
Gut Microbiota in Diagnosis, Therapy and Prognosis of Cholangiocarcinoma and Gallbladder Carcinoma—A Scoping Review

 ,
,  , and
, and
Abstract
:1. Introduction
1.1. Systematic of Biliary Tract Cancers
1.2. Diagnosis, Therapy and Prognosis of Biliary Tract Cancers
1.3. The Gut–Liver Axis
2. Methods
2.1. Population
2.2. Research Questions
3. Results
3.1. Do Patients with CCA or Gallbladder Carcinoma Show Distinct Gut Microbiota Changes Compared to Healthy Controls?
3.1.1. Gut Microbiota Changes in CCA Patients
3.1.2. Gut Microbiota Changes in Gallbladder Carcinoma
3.2. Does the Gut Microbiota Affect the Postoperative Outcome of CCA or Gallbladder Carcinoma Patients Who Underwent Curative-Intent Surgery?
3.3. Does the Gut Microbiota Affect the Chemotherapeutic or Systemic Treatment Response of CCA or Gallbladder Carcinoma Patients?
3.4. Does the Gut Microbiota Affect the Prognosis and the Overall Survival of Patients Suffering from CCA or Gallbladder Carcinoma?
4. Discussion
4.1. Limitations of the Included Studies
4.2. Alteration of Gut Microorganisms in CCA
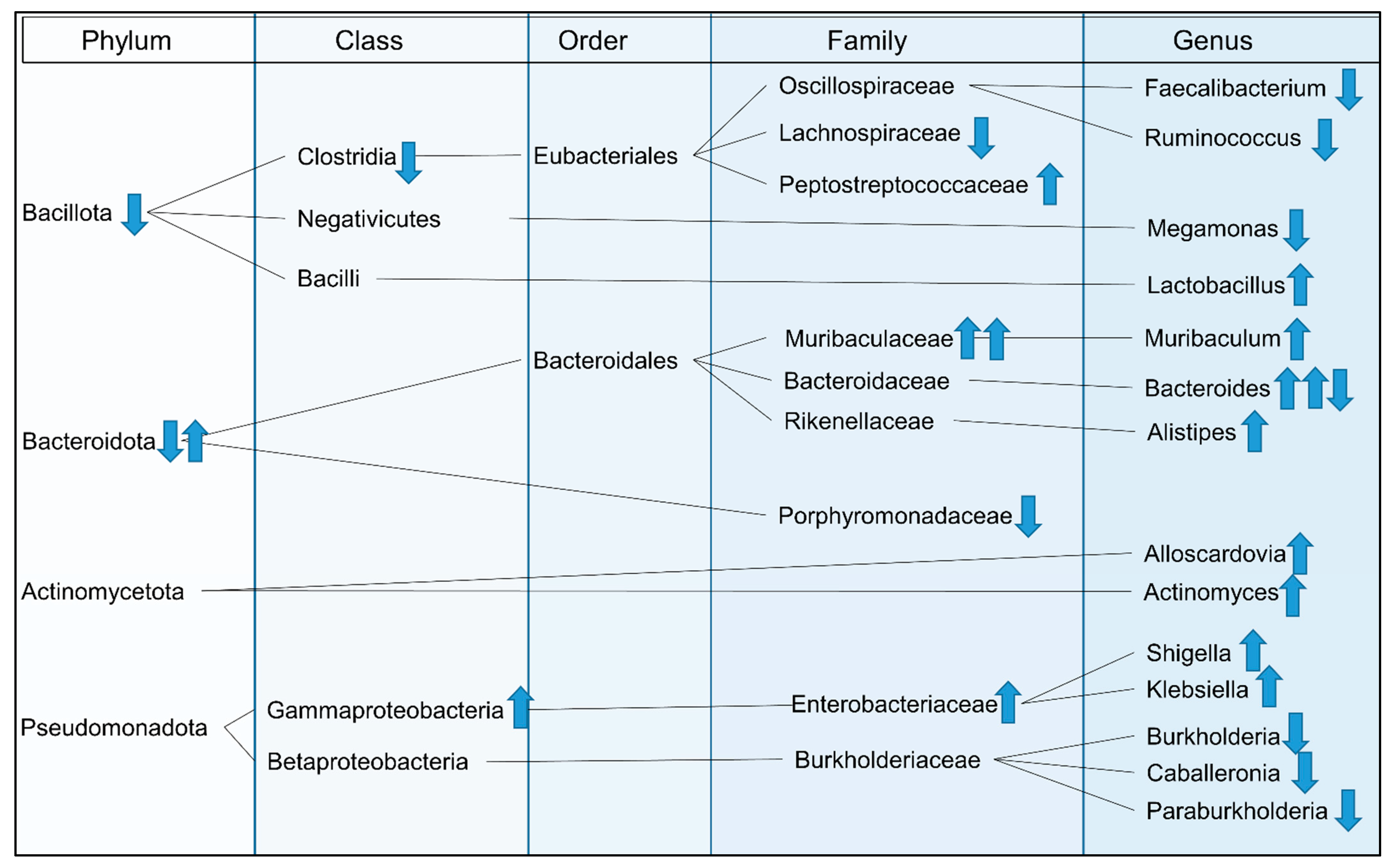
4.2.1. Genera with Lower Abundances in CCA
4.2.2. Genera with Higher Abundances in CCA
4.3. Clinical Consequences and Future Aspects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef]
- Squadroni, M.; Tondulli, L.; Gatta, G.; Mosconi, S.; Beretta, G.; Labianca, R. Cholangiocarcinoma. Crit. Rev. Oncol. Hematol. 2017, 116, 11–31. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.M.; Olaizola, P.; Paiva, N.A.; Olaizola, I.; Agirre-Lizaso, A.; Landa, A.; Bujanda, L.; Perugorria, M.J.; Banales, J.M. Pathogenesis of Cholangiocarcinoma. Annu. Rev. Pathol. Mech. Dis. 2021, 16, 433–463. [Google Scholar] [CrossRef] [PubMed]
- Ellington, T.D.; Momin, B.; Wilson, R.J.; Henley, S.J.; Wu, M.; Ryerson, A.B. Incidence and Mortality of Cancers of the Biliary Tract, Gallbladder, and Liver by Sex, Age, Race/Ethnicity, and Stage at Diagnosis: United States, 2013 to 2017. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.; Lee, S.; Azad, N.S.; Borad, M.J.; Kate Kelley, R.; Sivaraman, S.; Teschemaker, A.; Chopra, I.; Janjan, N.; Parasuraman, S.; et al. Temporal Changes in Cholangiocarcinoma Incidence and Mortality in the United States from 2001 to 2017. Oncologist 2022, 27, 874–883. [Google Scholar] [CrossRef]
- Welzel, T.M.; Mellemkjaer, L.; Gloria, G.; Sakoda, L.C.; Hsing, A.W.; Ghormli, L.E.; Olsen, J.H.; McGlynn, K.A. Risk factors for intrahepatic cholangiocarcinoma in a low-risk population: A nationwide case-control study. Int. J. Cancer 2007, 120, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Yang, T.; Wu, M.; Shen, F. Intrahepatic cholangiocarcinoma: Epidemiology, risk factors, diagnosis and surgical management. Cancer Lett. 2016, 379, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.-Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef]
- Khan, S.A.; Tavolari, S.; Brandi, G. Cholangiocarcinoma: Epidemiology and risk factors. Liver Int. 2019, 39, 19–31. [Google Scholar] [CrossRef]
- Ahn, D.H.; Bekaii-Saab, T. Biliary cancer: Intrahepatic cholangiocarcinoma vs. extrahepatic cholangiocarcinoma vs. gallbladder cancers: Classification and therapeutic implications. J. Gastrointest. Oncol. 2017, 8, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Roa, J.C.; García, P.; Kapoor, V.K.; Maithel, S.K.; Javle, M.; Koshiol, J. Gallbladder cancer. Nat. Rev. Dis. Primers 2022, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Wernberg, J.A.; Lucarelli, D.D. Gallbladder Cancer. Surg. Clin. N. Am. 2014, 94, 343–360. [Google Scholar] [CrossRef] [PubMed]
- Hamaoka, M.; Kozaka, K.; Matsui, O.; Komori, T.; Matsubara, T.; Yoneda, N.; Yoshida, K.; Inoue, D.; Kitao, A.; Koda, W.; et al. Early detection of intrahepatic cholangiocarcinoma. Jpn. J. Radiol. 2019, 37, 669–684. [Google Scholar] [CrossRef] [PubMed]
- Joo, I.; Lee, J.M. Imaging bile duct tumors: Pathologic concepts, classification, and early tumor detection. Abdom. Imaging 2013, 38, 1334–1350. [Google Scholar] [CrossRef] [PubMed]
- Doherty, B.; Nambudiri, V.E.; Palmer, W.C. Update on the Diagnosis and Treatment of Cholangiocarcinoma. Curr. Gastroenterol. Rep. 2017, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, A.; Edeline, J.; Goyal, L. How I treat biliary tract cancer. ESMO Open 2022, 7, 100378. [Google Scholar] [CrossRef]
- Bitzer, M.; Groß, S.; Albert, J.; Boda-Heggemann, J.; Brunner, T.; Caspari, R.; De Toni, E.; Dombrowski, F.; Evert, M.; Geier, A.; et al. S3-Leitlinie Diagnostik und Therapie biliärer Karzinome. Z. Gastroenterol. 2023, 61, 420–440. [Google Scholar] [CrossRef]
- Cillo, U.; Fondevila, C.; Donadon, M.; Gringeri, E.; Mocchegiani, F.; Schlitt, H.J.; Ijzermans, J.N.M.; Vivarelli, M.; Zieniewicz, K.; Olde Damink, S.W.M.; et al. Surgery for cholangiocarcinoma. Liver Int. 2019, 39, 143–155. [Google Scholar] [CrossRef]
- Machairas, N.; Lang, H.; Jayant, K.; Raptis, D.A.; Sotiropoulos, G.C. Intrahepatic cholangiocarcinoma: Limitations for resectability, current surgical concepts and future perspectives. Eur. J. Surg. Oncol. 2020, 46, 740–746. [Google Scholar] [CrossRef]
- Bartsch, F.; Heinrich, S.; Lang, H. Limits of Surgical Resection for Bile Duct Cancer. Visc. Med. 2015, 31, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Mueller, M.; Breuer, E.; Mizuno, T.; Bartsch, F.; Ratti, F.; Benzing, C.; Ammar-Khodja, N.; Sugiura, T.; Takayashiki, T.; Hessheimer, A.; et al. Perihilar Cholangiocarcinoma–Novel Benchmark Values for Surgical and Oncological Outcomes From 24 Expert Centers. Ann. Surg. 2021, 274, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy liver failure: A definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Koerkamp, B.G.; Wiggers, J.K.; Allen, P.J.; Besselink, M.G.; Blumgart, L.H.; Busch, O.R.C.; Coelen, R.J.; D’Angelica, M.I.; DeMatteo, R.P.; Gouma, D.J.; et al. Recurrence Rate and Pattern of Perihilar Cholangiocarcinoma after Curative Intent Resection. J. Am. Coll. Surg. 2015, 221, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Komaya, K.; Ebata, T.; Yokoyama, Y.; Igami, T.; Sugawara, G.; Mizuno, T.; Yamaguchi, J.; Nagino, M. Recurrence after curative-intent resection of perihilar cholangiocarcinoma: Analysis of a large cohort with a close postoperative follow-up approach. Surgery 2018, 163, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Sotiropoulos, G.C.; Sgourakis, G.; Schmitz, K.J.; Paul, A.; Hilgard, P.; Zöpf, T.; Trarbach, T.; Malagó, M.; Baba, H.A.; et al. Operations for Intrahepatic Cholangiocarcinoma: Single-Institution Experience of 158 Patients. J. Am. Coll. Surg. 2009, 208, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Knight, R.; Vrbanac, A.; Taylor, B.C.; Aksenov, A.; Callewaert, C.; Debelius, J.; Gonzalez, A.; Kosciolek, T.; McCall, L.-I.; McDonald, D.; et al. Best practices for analysing microbiomes. Nat. Rev. Microbiol. 2018, 16, 410–422. [Google Scholar] [CrossRef]
- Binda, C.; Gibiino, G.; Coluccio, C.; Sbrancia, M.; Dajti, E.; Sinagra, E.; Capurso, G.; Sambri, V.; Cucchetti, A.; Ercolani, G.; et al. Biliary Diseases from the Microbiome Perspective: How Microorganisms Could Change the Approach to Benign and Malignant Diseases. Microorganisms 2022, 10, 312. [Google Scholar] [CrossRef]
- Tanaka, A.; Mertens, J.C. Ulcerative Colitis with and without Primary Sclerosing Cholangitis: Two Different Diseases? Inflamm. Intest. Dis. 2016, 1, 9–14. [Google Scholar] [CrossRef]
- Bajer, L.; Kverka, M.; Kostovcik, M.; Macinga, P.; Dvorak, J.; Stehlikova, Z.; Brezina, J.; Wohl, P.; Spicak, J.; Drastich, P. Distinct gut microbiota profiles in patients with primary sclerosing cholangitis and ulcerative colitis. World J. Gastroenterol. 2017, 23, 4548. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, N.; Sasaki, N.; Aoki, R.; Miyamoto, K.; Suda, W.; Teratani, T.; Suzuki, T.; Koda, Y.; Chu, P.-S.; Taniki, N.; et al. Gut pathobionts underlie intestinal barrier dysfunction and liver T helper 17 cell immune response in primary sclerosing cholangitis. Nat. Microbiol. 2019, 4, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Hov, J.R.; Karlsen, T.H. The microbiota and the gut–liver axis in primary sclerosing cholangitis. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 135–154. [Google Scholar] [CrossRef]
- Sepich-Poore, G.D.; Zitvogel, L.; Straussman, R.; Hasty, J.; Wargo, J.A.; Knight, R. The microbiome and human cancer. Science 2021, 371, eabc4552. [Google Scholar] [CrossRef] [PubMed]
- Rao, B.; Ren, T.; Wang, X.; Wang, H.; Zou, Y.; Sun, Y.; Liu, S.; Ren, Z.; Yu, Z. Dysbiosis in the Human Microbiome of Cholangiocarcinoma. Front. Physiol. 2021, 12, 715536. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.M.; Manghi, P.; Asnicar, F.; Pasolli, E.; Armanini, F.; Zolfo, M.; Beghini, F.; Manara, S.; Karcher, N.; Pozzi, C.; et al. Metagenomic analysis of colorectal cancer datasets identifies cross-cohort microbial diagnostic signatures and a link with choline degradation. Nat. Med. 2019, 25, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Arthur, J.C.; Perez-Chanona, E.; Mühlbauer, M.; Tomkovich, S.; Uronis, J.M.; Fan, T.-J.; Campbell, B.J.; Abujamel, T.; Dogan, B.; Rogers, A.B.; et al. Intestinal inflammation targets cancer-inducing activity of the microbiota. Science 2012, 338, 120–123. [Google Scholar] [CrossRef]
- Dziubańska-Kusibab, P.J.; Berger, H.; Battistini, F.; Bouwman, B.A.M.; Iftekhar, A.; Katainen, R.; Cajuso, T.; Crosetto, N.; Orozco, M.; Aaltonen, L.A.; et al. Colibactin DNA-damage signature indicates mutational impact in colorectal cancer. Nat. Med. 2020, 26, 1063–1069. [Google Scholar] [CrossRef]
- Yoshimoto, S.; Loo, T.M.; Atarashi, K.; Kanda, H.; Sato, S.; Oyadomari, S.; Iwakura, Y.; Oshima, K.; Morita, H.; Hattori, M.; et al. Obesity-induced gut microbial metabolite promotes liver cancer through senescence secretome. Nature 2013, 499, 97–101. [Google Scholar] [CrossRef]
- Dapito, D.H.; Mencin, A.; Gwak, G.-Y.; Pradere, J.-P.; Jang, M.-K.; Mederacke, I.; Caviglia, J.M.; Khiabanian, H.; Adeyemi, A.; Bataller, R.; et al. Promotion of Hepatocellular Carcinoma by the Intestinal Microbiota and TLR4. Cancer Cell 2012, 21, 504–516. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Schreiber, G.; Haupt, C.C. Methodische Anleitung für Scoping Reviews (JBI-Methodologie). Z. Evidenz Fortbild. Qual. Gesundheitswesen 2019, 143, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nagaraja, V.; Eslick, G.D. Systematic review with meta-analysis: The relationship between chronic Salmonella typhi carrier status and gall-bladder cancer. Aliment. Pharmacol. Ther. 2014, 39, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Koshiol, J.; Wozniak, A.; Cook, P.; Adaniel, C.; Acevedo, J.; Azócar, L.; Hsing, A.W.; Roa, J.C.; Pasetti, M.F.; Miquel, J.F.; et al. Salmonella enterica serovar Typhi and gallbladder cancer: A case–control study and meta-analysis. Cancer Med. 2016, 5, 3310–3325. [Google Scholar] [CrossRef] [PubMed]
- Miyabe, K.; Chandrasekhara, V.; Wongjarupong, N.; Chen, J.; Yang, L.; Johnson, S.; Chia, N.; Walther-Antonio, M.; Yao, J.; Harrington, S.; et al. Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma. Cancers 2022, 14, 2120. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Li, J.; Jin, C.; Yang, J.; Zheng, C.; Chen, K.; Xie, Y.; Yang, Y.; Bo, Z.; Wang, J.; et al. Association of gut microbiome and primary liver cancer: A two-sample Mendelian randomization and case-control study. Liver Int. 2023, 43, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Deng, T.; Li, J.; He, B.; Chen, B.; Liu, F.; Chen, Z.; Zheng, J.; Shi, Z.; Zhang, T.; Deng, L.; et al. Gut microbiome alteration as a diagnostic tool and associated with inflammatory response marker in primary liver cancer. Hepatol. Int. 2022, 16, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Lu, S.; Zeng, Z.; Liu, Q.; Dong, Z.; Chen, Y.; Zhu, Z.; Hong, Z.; Zhang, T.; Du, G.; et al. Characterization of Gut Microbiota, Bile Acid Metabolism, and Cytokines in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 71, 893–906. [Google Scholar] [CrossRef]
- Zhang, T.; Zhang, S.; Jin, C.; Lin, Z.; Deng, T.; Xie, X.; Deng, L.; Li, X.; Ma, J.; Ding, X.; et al. A Predictive Model Based on the Gut Microbiota Improves the Diagnostic Effect in Patients with Cholangiocarcinoma. Front. Cell. Infect. Microbiol. 2021, 11, 1157. [Google Scholar] [CrossRef]
- Ito, Z.; Koido, S.; Kato, K.; Odamaki, T.; Horiuchi, S.; Akasu, T.; Saruta, M.; Hata, T.; Kumagai, Y.; Fujioka, S.; et al. Dysbiosis of the Fecal and Biliary Microbiota in Biliary Tract Cancer. Cancers 2022, 14, 5379. [Google Scholar] [CrossRef]
- Zhang, L.; Chen, C.; Chai, D.; Kuang, T.; Deng, W.; Wang, W. Alterations of gut mycobiota profiles in intrahepatic cholangiocarcinoma. Front. Microbiol. 2022, 13, 1090392. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Wang, D.; Long, J.; Yang, X.; Lin, J.; Song, Y.; Xie, F.; Xun, Z.; Wang, Y.; Wang, Y.; et al. Gut microbiome is associated with the clinical response to anti-PD-1 based immunotherapy in hepatobiliary cancers. J. Immunother. Cancer 2021, 9, e003334. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Zhao, R.; Zhou, C.; Zhong, Q.; Shi, J.; Su, C.; Li, Q.; Su, X.; Chi, H.; Lu, X.; et al. Feasibility and tolerability of sintilimab plus anlotinib as the second-line therapy for patients with advanced biliary tract cancers: An open-label, single-arm, phase II clinical trial. Int. J. Cancer 2023, 152, 1648–1658. [Google Scholar] [CrossRef]
- Zhang, Q.; Ma, C.; Duan, Y.; Heinrich, B.; Rosato, U.; Diggs, L.P.; Ma, L.; Roy, S.; Fu, Q.; Brown, Z.J.; et al. Gut Microbiome Directs Hepatocytes to Recruit MDSCs and Promote Cholangiocarcinoma. Cancer Discov. 2021, 11, 1248–1267. [Google Scholar] [CrossRef] [PubMed]
- Caygill, C.P.J.; Hill, M.J.; Braddick, M.; Sharp, J.C.M. Cancer mortality in chronic typhoid and paratyphoid carriers. Lancet 1994, 343, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Hanazaki, K.; Kajikawa, S.; Shimozawa, N.; Shimada, K.; Hiraguri, M.; Koide, N.; Adachi, W.; Amano, J. Prognostic factors of intrahepatic cholangiocarcinoma after hepatic resection: Univariate and multivariate analysis. Hepatogastroenterology 2002, 49, 311–316. [Google Scholar] [PubMed]
- Bartsch, F.; Baumgart, J.; Hoppe-Lotichius, M.; Schmidtmann, I.; Heinrich, S.; Lang, H. Visceral infiltration of intrahepatic cholangiocarcinoma is most prognostic after curative resection-Retrospective cohort study of 102 consecutive liver resections from a single center. Int. J. Surg. 2018, 55, 193–200. [Google Scholar] [CrossRef]
- Voigt, R.M.; Forsyth, C.B.; Green, S.J.; Engen, P.A.; Keshavarzian, A. Circadian Rhythm and the Gut Microbiome. Int. Rev. Neurobiol. 2016, 131, 193–205. [Google Scholar]
- Yoon, K.; Kim, N. Roles of Sex Hormones and Gender in the Gut Microbiota. J. Neurogastroenterol. Motil. 2021, 27, 314–325. [Google Scholar] [CrossRef]
- Voreades, N.; Kozil, A.; Weir, T.L. Diet and the development of the human intestinal microbiome. Front. Microbiol. 2014, 5, 494. [Google Scholar] [CrossRef]
- Zmora, N.; Suez, J.; Elinav, E. You are what you eat: Diet, health and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef] [PubMed]
- Hasuda, H.; Ikeda, T.; Makizaki, Y.; Yokota, H.; Tanaka, Y.; Ohno, H.; Shimokawa, M.; Matsuoka, H.; Kimura, Y.; Oki, E.; et al. Alterations in the gut microbiome in patients with esophageal carcinoma in response to esophagectomy and neoadjuvant treatment. Surg. Today 2022, 53, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.S.; Koller, K.R.; Ramaboli, M.C.; Nesengani, L.T.; Ocvirk, S.; Chen, C.; Flanagan, C.A.; Sapp, F.R.; Merritt, Z.T.; Bhatti, F.; et al. Diet and the Human Gut Microbiome: An International Review. Dig. Dis. Sci. 2020, 65, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, stability and resilience of the human gut microbiota. Nature 2012, 489, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Tischoff, I.; Tannapfel, A. Hepatozelluläres Karzinom und Cholangiokarzinom-Unterschiedliche Prognose, Pathogenese und Therapie. Zentralbl. Chir. 2007, 132, 300–305. [Google Scholar] [CrossRef]
- Mejia, J.C.; Pasko, J. Primary Liver Cancers. Surg. Clin. N. Am. 2020, 100, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Kohnert, E.; Kreutz, C.; Binder, N.; Hannibal, L.; Gorkiewicz, G.; Müller, A.; Storz, M.A.; Huber, R.; Lederer, A.-K. Changes in Gut Microbiota after a Four-Week Intervention with Vegan vs. Meat-Rich Diets in Healthy Participants: A Randomized Controlled Trial. Microorganisms 2021, 9, 727. [Google Scholar] [CrossRef]
- Ding, T.; Schloss, P.D. Dynamics and associations of microbial community types across the human body. Nature 2014, 509, 357–360. [Google Scholar] [CrossRef]
- Ohtani, N.; Hara, E. Gut-liver axis-mediated mechanism of liver cancer: A special focus on the role of gut microbiota. Cancer Sci. 2021, 112, 4433–4443. [Google Scholar] [CrossRef]
- Chu, H.; Duan, Y.; Yang, L.; Schnabl, B. Small metabolites, possible big changes: A microbiota-centered view of non-alcoholic fatty liver disease. Gut 2019, 68, 359–370. [Google Scholar] [CrossRef]
- Lederer, A.-K.; Chikhladze, S.; Kohnert, E.; Huber, R.; Müller, A. Current Insights: The Impact of Gut Microbiota on Postoperative Complications in Visceral Surgery—A Narrative Review. Diagnostics 2021, 11, 2099. [Google Scholar] [CrossRef]
- Ferreira-Halder, C.V.; de Sousa Faria, A.V.; Andrade, S.S. Action and function of Faecalibacterium prausnitzii in health and disease. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.B.; Yassour, M.; Sauk, J.; Garner, A.; Jiang, X.; Arthur, T.; Lagoudas, G.K.; Vatanen, T.; Fornelos, N.; Wilson, R.; et al. A novel Ruminococcus gnavus clade enriched in inflammatory bowel disease patients. Genome Med. 2017, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Asnicar, F.; Berry, S.E.; Valdes, A.M.; Nguyen, L.H.; Piccinno, G.; Drew, D.A.; Leeming, E.; Gibson, R.; Le Roy, C.; Al Khatib, H.; et al. Microbiome connections with host metabolism and habitual diet from 1,098 deeply phenotyped individuals. Nat. Med. 2021, 27, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Huang, C.; Ning, Z.; Zhang, Y.; Zhuang, M.; Yang, W.; Wang, X.; Wang, J.; Zhang, L.; Xiao, H.; et al. Ruminococcus gnavus plays a pathogenic role in diarrhea-predominant irritable bowel syndrome by increasing serotonin biosynthesis. Cell Host Microbe 2023, 31, 33–44.e5. [Google Scholar] [CrossRef] [PubMed]
- Baxter, N.T.; Schmidt, A.W.; Venkataraman, A.; Kim, K.S.; Waldron, C.; Schmidt, T.M. Dynamics of Human Gut Microbiota and Short-Chain Fatty Acids in Response to Dietary Interventions with Three Fermentable Fibers. MBio 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Ubachs, J.; Ziemons, J.; Soons, Z.; Aarnoutse, R.; Dijk, D.P.J.; Penders, J.; Helvoort, A.; Smidt, M.L.; Kruitwagen, R.F.P.M.; Baade-Corpelijn, L.; et al. Gut microbiota and short-chain fatty acid alterations in cachectic cancer patients. J. Cachexia Sarcopenia Muscle 2021, 12, 2007–2021. [Google Scholar] [CrossRef]
- Duan, M.; Wang, Y.; Zhang, Q.; Zou, R.; Guo, M.; Zheng, H. Characteristics of gut microbiota in people with obesity. PLoS ONE 2021, 16, e0255446. [Google Scholar] [CrossRef]
- Feng, J.; Zhao, F.; Sun, J.; Lin, B.; Zhao, L.; Liu, Y.; Jin, Y.; Li, S.; Li, A.; Wei, Y. Alterations in the gut microbiota and metabolite profiles of thyroid carcinoma patients. Int. J. Cancer 2019, 144, 2728–2745. [Google Scholar] [CrossRef]
- Vissenaekens, H.; Criel, H.; Grootaert, C.; Raes, K.; Smagghe, G.; Van Camp, J. Flavonoids and cellular stress: A complex interplay affecting human health. Crit. Rev. Food Sci. Nutr. 2022, 62, 8535–8566. [Google Scholar] [CrossRef]
- Lewis, E.R.G.; Torres, A.G. The art of persistence—The secrets to Burkholderia chronic infections. Pathog. Dis. 2016, 74, ftw070. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, W.; Huang, X.; Feng, Y.; Lu, J.; Gao, F. Intestinal flora differences between patients with ulcerative colitis of different ethnic groups in China. Medicine 2021, 100, e26932. [Google Scholar] [CrossRef] [PubMed]
- Könönen, E.; Wade, W.G. Actinomyces and related organisms in human infections. Clin. Microbiol. Rev. 2015, 28, 419–442. [Google Scholar] [CrossRef] [PubMed]
- Takiguchi, Y.; Nagayoshi, M.; Matsuura, Y.; Yokota, S.; Kajiwara, Y.; Akiba, Y. Thoracic empyema caused by Alloscardovia omnicolens and Bifidobacterium dentium. J. Infect. Chemother. 2022, 28, 1567–1570. [Google Scholar] [CrossRef] [PubMed]
- Slattery, C.; Cotter, P.D.; O’Toole, P.W. Analysis of Health Benefits Conferred by Lactobacillus Species from Kefir. Nutrients 2019, 11, 1252. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, J.; O’Toole, P.W. Lactobacillus: Host-microbe relationships. Curr. Top. Microbiol. Immunol. 2013, 358, 119–154. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhao, Q.; Li, T.; Lu, L.; Wang, F.; Zhang, H.; Liu, Z.; Ma, H.; Zhu, Q.; Wang, J.; et al. Lactobacillus plantarum-derived indole-3-lactic acid ameliorates colorectal tumorigenesis via epigenetic regulation of CD8+ T cell immunity. Cell Metab. 2023, 35, 943–960.e9. [Google Scholar] [CrossRef]
- Yu, J.S.; Youn, G.S.; Choi, J.; Kim, C.; Kim, B.Y.; Yang, S.; Lee, J.H.; Park, T.; Kim, B.K.; Kim, Y.B.; et al. Lactobacillus lactis and Pediococcus pentosaceus -driven reprogramming of gut microbiome and metabolome ameliorates the progression of non-alcoholic fatty liver disease. Clin. Transl. Med. 2021, 11, e634. [Google Scholar] [CrossRef]
- Wexler, H.M. Bacteroides: The Good, the Bad, and the Nitty-Gritty. Clin. Microbiol. Rev. 2007, 20, 593–621. [Google Scholar] [CrossRef]
- Zafar, H.; Saier, M.H. Gut Bacteroides species in health and disease. Gut Microbes 2021, 13, 1848158. [Google Scholar] [CrossRef]
- Wang, C.; Zhao, J.; Zhang, H.; Lee, Y.-K.; Zhai, Q.; Chen, W. Roles of intestinal bacteroides in human health and diseases. Crit. Rev. Food Sci. Nutr. 2021, 61, 3518–3536. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2013, 505, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Wang, F.; Yuan, J.; Li, J.; Jiang, D.; Zhang, J.; Li, H.; Wang, R.; Tang, J.; Huang, T.; et al. Effects of dietary fat on gut microbiota and faecal metabolites, and their relationship with cardiometabolic risk factors: A 6-month randomised controlled-feeding trial. Gut 2019, 68, 1417–1429. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wu, J.; Li, J.V.; Zhou, N.-Y.; Tang, H.; Wang, Y. Gut Microbiota Composition Modifies Fecal Metabolic Profiles in Mice. J. Proteome Res. 2013, 12, 2987–2999. [Google Scholar] [CrossRef] [PubMed]
- Bartolini, I.; Risaliti, M.; Ringressi, M.N.; Melli, F.; Nannini, G.; Amedei, A.; Muiesan, P.; Taddei, A. Role of gut microbiota-immunity axis in patients undergoing surgery for colorectal cancer: Focus on short and long-term outcomes. World J. Gastroenterol. 2020, 26, 2498–2513. [Google Scholar] [CrossRef] [PubMed]
- Mármol, I.; Sánchez-de-Diego, C.; Pradilla Dieste, A.; Cerrada, E.; Rodriguez Yoldi, M. Colorectal Carcinoma: A General Overview and Future Perspectives in Colorectal Cancer. Int. J. Mol. Sci. 2017, 18, 197. [Google Scholar] [CrossRef] [PubMed]
- Doocey, C.M.; Finn, K.; Murphy, C.; Guinane, C.M. The impact of the human microbiome in tumorigenesis, cancer progression, and biotherapeutic development. BMC Microbiol. 2022, 22, 53. [Google Scholar] [CrossRef] [PubMed]
- Parker, B.J.; Wearsch, P.A.; Veloo, A.C.M.; Rodriguez-Palacios, A. The Genus Alistipes: Gut Bacteria with Emerging Implications to Inflammation, Cancer, and Mental Health. Front. Immunol. 2020, 11, 906. [Google Scholar] [CrossRef]
- Prochazkova, P.; Roubalova, R.; Dvorak, J.; Kreisinger, J.; Hill, M.; Tlaskalova-Hogenova, H.; Tomasova, P.; Pelantova, H.; Cermakova, M.; Kuzma, M.; et al. The intestinal microbiota and metabolites in patients with anorexia nervosa. Gut Microbes 2021, 13, 1902771. [Google Scholar] [CrossRef]
- Pinquart, M.; Duberstein, P.R. Depression and cancer mortality: A meta-analysis. Psychol. Med. 2010, 40, 1797–1810. [Google Scholar] [CrossRef]
- Yuan, J.; Chen, C.; Cui, J.; Lu, J.; Yan, C.; Wei, X.; Zhao, X.; Li, N.; Li, S.; Xue, G.; et al. Fatty Liver Disease Caused by High-Alcohol-Producing Klebsiella pneumoniae. Cell Metab. 2019, 30, 675–688.e7. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference and Author | Year | Country | Type of Study | N | Groups | Excluded |
|---|---|---|---|---|---|---|
| [43] Nagaraja et al. | 2014 | Australia | systematic review | 255/861 | Salmonella typhi carrier/non-carrier | n. s. |
| [44] Koshiol et al. | 2016 | Chile | case–control | 13/9/13 | gallbladder cancer/cholelithiasis/healthy | n. s. |
| [48] Jia/Lu/Zeng et al. | 2019 | China | case–control | 28/28/16/12 | iCCA/HCC/cirrhosis/healthy | metastatic CCA, mixed-type CCA |
| [49] Zhang et al. | 2021 | China | case–control | 53/47/40 | aCCA/cholelithiasis/healthy | other gastrointestinal or oncological diseases |
| [47] Deng/Li et al. | 2022 | China | case–control | 46/143/40 | aCCA/HCC/healthy | other gastrointestinal or oncological diseases, age > 80 years |
| [50] Ito et al. | 2022 | Japan | case–control | 30/11/10 | aCCA/BBD */healthy | cholangitis, severe medical comorbidities, previous treatment + |
| [46] Ma et al. | 2023 | China | case–control | 63/184/40 | iCCA/HCC/healthy | other gastrointestinal or oncological diseases |
| [45] Miyabe et al. | 2023 | USA | case–control | 11/16/31 | pCCA #/PSC+CCA/PSC | unsuccessful cannulation of bile duct, no bile duct sample, abnormal postsurgical anatomy |
| [51] Zhang et al. | 2023 | China | case–control | 23/17 | iCCA/healthy | mixed-type CCA, infectious diseases, other gastrointestinal, autoimmune or oncological diseases |
| Ref. | Method | Time Point | Antibiotics or Probiotics | α-Diversity * | Abundance * |
|---|---|---|---|---|---|
| [43] | cultivation | n. s. | n. s. | n. s. | Salmonella typhi carrier status was associated with gallbladder carcinoma |
| [44] | cultivation | n. s. | n. s. | n. s. | no detection of Salmonella spp. (neither in gallbladder cancer patients nor in controls) |
| [48] | 16s RNA (V4) | n. s. | recently none | ↑ | ↑ family Peptostreptococcaceae ↑ genera Actinomyces, Lactobacillus, Alloscardovia |
| [49] | 16s rDNA (V3-V4) | before treatment | none for at least 2 months | no difference | ↑ family Muribaculaceae ↑ genera Bacteroides, Muribaculum, Alistipes ↓ genera Burkholderia, Caballeronia, Paraburkholderia, Faecalibacterium, Ruminococcus (suggested biomarkers for differentiation between CCA patients and healthy controls) |
| [47] | 16s rRNA (V3-V4) | n. s. | none for at least 8 weeks | no difference | ↑ phylum Bacteroidota, family Muribaculaceae ↑ genera Bacteroides, Shigella, Klebsiella, unclassified Lachnospiraceae NK4A136 group ↓ phylum Bacillota, genus Megamonas |
| [50] | 16s rRNA (V3-V4) | before treatment | none for at least 8 weeks | no difference | ↑ class Gammaproteobacteria (main family Enterobacteriaceae) ↓ class Clostridia (main family Lachnospiracea) genera Faecalibacterium and Coprococcus enriched in healthy controls |
| [46] | 16s rRNA (V3-V4) | before treatment | none for at least 2 months | ↓ | ↓ phylum Bacteroidota, family Porphyromonadaceae |
| [45] | 16S rRNA (n. s.) | Mixed | different antibiotics | n. s. + | n. s. + |
| [51] | ITS2 rDNA | before treatment | none for at least 3 months | ↓ | ↑ phylum Ascomycota, genus Candida (main species Candida albicans), genus Monographella (main species Monographella nivalis) ↓ phylum Mucoromycota, phylum Basidiomycota, genera Saccharomyces (main species Saccharomyces cerevisiae), Pichia (main species Pichia mandshurica), Mucor (main species Mucor circinelloides), Staphylotricum (main species Staphylotricum coccospurum), Actinomucor (main species Actinomucor elegans), Alternaria (main species Alternaria alternata), Fusarium (main species Fusarium oxysporum), Humicola (main species Humicola fuscoatra) |
| Reference and Author | Year | Country | Type of Study | n | Groups | Excluded |
|---|---|---|---|---|---|---|
| [52] Mao/Wang/Long/Yang et al. | 2021 | China | cohort | 30/35 | advanced HCC/BTC + | n. s. |
| [53] Jin et al. | 2023 | China | Phase II clinical trial | 11 * | local advanced aCCA (clinical stage IV) | age < 75 years, cardiac or autoimmune disease, immunosuppressive treatment |
| Ref. | Treatment | Method | Time Point | Antibiotics or Probiotics | α-Diversity * | Abundance * |
|---|---|---|---|---|---|---|
| [52] | anti-PD-1 based systemic therapy | sequencing, n. s. | after failure of first-line therapy | none for at least 3 months | n. s. | ↑ class Negativicutes, order Enterobacterales, order Veillonellales, family Veillonellaceae ↓ phylum Bacteroidota, order Bacteroidales |
| [53] | sintilimab plus anlotinib | 16s rRNA (V3-V4) | after failure of first-line therapy | n. s. | n. s. | ↑ phylum Pseudomonadota suggested species for response: Serratia Marcescens and Raoultella Planticola |
| Reference & Author | Year | Country | Type of Study | n | Groups | Excluded |
|---|---|---|---|---|---|---|
| [55] Caygill et al. | 1994 | UK | case–control | 83/386 | Salmonella carrier/non-carrier | subjects with ongoing infection |
| [48] Jia/Lu/Zeng et al. | 2019 | China | case–control | 28/28/16/12 | iCCA/HCC/cirrhosis/healthy | metastatic CCA, mixed-type CCA |
| [54] Zhang et al. | 2021 | USA | experimental (including mice) | n. s. | BDL mice/DSS-colitis mice/germ-free mice | - |
| [52] Mao/Wang/Long/Yang et al. | 2021 | China | cohort | 30/35 | advanced HCC/BTC + | n. s. |
| [51] Zhang et al. | 2023 | China | case–control | 23/17 | iCCA/healthy | mixed-type CCA, infectious diseases, other gastrointestinal, autoimmune or oncological diseases |
| Ref. | Method | Time Point | Antibiotics or Probiotics | Results |
|---|---|---|---|---|
| [55] | cultivation | - | n. s. | carriers of Salmonella typhi and Salmonella paratyphi had a large excess of cancer mortality, particularly of gallbladder carcinoma (compared to non-carriers) |
| [48] | 16s RNA (V4) | n. s. | recently none | in case of venous infiltration ↑ family Oscillospiraceae and ↓ family Eubacteriaceae, genera Allobaculum, Pediococcus, Pseudoramibacter, Peptostreptococcus |
| [54] | 16s RNA (V4) | - | none | treatment with neomycin for elimination of Gram-negative bacteria resulted in fewer CCA, after dysbiotic fecal microbial transplantation germ-free mice developed liver myeloid cell accumulation, which is associated with worse outcome of CCA |
| [52] | sequencing, n. s. | n. s. | none for at least 3 months | ↑ species Lachnospiraceae bacterium-GAM79, Erysipelotrichaceae bacterium-GAM147, Ruminococcus callidus, Alistipes megaguti and Bacteroides zoogleoformans => longer PFS and OS; ↑ family Veillonellaceae => shorter PFS and OS In biliary tract cancer patients: ↑ order Bacteroidales => longer PFS and OS, ↑ family Veillonellaceae = shorter PFS and OS |
| [51] | ITS2 rDNA | before treatment | none for at least 3 months | ↑ Candida spp. (main species Candida albicans), Dipodascus spp., family Ustilaginaceae, family Clavulinaceae, and Bipolaris spp. CCA patients with stage III–IV compared to those with stage I–II; ↑ class Sordariomycetes, order Xylariales, family Hyponectriaceae, Monographella spp., Annulohypoxylon spp., increased in CCA patients with stage I–II compared to stage III–IV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lederer, A.-K.; Rasel, H.; Kohnert, E.; Kreutz, C.; Huber, R.; Badr, M.T.; Dellweg, P.K.E.; Bartsch, F.; Lang, H. Gut Microbiota in Diagnosis, Therapy and Prognosis of Cholangiocarcinoma and Gallbladder Carcinoma—A Scoping Review. Microorganisms 2023, 11, 2363. https://doi.org/10.3390/microorganisms11092363
Lederer A-K, Rasel H, Kohnert E, Kreutz C, Huber R, Badr MT, Dellweg PKE, Bartsch F, Lang H. Gut Microbiota in Diagnosis, Therapy and Prognosis of Cholangiocarcinoma and Gallbladder Carcinoma—A Scoping Review. Microorganisms. 2023; 11(9):2363. https://doi.org/10.3390/microorganisms11092363
Chicago/Turabian StyleLederer, Ann-Kathrin, Hannah Rasel, Eva Kohnert, Clemens Kreutz, Roman Huber, Mohamed Tarek Badr, Patricia K. E. Dellweg, Fabian Bartsch, and Hauke Lang. 2023. "Gut Microbiota in Diagnosis, Therapy and Prognosis of Cholangiocarcinoma and Gallbladder Carcinoma—A Scoping Review" Microorganisms 11, no. 9: 2363. https://doi.org/10.3390/microorganisms11092363
APA StyleLederer, A.-K., Rasel, H., Kohnert, E., Kreutz, C., Huber, R., Badr, M. T., Dellweg, P. K. E., Bartsch, F., & Lang, H. (2023). Gut Microbiota in Diagnosis, Therapy and Prognosis of Cholangiocarcinoma and Gallbladder Carcinoma—A Scoping Review. Microorganisms, 11(9), 2363. https://doi.org/10.3390/microorganisms11092363