
A Systematic Approach to Healthcare Knowledge Management Systems in the Era of Big Data and Artificial Intelligence



Abstract
:1. Introduction
2. Background
2.1. Knowledge Management Systems
2.2. Apache Spark and Apache Kafka
2.3. Artificial Intelligence
2.3.1. Decision Trees
2.3.2. Deep-Learning Neural Networks
Faster R-CNN for Prediction
Inception ResNet v2 for Feature Extraction
2.3.3. Evaluation Metrics
3. Proposed Method
3.1. Data Layer
3.2. Information Layer
3.3. Knowledge Layer
3.3.1. Training Phase
3.3.2. Testing Phase
3.4. Process Layer
4. Healthcare Knowledge Management Systems
4.1. High Blood Pressure Diagnosis Support
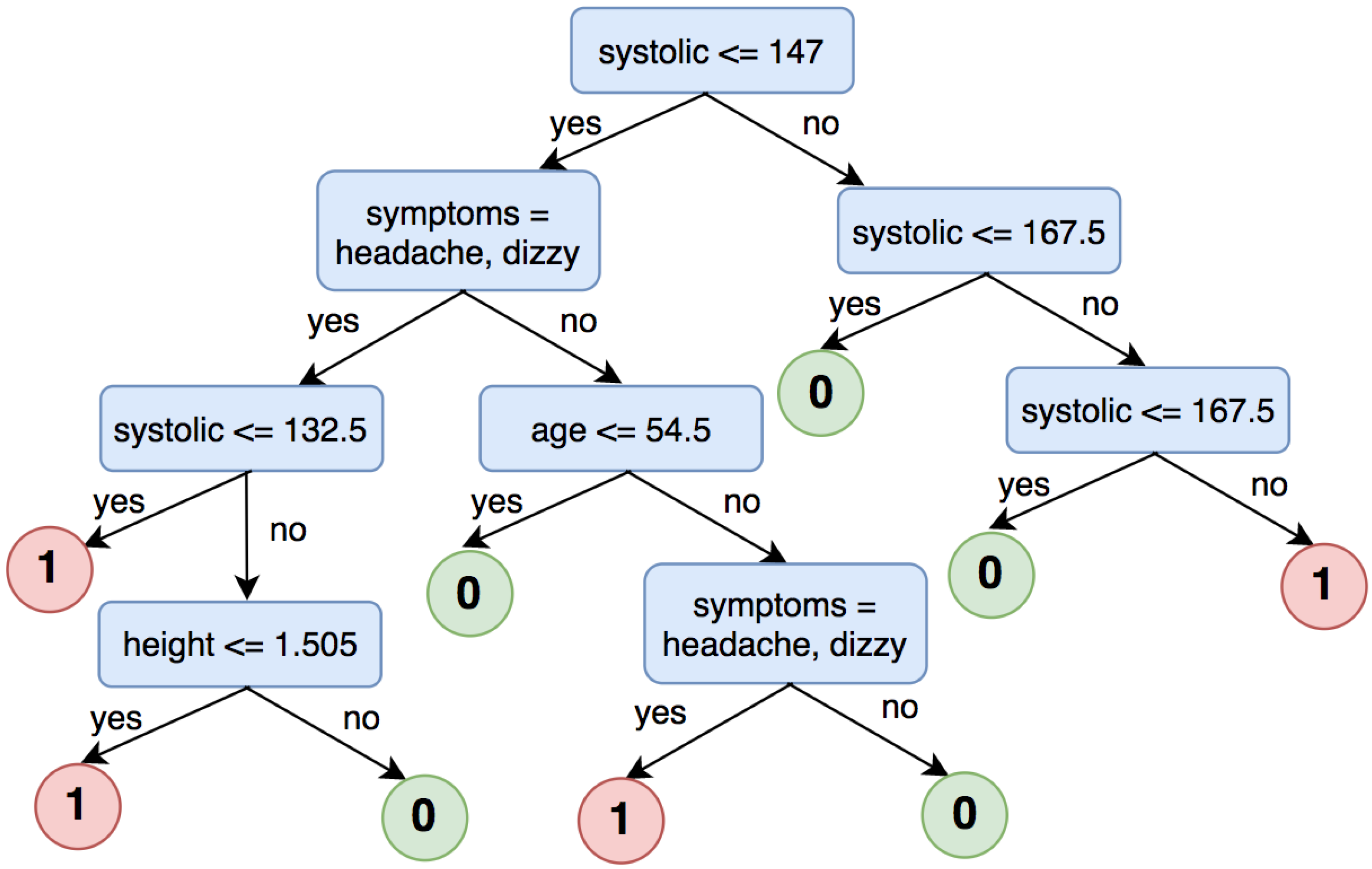
4.1.1. Decision Tree for High Blood Pressure Detection
Training Phase
Testing Phase
4.1.2. Decision Tree for High Blood Pressure Classification
- Label 0: systolic < 120 and diastolic < 80
- Label 1: systolic ≥ 120 and diastolic ≥ 80
- Label 2: systolic ≥ 140 and diastolic ≥ 90
- Label 3: systolic ≥ 160 and diastolic ≥ 100
4.1.3. Application
4.2. Brain Hemorrhage Diagnosis Support
4.2.1. Training Phase
4.2.2. Testing Phase
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Premier Healthcare Database being used by National Institutes of of Health to Evaluate Impact of COVID-19 on Patients Across the U.S. 2020. Available online: https://www.premierinc.com/newsroom/press-releases/premier-healthcare-database-being-used-by-national-institutes-of-health-to-evaluate-impact-of-covid-19-on-patients-across-the-u-s (accessed on 20 March 2022).
- Chung, B.I.; Leow, J.J.; Gelpi-Hammerschmidt, F.; Wang, Y.; Del Giudice, F.; De, S.; Chou, E.P.; Song, K.H.; Almario, L.; Chang, S.L. Racial disparities in postoperative complications after radical nephrectomy: A population-based analysis. Urology 2015, 85, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Cheung, H.; Wang, Y.; Chang, S.L.; Khandwala, Y.; Del Giudice, F.; Chung, B.I. Adoption of robot-assisted partial nephrectomies: A population-based analysis of US surgeons from 2004 to 2013. J. Endourol. 2017, 31, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.J.; Kim, J.H.; Min, G.E.; Park, H.K.; Li, S.; Del Giudice, F.; Han, D.H.; Chung, B.I. Changing trends in the treatment of nephrolithiasis in the real world. J. Endourol. 2019, 33, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Leidner, D.E. Knowledge management and knowledge management systems: Conceptual foundations and research issues. MIS Q. 2001, 25, 107–136. [Google Scholar] [CrossRef]
- Alavi, M.; Leidner, D. Knowledge management systems: Issues, challenges, and benefits. Commun. Assoc. Inf. Syst. 1999, 1, 7. [Google Scholar] [CrossRef]
- Gallupe, B. Knowledge management systems: Surveying the landscape. Int. J. Manag. Rev. 2001, 3, 61–77. [Google Scholar] [CrossRef]
- Suchanek, F.M.; Weikum, G. Knowledge bases in the age of big data analytics. PVLDB 2014, 7, 1713–1714. [Google Scholar] [CrossRef]
- Begoli, E.; Horey, J. Design principles for effective knowledge discovery from big data. In Proceedings of the 2012 Joint Working IEEE/IFIP Conference on Software Architecture and European Conference on Software Architecture, Helsinki, Finland, 20–24 August 2012; pp. 215–218. [Google Scholar]
- Dong, X.; Gabrilovich, E.; Heitz, G.; Horn, W.; Lao, N.; Murphy, K.; Strohmann, T.; Sun, S.; Zhang, W. Knowledge vault: A web-scale approach to probabilistic knowledge fusion. In Proceedings of the 20th ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, New York, NY, USA, 24–27 August 2014; pp. 601–610. [Google Scholar]
- Tretiakov, A.; Whiddett, D.; Hunter, I. Knowledge management systems success in healthcare: Leadership matters. Int. J. Med. Inform. 2017, 97, 331–340. [Google Scholar]
- Maramba, G.; Coleman, A.; Ntawanga, F.F. Causes of Challenges in Implementing Computer-Based Knowledge Management Systems in Healthcare Institutions: A Case Study of Private Hospitals in Johannesburg, South Africa. Afr. J. Inf. Syst. 2020, 12, 4. [Google Scholar]
- Manogaran, G.; Thota, C.; Lopez, D.; Vijayakumar, V.; Abbas, K.M.; Sundarsekar, R. Big data knowledge system in healthcare. In Internet of Things and Big Data Technologies for Next Generation Healthcare; Springer: Cham, Switzerland, 2017; pp. 133–157. [Google Scholar]
- Le Dinh, T.; Phan, T.C.; Bui, T. Towards an architecture for big data-driven knowledge management systems. In Proceedings of the 22nd Americas Conference on Information Systems (AMCIS 2016), San Diego, CA, USA, 11–14 August 2016; Association for Information Systems: Atlanta, GA, USA, 2016. [Google Scholar]
- Bierly, P.E.; Kessler, E.H.; Christensen, E.W. Organizational learning, knowledge and wisdom. J. Organ. Chang. Manag. 2000, 13, 595–618. [Google Scholar] [CrossRef]
- Le Dinh, T.; Rickenberg, T.A.; Fill, H.G.; Breitner, M.H. Enterprise content management systems as a knowledge infrastructure: The knowledge-based content management framework. Int. J. e-Collab. (IJeC) 2015, 11, 49–70. [Google Scholar] [CrossRef]
- Le Dinh, T.; Van, T.H.; Moreau, É. A Knowledge Management Framework for Knowledge-Intensive SMEs. In Proceedings of the 16th International Conference on Enterprise Information Systems ICEIS (3), Lisbon, Portugal, 27–30 April 2014; pp. 435–440. [Google Scholar]
- Chambers, B.; Zaharia, M. Spark: The Definitive Guide Big Data Processing Made Simple, 1st ed.; O’Reilly Media, Inc.: Newton, MA, USA, 2018. [Google Scholar]
- Singh, P. Natural Language Processing. In Machine Learning with PySpark: With Natural Language Processing and Recommender Systems; Apress: Berkeley, CA, USA, 2019; pp. 191–218. [Google Scholar]
- Kreps, J.; Narkhede, N.; Rao, J. Kafka: A distributed messaging system for log processing. Proc. NetDB 2011, 11, 1–7. [Google Scholar]
- Gates, M. Machine Learning: For Beginners—Definitive Guide For Neural Networks, Algorithms, Random Forests and Decision Trees Made Simple; CreateSpace Independent Publishing Platform: North Charleston, SC, USA, 2017. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster r-cnn: Towards real-time object detection with region proposal networks. In Proceedings of the 28th International Conference on Neural Information Processing Systems, Montreal, QC, Canada, 7–12 December 2015; pp. 91–99. [Google Scholar]
- Girshick, R. Fast r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Washington, DC, USA, 7–13 December 2015; pp. 1440–1448. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017. [Google Scholar]
- American Heart Association. What Is High Blood Pressure? South Carolina State Documents Depository: Washington, DC, USA, 2017; pp. 1–2. [Google Scholar]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ly, N.L.; Dong, V.H. Brain Injury; Medical Publishing House: HaNoi, Vietnam, 2013. [Google Scholar]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Systolic | Diastolic |
|---|---|---|
| Normal | <120 | and <80 |
| Prehypertension | 120–139 | or 80–89 |
| Stage 1 hypertension | 140–159 | or 90–99 |
| Stage 2 hypertension | ≥160 | or ≥100 |
| Symptoms | Diagnosis | Label | Index | Symptoms Classification | Features |
|---|---|---|---|---|---|
| Headache, vomit | Intracranial injury | 0 | 194 | (25,152, [194], [1.0]) | (25,163, [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 205], [17.0, 100.0, 60.0, 80.0, 18.0, 1.57, 22, 53, 48.0, 37.0, 1.0]) |
| Fiver | Chickenpox | 0 | 7 | (25,152, [7], [1.0]) | (25,163, [0, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 18], [1.0, 36.0, 140.0, 60.0, 78.0, 20.0, 1.7, 39, 68, 50.0, 39.0, 1.0]) |
| Tired | Hypertension | 1 | 1 | (25,152, [1], [1.0]) | (25,163, [0, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 12], [49.0, 210.0, 140.0, 104.0, 22.0, 1.73, 40, 55, 80.0, 37.0, 1.0]) |
| Abdominal pain | Acute appendicitis | 0 | 0 | (25,152, [0], [1.0]) | (25,163, [0, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11], [23.0, 110.0, 70.0, 87.0, 20.0, 1.46, 40.0, 50.0, 40.0, 37.0, 1.0]) |
| Dizzy | Vestibular dysfunction; Hypertension | 1 | 4 | (25,152, [4], [1.0]) | (25,163, [0, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15], [1.0, 53.0, 170.0, 100.0, 84.0, 18.0, 1.5, 42, 55, 50.0, 37.0, 1.0]) |
| Matter | Density (HU) |
|---|---|
| Air | −1000 |
| Water | 0 |
| White matter | 20 |
| Gray matter | 35–40 |
| Hematoma | 40–90 |
| Bone | 1000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phan, A.-C.; Phan, T.-C.; Trieu, T.-N. A Systematic Approach to Healthcare Knowledge Management Systems in the Era of Big Data and Artificial Intelligence. Appl. Sci. 2022, 12, 4455. https://doi.org/10.3390/app12094455
Phan A-C, Phan T-C, Trieu T-N. A Systematic Approach to Healthcare Knowledge Management Systems in the Era of Big Data and Artificial Intelligence. Applied Sciences. 2022; 12(9):4455. https://doi.org/10.3390/app12094455
Chicago/Turabian StylePhan, Anh-Cang, Thuong-Cang Phan, and Thanh-Ngoan Trieu. 2022. "A Systematic Approach to Healthcare Knowledge Management Systems in the Era of Big Data and Artificial Intelligence" Applied Sciences 12, no. 9: 4455. https://doi.org/10.3390/app12094455