
Acoustic-Field Beamforming-Based Generalized Coherence Factor for Handheld Ultrasound

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Acoustic Field Beamforming (AFB) Technology
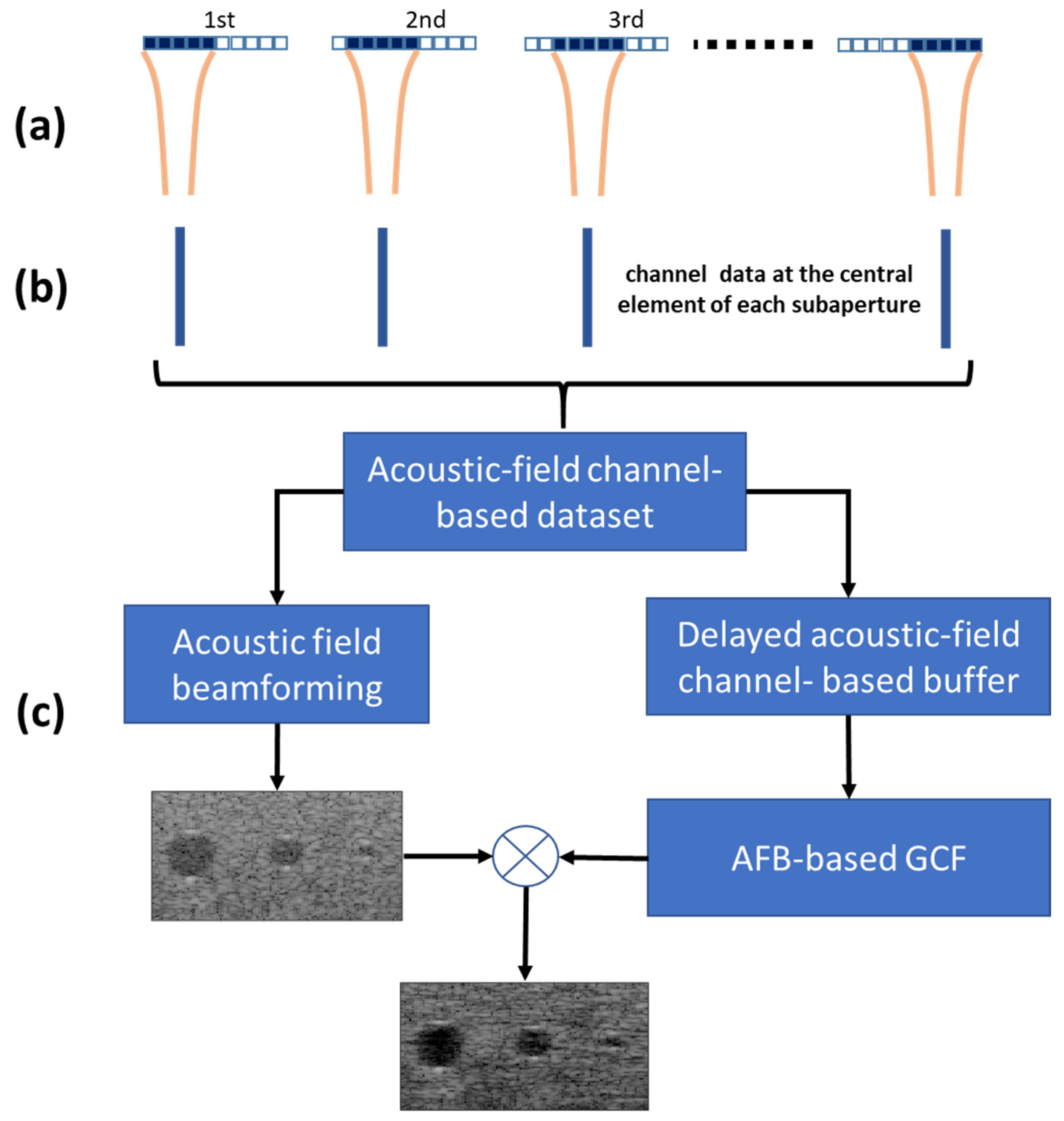
2.2. AFB-Based Generalized Coherence Factor (GCF) Technology
2.3. Point and Cyst Target Simulations
2.4. Experimental Setup
2.5. In Vivo Carotid Artery Data
2.6. Image Quality Estimation
2.7. Selection of M0
3. Results and Discussion
3.1. Point-Target Simulations
3.2. Anechoic Cyst Simulation
3.3. Experimental Results
3.4. In Vivo Carotid Artery
3.5. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yanikoglu, F.; Avci, H.; Celik, Z.C.; Tagtekin, D. Diagnostic performance of ICDAS II, FluoreCam and ultrasound for flat surface caries with different depths. Ultrasound Med. Biol. 2020, 46, 1755–1760. [Google Scholar] [CrossRef] [PubMed]
- Schapher, M.; Goncalves, M.; Mantsopoulos, K.; Iro, H.; Koch, M. Transoral ultrasound in the diagnosis of obstructive salivary gland pathologies. Ultrasound Med. Biol. 2019, 45, 2338–2348. [Google Scholar] [CrossRef]
- Moore, C.L.; Copel, J.A. Point-of-care ultrasonography. N. Engl. J. Med. 2011, 364, 749–757. [Google Scholar] [CrossRef] [Green Version]
- Kendall, J.L.; Hoffenberg, S.R.; Smith, R.S. History of emergency and critical care ultrasound: The evolution of a new imaging paradigm. Crit. Care Med. 2007, 35, S126–S130. [Google Scholar] [CrossRef] [PubMed]
- Cosby, K.S.; Kendall, J.L. Practical Guide to Emergency Ultrasound; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Mayron, R.; Gaudio, F.E.; Plummer, D.; Asinger, R.; Elsperger, J. Echocardiography performed by emergency physicians: Impact on diagnosis and therapy. Ann. Emerg. Med. 1988, 17, 150–154. [Google Scholar] [CrossRef]
- Nelson, B.P.; Narula, J. How relevant is point-of-care ultrasound in LMIC? Glob. Heart 2013, 8, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Daniels, J.M.; Hoppmann, R.A. Practical Point-of-Care Medical Ultrasound; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Wagner, M.S.; Garcia, K.; Martin, D.S. Point-of-care ultrasound in aerospace medicine: Known and potential applications. Aviat. Space Environ. Med. 2014, 85, 730–739. [Google Scholar] [CrossRef]
- Hwang, J.J.; Quistgaard, J.; Souquet, J.; Crum, L.A. Portable ultrasound device for battlefield trauma. In Proceedings of the 1998 IEEE Ultrasonics Symposium, Sendai, Japan, 5–8 October 1998; Volume 2, pp. 1663–1667. [Google Scholar]
- Nelson, B.P.; Chason, K. Use of ultrasound by emergency medical services: A review. Int. J. Emerg. Med. 2008, 1, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Thompson, M.R. The Future of Portable Ultrasound: Business Strategies for Survival. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2010. [Google Scholar]
- Rykkje, A.; Carlsen, J.F.; Nielsen, M.B. Hand-held ultrasound devices compared with high-end ultrasound systems: A systematic review. Diagnostics 2019, 9, 61. [Google Scholar] [CrossRef] [Green Version]
- Becker, D.M.; Tafoya, C.A.; Becker, S.L.; Kruger, G.H.; Tafoya, M.J.; Becker, T.K. The use of portable ultrasound devices in low-and middle-income countries: A systematic review of the literature. Trop. Med. Int. Health 2016, 21, 294–311. [Google Scholar] [CrossRef]
- Reeder, R.; Petersen, C. 8-Channel, 12-Bit, 10-MSPS to 50-MSPS Front End: The AD9271–A Revolutionary Solution for Portable Ultrasound. Analog. Dialogue 2007, 41, 3. [Google Scholar]
- Brunner, E. How ultrasound system considerations influence front-end component choice. Analog. Dialogue 2002, 36, 1–4. [Google Scholar]
- Szabo, T.L. Diagnostic Ultrasound Imaging: Inside Out; Academic Press: Cambridge, MA, USA, 2004. [Google Scholar]
- Qiu, W.; Yu, Y.; Tsang, F.K.; Sun, L. A multifunctional, reconfigurable pulse generator for high-frequency ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2012, 59, 1558–1567. [Google Scholar] [PubMed]
- Choi, H. Stacked transistor bias circuit of class-b amplifier for portable ultrasound systems. Sensors 2019, 19, 5252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, C.L.; Wu, G.Z.; Chang, C.C.; Li, M.L. Acoustic-Field Beamforming for Low-Power Portable Ultrasound. Ultrason. Imaging 2021, 43, 175–185. [Google Scholar] [CrossRef]
- Perrot, V.; Polichetti, M.; Varray, F.; Garcia, D. So you think you can DAS? A viewpoint on delay-and-sum beamforming. Ultrasonics 2021, 111, 106309. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Thomas, A.; Mayanglambam, S.S. Improvement of Delay and Sum beamforming photoacoustic imaging based on delay-multiply-sum-to-standard-deviation-factor. Int. Soc. Opt. Photonics 2021, 11642, 116423D. [Google Scholar]
- Steinberg, B.D. Digital beamforming in ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 1992, 39, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Eldar, Y.C. Sparse convolutional beamforming for ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2018, 65, 2390–2406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewener, H.; Risser, C.; Brausch, L.; Rohrer, T.; Tretbar, S. A mobile ultrasound system for majority detection. In Proceedings of the 2019 IEEE International Ultrasonics Symposium, Glasgow, UK, 6–9 October 2019; pp. 502–505. [Google Scholar]
- Alexander, J. Xilinx devices in portable ultrasound systems. WP378 (v1. 2). Available online: https://www.xilinx.com/support/documentation/white_papers/wp378-Xilinx-in-Portable-Ultrasound.pdf (accessed on 13 December 2021).
- Maxim, Datasheet MAX2082. Low-Power, High-Performance Octal Ultrasound Transceiver with Integrated AFE, Pulser, T/R Switch, and CWD Beamformer; Maxim Integrated Products: San Jose, CA, USA, 2014. [Google Scholar]
- Mallart, R.; Fink, M. Adaptive focusing in scattering media through sound-speed inhomogeneities: The van Cittert Zernike approach and focusing criterion. J. Acoust. Soc. Am. 1994, 96, 3721. [Google Scholar] [CrossRef]
- Rindal, O.M.H.; Austeng, A.; Torp, H.; Holm, S.; Rodriguez-Molares, A. The dynamic range of adaptive beamformers. In Proceedings of the 2016 IEEE International Ultrasonics Symposium, Tours, France, 18–21 September 2016; pp. 1–4. [Google Scholar]
- Hollman, K.W.; Rigby, K.W.; O’donnell, M. Coherence factor of speckle from a multi-row probe. In Proceedings of the 1999 IEEE Ultrasonics Symposium, Tahoe, NV, USA, 17–20 October 1999; Volume 2, pp. 1257–1260. [Google Scholar]
- Nilsen, C.I.C.; Holm, S. Wiener beamforming and the coherence factor in ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2010, 57, 1329–1346. [Google Scholar] [CrossRef]
- Camacho, J.; Parrilla, M.; Fritsch, C. Phase coherence imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2009, 56, 958–974. [Google Scholar] [CrossRef] [PubMed]
- Li, M.L.; Li, P.C. A new adaptive imaging technique using generalized coherence factor. In Proceedings of the 2002 IEEE Ultrasonics Symposium, Munich, Germany, 8–11 October 2002; Volume 2, pp. 1627–1630. [Google Scholar]
- Li, P.C.; Li, M.L. Adaptive imaging using the generalized coherence factor. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2003, 50, 128–141. [Google Scholar]
- Jensen, J.A. Field: A program for simulating ultrasound systems. In Proceedings of the 10th Nordic-Baltic Conference on Biomedical Imaging, Tampere, Finland, 9–13 June 1996; Volume 4, pp. 351–353. [Google Scholar]
- Jensen, J.A.; Svendsen, N.B. Calculation of pressure fields from arbitrarily shaped, apodized, and excited ultrasound transducers. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 1992, 39, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.L.; Cheng, I.C.; Huang, C.H.; Liao, Y.T.; Lin, W.-C.; Tsai, K.J.; Chi, C.H.; Chen, C.W.; Wu, C.H.; Lin, I.T.; et al. Dry Wearable Textile Electrodes for Portable Electrical Impedance Tomography. Sensors 2021, 21, 6789. [Google Scholar] [CrossRef] [PubMed]
- Saris, A.E.; Hansen, H.H.; Fekkes, S.; Nillesen, M.M.; Rutten, M.C.; de Korte, C.L. A comparison between compounding techniques using large beam-steered plane wave imaging for blood vector velocity imaging in a carotid artery model. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2016, 63, 1758–1771. [Google Scholar] [CrossRef] [PubMed]
- Liebgott, H.; Rodriguez-Molares, A.; Cervenansky, F.; Jensen, J.A.; Bernard, O. Plane-wave imaging challenge in medical ultrasound. In Proceedings of the 2016 IEEE International Ultrasonics Symposium, Tours, France, 18–21 September 2016; pp. 1–4. [Google Scholar]
- Smith, S.W.; Wagner, R.F. Ultrasond speckle size and lesion signal to noise ratio: Verification of theory. Ultrason. Imaging 1984, 6, 174–180. [Google Scholar] [CrossRef]
- Karaman, M.; Li, P.C.; O’Donnell, M. Synthetic aperture imaging for small scale systems. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 1995, 42, 429–442. [Google Scholar] [CrossRef]
- Xu, M.; Yang, X.; Ding, M.; Yuchi, M. Spatio-temporally smoothed coherence factor for ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2014, 61, 182–190. [Google Scholar] [CrossRef]
- Santos, P.; Koriakina, N.; Chakraborty, B.; Pedrosa, J.; Petrescu, A.M.; Voigt, J.U.; D’hooge, J. Evaluation of coherence-based beamforming for B-mode and speckle tracking echocardiography. In Proceedings of the 2018 IEEE International Ultrasonics Symposium, Kobe, Japan, 22–25 October 2018; pp. 1–4. [Google Scholar]
- Shen, C.C.; Xing, Y.Q.; Jeng, G. Autocorrelation-based generalized coherence factor for low-complexity adaptive beamforming. Ultrasonics 2016, 72, 177–183. [Google Scholar] [CrossRef]
- Hisatsu, M.; Mori, S.; Arakawa, M.; Kanai, H. Generalized coherence factor estimated from real signals in ultrasound beamforming. J. Med. Ultrason. 2020, 47, 179–192. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| −6 dB (mm) | 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 64 Tx/64 Rx DAS | 3 Tx/1 Rx AFB | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 3 Tx/1 Rx GCF | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF |
| 1st point (10 mm) | 1.12 | 1.29 | 1.64 | 0.62 | 0.67 | 0.96 | 0.62 | 0.66 | 0.96 |
| 2nd point (20 mm) | 1.49 | 1.05 | 1.38 | 0.67 | 0.54 | 1.2 | 0.68 | 0.55 | 1.21 |
| 3rd point (30 mm) | 2.54 | 1.11 | 0.58 | 0.82 | 0.59 | 1.65 | 0.84 | 0.61 | 1.68 |
| 4th point (40 mm) | 3.49 | 1.64 | 1.38 | 0.96 | 0.67 | 1.79 | 0.98 | 0.68 | 1.82 |
| 5th point (50 mm) | 6.18 | 3.8 | 3.2 | 1.26 | 1.42 | 2.06 | 1.28 | 1.43 | 2.08 |
| SNR (dB) | 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 64 Tx/64 Rx DAS | 3 Tx/1 Rx AFB | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 3 Tx/1 Rx GCF | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF |
| 1st point (10 mm) | 37.16 | 38.56 | 39.37 | 48.5 | 48.28 | 46.57 | 60.09 | 61.67 | 57.72 |
| 2nd point (20 mm) | 44.85 | 49.78 | 49.83 | 55.72 | 54.59 | 52.92 | 68.03 | 66.07 | 62.59 |
| 3rd point (30 mm) | 47.62 | 51.71 | 56.31 | 55.74 | 56.52 | 54.25 | 67.36 | 64.55 | 64.33 |
| 4th point (40 mm) | 43.82 | 45.52 | 45.61 | 54.19 | 55.37 | 54.01 | 66.44 | 65.67 | 65.64 |
| 5th point (50 mm) | 42.61 | 42.76 | 43.79 | 53.86 | 55.19 | 52.12 | 63.91 | 65.16 | 63.51 |
| CR (dB) | 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 64 Tx/64 Rx DAS | 3 Tx/1 Rx AFB | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 3 Tx/1 Rx GCF | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF |
| 2nd cyst (20 mm) | 23.02 | 28.25 | 20.92 | 10.52 | 12.22 | 15.14 | 29.34 | 32.44 | 33.38 |
| 3rd cyst (30 mm) | 24.92 | 30.68 | 37.1 | 14.14 | 16.38 | 12.75 | 36.13 | 37.65 | 30.73 |
| 4th cyst (40 mm) | 16.56 | 26.4 | 20.63 | 13.91 | 11.12 | 16.83 | 28.34 | 24.89 | 30.97 |
| STD (dB) | 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 64 Tx/64 Rx DAS | 3 Tx/1 Rx AFB | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 3 Tx/1 Rx GCF | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF |
| 2nd cyst (20 mm) | 7.18 | 7.38 | 6.81 | 5.41 | 5.77 | 5.94 | 9.5 | 8.9 | 8.69 |
| 3rd cyst (30 mm) | 5.74 | 6.15 | 6.1 | 6.41 | 5.56 | 6.14 | 7.5 | 7.6 | 8.59 |
| 4th cyst (40 mm) | 6.75 | 6.73 | 6.92 | 6.1 | 5.71 | 5.54 | 9.2 | 8.6 | 8.59 |
| CNR | 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 64 Tx/64 Rx DAS | 3 Tx/1 Rx AFB | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 3 Tx/1 Rx GCF | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF |
| 2nd cyst (20 mm) | 2.46 | 2.94 | 2.96 | 1.29 | 2.21 | 1.46 | 2.31 | 2.56 | 2.64 |
| 3rd cyst (30 mm) | 2.96 | 3.62 | 3.92 | 1.43 | 2.32 | 2.21 | 2.96 | 3.35 | 2.9 |
| 4th cyst (40 mm) | 1.91 | 2.96 | 2.98 | 1.66 | 2.01 | 2.2 | 2.31 | 2.35 | 2.87 |
| 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 64 Tx/64 Rx DAS | 3 Tx/1 Rx AFB | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 3 Tx/1 Rx GCF | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF | |
|---|---|---|---|---|---|---|---|---|---|
| CR (dB) | 20.43 | 22.85 | 23.22 | 19.02 | 19.23 | 19.06 | 33.41 | 33.9 | 33.76 |
| STD (dB) | 5.26 | 5.47 | 5.6 | 5.34 | 5.32 | 5.01 | 8.03 | 8.04 | 8.1 |
| CNR | 2.67 | 2.97 | 3 | 2.45 | 2.56 | 2.55 | 3.2 | 3.26 | 3.22 |
| 16 Tx/16 Rx DAS | 32 Tx/32 Rx DAS | 5 Tx/1 Rx AFB | 7 Tx/1 Rx AFB | 5 Tx/1 Rx GCF | 7 Tx/1 Rx GCF | |
|---|---|---|---|---|---|---|
| CR (dB) | 18.86 | 20.1 | 19.72 | 15.44 | 34.77 | 27.31 |
| Std (dB) | 6.87 | 5.51 | 6.32 | 6.34 | 7.51 | 7.91 |
| CNR | 2.01 | 2.32 | 2.23 | 1.86 | 2.52 | 2.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, C.-L.; Li, C.-J.; Cheng, I.-C.; Sun, P.-Z.; Hsu, B.; Cheng, H.-H.; Lin, Z.-S.; Lin, C.-W.; Li, M.-L. Acoustic-Field Beamforming-Based Generalized Coherence Factor for Handheld Ultrasound. Appl. Sci. 2022, 12, 560. https://doi.org/10.3390/app12020560
Hu C-L, Li C-J, Cheng I-C, Sun P-Z, Hsu B, Cheng H-H, Lin Z-S, Lin C-W, Li M-L. Acoustic-Field Beamforming-Based Generalized Coherence Factor for Handheld Ultrasound. Applied Sciences. 2022; 12(2):560. https://doi.org/10.3390/app12020560
Chicago/Turabian StyleHu, Chang-Lin, Chien-Ju Li, I-Cheng Cheng, Peng-Zhi Sun, Brian Hsu, Hsiao-Hsuan Cheng, Zhan-Sheng Lin, Chii-Wann Lin, and Meng-Lin Li. 2022. "Acoustic-Field Beamforming-Based Generalized Coherence Factor for Handheld Ultrasound" Applied Sciences 12, no. 2: 560. https://doi.org/10.3390/app12020560