Abstract
This is a prospective study that has been done to assess the lumbar sagittal alignment of patients positioned prone over an adjustable hinged carbon fiber operating table. The following three variations of table position have been considered: neutral, 20° convex, and 20° concave bending. A total of 33 patients who underwent lumbar disc herniation and lumbar canal stenosis surgery were enrolled. Patients who presented with spinal deformity akin to lumbar scoliosis or spondylolisthesis were excluded. For the surgical procedure, following the induction of endotracheal general anesthesia, patients were positioned prone on the adjustable hinged carbon fiber operating table. Radiographs of the lateral view of the lumbar spine were acquired for the three table positions, i.e., neutral, 20° convex, and 20° concave. The lumbar lordosis was measured on radiographs. The lumbar lordosis presented divergently in all three variations of the table (p < 0.01): 45.2 ± 11.0° in neutral; 52.0 ± 10.7° in 20° lumbar extension bending; and 35.9 ± 10.8° in 20° lumbar flexion bending. The efficacy of table bending was 46.5% in convex and 34.0% in concave bending. In conclusion, the lumbar lordosis in three different table positions were 35.9° in 20° convex bending, 45.2° in neutral, and 52.0° in concave bending. The efficacy of table bending was 46.5% in convex and 34.0% in concave bending.
1. Introduction
The alignment of the lumbar spine is of foremost importance to perform spinal surgery. For lumbar decompression surgery, it is a key to create a wider interlaminar window to remove ligamentum flavum or approach to the disc space in lumbar flexed position []. However, spinal deformity surgery needs to create adequate lumbar lordosis to obtain excellent surgical results [,]. To achieve these aims, the table bending angle should decrease or increase lumbar lordosis during decompression and instrumentation, respectively []. An adjustable hinged carbon fiber operating table (AHCFOT) is widely utilized to achieve this. This table allows surgeons to manipulate lumbar curve during prone spinal surgery []
Tan demonstrated the effect of various tables and patient positioning on making changes in lumbar lordosis during surgery []. While using the various frames such as the Andrews spine frame or the Hasting spine frame a marked reduction in lumbar lordosis occurred, which has specific clinical relevance []. The AHCFOT allows surgeons to manipulate lumbar lordosis during spine surgery by offering a bending mechanism by specific degree via remote control [,]. The AHCFOT allows for an arc of motion, from flexion to extension, in the lumbar curvature, without exerting impact on the overall lumbar lordosis beyond physiological levels [,].
Lumbar spinal alignment in both sagittal and coronal planes is of prime significance, and the repercussions of surgical correction over the physiological factors cannot be overemphasized. The authors reported a quantitative study of lateral table bending effects in patients with lateral decubitus position []. However, there is only one quantitative study to evaluate the table bending effect for lumbar lordosis []. The focus of this research is observation of the distinct changes in the lordosis of lumbar spine in three critical positional variations of a hinged operating table, while the patient is positioned in: neutral, 20° convex (lumbar flexion), and 20° concave (lumbar extension).
2. Materials and Methods
The ethics committee of our institution approved this research (No. 354). Informed consent, which was required, was duly sought from the patients.
2.1. Patient Selection
In the time period from January 2020 to December 2021, a cohort of 33 patients (22 men and 11 women, with mean age of 67.0 years) who were admitted to the hospital to undergo surgery for lumbar disc herniation or lumbar canal stenosis were included in our study (Table 1). Patients with diffuse idiopathic skeletal hyperostosis, spinal fracture, malignancy, and deformity such as lumbar scoliosis (Cobb angle > 10°) or spondylolisthesis were excluded. Procedural methods as described were carried out in compliance with relevant guidelines and regulations.

Table 1.
Patient demographic.
2.2. Outcomes of Measurements’ Data
After the pre-surgical general anesthetic induction, patients were positioned in the prone posture on the adjustable hinged carbon fiber operating table (AHCFOT) (Mizuho OSI, Union City, CA, USA; Figure 1). Radiographs of the lateral view of lumbar spine were obtained for three table positional variations: neutral, 20° convex (lumbar flexion), and 20° concave (lumbar extension). The sagittal lumbar alignment (lumbar lordosis) was measured from L1 to S1, on the obtained radiographs (Figure 2). Lumbar lordosis was measured by two senior spine surgeons by Clinical Intelligence Technology & Architecture (CITA) (Fujifilm Corporation, Tokyo, Japan) and mean lumbar lordosis was taken. Change in the lumbar lordosis was calculated from the neutral position to 20° convex bending and from the neutral position to 20° concave bending. The effective divergence of motion was calculated, as well as the value between the neutral position and 20° convex/concave bending. The efficacy of bed bending was calculated by the value of effective range of motion/bed bending angle 20°.

Figure 1.
Adjustable hinged carbon fiber operating table. (A): Lateral image, (B): Controller.
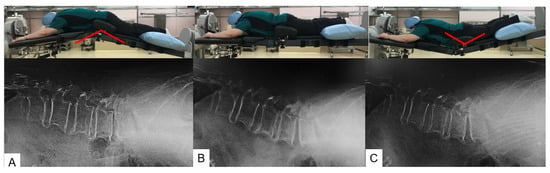
Figure 2.
Hinged carbon operating table bending. (A): 20° convex (lumbar flexion), (B): Neutral, (C): 20° concave (lumbar extension).
2.3. Statistical Analysis
Standard deviation (SD) and mean (M) of the angle of lumbar lordosis in the mentioned critical positions of the table were noted and analyzed. All the data gathered were processed for normality by the Shapiro–Wilk test. A two-way analysis of variance (ANOVA) was implied to compare the angle of lumbar lordosis in the three positional variations of the table. A two-tailed t-test was employed to collate the changes in angles and effectual divergence of motion, from neutral, 20° to the right, and 20° to the left in flexed positions of the table. Amongst men and women, analysis was performed using SPSS (version 19.0; IBM).
3. Results
A significant difference in prone lumbar lordosis for the three positions (p < 0.01) was noted: 35.9 ± 10.8° (range, 14–57) for the 20° convex (lumbar flexion) position, 45.2 ± 11.0° (range, 26–70) for the neutral position, and 52.0 ± 10.7° (range, 31–76) for the 20° concave (lumbar extension) position (Table 2, Figure 3). There was no significant difference of lumbar angles between male and female. Interrater agreement (Kappa coefficients for interrater reliability) in this study was 0.68 and is considered acceptable.
Table 2.
Lumbar lordosis in three different positions.
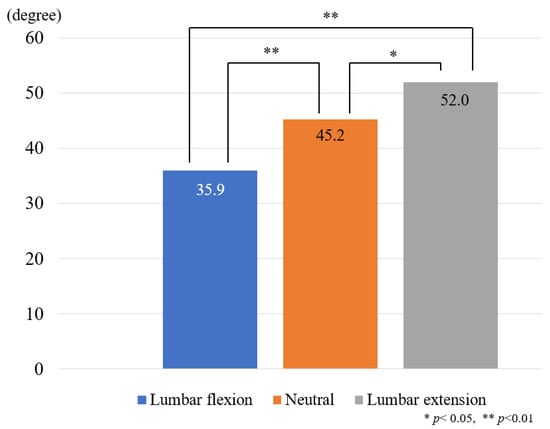
Figure 3.
Lumbar lordosis in three variant positions of the table.
The change in lumbar angle and the efficacy of bed bending are shown in Table 3. The efficacy of table bending in lumbar flexion position and extension position were 46.5% and 33.9%, respectively. Table flexion position in this table was significantly more effective than table extension position (p < 0.001) (Figure 4).
Table 3.
The change in lumbar lordosis and the efficacy of table bending.
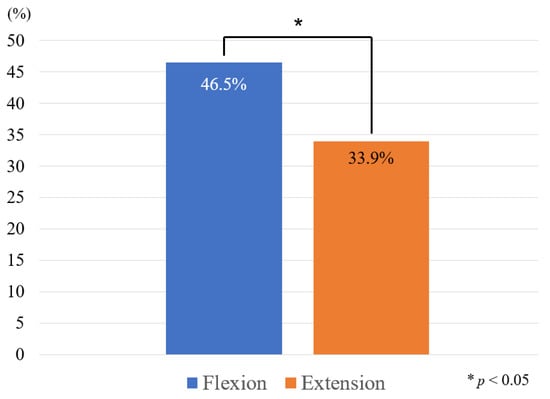
Figure 4.
Efficacy of table bending.
Case Presentation
- Case 1 75-year-old man, L4 degenerative spondylolisthesis
The patient underwent L4-5 OLIF because of low back pain and left sciatica (Figure 5).
- Case 2 72-year-old woman, adult spinal deformity

Figure 5.
75-year-old man, L4 degenerative spondylolisthesis, L4/5 oblique lumbar interbody fusion. (A): Preoperative anteroposterior radiogram, (B): Preoperative lateral radiogram (L4–5 local lordosis 8 degrees), (C): Postoperative anteroposterior radiogram, (D): Postoperative anteroposterior radiogram (L4–5 local lordosis 19 degrees).
The patient underwent T10-pelvis fixation because of low back pain and gait disturbance (Figure 6).
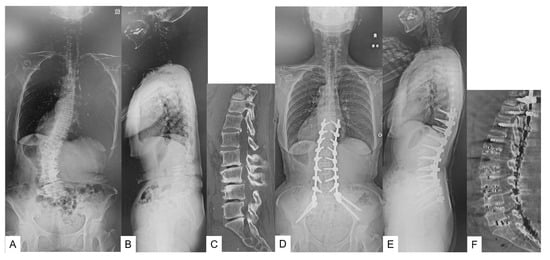
Figure 6.
72-year-old woman, adult spinal deformity, T10 pelvis fixation. (A): Preoperative anteroposterior radiogram, (B): Preoperative lateral radiogram (sagittal vertical axis 83 mm, lumbar lordosis 7 degrees, pelvic tilt 39 degrees), (C): Preoperative CT, (D): Postoperative anteroposterior radiogram, (E): Postoperative anteroposterior radiogram (sagittal vertical axis 0 mm, lumbar lordosis 46 degrees, pelvic tilt 24 degrees), (F): Postoperative CT.
4. Discussion
During lumbar surgeries—oblique lumbar inter-body fusion and direct lumbar inter-body fusion to name two—the patient must be positioned in a lateral decubitus position. Bending the AHCFOT to a convex 20° flexion makes it easier to open and access the desired disc space to perform lumbar interbody fusion []. In spite of providing flexibility in terms of patient position, the efficacy of table bending on sagittal alignment remains unclear.
In our study we have demonstrated the efficacy of 20° convex and concave AHCFOT bending on lumbar sagittal alignment. We found that the lordosis of the lumbar spine on AHCFOT in neutral position is 45.2 ± 11.0°. Average lumbar lordosis achieved in 20° convex bending (lumbar flexion) is 35.9 ± 10.8° and in 20° concave bending (lumbar extension) is 52.0 ± 10.7°. This elucidates that a significant corrective range of lumbar sagittal motion can be acquired by positioning the patients over a AHCFOT.
We found the 20° convex and 20° concave table bending efficacy to be 46.5% and 33.9%, respectively. These results provide better helps to predict lumbar lordosis. A previous AHCFOT study has shown a significant difference in coronal alignment between men and women, possibly due to high body mass index, joint laxity, muscle strength []. However, there was not a significant difference in sagittal alignment amongst men and women in our study. This is most likely due to the bending forces acting on coronal versus sagittal alignment on the facet joints.
In patients presenting with spondylolisthesis, during spine surgeries such as posterior lumbar inter-body fusion (PLIF), transforaminal lumbar inter-body fusion (TLIF), efficacy data of AHCFOT bending could be useful to achieve adequate lumbar lordosis []. No difference was found while performing short segment PLIF with different operating tables and patient positioning []. But in their study, they used a non-hinged conventional operating table. It is imperative that one should keep in mind that segmental loss of lordosis, at the spine levels being operated, in short segment fusions, may lead to compensatory hyper-lordosis at the adjacent levels and a possible accelerated degeneration []. Still, the long-term outcomes of positioning the patient on AHCFOT and lumbar lordosis achieved intraoperatively are not reported. In elderly patients with adult spinal deformity, deformity correction surgery has helped in relieving pain and improving functions []. For surgical management to correct the deformity and create adequate lumbar lordosis, one has to do all anterior and posterior release surgery, in situ rod bending, and preoperative patient positioning depending on severity of deformity [,]. According to our results, the surgeons can create an additional 6.8° lumbar lordosis by table bending alone.
Our research does have a few limitations, one of them being a small cohort size. A larger cohort size would lead to more accurate and predictive results. Also, patients enrolled in this study were average elderly patients. Because of that, they had more degenerative changes, so that little arc of motion on the flexible table has been achieved. We also did not consider the disc degeneration, analysis of segmental lordosis, whether the foraminal area changed or not. In this study, clinical relevance was not evaluated.
5. Conclusions
The lumbar lordosis in three different table positions were 35.9° in 20° convex bending, 45.2° in neutral, and 52.0° in 20° concave bending. The efficacy of table bending was 46.5% in convex and 34.0% in concave bending.
Author Contributions
M.T.: conceptualization, supervision; D.D.: writing—review and editing; Y.F. writing—original draft; S.A.: data collection; K.L. data collection; N.S. preparation, methodology; W.L.: data collection; Y.K. data collection; Y.M. data collection; T.Y.: data collection; D.D.: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This study received funding from Japan Organization of Occupational Health and Safety (No. 2021-32).
Institutional Review Board Statement
This study was conducted in compliance with the guidelines of the Declaration of Helsinki and approved by the institutional review boards at Okayama Rosai Hospital (approval No. 354, 13 June 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available in the article.
Acknowledgments
This study was supported by Okayama Spine Group.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Mouradian, W.H.; Simmons, E.H. A frame for spinal surgery to reduce intra-abdominal pressure while continuous traction is applied. J. Bone Jt. Surg. Am. 1977, 59, 1098–1099. [Google Scholar] [CrossRef]
- Girod, P.P.; Kögl, N.; Molliqaj, G.; Lener, S.; Hartmann, S.; Thomé, C. Flexing a standard hinge-powered operating table for lumbosacral three-column osteotomy (3-CO) site closure in 84 consecutive patients. Neurosurg. Rev. 2022, 45, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Relton, J.E.; Hall, J.E. An operation frame for spinal fusion. A new apparatus designed to reduce haemorrhage during operation. J. Bone Jt. Surg. Br. 1967, 49, 327–332. [Google Scholar] [CrossRef]
- Tan, S.B.; Kozak, J.A.; Dickson, J.H.; Nalty, T.J. Effect of operative position on sagittal alignment of the lumbar spine. Spine (Phila Pa 1976) 1994, 19, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.E.B.; Hunt, M.A.; Martin, C.T.; Polly, D.W. Controlled Pedicle Subtraction Osteotomy Site Closure Using Flexible Hinge-Powered Operating Table. Oper. Neurosurg. (Hagerstown) 2019, 17, E214–E218. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.T.; Jones, K.E.; Polly, D.W., Jr. The Deformity TLIF: Bilateral Facetectomy and Osteotomy Closure with a Hinged Table. Iowa Orthop. J. 2019, 39, 81–84. [Google Scholar] [PubMed]
- Sebastian, A.S.; Ahmed, A.; Vernon, B.; Nguyen, E.C.; Aleem, I.; Clarke, M.J.; Currier, B.L.; Anderson, P.; Bydon, M.; Nassr, A. Effect of an Adjustable Hinged Operating Table on Lumbar Lordosis During Lumbar Surgery. Spine (Phila Pa 1976) 2018, 43, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Nelson, L.M.; McManus, A.C.; Jackson, R.P. The effect of operative position on lumbar lordosis. A radiographic study of patients under anesthesia in the prone and 90-90 positions. Spine (Phila Pa 1976) 1995, 20, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Tanaka, M.; Fujiwara, Y.; Uotani, K.; Yamauchi, T.; Yorimitsu, M.; Yokoyama, Y.; Sonawane, S. Effect of an Adjustable Hinged Carbon Fiber Operating Table on the Coronal Alignment of the Lumbar Spine During Oblique Lateral Interbody Fusion. World Neurosurg. 2021, 149, e958–e962. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, J.H.; Yoon, K.S.; Kang, S.B.; Jo, C.H. Effect of intraoperative position used in posterior lumbar interbody fusion on the maintenance of lumbar lordosis. J. Neurosurg. Spine 2008, 8, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Dekutoski, M.B.; Schendel, M.J.; Ogilvie, J.W.; Olsewski, J.M.; Wallace, L.J.; Lewis, J.L. Comparison of in vivo and in vitro adjacent segment motion after lumbar fusion. Spine (Phila Pa 1976) 1994, 19, 1745–1751. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jia, Y.; Peng, Z.; Qin, Y.; Wang, G. Surgical versus Nonsurgical Treatment for Adult Spinal Deformity: A Systematic Review and Meta-Analysis. World Neurosurg. 2022, 159, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Fujiwara, Y.; Uotani, K.; Maste, P.; Yamauchi, T. C-Arm-Free Circumferential Minimally Invasive Surgery for Adult Spinal Deformity: Technical Note. World Neurosurg. 2020, 143, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y. Surgical treatment for adult spinal deformity: Conceptual approach and surgical strategy. Spine Surg. Relat. Res. 2017, 1, 56–60. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).