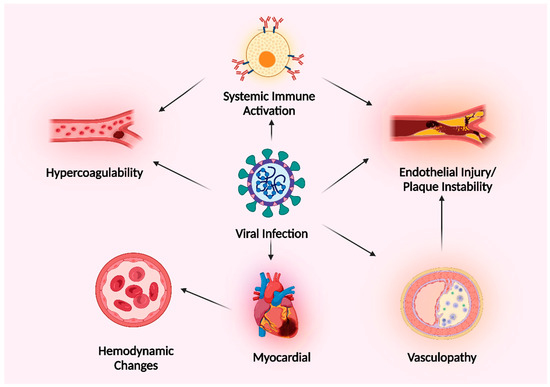
Figure 8.
A diagram demonstrating the different methods through which viral infections might cause ischemic stroke. Created with BioRender.com (https://app.biorender.com/illustrations/64cd3a53449ef0d0fd42f67d, accessed on 28 August 2023).
Acute ischemic stroke (AIS) is an emergent vascular complication in COVID-19 patients, with reported incidence rates ranging from 1% to 6% among hospitalized patients [139]. COVID-19 patients are more likely to have a stroke and have more severe symptoms and outcomes [140]. The classification of COVID-19 with ischemic stroke is based on two distinct classes determined by the underlying mechanism of occurrence.
The first category comprises senior individuals with a medical background with numerous coronary and cerebrovascular complications or who exhibit significant comorbidities before contracting the virus. These individuals are more susceptible to pulmonary embolism incidents [141]. The second category primarily comprises relatively young individuals without coronary and cerebrovascular factors or associated medical conditions before contracting the SARS-CoV-2 virus. This might be connected to how SARS-CoV-2 affects various bodily systems [142,143,144]. The coagulation process is essential in this phenomenon since around 25% of cases show evidence of systemic coagulation [145].
The initial inquiry explored the neurological signs observed in patients diagnosed with COVID-19 in Wuhan, China, which was the pandemic’s epicenter. The study revealed that out of the 214 patients included in the analysis, 78 individuals (36.4%) experienced neurological problems [28]. Patients with severe COVID-19 exhibited a higher prevalence of acute cerebrovascular disease than individuals with non-severe manifestations. It is important to note that individuals with severe illness showed higher D-dimer levels than non-severe infection [28].
The incidence of hemorrhagic stroke in individuals with COVID-19 is lower when compared to ischemic stroke. However, the causal link between COVID-19 infection and hemorrhagic stroke has not been demonstrated. Researchers performed a retrospective analysis of 11 individuals with acute cerebrovascular disease who had contracted COVID-19 in Wuhan. Among the patients, a 60-year-old man was identified as having a brain hemorrhage 10 days after a severe COVID-19 infection. The patient died 13 days after the stroke because of a high BP level (150/80 mmHg) [146].
According to Sharifi-Razavi et al., a 79-year-old man with a fever, cough, and acute loss of consciousness 3 days later was recorded. Without a history of elevated blood pressure or taking anticoagulant medication, the patient was admitted with a BP of 140/65 mmHg. In addition to intraventricular and subarachnoid hemorrhages, a CT scan revealed a severe intracerebral hemorrhage (ICH) in the right ventricle. However, CSF analysis was not performed despite the oropharyngeal swab revealing COVID-19 infection [147].
Cerebral venous thrombosis (CVT) is less common than cerebral infarction and hemorrhage [148,149], with a total frequency of 0.3% [150]. COVID-19 causes a hypercoagulable condition and systemic thrombosis, which includes CVT. Under the influence of COVID-19, patients without congenital CVT risk factors can develop excessive coagulation and thrombosis, leading to CVT [151,152]. These results collectively suggest that COVID-19 can cause cerebrovascular episodes, even though further thorough research is urgently needed. It is crucial to understand this information to avoid and treat the symptoms of cerebrovascular illness in COVID-19 individuals.
6.2. CNS Diseases by Direct Virus Transmission
Encephalitis is defined as inflammation of the brain parenchyma resulting from infections, which include neuronal destruction and nerve cell injury. The observation of viral encephalitis in many individuals who have contracted SARS-CoV-2 has led to speculation over the potential existence of this neurological consequence [153,154,155,156,157]. The presence of SARS-CoV-2 within the CSF of patients infected with COVID-19 was confirmed by the medical team working at Beijing Ditan Hospital using genome sequencing. This confirmation provided clinical evidence of viral encephalitis [120]. This makes it very likely that SARS-CoV-2 will cause encephalitis. However, images of brain tissue from SARS-CoV-2 cases showed no signs of inflammation [158].
Several autopsy findings indicate the presence of lymphocytic panencephalitis, meningitis [159], partial neuronal atrophy, and brain edema [160]. Around cerebral blood arteries, sparse or significant clumps of inflamed cells, mainly monocytes, have been seen. Soft focal meningitis is also found [161].
The prevalence of anosmia and ageusia is significantly elevated among people diagnosed with COVID-19. The prevalence of anosmia is more than 85.6%, whereas that of ageusia is reported to be 88.0% [130]. Some research studies believe this phenomenon can be attributed to the degeneration of olfactory sensory neurons resulting from many factors, such as dysfunction of supporting cells, apoptosis triggered by inflammation, or potentially direct infection [162]. However, the mechanism remains unclear. Symptoms in individuals with mild COVID-19 lasted approximately 10 days, with 89% of patients recovering within four weeks after diagnosis [163].
Brainstem encephalitis (BE) is a rare, severe, and quickly spreading inflammatory condition affecting the brainstem. Multiple experiments and animal models have indicated the potential transmission of SARS-CoV-2 to the brainstem nucleus via various pathways, including the olfactory nerve, trigeminal nerve, facial nerve, glossopharyngeal nerve, vagus nerve, dorsal root ganglia, etc. However, the evidence remains insufficient to support this hypothesis conclusively [141]. Brain autopsy findings revealed the presence of neuronal cell death and axonal degeneration exclusively inside the cerebral cortex. Further research is required to prove the association between COVID-19 and encephalitis, as the current understanding is based on theoretical pathways proposed in clinical observations and neuronal colonization.
6.3. Nervous System Damage Induced by Abnormal Immune and Inflammatory Reactions
The etiology of numerous neurological disorders can be linked to increased inflammation and immunological dysregulation resulting from infection. COVID-19 is not an exception. Acute necrotizing encephalopathy (ANE) is an uncommon disease that typically develops after a critical febrile illness, most commonly a viral infection, and is characterized by brain damage (encephalopathy) [164]. The predominant imaging characteristics widely observed include the presence of symmetrical multifocal lesions and the engagement of the thalamus [29]. Autopsy findings indicate the presence of significant vasculitis, characterized by varying levels of segmental and complete destruction of the endothelial cells. Thrombosis primarily affects the vascular bed’s microcirculation. Additionally, there is significant evidence of hemorrhagic necrosis, inflammation, and severe necrotizing damage to the neurons. Localized cerebral edema may also be present [165].
Guillain–Barré syndrome (GBS) is an uncommon autoimmune condition characterized by acquired nerve damage caused by the immune system, resulting in muscle weakness and, in some cases, paralysis. In COVID-19 patients, most GBS variants have been identified [166]. According to specific research, 60% of GBS patients achieve partial to full recovery [167]. In addition to its connection to ACE2, SARS-CoV-2 has been observed to require sialic-acid-containing glycoproteins and gangliosides for cellular entry [168]. The pathophysiology of GBS is tightly associated with these two sites as well. Hence, it is possible that cross-reactivity could manifest as a viable method by which SARS-CoV-2 may induce GBS [168].
Myalgia is a frequently encountered symptom seen in individuals diagnosed with COVID-19. The condition’s prevalence varies from 3.36% to 64%, with an estimated total prevalence of 19.3% [150,169]. In rare instances, myalgia and muscle injury have the potential to advance into the condition known as rhabdomyolysis [170]. The expression of ACE on skeletal muscle may be the primary cause of myalgia [171]. Further diagnostic investigations, including muscle biopsy and antibody screening, are required for individuals diagnosed with COVID-19 who exhibit indications of skeletal muscle damage.
6.4. Other COVID-19-Related Neurological Disorders
Myasthenia gravis (MG) is a persistent autoimmune condition characterized by the destruction of nerve–muscle communication by antibodies, leading to skeletal muscle weakening. Two new MG cases were identified in a survey of approximately 11,000 COVID-19 patients [172]. The mechanism may be connected to immunological dysfunction and infection-induced inflammation [173]. In addition, the research findings of another study revealed that out of 3558 patients diagnosed with Myasthenia Gravis (MG), 34 patients contracted the COVID-19 virus at a low rate (0.96%) [174]. Most MG patients become more seriously ill after contracting COVID-19. A total of 73% required mechanical ventilation, 87% required ICU care, and 30% passed away [175].
Multiple Sclerosis (MS) instances among individuals diagnosed with COVID-19 are rare. In a recent study, only two cases were documented out of a sample size of approximately 11,000 individuals [172]. In the context of multiple sclerosis (MS), it is essential to examine the potential impact of disease-modifying therapy (DMT) on the vulnerability of MS patients to contracting COVID-19. Nevertheless, it is necessary to note that the available data on (MS) are limited in scope, and further research is needed.
According to recent studies, the prevalence of dementia among individuals diagnosed with COVID-19 is reported to be 0.67% [176]. The average rate of newly diagnosed dementia within 14–90 days after COVID-19 among individuals aged 65 and above is reported to be 1.6% [177]. There is a significant correlation between dementia and the COVID-19 pandemic. Specific signs and symptoms associated with Alzheimer’s disease and related dementia (ADRD) can heighten susceptibility to COVID-19 infection. These symptoms encompass an impaired capacity to understand and comply with COVID-19 prevention instructions and standards and alterations in personality and memory [178,179].
7. Conclusions and Future Perspectives
COVID-19 presents a significant challenge to the global community. The investigation of the neurological implications of SARS-CoV-2 infections is a rapidly growing field among neuroscientists. Even though SARS-CoV-2 is primarily responsible for respiratory problems, mounting evidence points to the possibility of a neuroinvasion by this virus. SARS-CoV-2 isolation from CSF, the discovery of the virus on olfactory receptors, and numerous neurologic manifestations in COVID-19 patients have all provided evidence. CNS and PNS problems have reportedly been noticed in these patients. However, it is difficult to determine if CNS symptoms were caused by CNS infection or peripheral infection because of blood clotting, hypoxia, and cytokine storms in severe patients. Furthermore, the method by which SARS-CoV-2 invades the nervous system still needs to be better understood.
Currently, the potential pathways of SARS-CoV-2 neuroinvasion are:
- ✔
- Entry via the olfactory nerve;
- ✔
- Direct infection of vascular endothelial cells;
- ✔
- The initiation of inflammatory reactions that breach the BBB facilitates invasion.
All of the above routes are linked to ACE2 or NRP1; hence, the best optimal strategy for investigating the mechanism by which SARS-CoV-2 infiltrates the CNS would involve determining the respective distributions of NRP1 and ACE2. Understanding this wealth of knowledge is essential for preventing and controlling CNS symptoms and facilitating the rehabilitation process for those affected by COVID-19.
It is evident that the knowledge we have acquired thus far only scratches the surface, and there is still a significant amount of information to be comprehended in this field to facilitate effective therapeutic intervention.
Author Contributions
W.A. conceived, designed, and wrote the manuscript. J.F. and Y.Z. provided critical revision and helped in the analysis of the manuscript. L.C. supervised and contributed to the discussion of ideas and perspectives, helped in the correction, and proofread the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partially sponsored by the National Key R&D Program of China (2022YFA1104900 and 2022YFA1104904), the Innovation Team Project (2023KCXTD007) and the Special Project in Key Areas (2021ZDZX2011) of the Department of Education of Guangdong Province, the Natural Science Foundation of Guangdong Province (2021A1515010013), the Guangzhou Municipal Science and Technology Project (202201011760), and the President Foundation of the Integrated Hospital of Traditional Chinese Medicine of Southern Medical University (1202101003).
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank Talha Ahmed, Chengyang Gu, Haroon Khan, Adeel Khan, and Mohammad Hasan Molooy Zada for reviewing and proofreading the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bohmwald, K.; Gálvez, N.M.; Ríos, M.; Kalergis, A.M. Neurologic alterations due to respiratory virus infections. Front. Cell. Neurosci. 2018, 12, 386. [Google Scholar] [CrossRef] [PubMed]
- Desforges, M.; Le Coupanec, A.; Dubeau, P.; Bourgouin, A.; Lajoie, L.; Dubé, M.; Talbot, P.J. Human coronaviruses and other respiratory viruses: Underestimated opportunistic pathogens of the central nervous system? Viruses 2019, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Goldmann, D.A. Transmission of viral respiratory infections in the home. Pediatr. Infect. Dis. J. 2000, 19, S97–S102. [Google Scholar] [CrossRef] [PubMed]
- Nichols, W.G.; Peck Campbell, A.J.; Boeckh, M. Respiratory viruses other than influenza virus: Impact and therapeutic advances. Clin. Microbiol. Rev. 2008, 21, 274–290. [Google Scholar] [CrossRef]
- Talbot, H.K.; Falsey, A.R. The diagnosis of viral respiratory disease in older adults. Clin. Infect. Dis. 2010, 50, 747–751. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Schwarze, J.R. Respiratory viral infections in infants: Causes, clinical symptoms, virology, and immunology. Clin. Microbiol. Rev. 2010, 23, 74–98. [Google Scholar] [CrossRef]
- Berry, M.; Gamieldien, J.; Fielding, B.C. Identification of new respiratory viruses in the new millennium. Viruses 2015, 7, 996–1019. [Google Scholar] [CrossRef]
- Koralnik, I.J.; Tyler, K.L. COVID-19: A global threat to the nervous system. Ann. Neurol. 2020, 88, 1–11. [Google Scholar] [CrossRef]
- Masters, P.S. The molecular biology of coronaviruses. Adv. Virus Res. 2006, 66, 193–292. [Google Scholar]
- Nakagawa, S.; Miyazawa, T. Genome evolution of SARS-CoV-2 and its virological characteristics. Inflamm. Regen. 2020, 40, 17. [Google Scholar] [CrossRef]
- Lin, Y.; Shen, X.; Yang, R.F.; Li, Y.X.; Ji, Y.Y.; He, Y.Y.; Shi, M.D.; Lu, W.; Shi, T.L.; Wang, J. Identification of an epitope of SARS-coronavirus nucleocapsid protein. Cell Res. 2003, 13, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e278. [Google Scholar] [CrossRef] [PubMed]
- Sanclemente-Alaman, I.; Moreno-Jiménez, L.; Benito-Martín, M.S.; Canales-Aguirre, A.; Matías-Guiu, J.A.; Matías-Guiu, J.; Gómez-Pinedo, U. Experimental models for the study of central nervous system infection by SARS-CoV-2. Front. Immunol. 2020, 11, 2163. [Google Scholar] [CrossRef]
- Algahtani, H.; Subahi, A.; Shirah, B. Neurological complications of Middle East respiratory syndrome coronavirus: A report of two cases and review of the literature. Case Rep. Neurol. Med. 2016, 2016, 3502683. [Google Scholar] [CrossRef] [PubMed]
- Koyuncu, O.O.; Hogue, I.B.; Enquist, L.W. Virus infections in the nervous system. Cell Host Microbe 2013, 13, 379–393. [Google Scholar] [CrossRef]
- Li, Y.; Li, H.; Fan, R.; Wen, B.; Zhang, J.; Cao, X.; Wang, C.; Song, Z.; Li, S.; Li, X. Coronavirus infections in the central nervous system and respiratory tract show distinct features in hospitalized children. Intervirology 2017, 59, 163–169. [Google Scholar] [CrossRef]
- Meijer, W.J.; Linn, F.H.; Wensing, A.M.; Leavis, H.L.; van Riel, D.; GeurtsvanKessel, C.H.; Wattjes, M.P.; Murk, J.-L. Acute influenza virus-associated encephalitis and encephalopathy in adults: A challenging diagnosis. JMM Case Rep. 2016, 3. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L. COVID-19 in critically ill patients in the Seattle region—Case series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Acharya, A.; Kevadiya, B.D.; Gendelman, H.E.; Byrareddy, S.N. SARS-CoV-2 infection leads to neurological dysfunction. J. Neuroimmune Pharmacol. 2020, 15, 167–173. [Google Scholar] [CrossRef]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P.J.; Taquet, M. Neuropsychiatric disorders following SARS-CoV-2 infection. Brain 2023, 146, 2241–2247. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, M.; Lanza, G.; Falzone, L.; Fisicaro, F.; Ferri, R.; Bella, R. SARS-CoV-2 and the nervous system: From clinical features to molecular mechanisms. Int. J. Mol. Sci. 2020, 21, 5475. [Google Scholar] [CrossRef] [PubMed]
- Alshebri, M.S.; Alshouimi, R.A.; Alhumidi, H.A.; Alshaya, A.I. Neurological complications of SARS-CoV, MERS-CoV, and COVID-19. SN Compr. Clin. Med. 2020, 2, 2037–2047. [Google Scholar] [CrossRef] [PubMed]
- Kwong, K.C.N.K.; Mehta, P.R.; Shukla, G.; Mehta, A.R. COVID-19, SARS and MERS: A neurological perspective. J. Clin. Neurosci. 2020, 77, 13–16. [Google Scholar] [CrossRef]
- Verstrepen, K.; Baisier, L.; De Cauwer, H. Neurological manifestations of COVID-19, SARS and MERS. Acta Neurol. Belg. 2020, 120, 1051–1060. [Google Scholar] [CrossRef]
- Moriguchi, T.; Harii, N.; Goto, J.; Harada, D.; Sugawara, H.; Takamino, J.; Ueno, M.; Sakata, H.; Kondo, K.; Myose, N. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 2020, 94, 55–58. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef]
- Poyiadji, N.; Shahin, G.; Noujaim, D.; Stone, M.; Patel, S.; Griffith, B. COVID-19-associated acute hemorrhagic necrotizing encephalopathy: Imaging features. Radiology 2020, 296, E119–E120. [Google Scholar] [CrossRef]
- Llansó, L.; Urra, X. Posterior reversible encephalopathy syndrome in COVID-19 disease: A case-report. SN Compr. Clin. Med. 2020, 2, 1900–1902. [Google Scholar] [CrossRef]
- Klok, F.; Kruip, M.; Van der Meer, N.; Arbous, M.; Gommers, D.; Kant, K.; Kaptein, F.; van Paassen, J.; Stals, M.; Huisman, M. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Waqas, A.; Zhu, Z.; Chen, L. Exosomes: Applications in respiratory infectious diseases and prospects for coronavirus disease 2019 (COVID-19). J. Biomed. Nanotechnol. 2020, 16, 399–418. [Google Scholar] [CrossRef]
- Tyagi, K.; Rai, P.; Gautam, A.; Kaur, H.; Kapoor, S.; Suttee, A.; Jaiswal, P.K.; Sharma, A.; Singh, G.; Barnwal, R.P. Neurological manifestations of SARS-CoV-2: Complexity, mechanism and associated disorders. Eur. J. Med. Res. 2023, 28, 307. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.J. Neurologic complications of influenza. In Seminars in Pediatric Neurology; WB Saunders: Philadelphia, PA, USA, 2012; pp. 96–100. [Google Scholar]
- Khandaker, G.; Zurynski, Y.; Buttery, J.; Marshall, H.; Richmond, P.C.; Dale, R.C.; Royle, J.; Gold, M.; Snelling, T.; Whitehead, B. Neurologic complications of influenza A (H1N1) pdm09: Surveillance in 6 pediatric hospitals. Neurology 2012, 79, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Mylonaki, E.; Harrer, A.; Pilz, G.; Stalzer, P.; Otto, F.; Trinka, E.; Wipfler, P. Neurological complications associated with influenza in season 2017/18 in Austria-a retrospective single center study. J. Clin. Virol. 2020, 127, 104340. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.P.; Busl, K.M. Neurologic manifestations of severe respiratory viral contagions. Crit. Care Explor. 2020, 2, e0107. [Google Scholar] [CrossRef]
- Sellers, S.A.; Hagan, R.S.; Hayden, F.G.; Fischer, W.A. The hidden burden of influenza: A review of the extra-pulmonary complications of influenza infection. Influenza Other Respir. Viruses 2017, 11, 372–393. [Google Scholar] [CrossRef]
- Uyeki, T.M.; Bernstein, H.H.; Bradley, J.S.; Englund, J.A.; File, T.M., Jr.; Fry, A.M.; Gravenstein, S.; Hayden, F.G.; Harper, S.A.; Hirshon, J.M. Clinical practice guidelines by the Infectious Diseases Society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenza. Clin. Infect. Dis. 2019, 68, e1–e47. [Google Scholar] [CrossRef]
- Kho, N.; Kerrigan, J.F.; Tong, T.; Browne, R.; Knilans, J. Respiratory syncytial virus infection and neurologic abnormalities: Retrospective cohort study. J. Child Neurol. 2004, 19, 859–864. [Google Scholar] [CrossRef]
- Vehapoglu, A.; Turel, O.; Uygur Sahin, T.; Kutlu, N.O.; Iscan, A. Clinical significance of human metapneumovirus in refractory status epilepticus and encephalitis: Case report and review of the literature. Case Rep. Neurol. Med. 2015, 2015, 131780. [Google Scholar] [CrossRef]
- Mergeay, M.; Coeckelbergh, E.; De Cauwer, H.; Viaene, M.; Van der Mieren, G. An adult case of metapneumovirus-induced acute encephalitis. Acta Neurol. Belg. 2019, 119, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Jeannet, N.; van den Hoogen, B.G.; Schefold, J.C.; Suter-Riniker, F.; Sommerstein, R. Cerebrospinal Fluid Findings in an Adult with Human Metapneumovirus-Associated Encephalitis. Emerg. Infect. Dis. 2017, 23, 370. [Google Scholar] [CrossRef]
- Huang, H.; Chen, L.; Sanberg, P.R.; Dimitrijevic, M.; Shetty, A.K.; Sharma, H.S.; Wu, P.; Bryukhovetskiy, A.; Al-Zoubi, Z.M.; Chopp, M.; et al. Beijing Declaration of International Association of Neurorestoratology (2023 Xi’an version). J. Neurorestoratol. 2023, 11, 100055. [Google Scholar] [CrossRef]
- Huang, H.; Bach, J.R.; Sharma, H.S.; Saberi, H.; Jeon, S.R.; Guo, X.; Shetty, A.; Hawamdeh, Z.; Sharma, A.; Wild, K.v.; et al. The 2022 yearbook of Neurorestoratology. J. Neurorestoratol. 2023, 11, 100054. [Google Scholar] [CrossRef]
- Sharma, H.S.; Chopp, M.; Chen, L.; Sarnowska, A.; Xue, M.; Ao, Q.; Siniscalco, D.; Chen, L.; Hawamdeh, Z.; Huang, H. The 2021 yearbook of Neurorestoratology. J. Neurorestoratol. 2022, 10, 100008. [Google Scholar] [CrossRef]
- Huang, H.; Chen, L.; Chopp, M.; Young, W.; Robert Bach, J.; He, X.; Sarnowaska, A.; Xue, M.; Chunhua Zhao, R.; Shetty, A.; et al. The 2020 Yearbook of Neurorestoratology. J. Neurorestoratol. 2021, 9, 1–12. [Google Scholar] [CrossRef]
- Zhang, Q.; Jiu, Y. The regulation of host cytoskeleton during SARS-CoV-2 infection in the nervous system. Brain Sci. Adv. 2023, 9, 43–52. [Google Scholar] [CrossRef]
- Louveau, A.; Harris, T.H.; Kipnis, J. Revisiting the mechanisms of CNS immune privilege. Trends Immunol. 2015, 36, 569–577. [Google Scholar] [CrossRef]
- Takao, M.; Ohira, M. Neurological post-acute sequelae of SARS-CoV-2 infection. Psychiatry Clin. Neurosci. 2023, 77, 72–83. [Google Scholar] [CrossRef]
- Kaplan, L.; Chow, B.W.; Gu, C. Neuronal regulation of the blood–brain barrier and neurovascular coupling. Nat. Rev. Neurosci. 2020, 21, 416–432. [Google Scholar] [CrossRef]
- McGavern, D.B.; Kang, S.S. Illuminating viral infections in the nervous system. Nat. Rev. Immunol. 2011, 11, 318–329. [Google Scholar] [CrossRef] [PubMed]
- Swanson, P.A.; McGavern, D.B. Viral diseases of the central nervous system. Curr. Opin. Virol. 2015, 11, 44–54. [Google Scholar] [CrossRef]
- Tyrrell, D.; Bynoe, M. Cultivation of a novel type of common-cold virus in organ cultures. Br. Med. J. 1965, 1, 1467. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, S.; Swain, B.; Verma, R.; Gunthe, S.S. SARS-CoV, MERS-CoV, and 2019-nCoV viruses: An overview of origin, evolution, and genetic variations. VirusDisease 2020, 31, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; Zheng, B.; He, Y.; Liu, X.; Zhuang, Z.; Cheung, C.; Luo, S.; Li, P.H.; Zhang, L.; Guan, Y. Isolation and characterization of viruses related to the SARS coronavirus from animals in southern China. Science 2003, 302, 276–278. [Google Scholar] [PubMed]
- Gu, J.; Gong, E.; Zhang, B.; Zheng, J.; Gao, Z.; Zhong, Y.; Zou, W.; Zhan, J.; Wang, S.; Xie, Z. Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 2005, 202, 415–424. [Google Scholar] [CrossRef]
- Nassar, M.; Bakhrebah, M.; Meo, S.A.; Alsuabeyl, M.; Zaher, W. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection: Epidemiology, pathogenesis and clinical characteristics. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4956–4961. [Google Scholar]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef]
- Huang, H. Why is olfactory neuroepithelium? J. Neurorestoratol. 2021, 9, 211–218. [Google Scholar] [CrossRef]
- DosSantos, M.F.; Devalle, S.; Aran, V.; Capra, D.; Roque, N.R.; Coelho-Aguiar, J.d.M.; Spohr, T.C.L.d.S.e.; Subilhaga, J.G.; Pereira, C.M.; D’Andrea Meira, I. Neuromechanisms of SARS-CoV-2: A review. Front. Neuroanat. 2020, 14, 37. [Google Scholar] [CrossRef]
- Butowt, R.; Bilinska, K. SARS-CoV-2: Olfaction, brain infection, and the urgent need for clinical samples allowing earlier virus detection. ACS Chem. Neurosci. 2020, 11, 1200–1203. [Google Scholar] [CrossRef] [PubMed]
- García-García, S.; Cepeda, S.; Arrese, I.; Sarabia, R. Hemorrhagic conditions affecting the central nervous system in COVID-19 patients. Neurosurgery 2020, 87, E394–E396. [Google Scholar] [CrossRef] [PubMed]
- Saleki, K.; Banazadeh, M.; Saghazadeh, A.; Rezaei, N. The involvement of the central nervous system in patients with COVID-19. Rev. Neurosci. 2020, 31, 453–456. [Google Scholar] [CrossRef]
- Siddiqui, R.; Khan, N.A. Proposed intranasal route for drug administration in the management of central nervous system manifestations of COVID-19. ACS Chem. Neurosci. 2020, 11, 1523–1524. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.-Y.; Jin, W.-L. The COVID-19 pandemic: Consideration for brain infection. Neuroscience 2020, 437, 130. [Google Scholar] [CrossRef]
- Liang, F. Sustentacular cell enwrapment of olfactory receptor neuronal dendrites: An update. Genes 2020, 11, 493. [Google Scholar] [CrossRef] [PubMed]
- Thangaleela, S.; Sivamaruthi, B.S.; Kesika, P.; Bharathi, M.; Chaiyasut, C. Nasal Microbiota, Olfactory Health, Neurological Disorders and Aging—A Review. Microorganisms 2022, 10, 1405. [Google Scholar]
- Chen, M.; Shen, W.; Rowan, N.R.; Kulaga, H.; Hillel, A.; Ramanathan, M.; Lane, A.P. Elevated ACE-2 expression in the olfactory neuroepithelium: Implications for anosmia and upper respiratory SARS-CoV-2 entry and replication. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Bilinska, K.; Jakubowska, P.; Von Bartheld, C.S.; Butowt, R. Expression of the SARS-CoV-2 entry proteins, ACE2 and TMPRSS2, in cells of the olfactory epithelium: Identification of cell types and trends with age. ACS Chem. Neurosci. 2020, 11, 1555–1562. [Google Scholar] [CrossRef]
- Bryche, B.; St Albin, A.; Murri, S.; Lacôte, S.; Pulido, C.; Gouilh, M.A.; Lesellier, S.; Servat, A.; Wasniewski, M.; Picard-Meyer, E. Massive transient damage of the olfactory epithelium associated with infection of sustentacular cells by SARS-CoV-2 in golden Syrian hamsters. Brain Behav. Immun. 2020, 89, 579–586. [Google Scholar] [CrossRef]
- Deffner, F.; Scharr, M.; Klingenstein, S.; Klingenstein, M.; Milazzo, A.; Scherer, S.; Wagner, A.; Hirt, B.; Mack, A.F.; Neckel, P.H. Histological evidence for the enteric nervous system and the choroid plexus as alternative routes of neuroinvasion by SARS-CoV2. Front. Neuroanat. 2020, 14, 596439. [Google Scholar] [CrossRef] [PubMed]
- de Mattos Coelho-Aguiar, J.; Veríssimo, C.P.; da Silva Costa, D.V.; de Moraes Thomasi, B.B.; Frauches, A.C.B.; Ribeiro, F.P.; Gomes, A.L.T.; de Castro Brito, G.A.; Moura-Neto, V. The enteric glial network acts in the maintenance of intestinal homeostasis and in intestinal disorders. In Glia in Health and Disease; IntechOpen: London, UK, 2019; pp. 1–29. [Google Scholar]
- Chen, Y.; Chen, L.; Deng, Q.; Zhang, G.; Wu, K.; Ni, L.; Yang, Y.; Liu, B.; Wang, W.; Wei, C. The presence of SARS-CoV-2 RNA in the feces of COVID-19 patients. J. Med. Virol. 2020, 92, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Lamers, M.M.; Beumer, J.; van der Vaart, J.; Knoops, K.; Puschhof, J.; Breugem, T.I.; Ravelli, R.B.; Paul van Schayck, J.; Mykytyn, A.Z.; Duimel, H.Q. SARS-CoV-2 productively infects human gut enterocytes. Science 2020, 369, 50–54. [Google Scholar] [CrossRef]
- Esposito, G.; Pesce, M.; Seguella, L.; Sanseverino, W.; Lu, J.; Sarnelli, G. Can the enteric nervous system be an alternative entrance door in SARS-CoV2 neuroinvasion? Brain Behav. Immun. 2020, 87, 93. [Google Scholar] [CrossRef] [PubMed]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S. Multiorgan and renal tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 590–592. [Google Scholar] [CrossRef]
- Wang, Y.; Cao, Y.; Mangalam, A.K.; Guo, Y.; LaFrance-Corey, R.G.; Gamez, J.D.; Atanga, P.A.; Clarkson, B.D.; Zhang, Y.; Wang, E. Neuropilin-1 modulates interferon-γ-stimulated signaling in brain microvascular endothelial cells. J. Cell Sci. 2016, 129, 3911–3921. [Google Scholar] [CrossRef] [PubMed]
- Paniz-Mondolfi, A.; Bryce, C.; Grimes, Z.; Gordon, R.E.; Reidy, J.; Lednicky, J.; Sordillo, E.M.; Fowkes, M. Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J. Med. Virol. 2020, 92, 699–702. [Google Scholar] [CrossRef]
- Monteil, V.; Kwon, H.; Prado, P.; Hagelkrüys, A.; Wimmer, R.A.; Stahl, M.; Leopoldi, A.; Garreta, E.; Del Pozo, C.H.; Prosper, F. Inhibition of SARS-CoV-2 infections in engineered human tissues using clinical-grade soluble human ACE2. Cell 2020, 181, 905–913.e907. [Google Scholar] [CrossRef]
- Hawkins, B.T.; Davis, T.P. The blood-brain barrier/neurovascular unit in health and disease. Pharmacol. Rev. 2005, 57, 173–185. [Google Scholar] [CrossRef]
- Pellegrini, L.; Albecka, A.; Mallery, D.L.; Kellner, M.J.; Paul, D.; Carter, A.P.; James, L.C.; Lancaster, M.A. SARS-CoV-2 infects the brain choroid plexus and disrupts the blood-CSF barrier in human brain organoids. Cell Stem Cell 2020, 27, 951–961.e955. [Google Scholar] [CrossRef] [PubMed]
- Kempuraj, D.; Selvakumar, G.P.; Ahmed, M.E.; Raikwar, S.P.; Thangavel, R.; Khan, A.; Zaheer, S.A.; Iyer, S.S.; Burton, C.; James, D. COVID-19, mast cells, cytokine storm, psychological stress, and neuroinflammation. Neuroscientist 2020, 26, 402–414. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of theCytokine Storm’in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Wang, T.; Cai, D.; Hu, Z.; Liao, H.; Zhi, L.; Wei, H.; Zhang, Z.; Qiu, Y.; Wang, J. Cytokine storm intervention in the early stages of COVID-19 pneumonia. Cytokine Growth Factor Rev. 2020, 53, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Coperchini, F.; Chiovato, L.; Croce, L.; Magri, F.; Rotondi, M. The cytokine storm in COVID-19: An overview of the involvement of the chemokine/chemokine-receptor system. Cytokine Growth Factor Rev. 2020, 53, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.; Ge, Y.; Wu, B.; Zhang, W.; Wu, T.; Wen, T.; Liu, J.; Guo, X.; Huang, C.; Jiao, Y. Serum cytokine and chemokine profile in relation to the severity of coronavirus disease 2019 in China. J. Infect. Dis. 2020, 222, 746–754. [Google Scholar] [CrossRef]
- Sfera, A.; Rahman, L.; Zapata-Martín del Campo, C.M.; Kozlakidis, Z. Long COVID as a Tauopathy: Of “Brain Fog” and “Fusogen Storms”. Int. J. Mol. Sci. 2023, 24, 12648. [Google Scholar] [CrossRef]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the nervous system. Cell 2020, 183, 16–27.e1. [Google Scholar] [CrossRef]
- Li, Z.; Liu, T.; Yang, N.; Han, D.; Mi, X.; Li, Y.; Liu, K.; Vuylsteke, A.; Xiang, H.; Guo, X. Neurological manifestations of patients with COVID-19: Potential routes of SARS-CoV-2 neuroinvasion from the periphery to the brain. Front. Med. 2020, 14, 533–541. [Google Scholar] [CrossRef]
- Nile, S.H.; Nile, A.; Qiu, J.; Li, L.; Jia, X.; Kai, G. COVID-19: Pathogenesis, cytokine storm and therapeutic potential of interferons. Cytokine Growth Factor Rev. 2020, 53, 66–70. [Google Scholar] [CrossRef]
- Al-Obaidi, M.J.; Bahadoran, A.; Wang, S.; Manikam, R.; Raju, C.S.; Sekaran, S. Disruption of the blood brain barrier is vital property of neurotropic viral infection of the central nervous system. Acta Virol. 2018, 62, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Miner, J.J.; Diamond, M.S. Mechanisms of restriction of viral neuroinvasion at the blood–brain barrier. Curr. Opin. Immunol. 2016, 38, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Doobay, M.F.; Talman, L.S.; Obr, T.D.; Tian, X.; Davisson, R.L.; Lazartigues, E. Differential expression of neuronal ACE2 in transgenic mice with overexpression of the brain renin-angiotensin system. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R373–R381. [Google Scholar] [PubMed]
- Song, E.; Zhang, C.; Israelow, B.; Lu-Culligan, A.; Prado, A.V.; Skriabine, S.; Lu, P.; Weizman, O.-E.; Liu, F.; Dai, Y. Neuroinvasion of SARS-CoV-2 in human and mouse brain. J. Exp. Med. 2021, 218, e20202135. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Han, Y.; Nilsson-Payant, B.E.; Gupta, V.; Wang, P.; Duan, X.; Tang, X.; Zhu, J.; Zhao, Z.; Jaffré, F. A human pluripotent stem cell-based platform to study SARS-CoV-2 tropism and model virus infection in human cells and organoids. Cell Stem Cell 2020, 27, 125–136.e7. [Google Scholar] [PubMed]
- Brasso, C.; Bellino, S.; Blua, C.; Bozzatello, P.; Rocca, P. The Impact of SARS-CoV-2 Infection on Youth Mental Health: A Narrative Review. Biomedicines 2022, 10, 772. [Google Scholar] [CrossRef] [PubMed]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host–Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef]
- MacLean, M.; Kamintsky, L.; Leck, E.; Friedman, A. The potential role of microvascular pathology in the neurological manifestations of coronavirus infection. Fluids Barriers CNS 2020, 17, 55. [Google Scholar] [CrossRef]
- Desforges, M.; Le Coupanec, A.; Stodola, J.K.; Meessen-Pinard, M.; Talbot, P.J. Human coronaviruses: Viral and cellular factors involved in neuroinvasiveness and neuropathogenesis. Virus Res. 2014, 194, 145–158. [Google Scholar] [CrossRef]
- Tremblay, M.-E.; Madore, C.; Bordeleau, M.; Tian, L.; Verkhratsky, A. Neuropathobiology of COVID-19: The role for glia. Front. Cell. Neurosci. 2020, 14, 592214. [Google Scholar] [CrossRef]
- Vazana, U.; Veksler, R.; Pell, G.S.; Prager, O.; Fassler, M.; Chassidim, Y.; Roth, Y.; Shahar, H.; Zangen, A.; Raccah, R. Glutamate-mediated blood–brain barrier opening: Implications for neuroprotection and drug delivery. J. Neurosci. 2016, 36, 7727–7739. [Google Scholar] [CrossRef] [PubMed]
- Merkler, A.E.; Parikh, N.S.; Mir, S.; Gupta, A.; Kamel, H.; Lin, E.; Lantos, J.; Schenck, E.J.; Goyal, P.; Bruce, S.S. Risk of ischemic stroke in patients with coronavirus disease 2019 (COVID-19) vs patients with influenza. JAMA Neurol. 2020, 77, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, P.N.; Schaal, H. Human brain organoids to explore SARS-CoV-2-induced effects on the central nervous system. Rev. Med. Virol. 2023, 33, e2430. [Google Scholar] [CrossRef] [PubMed]
- Mollica, V.; Rizzo, A.; Massari, F. The pivotal role of TMPRSS2 in coronavirus disease 2019 and prostate cancer. Future Med. 2020, 16, 2029–2033. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.; Li, W.; Bao, J.; Peng, Q.; Wen, D.; Wang, J.; Sun, B. The expression of SARS-CoV-2 receptor ACE2 and CD147, and protease TMPRSS2 in human and mouse brain cells and mouse brain tissues. Biochem. Biophys. Res. Commun. 2020, 533, 867–871. [Google Scholar] [CrossRef]
- Cantuti-Castelvetri, L.; Ojha, R.; Pedro, L.D.; Djannatian, M.; Franz, J.; Kuivanen, S.; van der Meer, F.; Kallio, K.; Kaya, T.; Anastasina, M. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science 2020, 370, 856–860. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368. [Google Scholar] [CrossRef]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L.; Guo, R.; Chen, T.; Hu, J. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat. Commun. 2020, 11, 1620. [Google Scholar] [CrossRef]
- Chen, Z.; Mi, L.; Xu, J.; Yu, J.; Wang, X.; Jiang, J.; Xing, J.; Shang, P.; Qian, A.; Li, Y. Function of HAb18G/CD147 in invasion of host cells by severe acute respiratory syndrome coronavirus. J. Infect. Dis. 2005, 191, 755–760. [Google Scholar] [CrossRef]
- Wang, K.; Chen, W.; Zhou, Y.-S.; Lian, J.-Q.; Zhang, Z.; Du, P.; Gong, L.; Zhang, Y.; Cui, H.-Y.; Geng, J.-J. SARS-CoV-2 invades host cells via a novel route: CD147-spike protein. bioRxiv 2020. [Google Scholar] [CrossRef]
- Simmons, G.; Gosalia, D.N.; Rennekamp, A.J.; Reeves, J.D.; Diamond, S.L.; Bates, P. Inhibitors of cathepsin L prevent severe acute respiratory syndrome coronavirus entry. Proc. Natl. Acad. Sci. USA 2005, 102, 11876–11881. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.-C.; Bosch, B.J.; Li, F.; Li, W.; Lee, K.H.; Ghiran, S.; Vasilieva, N.; Dermody, T.S.; Harrison, S.C.; Dormitzer, P.R. SARS coronavirus, but not human coronavirus NL63, utilizes cathepsin L to infect ACE2-expressing cells. J. Biol. Chem. 2006, 281, 3198–3203. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.-X.; Zheng, X.-R.; Peng, W.; Wu, M.-L.; Mao, X.-Y. Vascular endothelial growth factor (VEGF) as a vital target for brain inflammation during the COVID-19 outbreak. ACS Chem. Neurosci. 2020, 11, 1704–1705. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Han, J.; Wu, X.; Zeng, H.; Liu, J.; Zhang, H. VEGF-D: A novel biomarker for detection of COVID-19 progression. Crit. Care 2020, 24, 373. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Vardeny, O.; Michel, T.; McMurray, J.J.; Pfeffer, M.A.; Solomon, S.D. Renin–angiotensin–aldosterone system inhibitors in patients with COVID-19. N. Engl. J. Med. 2020, 382, 1653–1659. [Google Scholar] [CrossRef]
- Rhoades, R.; Solomon, S.; Johnson, C.; Teng, S. Impact of SARS-CoV-2 on host factors involved in mental disorders. Front. Microbiol. 2022, 13, 845559. [Google Scholar] [CrossRef]
- Polidoro, R.B.; Hagan, R.S.; de Santis Santiago, R.; Schmidt, N.W. Overview: Systemic inflammatory response derived from lung injury caused by SARS-CoV-2 infection explains severe outcomes in COVID-19. Front. Immunol. 2020, 11, 1626. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Méndez-García, L.A.; Solleiro-Villavicencio, H.; Guartazaca-Guerrero, S.; Rodríguez-Morales, J.; Carrillo-Ruiz, J.D. Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients. Trop. Med. Infect. Dis. 2023, 8, 290. [Google Scholar] [CrossRef]
- Picone, P.; Sanfilippo, T.; Guggino, R.; Scalisi, L.; Monastero, R.; Baschi, R.; Mandalà, V.; San Biagio, L.; Rizzo, M.; Giacomazza, D. Neurological consequences, mental health, physical care, and appropriate nutrition in long-COVID-19. Cell. Mol. Neurobiol. 2023, 43, 1685–1695. [Google Scholar] [CrossRef]
- Tsukahara, T.; Brann, D.H.; Datta, S.R. Mechanisms of SARS-CoV-2-associated anosmia. Physiol. Rev. 2023, 103, 2759–2766. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M. Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.; Sabadia, S.; La Ichan, R. A prospective study of neurological disorders in hospitalized COVID-19 patients in New York city. Neurology 2020. [Google Scholar] [CrossRef]
- Peron, J.P.S. Direct and indirect impact of SARS-CoV-2 on the brain. Hum. Genet. 2023, 142, 1317–1326. [Google Scholar] [CrossRef]
- Ahmadi, S.; Khaledi, S. Brain Renin–Angiotensin System: From Physiology to Pathology in Neuronal Complications Induced by SARS-CoV-2. Anal. Cell. Pathol. 2023, 2023, 8883492. [Google Scholar] [CrossRef]
- Yan, C.H.; Faraji, F.; Prajapati, D.P.; Boone, C.E.; DeConde, A.S. Association of chemosensory dysfunction and COVID-19 in patients presenting with influenza-like symptoms. In International Forum of Allergy & Rhinology; John and Wiley and Sons: Hoboken, NJ, USA, 2020; pp. 806–813. [Google Scholar]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Granholm, A.-C. Long-term effects of SARS-CoV-2 in the brain: Clinical consequences and molecular mechanisms. J. Clin. Med. 2023, 12, 3190. [Google Scholar] [CrossRef]
- Ahmed, W.; Kuniyan, M.S.; Jawed, A.M.; Chen, L. Engineered Extracellular Vesicles for Drug Delivery in Therapy of Stroke. Pharmaceutics 2023, 15, 2173. [Google Scholar] [CrossRef]
- Abboud, H.; Abboud, F.Z.; Kharbouch, H.; Arkha, Y.; El Abbadi, N.; El Ouahabi, A. COVID-19 and SARS-CoV-2 infection: Pathophysiology and clinical effects on the nervous system. World Neurosurg. 2020, 140, 49–53. [Google Scholar] [CrossRef]
- Zhu, Z.-H.; Jia, F.; Ahmed, W.; Zhang, G.-L.; Wang, H.; Lin, C.-Q.; Chen, W.-H.; Chen, L.-K. Neural stem cell-derived exosome as a nano-sized carrier for BDNF delivery to a rat model of ischemic stroke. Neural Regen. Res. 2023, 18, 404. [Google Scholar] [PubMed]
- Forero, K.; Buqaileh, R.; Sunderman, C.; AbouAlaiwi, W. COVID-19 and Neurological Manifestations. Brain Sci. 2023, 13, 1137. [Google Scholar] [CrossRef] [PubMed]
- Fugate, J.E.; Lyons, J.L.; Thakur, K.T.; Smith, B.R.; Hedley-Whyte, E.T.; Mateen, F.J. Infectious causes of stroke. Lancet Infect. Dis. 2014, 14, 869–880. [Google Scholar] [CrossRef] [PubMed]
- Nagel, M.; Cohrs, R.; Mahalingam, R.; Wellish, M.C.; Forghani, B.; Schiller, A.; Safdieh, J.E.; Kamenkovich, E.; Ostrow, L.W.; Levy, M. The varicella zoster virus vasculopathies: Clinical, CSF, imaging, and virologic features. Neurology 2008, 70, 853–860. [Google Scholar] [CrossRef]
- Ghotbi, Z.; Estakhr, M.; Hosseini, M.; Shahripour, R.B. Cerebral Vasomotor Reactivity in COVID-19: A Narrative Review. Life 2023, 13, 1614. [Google Scholar] [CrossRef]
- Stein, L.K.; Mayman, N.A.; Dhamoon, M.S.; Fifi, J.T. The emerging association between COVID-19 and acute stroke. Trends Neurosci. 2021, 44, 527–537. [Google Scholar] [CrossRef]
- Maury, A.; Lyoubi, A.; Peiffer-Smadja, N.; de Broucker, T.; Meppiel, E. Neurological manifestations associated with SARS-CoV-2 and other coronaviruses: A narrative review for clinicians. Rev. Neurol. 2021, 177, 51–64. [Google Scholar] [CrossRef]
- Carod-Artal, F.J. Complicaciones neurológicas por coronavirus y COVID-19. Rev. Neurol. 2020, 70, 311–322. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A. Large-vessel stroke as a presenting feature of COVID-19 in the young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef]
- Wang, L.; Ren, Z.; Ma, L.; Han, Y.; Wei, W.; Jiang, E.; Ji, X.-Y. Progress in research on SARS-CoV-2 infection causing neurological diseases and its infection mechanism. Front. Neurol. 2021, 11, 592888. [Google Scholar] [CrossRef] [PubMed]
- Morassi, M.; Bagatto, D.; Cobelli, M.; D’Agostini, S.; Gigli, G.L.; Bnà, C.; Vogrig, A. Stroke in patients with SARS-CoV-2 infection: Case series. J. Neurol. 2020, 267, 2185–2192. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, M.; Wang, M.; Zhou, Y.; Chang, J.; Xian, Y.; Wang, D.; Mao, L.; Jin, H.; Hu, B. Acute cerebrovascular disease following COVID-19: A single center, retrospective, observational study. Stroke Vasc. Neurol. 2020, 5. [Google Scholar] [CrossRef]
- Sharifi-Razavi, A.; Karimi, N.; Rouhani, N. COVID-19 and intracerebral haemorrhage: Causative or coincidental? New Microbes New Infect. 2020, 35, 100669. [Google Scholar] [CrossRef] [PubMed]
- Siegler, J.E.; Cardona, P.; Arenillas, J.F.; Talavera, B.; Guillen, A.N.; Chavarría-Miranda, A.; de Lera, M.; Khandelwal, P.; Bach, I.; Patel, P. Cerebrovascular events and outcomes in hospitalized patients with COVID-19: The SVIN COVID-19 multinational registry. Int. J. Stroke 2021, 16, 437–447. [Google Scholar] [CrossRef]
- Sharifian-Dorche, M.; Huot, P.; Osherov, M.; Wen, D.; Saveriano, A.; Giacomini, P.S.; Antel, J.P.; Mowla, A. Neurological complications of coronavirus infection; a comparative review and lessons learned during the COVID-19 pandemic. J. Neurol. Sci. 2020, 417, 117085. [Google Scholar] [CrossRef]
- Favas, T.T.; Dev, P.; Chaurasia, R.N.; Chakravarty, K.; Mishra, R.; Joshi, D.; Mishra, V.N.; Kumar, A.; Singh, V.K.; Pandey, M.; et al. Neurological manifestations of COVID-19: A systematic review and meta-analysis of proportions. Neurol. Sci. 2020, 41, 3437–3470. [Google Scholar] [CrossRef]
- Rigamonti, A.; Mantero, V.; Piamarta, F.; Spena, G.; Salmaggi, A. Cerebral venous thrombosis associated with coronavirus infection: An underestimated entity? Neurol. Sci. 2021, 42, 317–318. [Google Scholar] [CrossRef]
- Chougar, L.; Mathon, B.; Weiss, N.; Degos, V.; Shor, N. Atypical Deep Cerebral Vein Thrombosis with Hemorrhagic Venous Infarction in a Patient Positive for COVID-19. Am. J. Neuroradiol. 2020, 41, 1377–1379. [Google Scholar] [CrossRef]
- Huang, Y.H.; Jiang, D.; Huang, J.T. SARS-CoV-2 detected in cerebrospinal fluid by PCR in a case of COVID-19 encephalitis. Brain Behav. Immun. 2020, 87, 149. [Google Scholar] [CrossRef]
- Efe, I.E.; Aydin, O.U.; Alabulut, A.; Celik, O.; Aydin, K. COVID-19—Associated encephalitis mimicking glial tumor. World Neurosurg. 2020, 140, 46–48. [Google Scholar] [CrossRef] [PubMed]
- McAbee, G.N.; Brosgol, Y.; Pavlakis, S.; Agha, R.; Gaffoor, M. Encephalitis associated with COVID-19 infection in an 11-year-old child. Pediatr. Neurol. 2020, 109, 94. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Khan, A.; Sundar, W.H.; Naseem, H.; Chen, W.; Feng, J.; Durrani, S.; Chen, L. Neurological diseases caused by coronavirus infection of the respiratory airways. Brain Sci. Adv. 2020, 6, 324–343. [Google Scholar] [CrossRef]
- Reiss, A.B.; Greene, C.; Dayaramani, C.; Rauchman, S.H.; Stecker, M.M.; De Leon, J.; Pinkhasov, A. Long COVID, the Brain, Nerves, and Cognitive Function. Neurol. Int. 2023, 15, 821–841. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pinedo, U.; Matias-Guiu, J.; Sanclemente-Alaman, I.; Moreno-Jimenez, L.; Montero-Escribano, P.; Matias-Guiu, J.A. SARS-CoV-2 as a potential trigger of neurodegenerative diseases. Mov. Disord. 2020, 35, 1104. [Google Scholar] [CrossRef]
- von Weyhern, C.H.; Kaufmann, I.; Neff, F.; Kremer, M. Early evidence of pronounced brain involvement in fatal COVID-19 outcomes. Lancet 2020, 395, e109. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F.; Sabeti, P. Neuropathological Features of COVID-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef]
- Welge-Lüssen, A.; Wolfensberger, M. Olfactory disorders following upper respiratory tract infections. Tast. Smell 2006, 63, 125–132. [Google Scholar]
- Boscolo-Rizzo, P.; Borsetto, D.; Fabbris, C.; Spinato, G.; Frezza, D.; Menegaldo, A.; Mularoni, F.; Gaudioso, P.; Cazzador, D.; Marciani, S.; et al. Evolution of Altered Sense of Smell or Taste in Patients With Mildly Symptomatic COVID-19. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 729–732. [Google Scholar] [CrossRef]
- Zubair, A.S.; McAlpine, L.S.; Gardin, T.; Farhadian, S.; Kuruvilla, D.E.; Spudich, S. Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review. JAMA Neurol. 2020, 77, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Ermilov, V.; Barkanov, V.; Barkanova, O.; Dorofeev, N.; Filatov, V. Clinical and anatomical features of SARS-CoV-2 with acute hemorrhagic necrotizing encephalopathy. Arkhiv Patol. 2021, 83, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Keyhanian, K.; Umeton, R.P.; Mohit, B.; Davoudi, V.; Hajighasemi, F.; Ghasemi, M. SARS-CoV-2 and nervous system: From pathogenesis to clinical manifestation. J. Neuroimmunol. 2021, 350, 577436. [Google Scholar] [CrossRef] [PubMed]
- Alberti, P.; Beretta, S.; Piatti, M.; Karantzoulis, A.; Piatti, M.L.; Santoro, P.; Viganò, M.; Giovannelli, G.; Pirro, F.; Montisano, D.A. Guillain-Barré syndrome related to COVID-19 infection. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7. [Google Scholar] [CrossRef]
- Fantini, J.; Di Scala, C.; Chahinian, H.; Yahi, N. Structural and molecular modelling studies reveal a new mechanism of action of chloroquine and hydroxychloroquine against SARS-CoV-2 infection. Int. J. Antimicrob. Agents 2020, 55, 105960. [Google Scholar] [CrossRef]
- Tiet, M.Y.; AlShaikh, N. Guillain-Barré syndrome associated with COVID-19 infection: A case from the UK. BMJ Case Rep. CP 2020, 13, e236536. [Google Scholar] [CrossRef]
- Jin, M.; Tong, Q. Rhabdomyolysis as potential late complication associated with COVID-19. Emerg. Infect. Dis. 2020, 26, 1618. [Google Scholar] [CrossRef]
- Jiang, X.; Coffee, M.; Bari, A.; Wang, J.; Jiang, X.; Huang, J.; Shi, J.; Dai, J.; Cai, J.; Zhang, T.; et al. Towards an Artificial Intelligence Framework for Data-Driven Prediction of Coronavirus Clinical Severity. Comput. Mater. Contin. 2020, 63, 537–551. [Google Scholar] [CrossRef]
- Yuksel, H.; Gursoy, G.T.; Dirik, E.B.; Kenar, S.G.; Bektas, H.; Yamanel, L.; Guner, H.R. Neurological manifestations of COVID-19 in confirmed and probable cases: A descriptive study from a large tertiary care center. J. Clin. Neurosci. 2021, 86, 97–102. [Google Scholar] [CrossRef]
- Galassi, G.; Marchioni, A. Myasthenia gravis at the crossroad of COVID-19: Focus on immunological and respiratory interplay. Acta Neurol. Belg. 2021, 121, 633–642. [Google Scholar] [CrossRef]
- Solé, G.; Mathis, S.; Friedman, D.; Salort-Campana, E.; Tard, C.; Bouhour, F.; Magot, A.; Annane, D.; Clair, B.; Le Masson, G. Impact of coronavirus disease 2019 in a French cohort of myasthenia gravis. Neurology 2021, 96, e2109–e2120. [Google Scholar] [CrossRef] [PubMed]
- Camelo-Filho, A.E.; Silva, A.M.; Estephan, E.P.; Zambon, A.A.; Mendonça, R.H.; Souza, P.V.; Pinto, W.B.; Oliveira, A.S.; Dangoni-Filho, I.; Pouza, A.F. Myasthenia gravis and COVID-19: Clinical characteristics and outcomes. Front. Neurol. 2020, 11, 1053. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Geddes, J.R.; Husain, M.; Luciano, S.; Harrison, P.J. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospective cohort study using electronic health records. Lancet Psychiatry 2021, 8, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62,354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.E.; Kumar, S.; Rajji, T.K.; Pollock, B.G.; Mulsant, B.H. Anticipating and Mitigating the Impact of the COVID-19 Pandemic on Alzheimer’s Disease and Related Dementias. Am. J. Geriatr. Psychiatry 2020, 28, 712–721. [Google Scholar] [CrossRef]
- Suzuki, M.; Hotta, M.; Nagase, A.; Yamamoto, Y.; Hirakawa, N.; Satake, Y.; Nagata, Y.; Suehiro, T.; Kanemoto, H.; Yoshiyama, K.; et al. The behavioral pattern of patients with frontotemporal dementia during the COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1231–1234. [Google Scholar] [CrossRef]
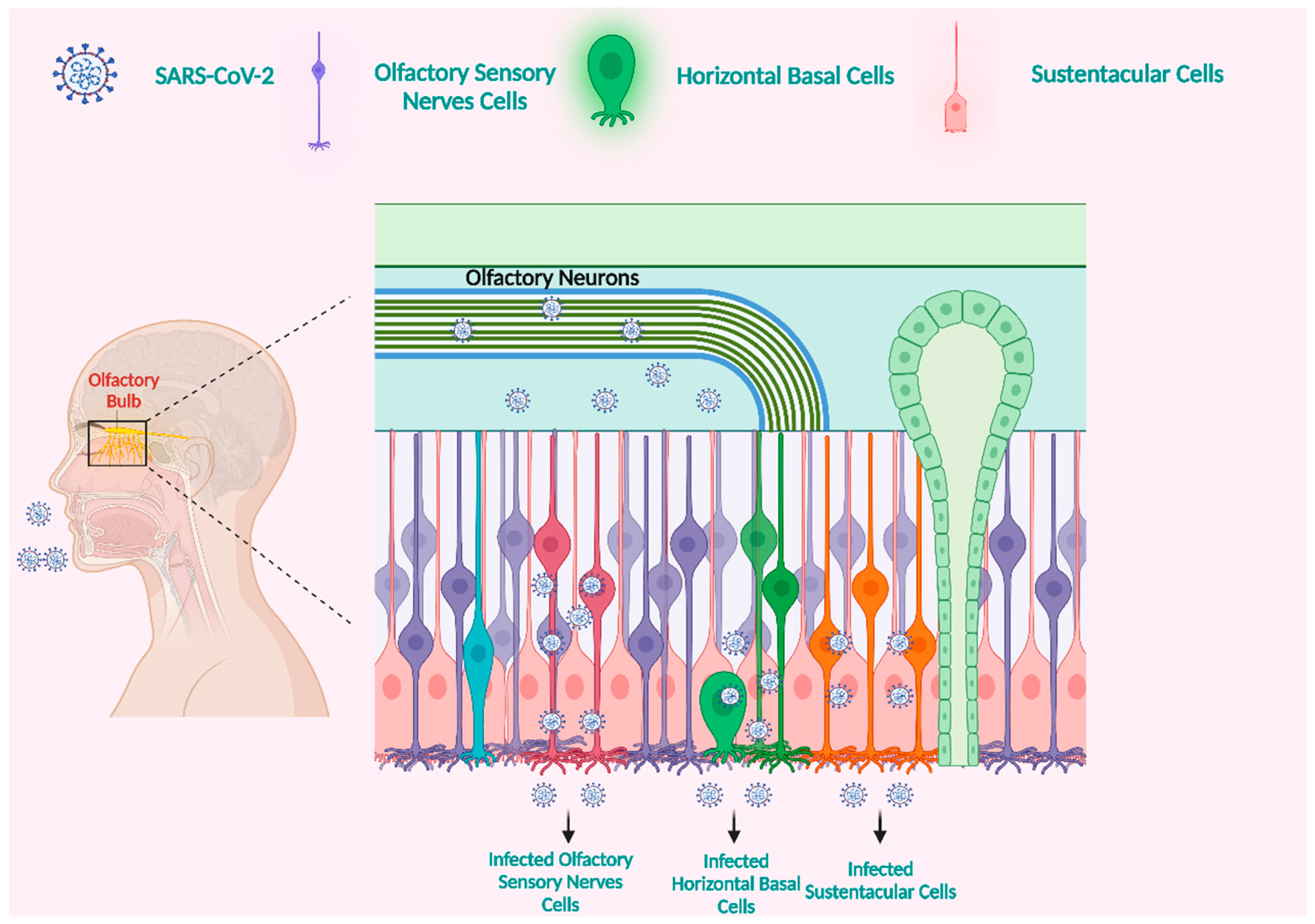
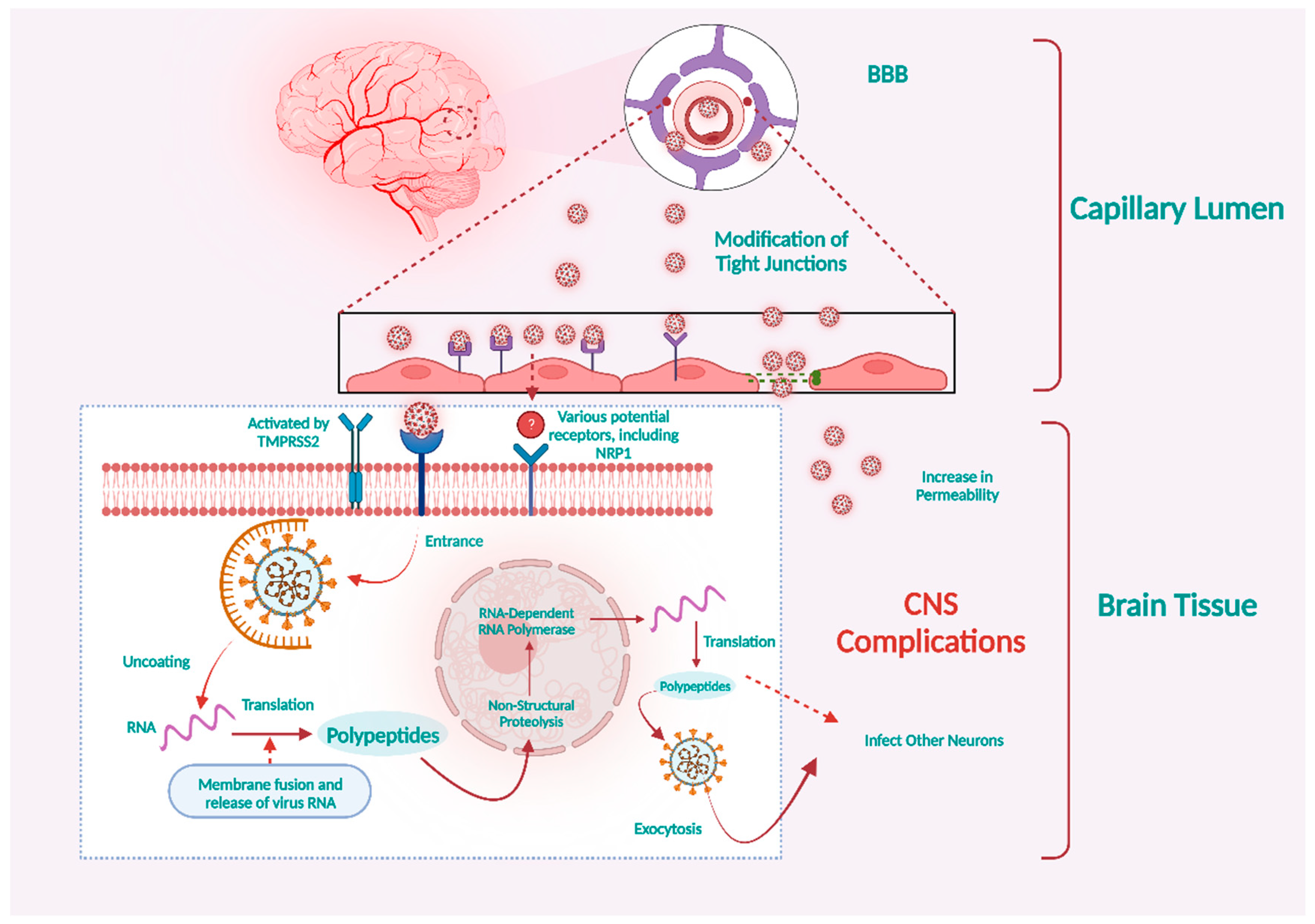
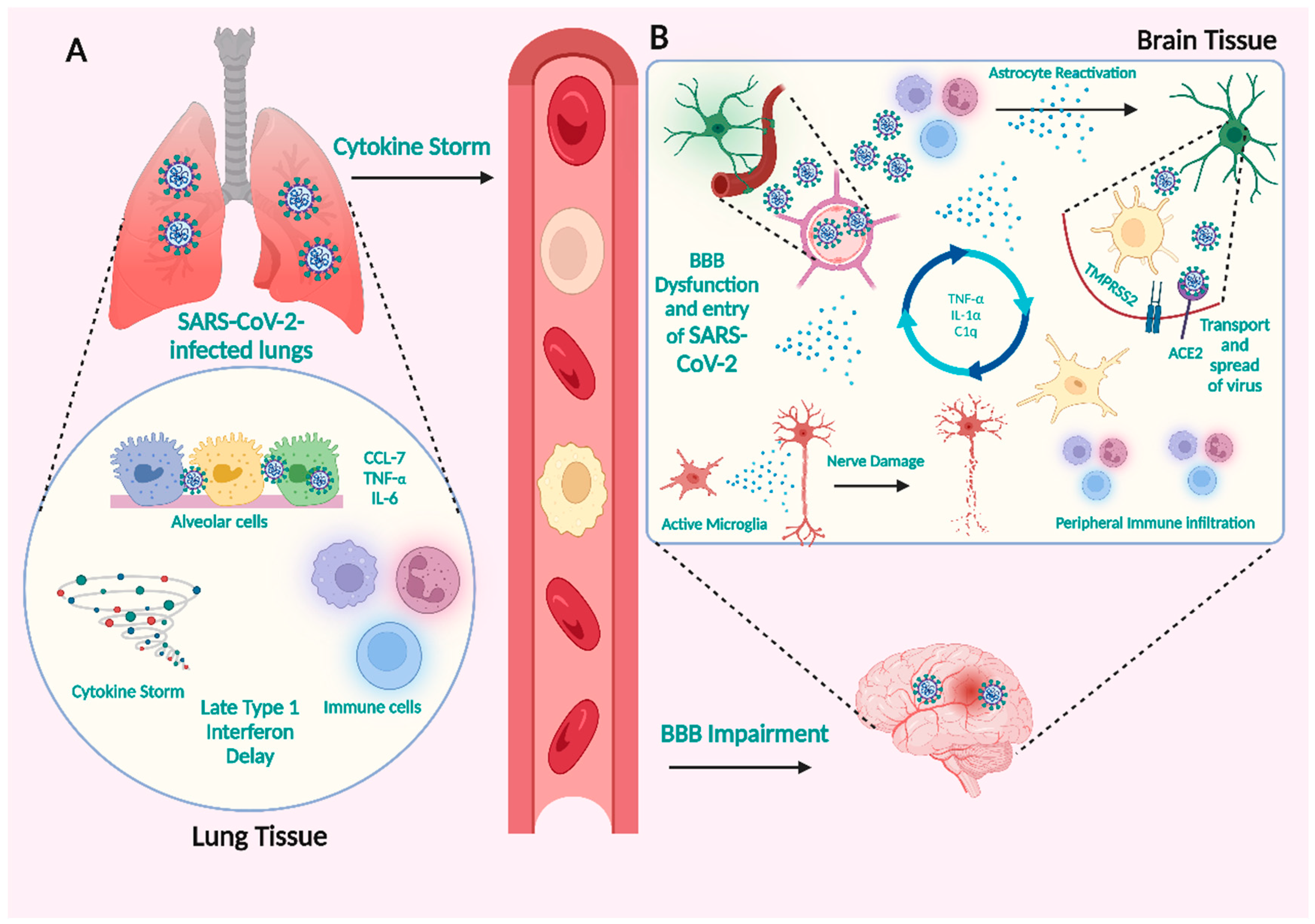
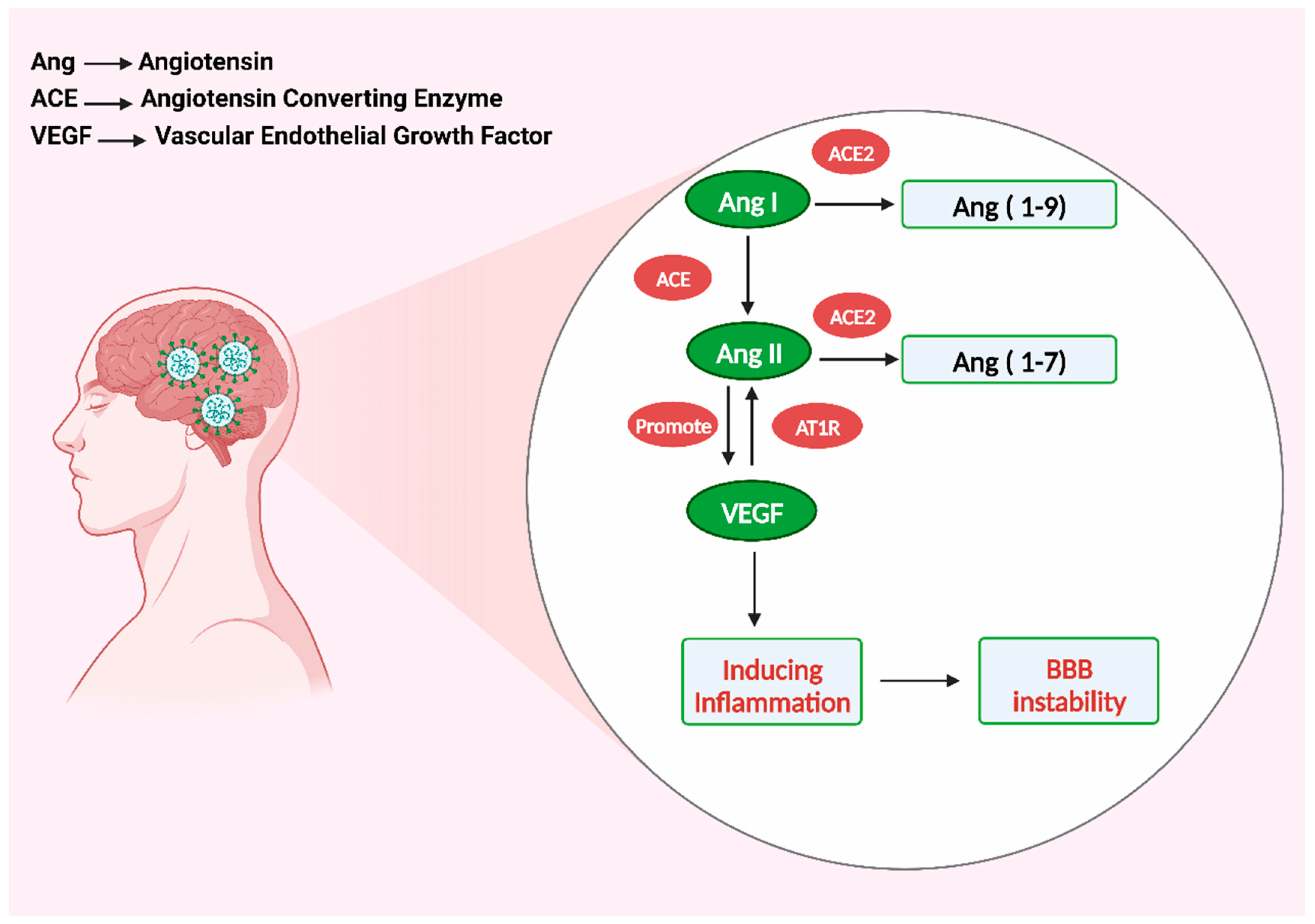
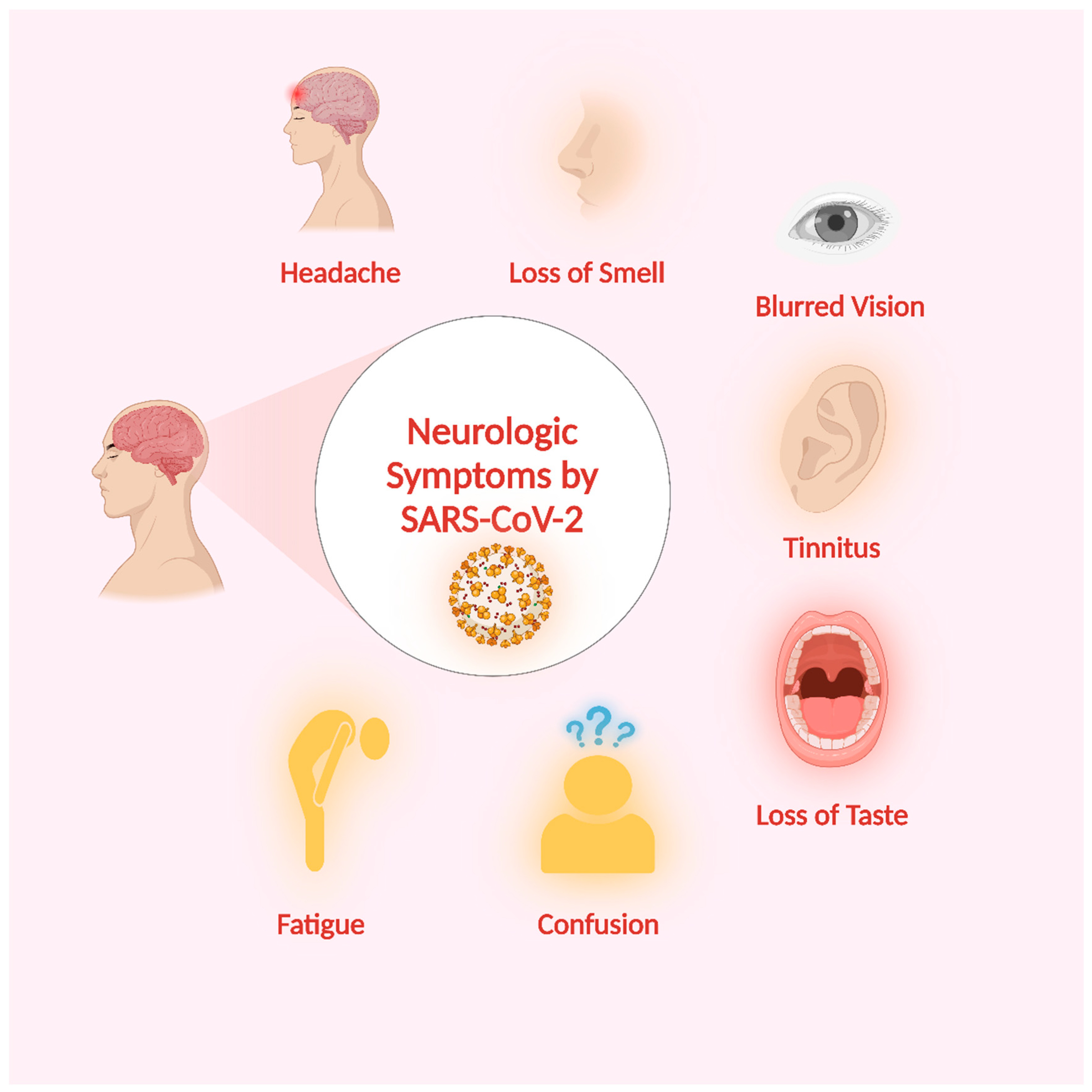
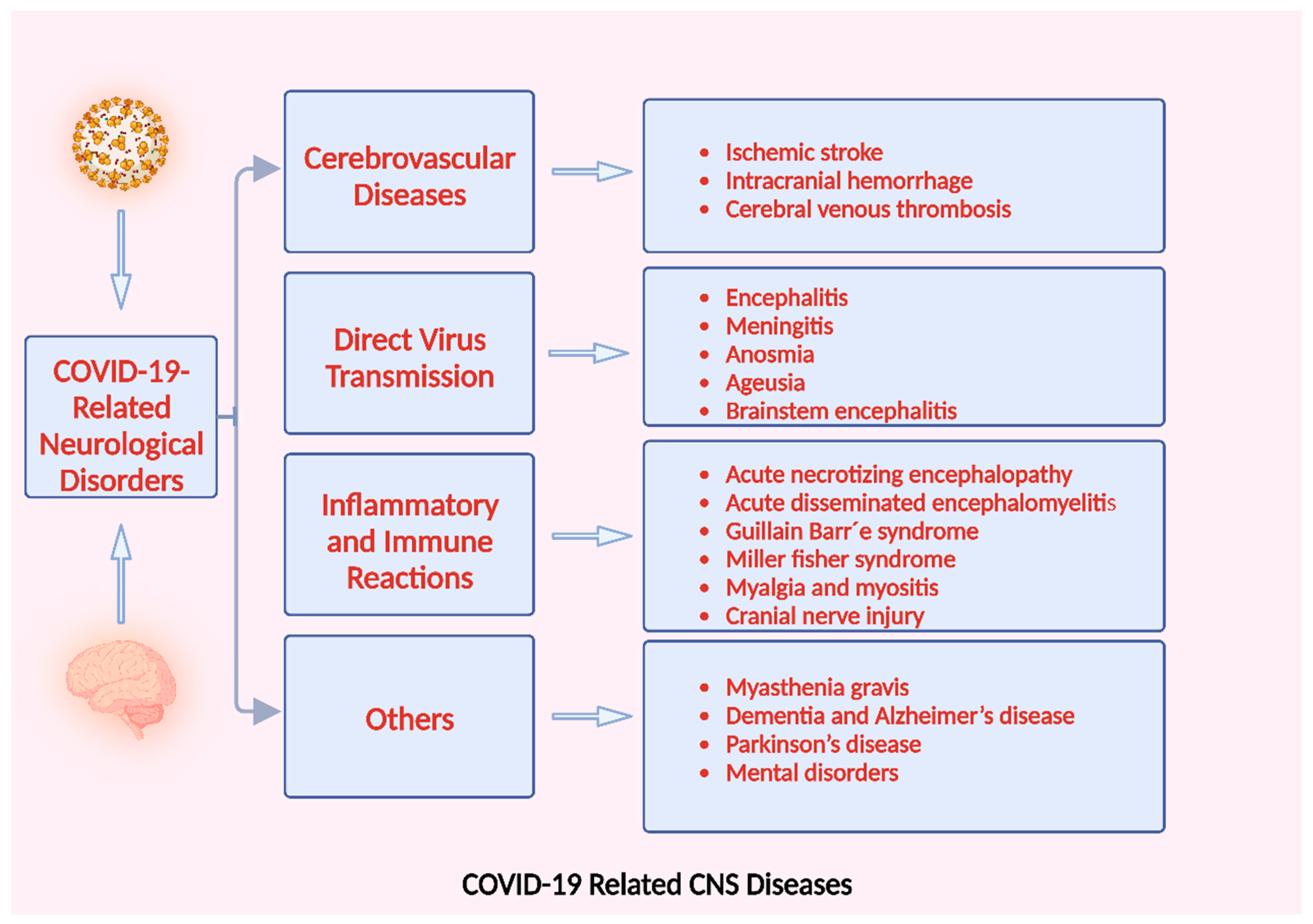
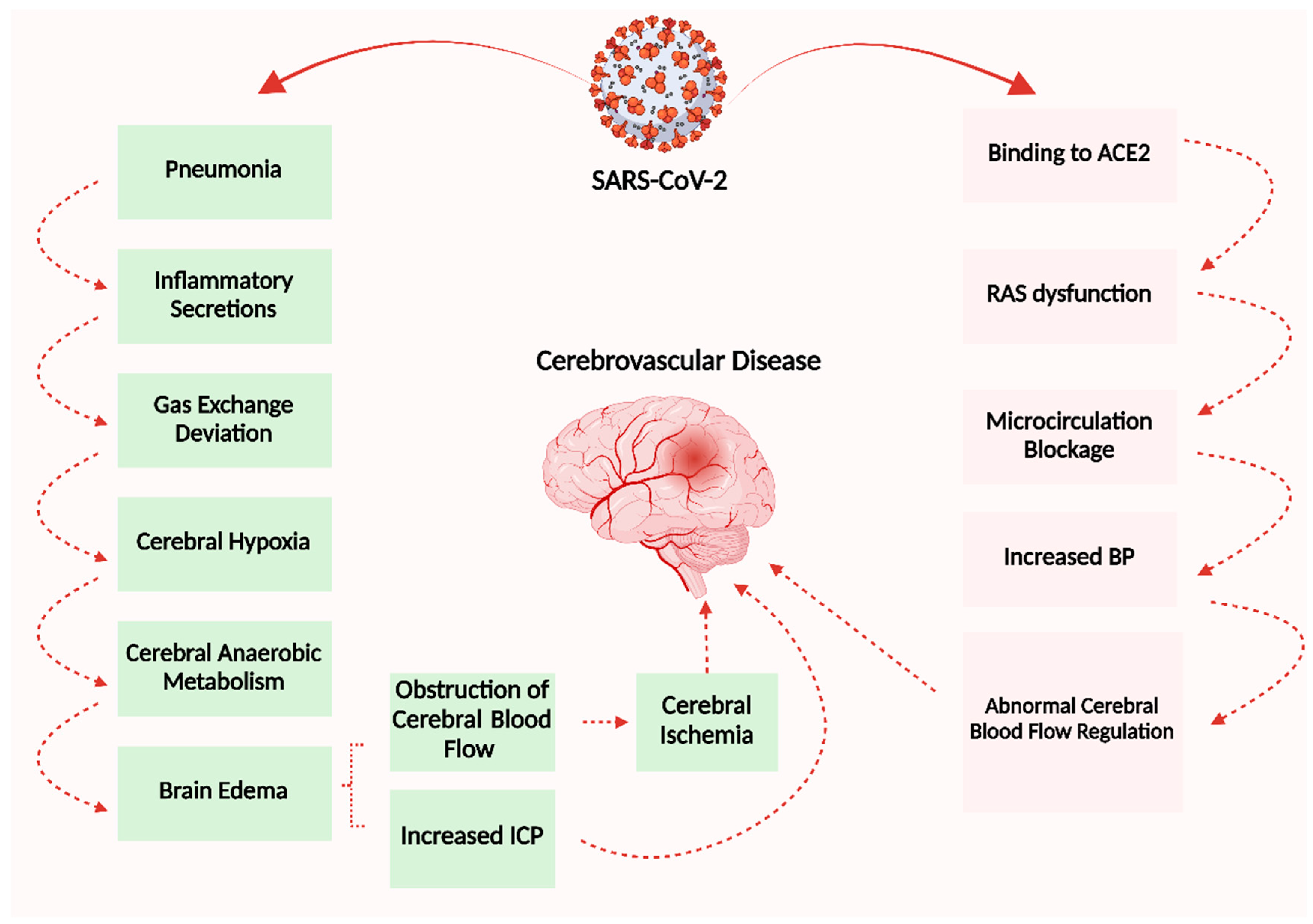
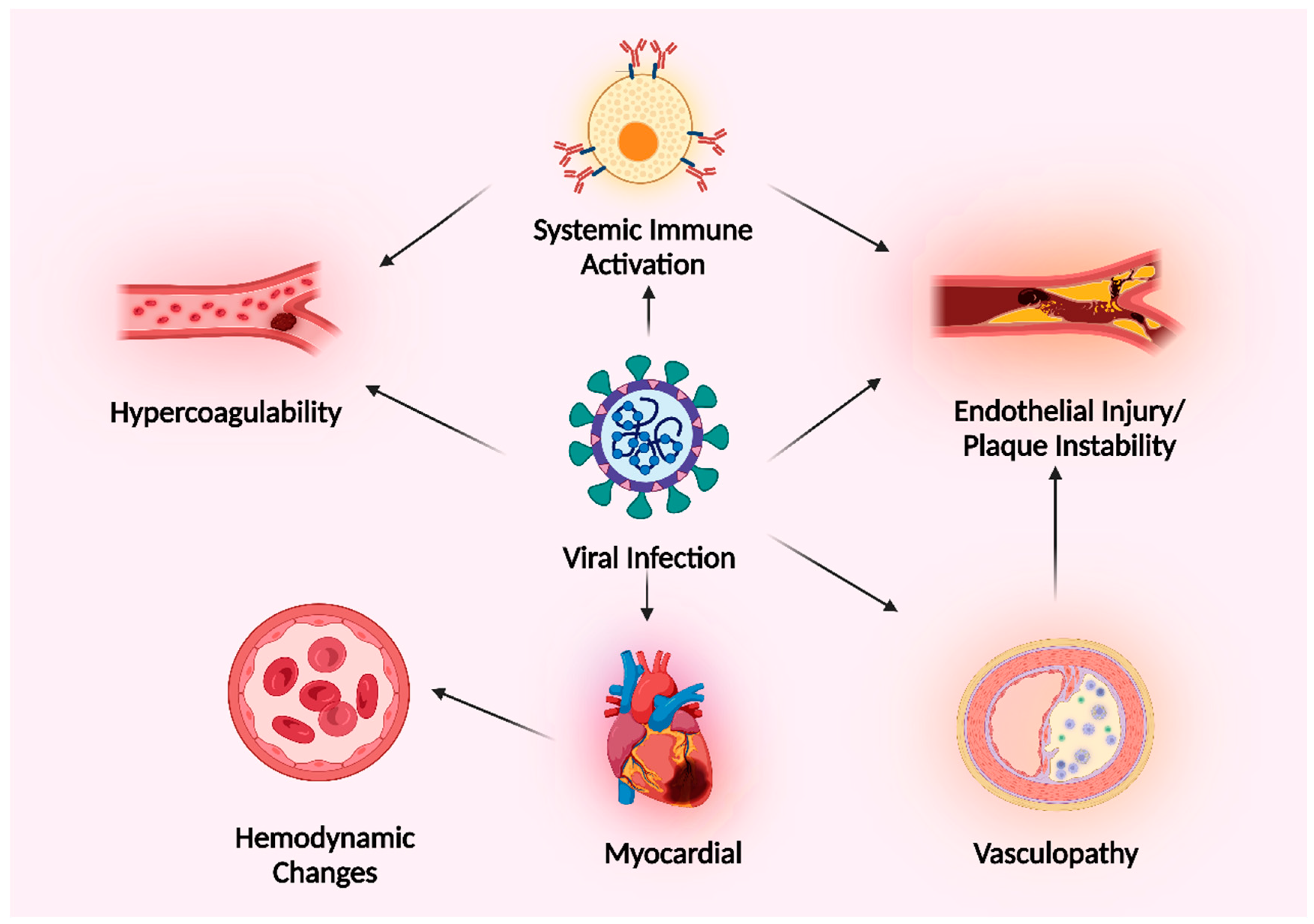
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).