Biomechanical Study of Proximal Femur for Designing Stems for Total Hip Replacement



Abstract
:1. Introduction
2. Materials and Methods
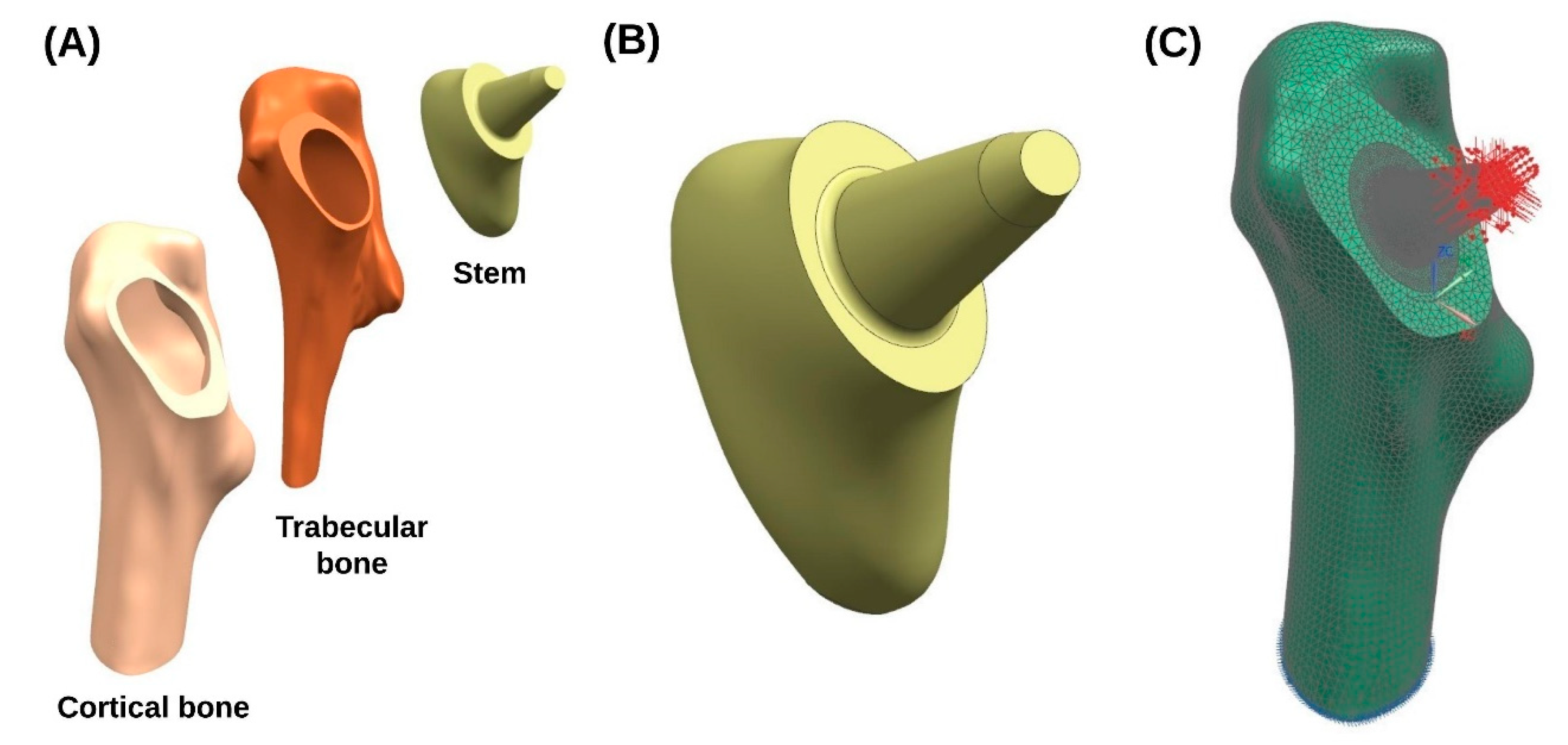
2.1. Geometric Model
2.2. Finite Element Model
2.3. Boundary Conditions
2.4. Post-Processing
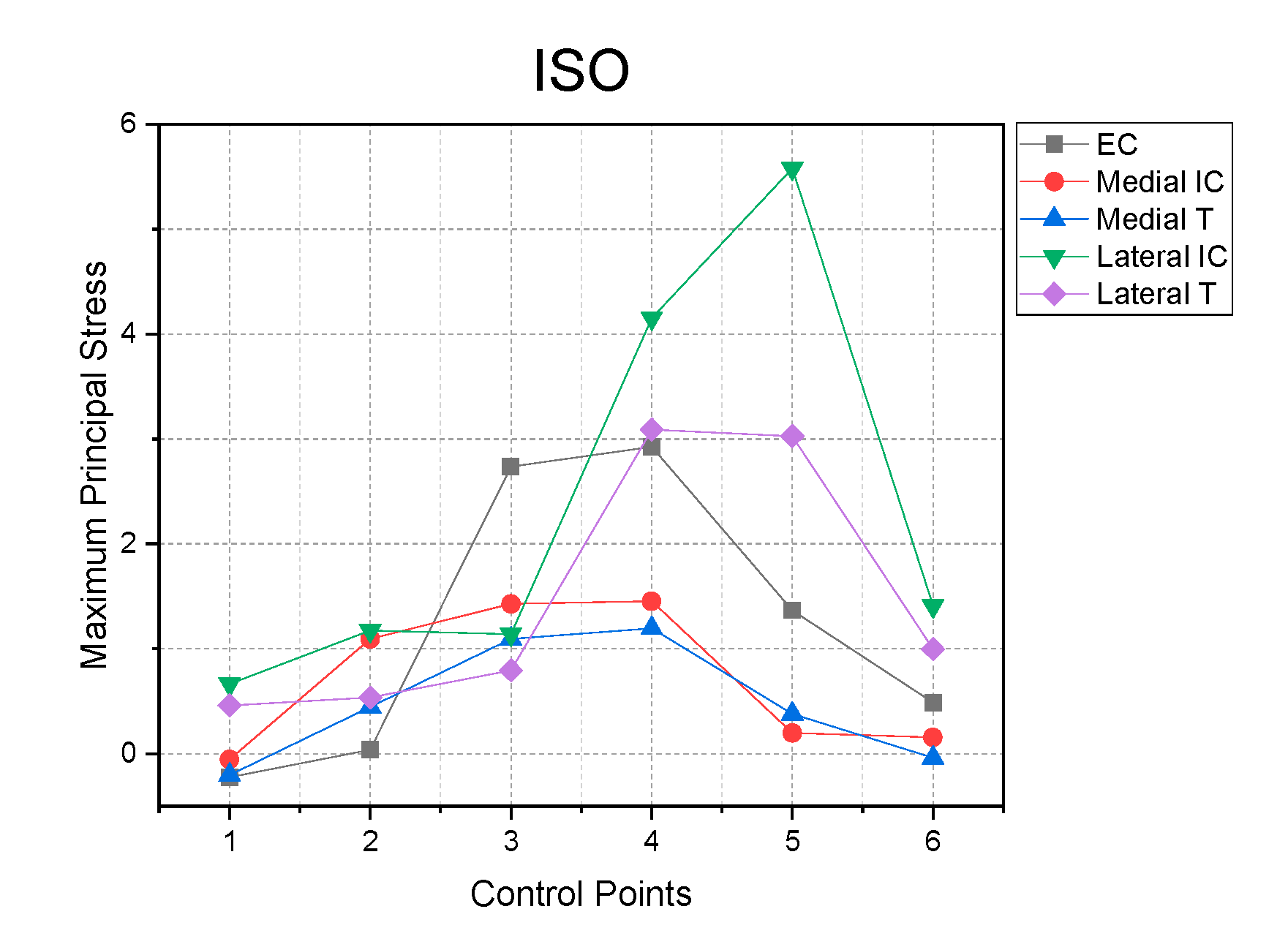
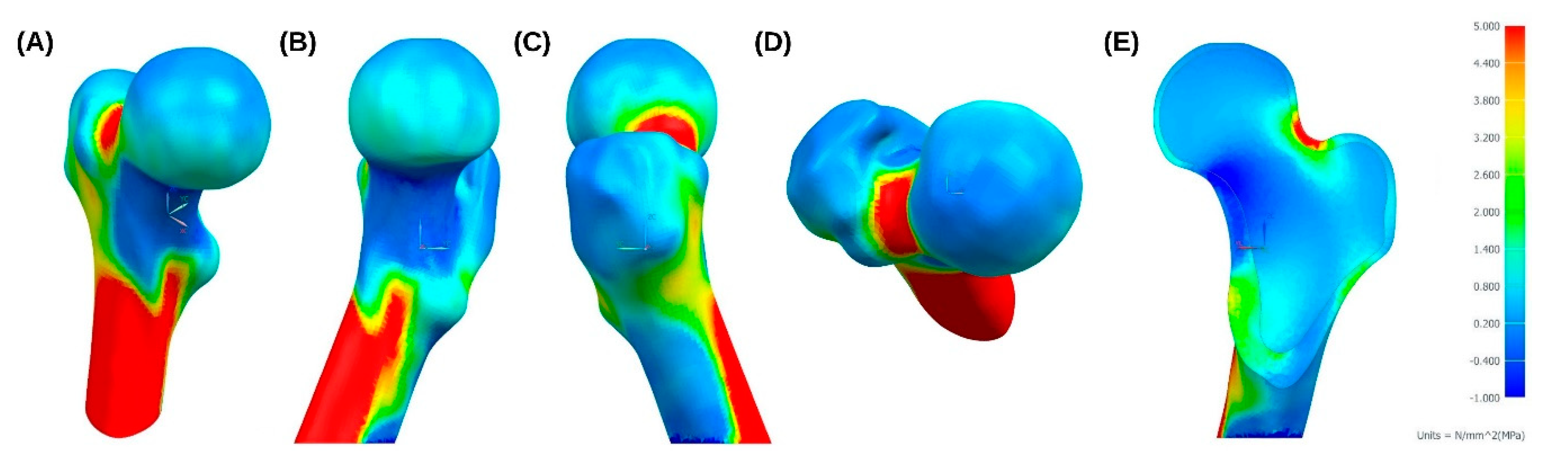
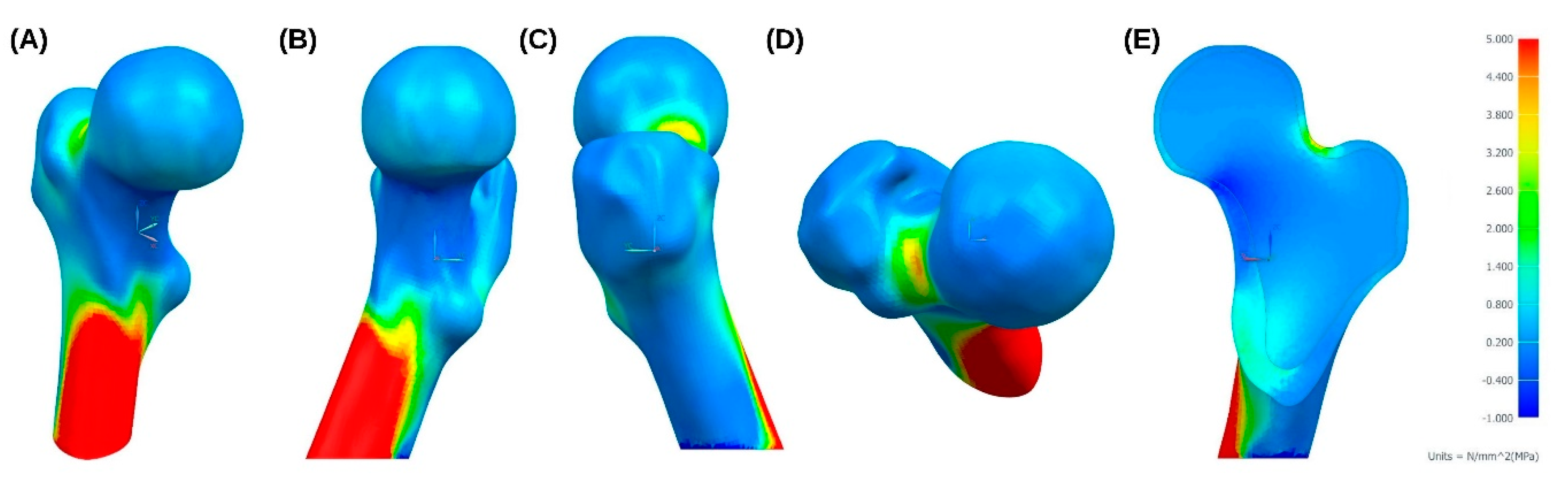
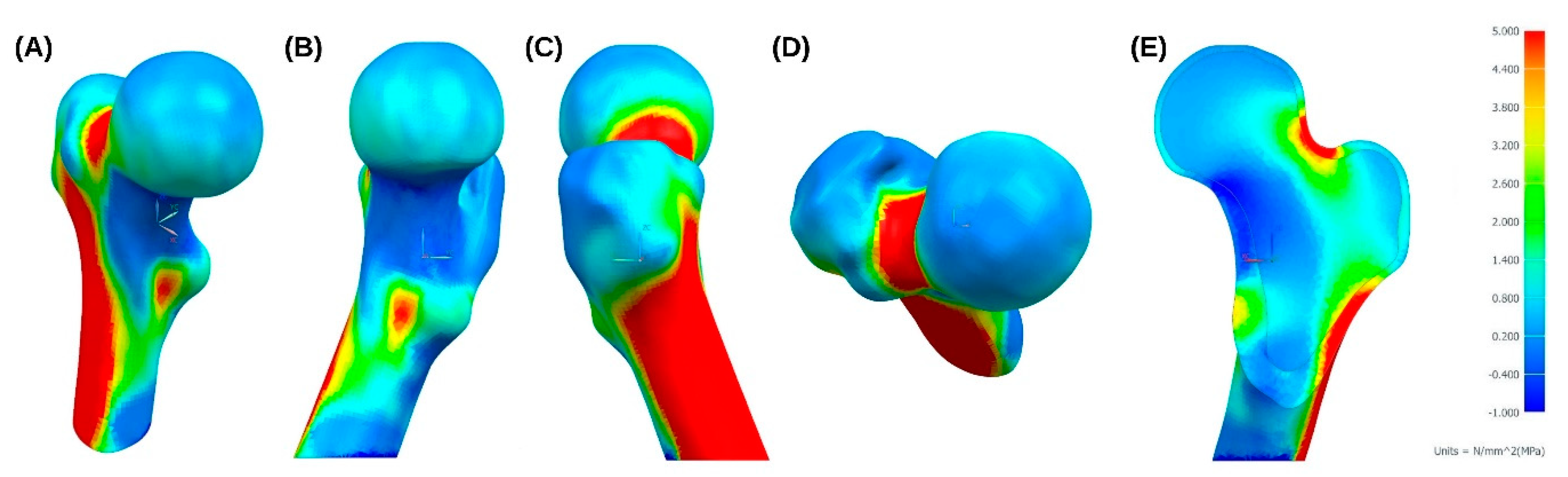
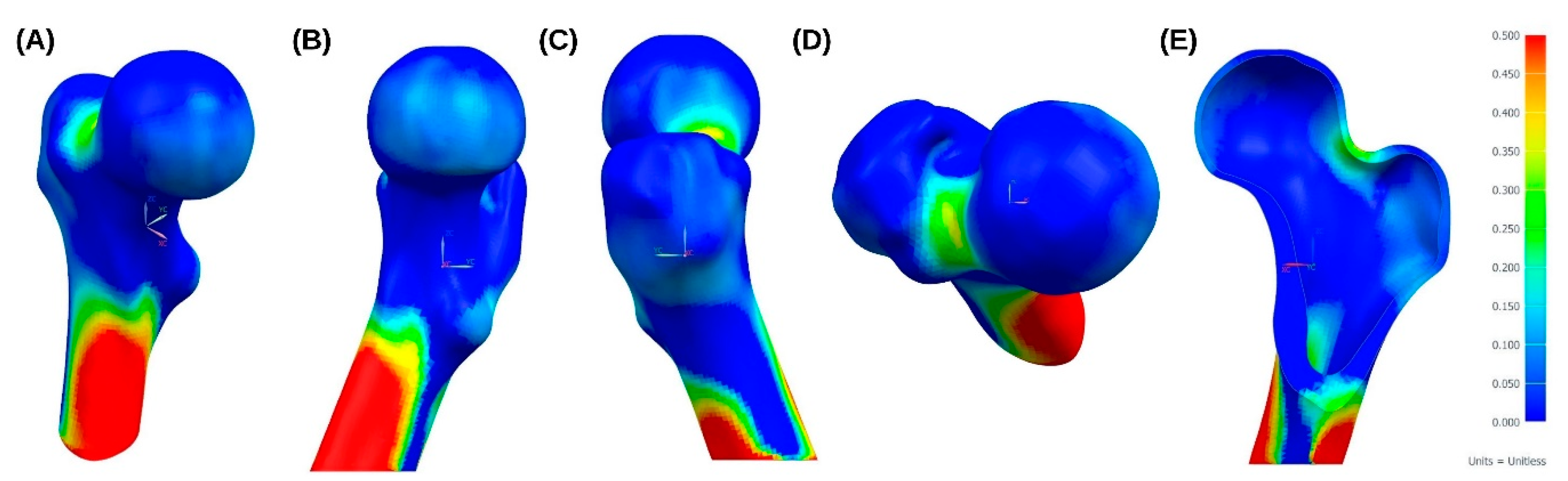
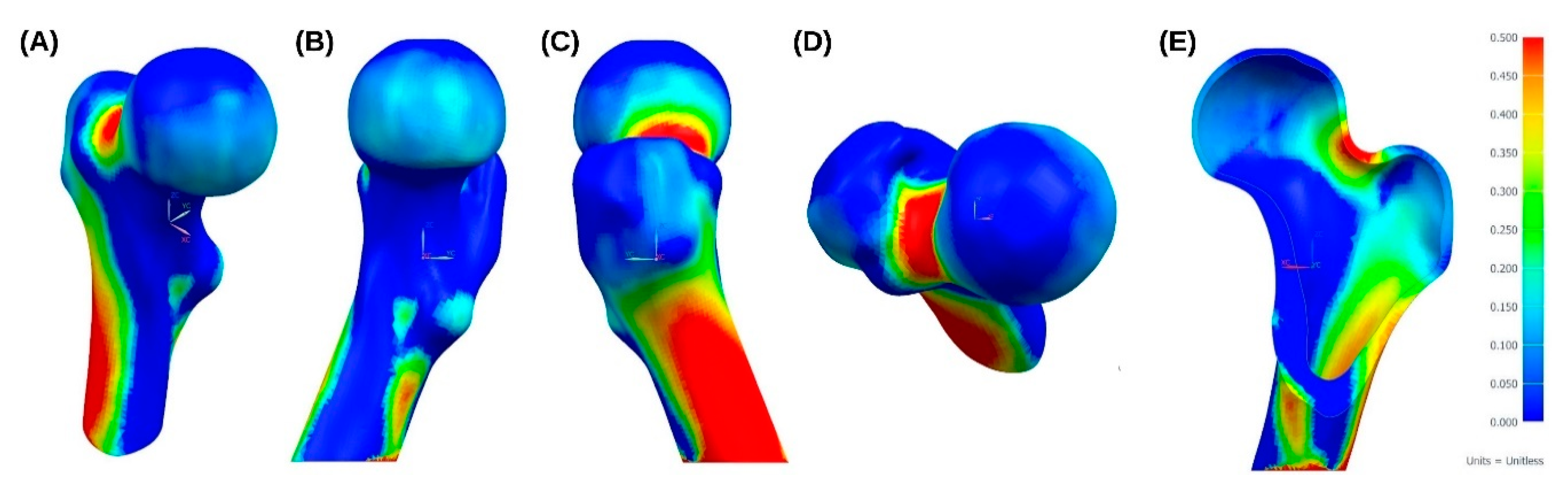
3. Results
4. Discussion and Future Proposals
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weiner, S.; Wagner, H.D. The material bone: Structure-mechanical function relations. Annu. Rev. Mater. Sci. 1998, 28, 271–298. [Google Scholar] [CrossRef]
- Clarke, B. Normal bone anatomy and physiology. Clin. J. Am. Soc. Nephrol. 2008, 3 (Suppl. 3), 131–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannesdottir, F.; Bouxsein, M.L. Bone structure and biomechanics. In Encyclopedia of Endocrine Diseases; Elsevier: Amsterdam, The Netherlands, 2018; pp. 19–30. [Google Scholar]
- Taichman, R.S. Blood and bone: Two tissues whose fates are intertwined to create the hematopoietic stem-cell niche. Blood 2005, 105, 2631–2639. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, R.K.; Thompson, W.R.; Warden, S.J. Bone biology. In Bone Repair Biomaterials; Elsevier: Amsterdam, The Netherlands, 2019; pp. 15–52. [Google Scholar]
- Hart, N.H.; Nimphius, S.; Rantalainen, T.; Ireland, A.; Siafarikas, A.; Newton, R.U. Mechanical basis of bone strength: Influence of bone material, bone structure and muscle action. J. Musculoskelet Neuronal Interact. 2017, 17, 114–139. [Google Scholar] [PubMed]
- Florencio-Silva, R.; Sasso, G.R.; Sasso-Cerri, E.; Simões, M.J.; Cerri, P.S. Biology of bone tissue: Structure, function, and factors that influence bone cells. BioMed Res. Int. 2015, 2015, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrer Cañabate, J.; Tovar, I.; Martínez, P. Osteoprotegerina y Sistema RANKL/RANK: ¿el futuro fel metabolismo óseo? Anales de Medicina Interna 2002, 19, 5–8. [Google Scholar] [CrossRef] [Green Version]
- Caetano-Lopes, J.; Canhão, H.; Fonseca, J.E. Osteoblasts and bone formation. Acta Reumatol. Port. 2007, 32, 103–110. [Google Scholar]
- Arboleya, L.; Castañeda, S. Osteoclastos: Mucho más que células remodeladoras del hueso. Rev. Osteoporos. Metab. Miner. 2014, 6, 109–121. [Google Scholar] [CrossRef]
- Bilezikian, J.P.; Raisz, L.G.; Martin, T.J. Principles of Bone Biology, 3rd ed.; Academic Press/Elsevier: San Diego, CA, USA, 2008. [Google Scholar]
- Bozal, C.B. Osteocytes as mechanosensors in bone. Actual. Osteol. 2013, 9, 176–193. [Google Scholar]
- Doblaré, M.; García, J.M.; Gómez, M.J. Modelling bone tissue fracture and healing: A review. Eng. Fract. Mech. 2004, 71, 1809–1840. [Google Scholar] [CrossRef]
- Rucci, N. Molecular biology of bone remodelling. Clin. Cases Miner. Bone Metab. 2008, 5, 49–56. [Google Scholar] [PubMed]
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjidakis, D.J.; Androulakis, I.I. Bone remodeling. Ann. N. Y. Acad. Sci. 2006, 1092, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J. Das Gesetz der Transformation der Knochen; Pro Business: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Skedros, J.G.; Brand, R.A. Biographical sketch: Georg hermann von meyer (1815–1892). Clin. Orthop. Relat. Res. 2011, 469, 3072–3076. [Google Scholar] [CrossRef] [Green Version]
- Hammer, A. The paradox of wolff’s theories. Ir. J. Med. Sci. 2015, 184, 13–22. [Google Scholar] [CrossRef]
- Koch, J.C. The laws of bone architecture. Am. J. Anat. 1917, 21, 177–298. [Google Scholar] [CrossRef]
- Rybicki, E.F.; Simonen, F.A.; Weis, E.B. On the mathematical analysis of stress in the human femur. J. Biomech. 1972, 5, 203–215. [Google Scholar] [CrossRef]
- Fetto, J.F.; Bettinger, P.; Austin, K. Reexamination of hip biomechanics during unilateral stance. Am. J. Orthop. 1995, 24, 605–612. [Google Scholar]
- Santori, N.; Lucidi, M.; Santori, F.S. Proximal load transfer with a stemless uncemented femoral implant. J. Orthopaed. Traumatol. 2006, 7, 154–160. [Google Scholar] [CrossRef]
- Rho, J.Y.; Hobatho, M.C.; Ashman, R.B. Relations of mechanical properties to density and CT numbers in human bone. Med. Eng. Phys. 1995, 17, 347–355. [Google Scholar] [CrossRef]
- Keyak, J.H.; Kaneko, T.S.; Tehranzadeh, J.; Skinner, H.B. Predicting proximal femoral strength using structural engineering models. Clin. Orthop. Relat. Res. 2005, 437, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Pithioux, M. Lois de Comportement et Modèles de Rupture des os Longs en Accidentologie. Ph.D. Thesis, Université de la Méditerranée, Marseille, France, 2000. [Google Scholar]
- Pithioux, M.; Lasaygues, P.; Chabrand, P. An Alternative ultrasonic method for measuring the elastic properties of cortical bone. J. Biomech. 2002, 35, 961–968. [Google Scholar] [CrossRef] [Green Version]
- Peng, L.; Bai, J.; Zeng, X.; Zhou, Y. Comparison of isotropic and orthotropic material property assignments on femoral finite element models under two loading conditions. Med. Eng. Phys. 2006, 28, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Tellache, M.; Pithioux, M.; Chabrand, P.; Hochard, C. Femoral neck fracture prediction by anisotropic yield criteria. Eur. J. Comput. Mech. 2009, 18, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Bergmann, G.; Bender, A.; Dymke, J.; Duda, G.; Damm, P. Standardized loads acting in hip implants. PLoS ONE 2016, 11, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, I.; Chandraphak, S.; Mahakkanukrauh, P. Femoral neck-shaft angle in humans: Variation relating to climate, clothing, lifestyle, sex, age and side. J. Anat. 2013, 223, 133–151. [Google Scholar] [CrossRef]
- Mu Jung, J.; Sang Kim, C. Analysis of stress distribution around total hip stems custom-designed for the standardized Asian femur configuration. Biotechnol. Biotechnol. Equip. 2014, 28, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Rabbani, M.; Saidpour, H. stress analysis of a total hip replacement subjected to realistic loading conditions. J. Robot. Mech. Eng. Res. 2015, 1, 18–23. [Google Scholar]
- Schileo, E.; Taddei, F.; Cristofolini, L.; Viceconti, M. Subject-specific finite element models implementing a maximum principal strain criterion are able to estimate failure risk and fracture location on human femurs tested in vitro. J. Biomech. 2008, 41, 356–367. [Google Scholar] [CrossRef]
- Ojeda, C. Estudio de la Influencia de Estabilidad Primaria en el Diseño de Vástagos de Prótesis Femorales Personalizadas: Aplicación a Paciente Específico. Ph.D. Thesis, Universidad Politécnica de Madrid, Madrid, Spain, 2009. [Google Scholar]
- Cheruvu, B.; Venkatarayappa, I.; Goswami, T. Stress shielding in cemented hip implants assessed from computed tomography. Biomed. J. Sci. Tech. Res. 2019, 18, 13637–13641. [Google Scholar]
- Gargiulo, P.; Gislason, M.K.; Edmunds, K.J.; Pitocchi, J.; Carraro, U.; Esposito, L.; Fraldi, M.; Bifulco, P.; Cesarelli, M.; Jónsson, H. CT-based bone and muscle assessment in normal and pathological conditions. In Encyclopedia of Biomedical Engineering; Elsevier: Amsterdam, The Netherlands, 2019; pp. 119–134. [Google Scholar]
- Yao, Z.; Lin, T.-H.; Pajarinen, J.; Sato, T.; Goodman, S. Host response to orthopedic implants (metals and plastics). In Host Response to Biomaterials; Elsevier: Amsterdam, The Netherlands, 2015; pp. 315–373. [Google Scholar]
- Cooper, R.R. The Scientific Basis of Joint Replacement. JAMA 1977, 238, 2731. [Google Scholar] [CrossRef]
- Morales de Cano, J.; Vergara, P.; Valero, J.; Clos, R. Utilización de los vástagos metafisarios «Próxima» DePuy: Nuestra experiencia a más de cinco años. Acta Ortopédica Mexicana 2018, 32, 88–92. [Google Scholar] [PubMed]
- Shin, Y.-S.; Suh, D.-H.; Park, J.-H.; Kim, J.-L.; Han, S.-B. Comparison of specific femoral short stems and conventional-length stems in primary cementless total hip arthroplasty. Orthopedics 2016, 39, 311–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Properties | Cortical Bone | Trabecular Bone |
|---|---|---|
| (MPa) | 9753.3 | 3969.8 |
| (MPa) | 9753.3 | 3969.8 |
| (MPa) | 16255.6 | 6616.3 |
| (MPa) | 2835.7 | 2835.7 |
| (MPa) | 4063.9 | 4063.9 |
| (MPa) | 4063.9 | 4063.9 |
| 0.4 | 0.4 | |
| 0.25 | 0.25 | |
| 0.25 | 0.25 |
| Yield Limits (MPa) | Cortical Bone |
|---|---|
| 35.5 | |
| , | 21.3 |
| 71.1 | |
| , | 42.6 |
| 10.7 | |
| 17.8 |
| Tsai–Wu Coefficients | |
|---|---|
| (mm2/N) | 0.0141 |
| (mm2/N) | 0.0235 |
| (mm4/N2) | 3.96 × 10−4 |
| (mm4/N2) | 1.1 × 10−3 |
| (mm4/N2) | 3.168 × 10−3 |
| (mm4/N2) | 8.8 × 10−3 |
| Cycling | Sitting Down | Standing Up | Walking | Staying | Stairs Up | Knee Bending | Stairs Down | Jogging | ISO * Force | |
|---|---|---|---|---|---|---|---|---|---|---|
| −FX (N) | 299.5 | 714.4 | 1125.1 | 596.8 | 681.6 | 829.9 | 857 | 773.6 | 884.8 | - |
| FY (N) | −41.4 | −62.7 | 49.9 | 17.1 | −35.7 | −48.5 | −37.1 | −55.6 | −15 | - |
| −FZ (N) | 805.7 | 1931.5 | 2481.2 | 1931.5 | 2280.2 | 2763.6 | 2054.9 | 2611 | 3222 | 2300 |
| Cycling | Sitting Down | Standing Up | Walking | Staying | Stairs Up | Knee Bending | Stairs Down | Jogging | ISO Force | |
|---|---|---|---|---|---|---|---|---|---|---|
| Max. MPS (MPa) | 6.09 | 14.51 | 27.67 | 13.96 | 14.29 | 17.26 | 20 | 15.77 | 20.25 | 42 |
| Min. MPS (MPa) | −11.37 | −27.82 | −46.81 | −25.57 | −27.87 | −33.78 | −34.18 | −31.27 | −37.31 | −23.24 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solórzano, W.; Ojeda, C.; Diaz Lantada, A. Biomechanical Study of Proximal Femur for Designing Stems for Total Hip Replacement. Appl. Sci. 2020, 10, 4208. https://doi.org/10.3390/app10124208
Solórzano W, Ojeda C, Diaz Lantada A. Biomechanical Study of Proximal Femur for Designing Stems for Total Hip Replacement. Applied Sciences. 2020; 10(12):4208. https://doi.org/10.3390/app10124208
Chicago/Turabian StyleSolórzano, William, Carlos Ojeda, and Andres Diaz Lantada. 2020. "Biomechanical Study of Proximal Femur for Designing Stems for Total Hip Replacement" Applied Sciences 10, no. 12: 4208. https://doi.org/10.3390/app10124208
APA StyleSolórzano, W., Ojeda, C., & Diaz Lantada, A. (2020). Biomechanical Study of Proximal Femur for Designing Stems for Total Hip Replacement. Applied Sciences, 10(12), 4208. https://doi.org/10.3390/app10124208