Manual Therapy Versus Closed Kinematic Exercises—The Influence on the Range of Movement in Patients with Knee Osteoarthritis: A Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- advanced inflammatory osteoarthritis of the knee (Kellegren–Lawrence stage 3 or 4),
- patellofemoral disorders,
- neurological diseases,
- age below 55 or above 75 years,
- neoplastic disease,
- other rheumatic conditions (rheumatoid arthritis, ankylosing spondylitis, psoriatic spondylitis),
- sciatic neuralgia,
- status post major lower limb trauma,
- status post lower limb surgery (e.g. arthroscopy, replacement arthroplasty),
- congenital defects and deformation of the lower limbs.
2.2. Experimental Procedures and Instruments
2.2.1. Range of Motion (Orthyo System)
- Range of active knee motion: test in the open kinematic chain. The patient performed the test in the prone position with the lower limbs extended. The patient was requested to perform maximum knee flexion that would not elicit pain. The test was recorded by the motion sensors that calculated the difference between the initial and maximum angle (Figure 1).
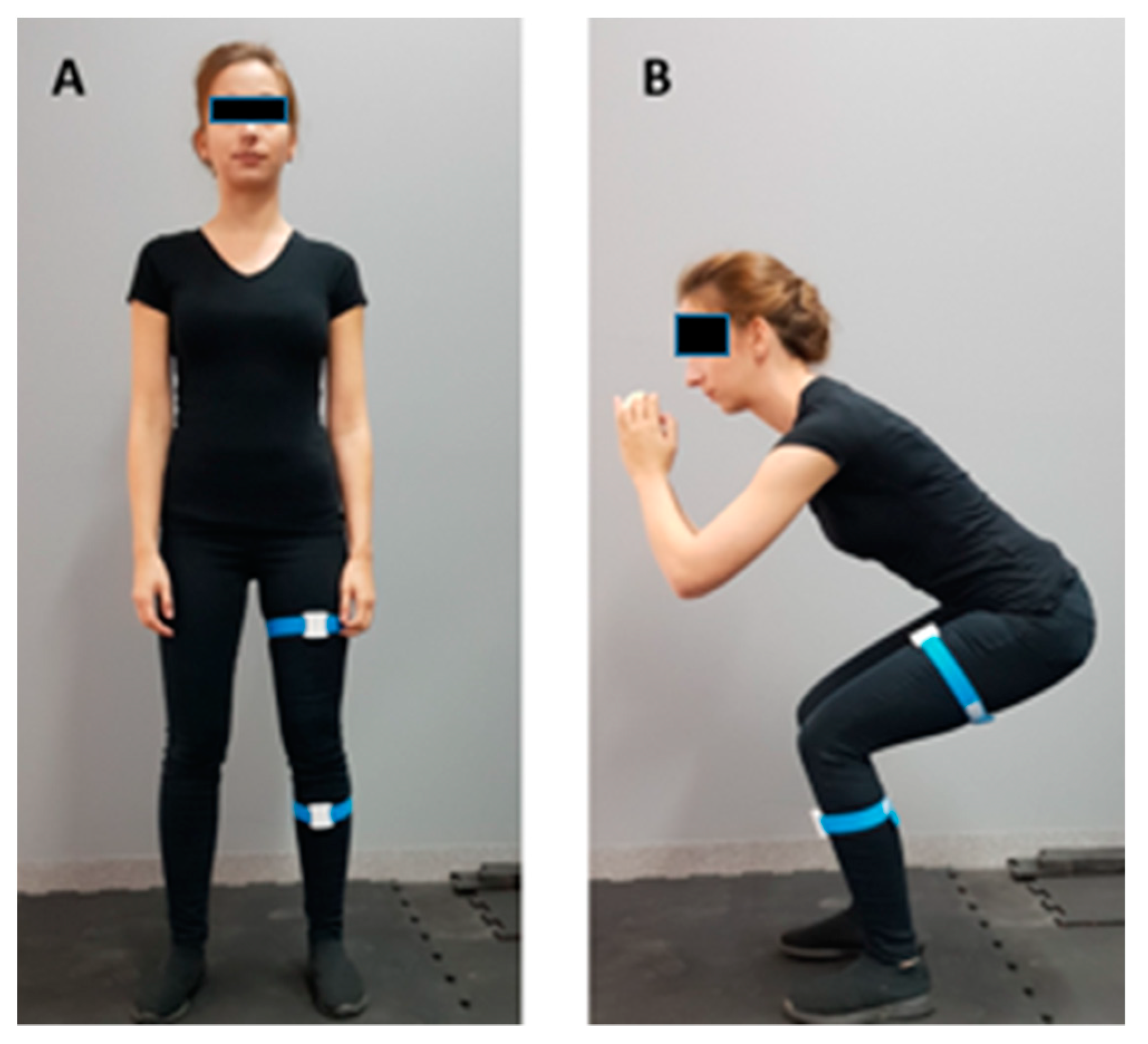
- Maximum range of knee motion test while squatting. The patient performed the test in a standing position with the lower limbs hip-width apart. Subsequently, the patient was asked to squat as much as possible without feeling pain (Figure 2).
2.2.2. WOMAC
2.2.3. VAS
2.3. Intervention
2.4. Statistical Analysis
3. Results
3.1. Range of Motion Measurements
3.2. WOMAC
3.3. VAS
4. Discussion
5. Conclusions
- Manual 10-day therapy is beneficial for the range of knee motion in patients with OAK.
- Synergistic 10-day lower limb movement exercises in the closed chain achieve greater squat depth without pain in patients with OAK.
- Manual therapy in combination with exercises may potentially achieve a greater functional effect.
- Measurements in different biomechanical conditions are useful when evaluating the range of motion.
- Inertial sensors are a reliable and objective tool for evaluating the range of motion in different biomechanical conditions.
- There is a need for further research aimed at assessing the long-term effect of the therapy.
5.1. Clinical Implications
5.2. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Park, E.; Park, H.-R.; Choi, E.-S. Barriers to and Facilitators of Physical Activity among Korean Female Adults with Knee Osteoarthritis and Comorbidity: A Qualitative Study. Healthcare 2020, 8, 226. [Google Scholar] [CrossRef]
- Xu, H.; Zhao, G.; Xia, F.; Liu, X.; Gong, L.; Wen, X. The diagnosis and treatment of knee osteoarthritis: A literature review. Int. J. Clin. Exp. Med. 2019, 12, 4589–4599. [Google Scholar]
- Uchio, Y.; Enomoto, H.; Ishida, M.; Tsuji, T.; Ochiai, T.; Konno, S. Safety and efficacy of duloxetine in Japanese patients with chronic knee pain due to osteoarthritis: An open-label, long-term, Phase III extension study. J. Pain Res. 2018, 11, 1391–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clynes, M.A.; Jameson, K.A.; Edwards, M.H.; Cooper, C.; Dennison, E.M. Impact of osteoarthritis on activities of daily living: Does joint site matter? Aging Clin. Exp. Res. 2019, 31, 1049–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyodo, K.; Masuda, T.; Aizawa, J.; Jinno, T.; Morita, S. Hip, knee, and ankle kinematics during activities of daily living: A cross-sectional study. Braz. J. Phys. Ther. 2017, 21, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Holla, J.F.M.; Steultjens, M.P.M.; van der Leeden, M.; Roorda, L.D.; Bierma-Zeinstra, S.M.A.; den Broeder, A.A.; Dekker, J. Determinants of range of joint motion in patients with early symptomatic osteoarthritis of the hip and/or knee: An exploratory study in the CHECK cohort. Osteoarthr. Cartil. 2011, 19, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Jevsevar, D.S.; Riley, P.O.; Hodge, W.A.; Krebs, D.E. Knee Kinematics and Kinetics During Locomotor Activities of Daily Living in Subjects with Knee Arthroplasty and in Healthy Control Subjects. Physical. Ther. 1993, 73, 229–239. [Google Scholar] [CrossRef] [Green Version]
- Andriacchi, T.P.; Andersson, G.; Fermier, R.; Stern, D.; Galante, J. A study of lower-limb mechanics during stair-climbing. J. Bone Jt. Surg. Am. Vol. 1980, 62, 749–757. [Google Scholar] [CrossRef]
- Stevermer, C. Functional Movement Assessment for Individuals with Knee Osteoarthritis. Ph.D. Thesis, Iowa State University, Ames, IA, USA, 2010. [Google Scholar]
- Lambert, S.J. A Comparison of Closed v& Open Kinetic Chain Exercises in the Rehabilitation of Anterior Cruciate Ligament Injuries. An Honors Thesis, Ball State University, Muncie, Indiana, 1998; pp. 1–15. [Google Scholar]
- Skou, S.T.; Roos, E.M.; Laursen, M.B.; Rathleff, M.S.; Arendt-Nielsen, L.; Rasmussen, S.; Simonsen, O. Total knee replacement and non-surgical treatment of knee osteoarthritis: 2-year outcome from two parallel randomized controlled trials. Osteoarthr. Cartil. 2018, 26, 1170–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisiński, P.; Wareńczak, A.; Hejdysz, K.; Sip, P.; Gośliński, J.; Owczarek, P.; Jonak, J.; Goślińska, J. Mobile Applications in Evaluations of Knee Joint Kinematics: A Pilot Study. Sensors 2019, 19, 3675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jogi, P.; Overend, T.J.; Spaulding, S.J.; Zecevic, A.; Kramer, J.F. Effectiveness of balance exercises in the acute post-operative phase following total hip and knee arthroplasty: A randomized clinical trial. SAGE Open Med. 2015, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brokelman, R.B.G.; Haverkamp, D.; van Loon, C.; Hol, A.; van Kampen, A.; Veth, R. The validation of the visual analogue scale for patient satisfaction after total hip arthroplasty. Eur. Orthop. Traumatol. 2012, 3, 101–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Lai, Z.; Wang, L. Effects of Taichi exercise on knee and ankle proprioception among individuals with knee osteoarthritis. Res. Sports Med. 2020, 28, 268–278. [Google Scholar] [CrossRef]
- Lin, D.-H.; Lin, Y.-F.; Chai, H.-M.; Chai, H.-M.; Han, Y.-C.; Jan, M.-H. Comparison of proprioceptive functions between computerized proprioception facilitation exercise and closed kinetic chain exercise in patients with knee osteoarthritis. Clin. Rheumatol. 2007, 26, 520–528. [Google Scholar] [CrossRef]
- Kumar, S.; Kumar, A.; Kumar, R. Proprioceptive training as an adjunct in osteoarthritis of knee. J. Musculoskelet. Res. 2013, 16, 1350002. [Google Scholar] [CrossRef]
- Sekir, U.; Gür, H. A multi-station proprioceptive exercise program in patients with bilateral knee osteoarthrosis: Functional capacity, pain and sensoriomotor function. A randomized controlled trial. J Sports Sci. Med. 2005, 4, 590–603. [Google Scholar]
- Huang, D.; Wang, H.-G.; Wu, W.-Z.; Zhang, H.-R.; Lin, H. Functional and aesthetic results of immediate reconstruction of traumatic thumb defects by toe-to-thumb transplantation. Int. Orthop. 2011, 35, 543–547. [Google Scholar] [CrossRef] [Green Version]
- Abdelazeem, F.; Nambi, G.; Elnegamy, T. Comparative study on Virtual Reality Training (VRT) over Sensory Motor Training (SMT) in Unilateral Chronic Osteoarthritis—A Randomized Control Trial. Int. J. Med. Res. Health Sci. 2016, 5, 7–16. [Google Scholar]
- Sobel, D.; Kwiatkowski, J.; Ryt, A.; Domzal, M.; Jedrasiak, K.; Janik, L.; Nawrat, A. Range of Motion Measurements Using Motion Capture Data and Augmented Reality Visualisation. In Proceedings of the Computer Vision and Graphics, Warsaw, Poland, 15–17 September 2014; Chmielewski, L.J., Kozera, R., Shin, B.-S., Wojciechowski, K., Eds.; Springer International Publishing: Cham, Switzerland, 2014; pp. 594–601. [Google Scholar]
- Sharma, B.M.; Vidhya, S.; Kumar, N. System for measurement of joint range of motion using inertial sensors. Biomed. Res. 2017, 3699–3704. [Google Scholar]
- Fennema, M.C.; Bloomfield, R.A.; Lanting, B.A.; Birmingham, T.B.; Teeter, M.G. Repeatability of measuring knee flexion angles with wearable inertial sensors. Knee 2019, 26, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Van der Kruk, E.; Reijne, M.M. Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef]
- Alkhawajah, H.A.; Alshami, A.M. The effect of mobilization with movement on pain and function in patients with knee osteoarthritis: A randomized double-blind controlled trial. BMC Musculoskelet. Disord. 2019, 20, 452. [Google Scholar] [CrossRef]
- Field, T.; Diego, M.; Gonzalez, G.; Funk, C.G. Knee arthritis pain is reduced and range of motion is increased following moderate pressure massage therapy. Complement. Ther. Clin. Pract. 2015, 21, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Arshad, N.; Gondal, M.I.; Qamar, M.M.; Basharat, A. Download citation of Manual therapy can be a potential therapy in knee osteoarthritis. Saudi J. Sports Med. 2018, 18, 18–21. [Google Scholar]
- Perlman, A.I.; Ali, A.; Njike, V.Y.; Hom, D.; Davidi, A.; Gould-Fogerite, S.; Milak, C.; Katz, D.L. Massage Therapy for Osteoarthritis of the Knee: A Randomized Dose-Finding Trial. PLoS ONE 2012, 7, e30248. [Google Scholar] [CrossRef] [Green Version]
- Dor, A.; Kalichman, L. A myofascial component of pain in knee osteoarthritis. J. Bodyw. Mov. Ther. 2017, 21, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Courtney, C.A.; Steffen, A.D.; Fernández-de-Las-Peñas, C.; Kim, J.; Chmell, S.J. Joint Mobilization Enhances Mechanisms of Conditioned Pain Modulation in Individuals with Osteoarthritis of the Knee. J. Orthop. Sports Phys. Ther. 2016, 46, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizis, P.; Manko, G.; Kobza, W.; Para, B. Manual Therapy with Cryotherapy versus Kinesiotherapy with Cryotherapy for Knee Osteoarthritis: A Randomized Controlled Trial. Altern. Ther. Health Med. 2019, 25, 40–45. [Google Scholar]
- Hameed, R.; Waqas, M.; Akhtar, F.; Robinson, J.; Niazi, A. Mahmood Effect of Manual Therapy on Knee Osteoarthritis (OA) Pain, A Randomized Control Trial. Int. J. Res. Stud. Med. Health Sci. 2017, 2, 19–22. [Google Scholar] [CrossRef]
- Cliborne, A.V.; Wainner, R.S.; Rhon, D.I.; Judd, C.D.; Fee, T.T.; Matekel, R.L.; Whitman, J.M. Clinical hip tests and a functional squat test in patients with knee osteoarthritis: Reliability, prevalence of positive test findings, and short-term response to hip mobilization. J. Orthop. Sports Phys. Ther. 2004, 34, 676–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchio, L.D. The health and performance benefits of the squat, deadlift, and bench press. MOJYPT 2018, 3, 40–47. [Google Scholar] [CrossRef]
- Fox, J.T.; Hefzy, M.S. Knee and Ankle Biomechanics during Squatting with Heels on and Off of the Ground, with and without Weight Shifting. Bone Muscle 2019, 2, 1–9. [Google Scholar]
- Mondam, S.; Babu, S.; Kumar, R.; Prakash, J. A Comparative Study of Proprioceptive Exercises versus Conventional Training Program on Osteoarthritis of Knee. RJRS 2012, 1, 2277–2502. [Google Scholar]
- AdemolaGbiri, C. Comparative Efficacy of Open-chain and Close-chain Kinematics on Proprioception, Muscles’ Strength and Functional Performances in Individual with Knee Osteoarthritis. Occup. Med. Health Aff. 2013, 1, 1–5. [Google Scholar] [CrossRef]
- Reid, D.A.; McNair, P.J. Effects of an acute hamstring stretch in people with and without osteoarthritis of the knee. Physiotherapy 2010, 96, 14–21. [Google Scholar] [CrossRef]
- Rhon, D.; Deyle, G.; Gill, N.; Rendeiro, D. Manual physical therapy and perturbation exercises in knee osteoarthritis. J. Man. Manip. Ther. 2013, 21, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Abbott, J.H.; Usiskin, I.M.; Wilson, R.; Hansen, P.; Losina, E. The quality-of-life burden of knee osteoarthritis in New Zealand adults: A model-based evaluation. PLoS ONE 2017, 12, e0185676. [Google Scholar] [CrossRef] [Green Version]
- Deyle, G.D.; Allison, S.C.; Matekel, R.L.; Ryder, M.G.; Stang, J.M.; Gohdes, D.D.; Hutton, J.P.; Henderson, N.E.; Garber, M.B. Physical therapy treatment effectiveness for osteoarthritis of the knee: A randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys. Ther. 2005, 85, 1301–1317. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Mean ± SD | Median | Min–Max | p |
|---|---|---|---|---|---|
| age (years) | E | 62.4 ± 5.4 | 62.0 | 55.0–75.0 | 0.13 |
| MT | 65.2 ± 3.1 | 65.0 | 58.0–70.0 | ||
| C | 64.0 ± 5.7 | 63.0 | 55.0–75.0 | ||
| weight (kg) | E | 78.0 ± 12.2 | 75.0 | 58.0–100.0 | 0.15 |
| MT | 78.2 ± 12.5 | 75.0 | 58.0–105.0 | ||
| C | 71.1 ± 12.2 | 68.0 | 56.0–90.0 | ||
| height (m) | E | 1.68 ± 0.08 | 1.67 | 1.53–1.82 | 0.88 |
| MT | 1.65 ± 0.08 | 1.64 | 1.55–1.81 | ||
| C | 1.68 ± 0.07 | 1.68 | 1.56–1.80 | ||
| body mass index (BMI) | E | 27.6 ± 3.7 | 27.1 | 20.4–36.1 | 0.40 |
| MT | 28.6 ± 4.3 | 28.3 | 20.9–38.3 | ||
| C | 25.1 ± 3.9 | 24.0 | 19.8–34.3 |
| Variable | Group | Before | After | p3 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Range | p1 | Mean ± SD | Median | Range | p2 | |||
| Active range (°) | E MT C | 100.1 ± 22.5 98.4 ± 21.2 111.4 ± 15.5 | 106.4 97.6 112.9 | 19.7–141.2 51.0–139.0 72.2–135.2 | 0.02 0.27 * | 103.5 ± 22.2 104.1 ± 16.8 112.2 ± 13.9 | 104.5 103.2 115.9 | 26.8–139.0 64.5–142.5 85.9–141.2 | 0.04 0.92 * | 0.57 0.01 * 0.73 * |
| Squat (°) | E MT C | 71.5 ± 15.3 81.1 ± 19.2 80.8 ± 16.4 | 73.2 80.7 82.6 | 33.2–95.8 43.1–118.5 52.7–122.8 | 0.06 | 74.6 ± 15.5 84.0 ± 17.8 82.1 ± 16.1 | 76.5 81.5 79.4 | 38.1–100.6 45.9–115.0 56.3–114.6 | 0.07 | < 0.01 * 0.12 * 0.36 * |
| Variable | Group | Before | After | p3 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Range | p1 | Mean ± SD | Median | Range | p2 | |||
| WOMAC | E | 41.8 ± 138 | 41.0 | 19.0–65.0 | <0.01 | 36.4 ± 14.1 | 39.0 | 08.0–58.0 | < 0.01 | <0.01 |
| MT | 48.2 ± 19.6 | 47.0 | 2.0–81.0 | 41.0 ± 28.8 | 32.0 | 1.0–84.0 | 0.01 | |||
| C | 19.7 ± 19.3 | 12.5 | 2.0–78.0 | 19.0 ± 20.6 | 11.0 | 1.0–75.0 | 0.18 * | |||
| VAS left | E | 4.9 ± 2.7 | 5.5 | 0.0–10.0 | 0.96 | 2.5 ± 2.1 | 2.5 | 0.0–6.0 | 0.67 | <0.01 * |
| MT | 4.9 ± 2.5 | 5.0 | 0.0–8.0 | 3.1 ± 2.7 | 3.0 | 0.0–8.0 | <0.01 | |||
| VAS right | E | 5.0 ± 2.6 | 5.0 | 0.0–10.0 | 0.09 | 2.8 ± 2.0 | 3.0 | 0.0–6.0 | 0.34 | <0.01 |
| MT | 4.8 ± 2.5 | 5.0 | 0.0–8.0 | 3.2 ± 2.7 | 3.0 | 0.0–8.0 | <0.01 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hejdysz, K.; Goślińska, J.; Wareńczak, A.; Dudzińska, J.; Adamczyk, E.; Sip, P.; Gośliński, J.; Owczarek, P.; Woźniak, A.; Lisiński, P. Manual Therapy Versus Closed Kinematic Exercises—The Influence on the Range of Movement in Patients with Knee Osteoarthritis: A Pilot Study. Appl. Sci. 2020, 10, 8605. https://doi.org/10.3390/app10238605
Hejdysz K, Goślińska J, Wareńczak A, Dudzińska J, Adamczyk E, Sip P, Gośliński J, Owczarek P, Woźniak A, Lisiński P. Manual Therapy Versus Closed Kinematic Exercises—The Influence on the Range of Movement in Patients with Knee Osteoarthritis: A Pilot Study. Applied Sciences. 2020; 10(23):8605. https://doi.org/10.3390/app10238605
Chicago/Turabian StyleHejdysz, Krystyna, Jagoda Goślińska, Agnieszka Wareńczak, Joanna Dudzińska, Ewa Adamczyk, Paweł Sip, Jarosław Gośliński, Piotr Owczarek, Adam Woźniak, and Przemysław Lisiński. 2020. "Manual Therapy Versus Closed Kinematic Exercises—The Influence on the Range of Movement in Patients with Knee Osteoarthritis: A Pilot Study" Applied Sciences 10, no. 23: 8605. https://doi.org/10.3390/app10238605