
Impact of Inflammatory Burden on Voriconazole Exposure in Oncohematological Pediatric Patients Receiving Antifungal Prophylaxis after Allogeneic HCT
 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Voriconazole Dosing Regimens, Sampling Procedure, and Definition of Optimal Exposure
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Groll, A.H.; Pana, D.; Lanternier, F.; Mesini, A.; Ammann, R.A.; Averbuch, D.; Castagnola, E.; Cesaro, S.; Engelhard, D.; Garcia-Vidal, C.; et al. 8th European Conference on Infections in Leukaemia: 2020 Guidelines for the Diagnosis, Prevention, and Treatment of Invasive Fungal Diseases in Paediatric Patients with Cancer or Post-Haematopoietic Cell Transplantation. Lancet Oncol. 2021, 22, e254–e269. [Google Scholar] [CrossRef] [PubMed]
- Lehrnbecher, T.; Fisher, B.T.; Phillips, B.; Beauchemin, M.; Carlesse, F.; Castagnola, E.; Duong, N.; Dupuis, L.L.; Fioravantti, V.; Groll, A.H.; et al. Clinical Practice Guideline for Systemic Antifungal Prophylaxis in Pediatric Patients With Cancer and Hematopoietic Stem-Cell Transplantation Recipients. J. Clin. Oncol. 2020, 38, 3205–3216. [Google Scholar] [CrossRef] [PubMed]
- Tragiannidis, A.; Dokos, C.; Lehrnbecher, T.; Groll, A.H. Antifungal Chemoprophylaxis in Children and Adolescents with Haematological Malignancies and Following Allogeneic Haematopoietic Stem Cell Transplantation: Review of the Literature and Options for Clinical Practice. Drugs 2012, 72, 685–704. [Google Scholar] [CrossRef] [PubMed]
- Arad-Cohen, N.; Rowe, J.M.; Shachor-Meyouhas, Y. Pharmacological Prophylaxis of Infection in Pediatric Acute Myeloid Leukemia Patients. Expert Opin. Pharmacother. 2020, 21, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Bury, D.; Tissing, W.J.E.; Muilwijk, E.W.; Wolfs, T.F.W.; Brüggemann, R.J. Clinical Pharmacokinetics of Triazoles in Pediatric Patients. Clin. Pharmacokinet. 2021, 60, 1103–1147. [Google Scholar] [CrossRef] [PubMed]
- Hsu, A.J.; Tamma, P.D.; Fisher, B.T. Challenges in the Treatment of Invasive Aspergillosis in Immunocompromised Children. Antimicrob. Agents Chemother. 2022, 66, e0215621. [Google Scholar] [CrossRef]
- Ashbee, H.R.; Barnes, R.A.; Johnson, E.M.; Richardson, M.D.; Gorton, R.; Hope, W.W. Therapeutic Drug Monitoring (TDM) of Antifungal Agents: Guidelines from the British Society for Medical Mycology. J. Antimicrob. Chemother. 2014, 69, 1162–1176. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, I.H.; Wolfs, T.; Jonker, M.; de Waal, M.; Egberts, T.C.G.; Ververs, T.T.; Boelens, J.J.; Bierings, M. Highly Variable Plasma Concentrations of Voriconazole in Pediatric Hematopoietic Stem Cell Transplantation Patients. Antimicrob. Agents Chemother. 2013, 57, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lai, F.; Jiang, Z.; Li, M.; Chen, Z.; Cheng, J.; Cui, H.; Wen, F. Effects of Inflammation on Voriconazole Levels: A Systematic Review. Br. J. Clin. Pharmacol. 2022, 88, 5166–5182. [Google Scholar] [CrossRef] [PubMed]
- Veringa, A.; Ter Avest, M.; Span, L.F.R.; van den Heuvel, E.R.; Touw, D.J.; Zijlstra, J.G.; Kosterink, J.G.W.; van der Werf, T.S.; Alffenaar, J.-W.C. Voriconazole Metabolism Is Influenced by Severe Inflammation: A Prospective Study. J. Antimicrob. Chemother. 2017, 72, 261–267. [Google Scholar] [CrossRef]
- Encalada Ventura, M.A.; Span, L.F.R.; van den Heuvel, E.R.; Groothuis, G.M.M.; Alffenaar, J.-W.C. Influence of Inflammation on Voriconazole Metabolism. Antimicrob. Agents Chemother. 2015, 59, 2942–2943. [Google Scholar] [CrossRef] [PubMed]
- Encalada Ventura, M.A.; van Wanrooy, M.J.P.; Span, L.F.R.; Rodgers, M.G.G.; van den Heuvel, E.R.; Uges, D.R.A.; van der Werf, T.S.; Kosterink, J.G.W.; Alffenaar, J.W.C. Longitudinal Analysis of the Effect of Inflammation on Voriconazole Trough Concentrations. Antimicrob. Agents Chemother. 2016, 60, 2727–2731. [Google Scholar] [CrossRef] [PubMed]
- Boglione-Kerrien, C.; Zerrouki, S.; Le Bot, A.; Camus, C.; Marchand, T.; Bellissant, E.; Tron, C.; Verdier, M.-C.; Gangneux, J.-P.; Lemaitre, F. Can We Predict the Influence of Inflammation on Voriconazole Exposure? An Overview. J. Antimicrob. Chemother. 2023, 78, 2630–2636. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Pea, F. The Cytokine Release Syndrome and/or the Proinflammatory Cytokines as Underlying Mechanisms of Downregulation of Drug Metabolism and Drug Transport: A Systematic Review of the Clinical Pharmacokinetics of Victim Drugs of This Drug–Disease Interaction Under Different Clinical Conditions. Clin. Pharmacokinet. 2022, 61, 1519–1544. [Google Scholar] [CrossRef] [PubMed]
- White, C.M. Inflammation Suppresses Patients’ Ability to Metabolize Cytochrome P450 Substrate Drugs. Ann. Pharmacother. 2022, 56, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Ngwa, D.N.; Pathak, A.; Agrawal, A. IL-6 Regulates Induction of C-Reactive Protein Gene Expression by Activating STAT3 Isoforms. Mol. Immunol. 2022, 146, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, P.; Coelho, L.; Dal-Pizzol, F.; Ferrer, R.; Huttner, A.; Conway Morris, A.; Nobre, V.; Ramirez, P.; Rouze, A.; Salluh, J.; et al. How to Use Biomarkers of Infection or Sepsis at the Bedside: Guide to Clinicians. Intensive Care Med. 2023, 49, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Spitzer, T.R. Engraftment Syndrome: Double-Edged Sword of Hematopoietic Cell Transplants. Bone Marrow Transplant. 2015, 50, 469–475. [Google Scholar] [CrossRef]
- Ter Avest, M.; Veringa, A.; van den Heuvel, E.R.; Kosterink, J.G.W.; Schölvinck, E.H.; Tissing, W.J.E.; Alffenaar, J.-W.C. The Effect of Inflammation on Voriconazole Trough Concentrations in Children. Br. J. Clin. Pharmacol. 2017, 83, 678–680. [Google Scholar] [CrossRef]
- Luo, X.; Li, T.; Hu, L.; Liu, S.; Zhao, H.; Zhang, J.; Feng, Y.; Huang, L. Differential Effects of C-Reactive Protein Levels on Voriconazole Metabolism at Three Age Groups in Allogeneic Hematopoietic Cell Transplant Recipients. J. Chemother. 2021, 33, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Campoli, C.; Belotti, T.; Cojutti, P.G.; Masetti, R.; Pession, A.; Viale, P.; Pea, F. Real-World Comparison of Isavuconazole and Voriconazole in Terms of the Need for Dosage Adjustments Guided by Clinical Pharmacological Advice During Primary Prophylaxis of Invasive Fungal Infections in Pediatric Patients with Hemato-Oncological Malignancies. Ther. Drug Monit. 2022, 44, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Chromsystems Instruments & Chemicals GmbH. MassTox TDM Series A; 2022; Available online: https://chromsystems.com/en/products/therapeutic-drug-monitoring.html#brochure (accessed on 1 June 2024).
- Jin, H.; Wang, T.; Falcione, B.A.; Olsen, K.M.; Chen, K.; Tang, H.; Hui, J.; Zhai, S. Trough Concentration of Voriconazole and Its Relationship with Efficacy and Safety: A Systematic Review and Meta-Analysis. J. Antimicrob. Chemother. 2016, 71, 1772–1785. [Google Scholar] [CrossRef] [PubMed]
- Hanai, Y.; Hamada, Y.; Kimura, T.; Matsumoto, K.; Takahashi, Y.; Fujii, S.; Nishizawa, K.; Takesue, Y. Optimal Trough Concentration of Voriconazole with Therapeutic Drug Monitoring in Children: A Systematic Review and Meta-Analysis. J. Infect. Chemother. 2021, 27, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Luong, M.-L.; Al-Dabbagh, M.; Groll, A.H.; Racil, Z.; Nannya, Y.; Mitsani, D.; Husain, S. Utility of Voriconazole Therapeutic Drug Monitoring: A Meta-Analysis. J. Antimicrob. Chemother. 2016, 71, 1786–1799. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Yee, J.; Kim, J.Y.; Han, H.W.; Kang, S.O.; Lee, K.E.; Gwak, H.S. Factors Associated With Voriconazole Concentration in Pediatric Patients. Ther. Drug Monit. 2020, 42, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Valle-T-Figueras, J.M.; Renedo Miró, B.; Benítez Carabante, M.I.; Díaz-de-Heredia, C.; Vima Bofarull, J.; Mendoza-Palomar, N.; Martín-Gómez, M.T.; Soler-Palacín, P. Voriconazole Use in Children: Therapeutic Drug Monitoring and Control of Inflammation as Key Points for Optimal Treatment. J. Fungi 2021, 7, 456. [Google Scholar] [CrossRef] [PubMed]
- Zane, N.R.; Chen, Y.; Wang, M.Z.; Thakker, D.R. Cytochrome P450 and Flavin-Containing Monooxygenase Families: Age-Dependent Differences in Expression and Functional Activity. Pediatr. Res. 2018, 83, 527–535. [Google Scholar] [CrossRef]
- Duong, A.; Sweet, A.; Jain, R.; Hill, J.A.; Pergam, S.A.; Boeckh, M.; Liu, C. Clinically Significant Drug Interaction: Letermovir and Voriconazole. J. Antimicrob. Chemother. 2020, 75, 775–777. [Google Scholar] [CrossRef]
- Nakashima, T.; Inamoto, Y.; Fukushi, Y.; Doke, Y.; Hashimoto, H.; Fukuda, T.; Yamaguchi, M. Drug Interaction between Letermovir and Voriconazole after Allogeneic Hematopoietic Cell Transplantation. Int. J. Hematol. 2021, 113, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Cojutti, P.G.; Londero, A.; Della Siega, P.; Givone, F.; Fabris, M.; Biasizzo, J.; Tascini, C.; Pea, F. Comparative Population Pharmacokinetics of Darunavir in SARS-CoV-2 Patients vs. HIV Patients: The Role of Interleukin-6. Clin. Pharmacokinet. 2020, 59, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Gautier-Veyret, E.; Truffot, A.; Bailly, S.; Fonrose, X.; Thiebaut-Bertrand, A.; Tonini, J.; Cahn, J.-Y.; Stanke-Labesque, F. Inflammation Is a Potential Risk Factor of Voriconazole Overdose in Hematological Patients. Fundam Clin. Pharmacol. 2019, 33, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Le Daré, B.; Boglione-Kerrien, C.; Reizine, F.; Gangneux, J.-P.; Bacle, A. Toward the Personalized and Integrative Management of Voriconazole Dosing during COVID-19-Associated Pulmonary Aspergillosis. Crit. Care 2021, 25, 152. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Fornaro, G.; Pasquini, Z.; Zanoni, A.; Bartoletti, M.; Viale, P.; Pea, F. Impact of Inflammation on Voriconazole Exposure in Critically Ill Patients Affected by Probable COVID-19-Associated Pulmonary Aspergillosis. Antibiotics 2023, 12, 764. [Google Scholar] [CrossRef] [PubMed]
- Tragiannidis, A.; Gkampeta, A.; Vousvouki, M.; Vasileiou, E.; Groll, A.H. Antifungal Agents and the Kidney: Pharmacokinetics, Clinical Nephrotoxicity, and Interactions. Expert Opin. Drug Saf. 2021, 20, 1061–1074. [Google Scholar] [CrossRef] [PubMed]
- Groll, A.H.; Townsend, R.; Desai, A.; Azie, N.; Jones, M.; Engelhardt, M.; Schmitt-Hoffman, A.-H.; Brüggemann, R.J.M. Drug-Drug Interactions between Triazole Antifungal Agents Used to Treat Invasive Aspergillosis and Immunosuppressants Metabolized by Cytochrome P450 3A4. Transpl. Infect. Dis. 2017, 19, e12751. [Google Scholar] [CrossRef]
- Kyriakidis, I.; Tragiannidis, A.; Munchen, S.; Groll, A.H. Clinical Hepatotoxicity Associated with Antifungal Agents. Expert Opin. Drug Saf. 2017, 16, 149–165. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Patient Demographic | Patients (N = 39) |
|---|---|
| Age (years) [median (IQR)] | 10 (5–15) |
| Age < 2 years | 1 (2.6) |
| Age 2–11 years | 21 (53.8) |
| Age ≥ 12 years | 17 (43.6) |
| Gender (male/female) [n (%)] | 26/13 (66.7–33.3) |
| Body weight (kg) [median (IQR)] | 41.0 (19.7–61.0) |
| Body surface area (m2) [median (IQR)] | 1.29 (0.78–1.67) |
| Underlying oncohematologic disease [n (%)] | |
| ALL | 20 (51.2) |
| AML | 10 (25.6) |
| JMML | 2 (5.1) |
| Fanconi anemia | 1 (2.6) |
| Beta-thalassemia | 1 (2.6) |
| Aplastic anemia | 1 (2.6) |
| Anaplastic large cell lymphoma | 1 (2.6) |
| HL | 1 (2.6) |
| NHL | 1 (2.6) |
| Myelodysplastic syndrome | 1 (2.6) |
| Donor [n (%)] | |
| MUD | 21 (53.9) |
| Haploidentical | 16 (41.0) |
| Sibling | 2 (5.1) |
| Stem cell source [n (%)] | |
| Bone Marrow | 26 (66.7) |
| Peripheral Blood | 13 (33.3) |
| Voriconazole prophylaxis | |
| Median dose (mg/kg/daily) [median (IQR)] | 13.9 (8.8–22.2) |
| Length of prophylaxis [days; median (IQR)] | 46 (33.5–75.0) |
| No. of TDM assessments per patient [median (IQR)] | 13 (8.5–21.5) |
| Average Cmin (mg/L) [median (IQR)] | 1.7 (0.7–3.0) |
| Median time to first TDM (days) [median (IQR)] | 3 (2.5–4) |
| No. of patients experiencing voriconazole overexposure during the first three weeks after HCT | 31 (79.5) |
| Serum inflammatory biomarkers level [median (IQR)] | |
| C-reactive protein (mg/dL) | 1.38 (0.41–8.07) |
| Procalcitonin (ng/mL) | 0.8 (0.3–3.0) |
| Interleukin-6 (pg/mL) | 72.8 (21.4–270.6) |
| Concomitant agents [n (%)] | |
| Modulators of CYP2C9, CYP2C19 and/or CYP3A4 | 39 (100.0) |
| Proton pump inhibitors | 38 (97.4) |
| Corticosteroids | 26 (66.7) |
| Letermovir | 6 (15.4) |
| HCT complications [n (%)] | |
| Documented Gram-negative bacteremia | 14 (35.9) |
| ICU admission | 9 (23.1) |
| Acute and/or chronic GvHD | 20 (51.3) |
| Clinical outcome [n (%)] | |
| Breakthrough IFI | 0 (0.0) |
| Voriconazole withdrawal due to suspected toxicity | 4 (10.3) |
| Clinical Variables | Patients < 12 Years (N = 22) | Patients ≥ 12 Years (N = 17) | p Value |
|---|---|---|---|
| Underlying oncohematologic disease [n (%)] | |||
| ALL | 10 (45.5) | 10 (58.8) | 0.41 |
| AML | 7 (31.9) | 3 (17.6) | 0.46 |
| JMML | 2 (9.1) | 0 (0.0) | 0.50 |
| Fanconi anemia | 1 (4.5) | 0 (0.0) | 0.99 |
| Beta-thalassemia | 1 (4.5) | 0 (0.0) | 0.99 |
| Aplastic anemia | 0 (0.0) | 1 (5.9) | 0.44 |
| Anaplastic large cell lymphoma | 1 (4.5) | 0 (0.0) | 0.99 |
| HL | 0 (0.0) | 1 (5.9) | 0.44 |
| NHL | 0 (0.0) | 1 (5.9) | 0.44 |
| Myelodysplastic syndrome | 0 (0.0) | 1 (5.9) | 0.44 |
| Voriconazole prophylaxis | |||
| Median dose (mg/kg/daily) [median (IQR)] | 18.0 (13.1–26.4) | 9.1 (5.9–12.1) | <0.0001 |
| Length of prophylaxis [days; median (IQR)] | 56.5 (42.75–107.75) | 38 (26–48) | 0.005 |
| No. of TDM assessments per patient [median (IQR)] | 14 (9.25–24.25) | 12 (7–14) | 0.19 |
| Average Cmin (mg/L) [median (IQR)] | 1.7 (0.7–3.2) | 1.4 (0.8–2.8) | 0.43 |
| Median time to first TDM (days) [median (IQR)] | 4 (3–5) | 3 (2–3) | 0.002 |
| No. of patients experiencing voriconazole overexposure in the first three weeks after HCT [n (%)] | 20 (90.9) | 11 (64.7) | 0.06 |
| Concomitant agents | |||
| Modulators of CYP2C9, 2C19, and/or 3A4 | 22 (100.0) | 17 (100.0) | 0.42 |
| Proton pump inhibitors | 22 (100.0) | 16 (94.1) | 0.44 |
| Corticosteroids | 17 (77.3) | 9 (52.9) | 0.11 |
| Letermovir | 1 (4.5) | 5 (29.4) | 0.06 |
| HCT complications | |||
| Documented Gram-negative bacteremia | 4 (18.2) | 10 (58.9) | 0.017 |
| ICU admission | 2 (9.1) | 7 (41.2) | 0.026 |
| Acute and/or chronic GVHD | 13 (59.1) | 7 (41.2) | 0.34 |
| Clinical outcome [n (%)] | |||
| Breakthrough IFI | 0 (0.0) | 0 (0.0) | 0.99 |
| Voriconazole withdrawn for suspected toxicity | 4 (18.2) | 0 (0.0) | 0.12 |
| Inflammatory Biomarkers | No. of Assessments | Serum Threshold Value | AUC ROC Curve (95%CI) | Sensitivity | Specificity | p Value |
|---|---|---|---|---|---|---|
| Overall | ||||||
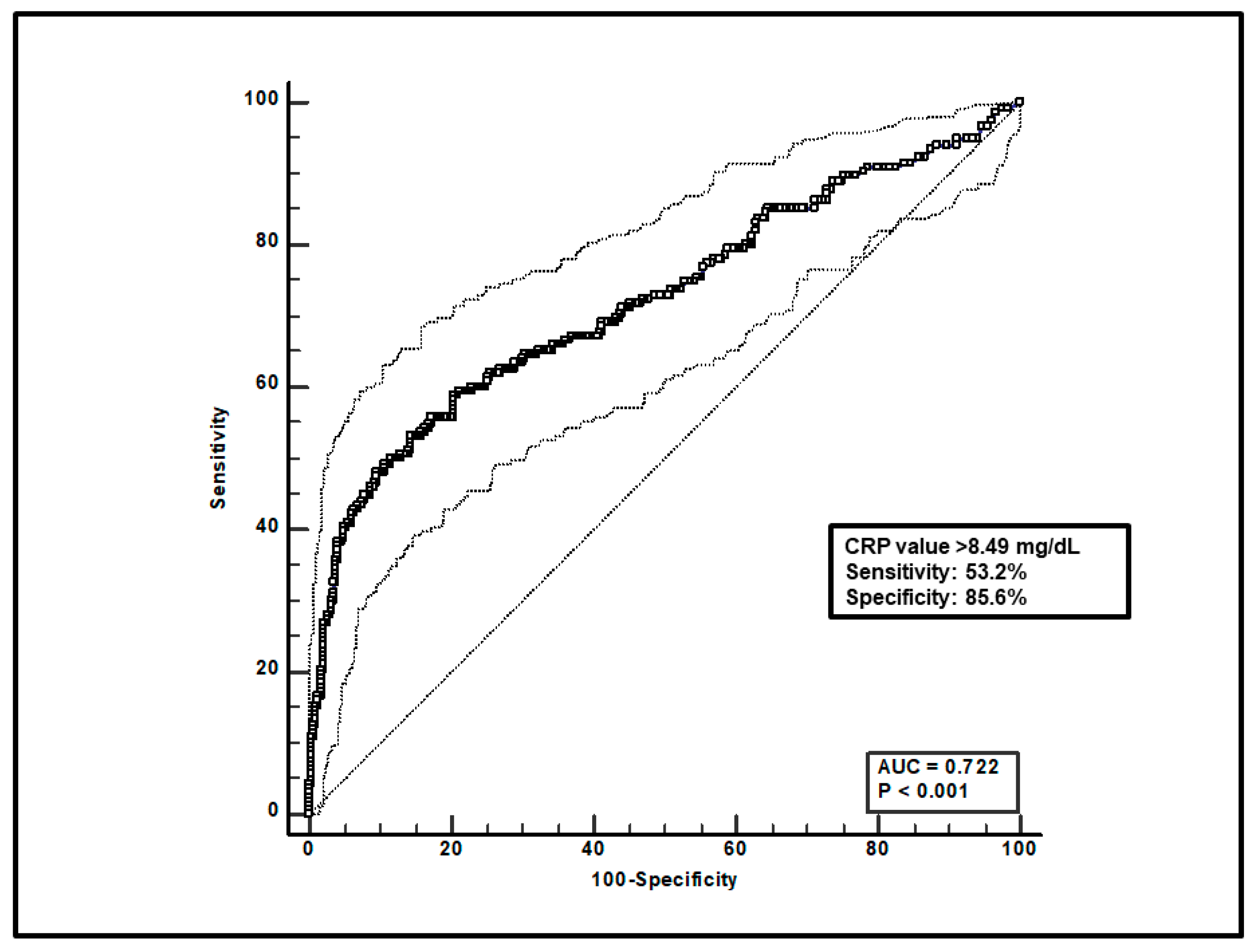
| C-reactive protein | 599 | 8.49 mg/dL | 0.72 (0.68–0.76) | 53.2% | 85.6% | <0.0001 |
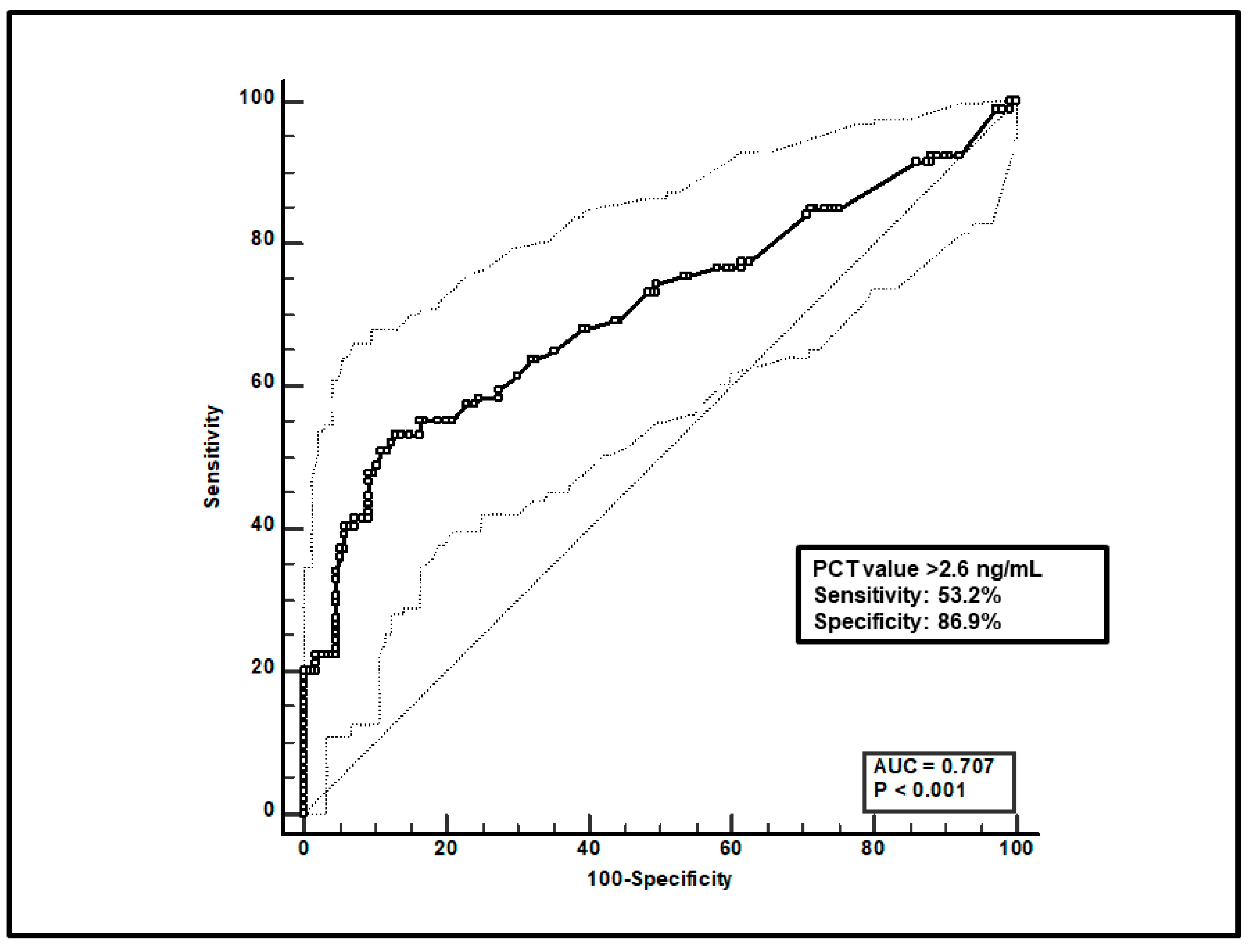
| Procalcitonin | 247 | 2.6 ng/mL | 0.71 (0.63–0.77) | 53.2% | 86.9% | <0.0001 |
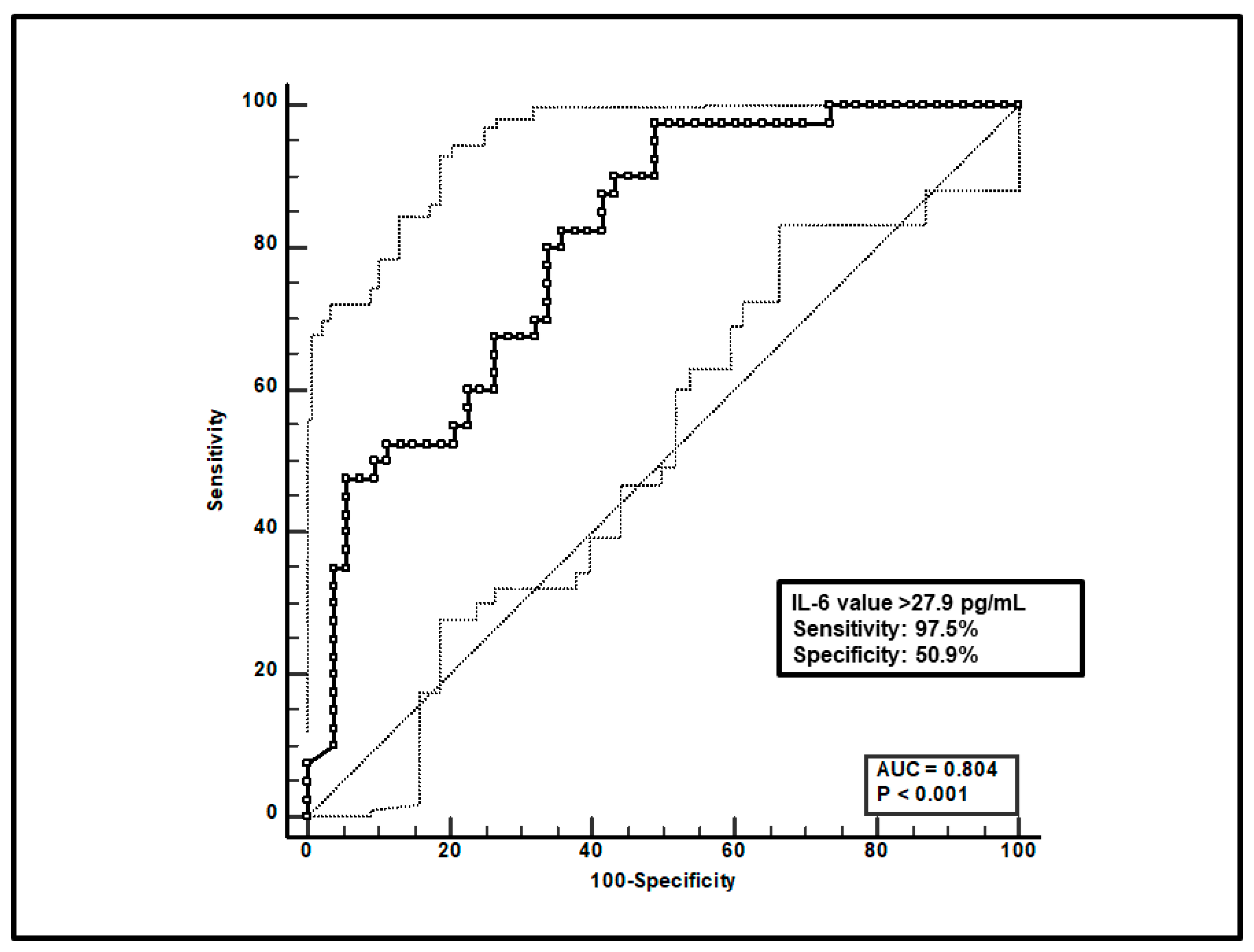
| IL-6 | 93 | 27.9 pg/mL | 0.80 (0.71–0.88) | 97.5% | 50.9% | <0.0001 |
| Age < 12 years | ||||||
| C-reactive protein | 390 | 5.49 mg/dL | 0.68 (0.63–0.71) | 46.0% | 85.6% | <0.0001 |
| Procalcitonin | 132 | 2.92 ng/mL | 0.63 (0.54–0.71) | 33.9% | 93.4% | 0.01 |
| IL-6 | 61 | 27.9 pg/mL | 0.76 (0.64–0.86) | 96.3% | 52.9% | <0.0001 |
| Age ≥ 12 years | ||||||
| C-reactive protein | 209 | 12.38 mg/dL | 0.92 (0.87–0.95) | 83.7% | 89.2% | <0.0001 |
| Procalcitonin | 115 | 2.4 ng/mL | 0.86 (0.78–0.91) | 81.6% | 81.8% | <0.0001 |
| IL-6 | 32 | 52.0 pg/mL | 0.87 (0.71–0.97) | 92.3% | 73.7% | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gatti, M.; Campoli, C.; Muratore, E.; Belotti, T.; Masetti, R.; Lanari, M.; Viale, P.; Pea, F. Impact of Inflammatory Burden on Voriconazole Exposure in Oncohematological Pediatric Patients Receiving Antifungal Prophylaxis after Allogeneic HCT. Microorganisms 2024, 12, 1388. https://doi.org/10.3390/microorganisms12071388
Gatti M, Campoli C, Muratore E, Belotti T, Masetti R, Lanari M, Viale P, Pea F. Impact of Inflammatory Burden on Voriconazole Exposure in Oncohematological Pediatric Patients Receiving Antifungal Prophylaxis after Allogeneic HCT. Microorganisms. 2024; 12(7):1388. https://doi.org/10.3390/microorganisms12071388
Chicago/Turabian StyleGatti, Milo, Caterina Campoli, Edoardo Muratore, Tamara Belotti, Riccardo Masetti, Marcello Lanari, Pierluigi Viale, and Federico Pea. 2024. "Impact of Inflammatory Burden on Voriconazole Exposure in Oncohematological Pediatric Patients Receiving Antifungal Prophylaxis after Allogeneic HCT" Microorganisms 12, no. 7: 1388. https://doi.org/10.3390/microorganisms12071388