
Quantification of HPV16 E7 Oncoproteins in Urine Specimens from Women with Cervical Intraepithelial Neoplasia

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Specimens and Ethics
2.2. Ultrasensitive ELISA with Thio-NAD Cycling
2.3. Spike-and-Recovery Test
- (1)
- 50 μL TBS with 0.1% BSA or 50 μL ThinPrep solution, this was used for the blank experiment;
- (2)
- (50 − x) μL TBS with 0.1% BSA and x μL control urine (Serotec, Sapporo, Japan), this was also used for the blank experiment;
- (3)
- 50 μL E7 antigen at a concentration of 0.2 pg/50 µL or 50 μL SiHa cells at a concentration of 500 cells/50 µL, this was used for the spike-and-recovery experiment;
- (4)
- (50 − x) μL E7 antigen at a concentration of 0.2 pg/(50 − x) µL or (50 − x) μL SiHa cells at a concentration of 500 cells/(50 − x) µL, and x μL control urine, this was also used for the spike-and-recovery experiment.
2.4. Determination of the ELISA Index
2.5. Uniplex E6/E7 PCR
2.6. Statistical Analysis
3. Results
3.1. LOD and LOQ for the Measurement of HPV16 E7 Oncoproteins in a Buffer
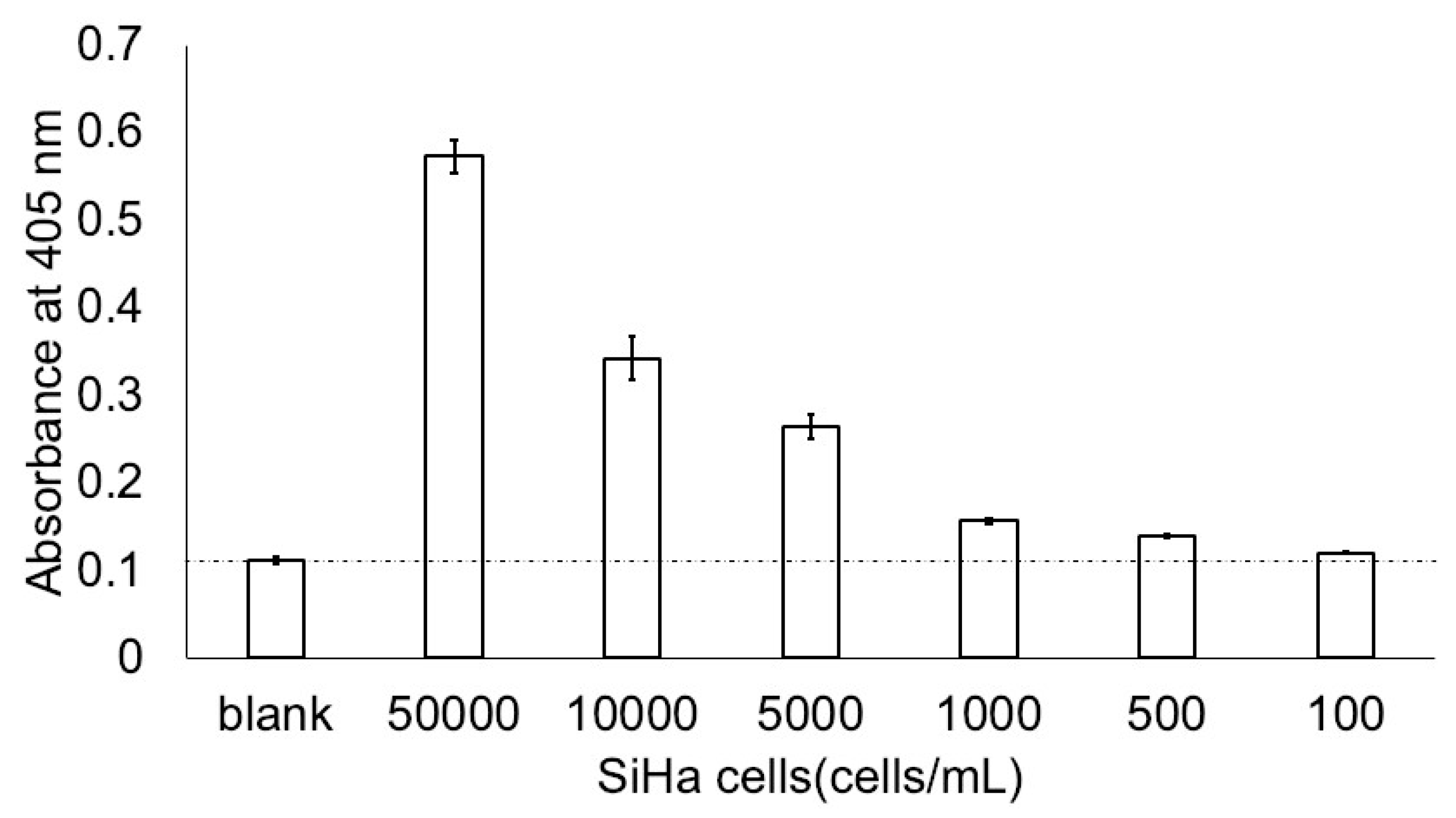
3.2. Minimum Detection of SiHa Cells in ThinPrep Solution
3.3. Effects of Urine on Ultrasensitive ELISA Measurements of E7 Oncoproteins and SiHa Cells
3.4. Determination of ELISA Index to Indicate Cutoff Value for the Presence of E7 Oncoproteins
3.5. Detection of E7 Oncoproteins in Urine Specimens Collected from Women with HPV16 DNA-Positive CIN Lesions
3.6. Effects of Blood and Skin Cells on Measurements of E7 Oncoprotein by Our Ultrasensitive ELISA
3.7. Relationship between the ELISA Index and CIN Grade
3.8. Specific Detection of E7 Oncoproteins in HPV16 and Its Related Types but Not HPV18-Positive Cells
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Cervical Cancer. Available online: https://www.who.int/health-topics/cervical-cancer#tab=tab_1 (accessed on 13 June 2024).
- WHO. Cervical Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer#:~:text=Persistent%20infection%20with%20high-risk,causes%2095%25%20of%20cervical%20cancers (accessed on 13 June 2024).
- Magdi, R.; Elshafeey, F.; Elshebiny, M.; Kamel, M.; Abuelnaga, Y.; Ghonim, M.; Nabhan, A.; ECEBM Working Group. A systematic review and meta-analysis of diagnostic accuracy of HPV tests for the screening of cervical cancer in low-resource settings. Int. J. Gynaecol. Obstet. 2021, 152, 12–18. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Recommends DNA Testing as a First-Choice Screening Method for Cervical Cancer Prevention. 2021. Available online: https://www.who.int/europe/news/item/11-09-2021-who-recommends-dna-testing-as-a-first-choice-screening-method-for-cervical-cancer-prevention (accessed on 13 June 2024).
- Lie, A.K.; Risberg, B.; Borge, B.; Sandstad, B.; Delabie, J.; Rimala, R.; Onsrud, M.; Thoresen, S. DNA- versus RNA-based methods for human papillomavirus detection in cervical neoplasia. Gynecol. Oncol. 2005, 97, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Duvlis, S.; Popovska-Jankovic, K.; Arsova, Z.S.; Memeti, S.; Popeska, Z.; Plaseska-Karanfilska, D. HPV E6/E7 mRNA versus HPV DNA biomarker in cervical cancer screening of a group of Macedonian women. J. Med. Virol. 2015, 87, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, K.S.; Whitley, M.J.; Cubie, H.A. Human papillomavirus type specific DNA and RNA persistence—Implications for cervical disease progression and monitoring. J. Med. Virol. 2004, 73, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Molden, T.; Kraus, I.; Karlsen, F.; Skomedal, H.; Nygård, J.F.; Hagmar, B. Comparison of human papillomavirus messenger RNA and DNA detection: A cross-sectional study of 4136 women >30 years of age with a 2-year follow-up of high-grade squamous intraepithelial lesion. Cancer Epidemiol. Biomark. Prev. 2005, 14, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Molden, T.; Nygård, J.F.; Kraus, I.; Karlsen, F.; Nygård, M.; Skare, G.B.; Skomedal, H.; Thoresen, S.O.; Hagmar, B. Predicting CIN2+ when detecting HPV mRNA and DNA by PreTect HPV-proofer and consensus PCR: A 2-year follow-up of women with ASCUS or LSIL Pap smear. Int. J. Cancer 2005, 114, 973–976. [Google Scholar] [CrossRef] [PubMed]
- Molden, T.; Kraus, I.; Karlsen, F.; Skomedal, H.; Hagmar, B. Human papillomavirus E6/E7 mRNA expression in women younger than 30 years of age. Gynecol. Oncol. 2006, 100, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Hammer, A.; Blaakaer, J.; de Koning, M.N.C.; Steiniche, T.; Mejlgaard, E.; Svanholm, H.; Roensbo, M.T.; Fuglsang, K.; Doorbar, J.; Andersen, R.H.; et al. Evidence of latent HPV infection in older Danish women with a previous history of cervical dysplasia. Acta Obstet. Gynecol. Scand. 2022, 101, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, M.; Giubbi, C.; Sechi, I.; Bottari, F.; Iacobone, A.D.; Musumeci, R.; Perdoni, F.; Muresu, N.; Piana, A.; Fruscio, R.; et al. Evaluation of BD Onclarity™ HPV assay on self-collected vaginal and first-void urine samples as compared to clinician-collected cervical samples: A pilot study. Diagnostics 2022, 12, 3075. [Google Scholar] [CrossRef]
- Martinelli, M.; Latsuzbaia, A.; Bonde, J.; Pedersen, H.; Iacobone, A.D.; Bottari, F.; Piana, A.F.; Pietri, R.; Cocuzza, C.E.; Arbyn, M.; et al. Performance of BD Onclarity HPV assay on FLOQSwabs vaginal self-samples. Microbiol. Spectr. 2024, 12, e0287223. [Google Scholar] [CrossRef] [PubMed]
- Daponte, A.; Michail, G.; Daponte, A.I.; Daponte, N.; Valasoulis, G. Urine HPV in the context of genital and cervical cancer screening—An update of current literature. Cancers 2021, 13, 1640. [Google Scholar] [CrossRef] [PubMed]
- Watabe, S.; Kodama, H.; Kaneda, M.; Morikawa, M.; Nakaishi, K.; Yoshimura, T.; Iwai, A.; Miura, T.; Ito, E. Ultrasensitive enzyme-linked immunosorbent assay (ELISA) of proteins by combination with the thio-NAD cycling method. Biophysics 2014, 10, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, J.; Saito, M.; Zhang, S.; Takakura, M.; Takagi, H.; Sasagawa, T. Determination of human papillomavirus type in archival tissue specimens of invasive cervical cancer using molecular mapping and E6/E7-based polymerase chain reaction. PLoS ONE 2022, 17, e0265996. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J.; Bergeron, C.; von Knebel Doeberitz, M.; Gravitt, P.; Jeronimo, J.; Lorincz, A.T.; Meijer, C.J.L.M.; Sankaranarayanan, R.; Snijders, P.J.F.; Szarewski, A. New technologies and procedures for cervical cancer screening. Vaccine 2012, 30 (Suppl. S5), F107–F116. [Google Scholar] [CrossRef] [PubMed]
- Yim, E.K.; Park, J.S. The role of HPV E6 and E7 oncoproteins in HPV-associated cervical carcinogenesis. Cancer Res. Treat. 2005, 37, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Piña, D.A.; Pedroza-Saavedra, A.; Cruz-Valdez, A.; Ortiz-Panozo, E.; Maldonado-Gama, M.; Chihu-Amparan, L.; Rodriguez-Ocampo, A.N.; Orozco-Fararoni, E.; Esquivel-Guadarrama, F.; Gutierrez-Xicotencatl, L. Validation of serological antibody profiles against human papillomavirus type 16 antigens as markers for early detection of cervical cancer. Medicine 2016, 95, e2769. [Google Scholar] [CrossRef] [PubMed]
- Estêvão, D.; Costa, N.R.; Gil da Costa, R.M.; Medeiros, R. Hallmarks of HPV carcinogenesis: The role of E6, E7 and E5 oncoproteins in cellular malignancy. Biochim. Biophys. Acta Gene Regul. Mech. 2019, 1862, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Halbert, C.L.; Demers, G.W.; Galloway, D.A. The E7 gene of human papillomavirus type 16 is sufficient for immortalization of human epithelial cells. J. Virol. 1991, 65, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.R.; Duensing, S.; Brake, T.; Münger, K.; Lambert, P.F.; Arbeit, J.M. Dissection of human papillomavirus E6 and E7 function in transgenic mouse models of cervical carcinogenesis. Cancer Res. 2003, 63, 4862–4871. [Google Scholar] [PubMed]
- Nogueira, M.O.; Hošek, T.; Calçada, E.O.; Castiglia, F.; Massimi, P.; Banks, L.; Felli, I.C.; Pierattelli, R. Monitoring HPV-16 E7 phosphorylation events. Virology 2017, 503, 70–75. [Google Scholar] [CrossRef]
- Sasagawa, T.; Basha, W.; Yamazaki, H.; Inoue, M. High-risk and multiple human papillomavirus infections associated with cervical abnormalities in Japanese women. Cancer Epidemiol. Biomark. Prev. 2001, 10, 45–52. [Google Scholar]
- Kyosei, Y.; Yoshimura, T.; Ito, E. Removal of soluble ACE2 in VeroE6 cells by 17β-estradiol reduces SARS-CoV-2 infectivity. Biol. Pharm. Bull. 2023, 46, 1842–1845. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.K.; Chang, J.H.; Ke, L.Y.; Kao, J.K.; Chen, C.H.; Yang, R.C.; Yoshimura, T.; Ito, E.; Tsai, J.J. Advanced detection method for dengue NS1 protein using ultrasensitive ELISA with thio-NAD cycling. Viruses 2023, 15, 1894. [Google Scholar] [CrossRef] [PubMed]
- Hoppe-Seyler, K.; Honegger, A.; Bossler, F.; Sponagel, J.; Bulkescher, J.; Lohrey, C.; Hoppe-Seyler, F. Viral E6/E7 oncogene and cellular hexokinase 2 expression in HPV-positive cancer cell lines. Oncotarget 2017, 8, 106342–106351. [Google Scholar] [CrossRef] [PubMed]
- Okodo, M.; Okayama, K.; Teruya, K.; Sasagawa, T. Uniplex E6/E7 PCR method detecting E6 or E7 genes in 39 human papillomavirus types. J. Med. Virol. 2018, 90, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Gooding, J.J. What does ultrasensitive really mean? ACS Sens. 2019, 4, 528. [Google Scholar] [CrossRef] [PubMed]
- Derbie, A.; Mekonnen, D.; Woldeamanuel, Y.; Van Ostade, X.; Abebe, T. HPV E6/E7 mRNA test for the detection of high grade cervical intraepithelial neoplasia (CIN2+): A systematic review. Infect. Agents Cancer 2020, 15, 9. [Google Scholar] [CrossRef] [PubMed]
- Burger, E.A.; Kornør, H.; Klemp, M.; Lauvrak, V.; Kristiansen, I.S. HPV mRNA tests for the detection of cervical intraepithelial neoplasia: A systematic review. Gynecol. Oncol. 2011, 120, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Broccolo, F.; Fusetti, L.; Rosini, S.; Caraceni, D.; Zappacosta, R.; Ciccocioppo, L.; Matteoli, B.; Halfon, P.; Malnati, M.S.; Ceccherini-Nelli, L. Comparison of oncogenic HPV type-specific viral DNA load and E6/E7 mRNA detection in cervical samples: Results from a multicenter study. J. Med. Virol. 2012, 84, 1968–1974. [Google Scholar] [CrossRef]
- Kitamura, K.; Nimura, K.; Ito, R.; Saga, K.; Inohara, H.; Kaneda, Y. Evaluation of HPV16 E7 expression in head and neck carcinoma cell lines and clinical specimens. Sci. Rep. 2020, 10, 22138. [Google Scholar] [CrossRef]
- Zheng, Y.; Li, X.; Jiao, Y.; Wu, C. High-risk human papillomavirus oncogenic E6/E7 mRNAs splicing regulation. Front. Cell. Infect. Microbiol. 2022, 12, 929666. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.V. The human papillomavirus replication cycle, and its links to cancer progression: A comprehensive review. Clin. Sci. 2017, 131, 2201–2221. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, M.; Stites, D.P.; Patel, S.; Farhat, S.; Scott, M.; Hills, N.K.; Palefsky, J.M.; Moscicki, A.B. Persistence of human papillomavirus type 16 infection is associated with lack of cytotoxic T lymphocyte response to the E6 antigens. J. Infect. Dis. 2000, 182, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Sasagawa, T.; Inoue, M.; Tanizawa, O.; Yutsudo, M.; Hakura, A. Identification of antibodies against human papillomavirus type 16 E6 and E7 proteins in sera of patients with cervical neoplasias. Jpn. J. Cancer Res. 1992, 83, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, D.; Wichmann, G.; Baboci, L.; Michel, A.; Höfler, D.; Wiesenfarth, M.; Schroeder, L.; Boscolo-Rizzo, P.; Herold-Mende, C.; Dyckhoff, G.; et al. Sensitivity and specificity of antibodies against HPV16 E6 and other early proteins for the detection of HPV16-driven oropharyngeal squamous cell carcinoma. Int. J. Cancer 2017, 140, 2748–2757. [Google Scholar] [CrossRef] [PubMed]
- Maglennon, G.A.; McIntosh, P.B.; Doorbar, J. Immunosuppression facilitates the reactivation of latent papillomavirus infections. J. Virol. 2014, 88, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Maglennon, G.A.; McIntosh, P.; Doorbar, J. Persistence of viral DNA in the epithelial basal layer suggests a model for papillomavirus latency following immune regression. Virology 2011, 414, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Della Fera, A.N.; Warburton, A.; Coursey, T.L.; Khurana, S.; McBride, A.A. Persistent human papillomavirus infection. Viruses 2021, 13, 321. [Google Scholar] [CrossRef] [PubMed]
- Poljak, M.; Oštrbenk Valenčak, A.; Cuschieri, K.; Bohinc, K.B.; Arbyn, M. 2023 global inventory of commercial molecular tests for human papillomaviruses (HPV). J. Clin. Virol. 2024, 172, 105671. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, J.A.; Rahmani, M.Z.; Jones, W.E.; Chaturvedi, A.K.; Hagensee, M.E. Optimization of PCR based detection of human papillomavirus DNA from urine specimens. J. Clin. Virol. 2004, 29, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Prusty, B.K.; Kumar, A.; Arora, R.; Batra, S.; Das, B.C. Human papillomavirus (HPV) DNA detection in self-collected urine. Int. J. Gynaecol. Obstet 2005, 90, 223–227. [Google Scholar] [CrossRef] [PubMed]
- MacLaughlin, K.L.; Jacobson, R.M.; Radecki Breitkopf, C.; Wilson, P.M.; Jacobson, D.J.; Fan, C.; St Sauver, J.L.; Rutten, L.J.F. Trends over time in pap and pap-HPV cotesting for cervical cancer screening. J. Womens Health 2019, 28, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Neilson, A.; Jones, R.K. Women’s lay knowledge of cervical cancer/cervical screening: Accounting for non-attendance at cervical screening clinics. J. Adv. Nurs. 1998, 28, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Breithaupt, L.; Des Marais, A.; Rastas, C.; Richman, A.; Barclay, L.; Brewer, N.T.; Smith, J.S. Acceptability and ease of use of mailed HPV self-collection among infrequently screened women in North Carolina. Sex. Transm. Infect. 2018, 94, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Vega Crespo, B.; Neira, V.A.; Ortíz, S.J.; Maldonado-Rengel, R.; López, D.; Gómez, A.; Vicuña, M.J.; Mejía, J.; Benoy, I.; Carreño, T.P.; et al. Evaluation of urine and vaginal self-sampling versus clinician-based sampling for cervical cancer screening: A field comparison of the acceptability of three sampling tests in a rural community of Cuenca, Ecuador. Healthcare 2022, 10, 1614. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blank | Specimen | |||
|---|---|---|---|---|
| Solution | (1) | (2) | (3) | (4) |
| TBS including 0.1% BSA or ThinPrep (μL/well) | 50 | 50 − x | 50 | 50 − x |
| control urine (μL/well) | 0 | X | 0 | X |
| E7 antigen (0.2 pg/mL) or SiHa cells (500 cells/well) | – | – | + | + |
| Dilution Rate of Urine (%) | Spike-and-Recovery Rate (%) |
|---|---|
| 50 | 98 |
| 100 | 91 |
| 200 | 94 |
| Dilution Rate of Urine (%) | Spike-and-Recovery Rate (%) |
|---|---|
| 50 | 89 |
| 100 | 91 |
| 200 | 108 |
| CIN1 | CIN2 | CIN3 | Sum | ||
|---|---|---|---|---|---|
| Uniplex E6/E7 PCR | Positive | 5 (42%) | 7 (47%) | 8 (44%) | 20 (44%) |
| Negative | 7 (58%) | 8 (53%) | 10 (56%) | 25 (56%) | |
| Sum | 12 | 15 | 18 | 45 |
| Dilution Time of Control Serum | Spike-and-Recovery Rate (%) |
|---|---|
| 500,000 | 73 |
| 100,000 | 61 |
| 50,000 | 56 |
| 10,000 | 28 |
| 1000 | 9 |
| HSC-1 (Cells/mL) | Spike-and-Recovery Rate (%) |
|---|---|
| 1000 | 80 |
| 5000 | 55 |
| 10,000 | 35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makioka, D.; Inada, M.; Awano, M.; Saito, E.; Shinoda, T.; Abe, S.; Yoshimura, T.; Müller, M.; Sasagawa, T.; Ito, E. Quantification of HPV16 E7 Oncoproteins in Urine Specimens from Women with Cervical Intraepithelial Neoplasia. Microorganisms 2024, 12, 1205. https://doi.org/10.3390/microorganisms12061205
Makioka D, Inada M, Awano M, Saito E, Shinoda T, Abe S, Yoshimura T, Müller M, Sasagawa T, Ito E. Quantification of HPV16 E7 Oncoproteins in Urine Specimens from Women with Cervical Intraepithelial Neoplasia. Microorganisms. 2024; 12(6):1205. https://doi.org/10.3390/microorganisms12061205
Chicago/Turabian StyleMakioka, Daiki, Mikio Inada, Masayuki Awano, Ema Saito, Takuya Shinoda, Satoko Abe, Teruki Yoshimura, Martin Müller, Toshiyuki Sasagawa, and Etsuro Ito. 2024. "Quantification of HPV16 E7 Oncoproteins in Urine Specimens from Women with Cervical Intraepithelial Neoplasia" Microorganisms 12, no. 6: 1205. https://doi.org/10.3390/microorganisms12061205
APA StyleMakioka, D., Inada, M., Awano, M., Saito, E., Shinoda, T., Abe, S., Yoshimura, T., Müller, M., Sasagawa, T., & Ito, E. (2024). Quantification of HPV16 E7 Oncoproteins in Urine Specimens from Women with Cervical Intraepithelial Neoplasia. Microorganisms, 12(6), 1205. https://doi.org/10.3390/microorganisms12061205