Appendix A
Appendix A.1. Survey
In the context of the Master’s Dissertation entitled “Building Sustainability Assessment Methods for Healthcare–critical comparative analysis to apply in Brazilian context”, the questionnaire was formulated representing a proposal to develop an indicators structure based on international rating systems (LEED v4 for Building Design and Construction, BREEAM New Construction, and Healthcare Building Sustainability Assessment tool–Portugal).
The survey aims to check the sustainability level of hospitals in Brazil. The objective of the evaluation is to contribute to the applicability of the indicator to a broader context, making it more reliable and robust for practical applications and contributing to the development of the measurement of the Sustainable Assessment Method for Healthcare Buildings. This evaluation is carried out through the expert’s judgment using specific criteria divided into categories: Environmental, Sociocultural and Functional, Economy, Technical, and Site.
The answers will be critical to the credibility of the final results and should be given the most genuine opinions on all the questions presented. All data processing will be performed for the Dissertation mentioned, respecting their anonymity and confidentiality.
The estimated time to complete the survey is 20 min.
Thank you in advance for your cooperation!
1. To identify the individual expectations of each involved, identify the group to which they belong. If you belong to more than one of the groups listed, please select as many options as necessary.
1.1. Occupation or position currently held (choose one or more of the following):
• Architect
![Applsci 13 03807 i001]()
With less than five years of experience
![Applsci 13 03807 i001]()
With over five years of experience
![Applsci 13 03807 i001]()
With experience in hospital projects
• Civil engineer
![Applsci 13 03807 i001]()
With less than five years of experience
![Applsci 13 03807 i001]()
With over five years of experience
![Applsci 13 03807 i001]()
With experience in hospital projects
• Sustainable Construction Consultant/Expert
![Applsci 13 03807 i001]()
With less than five years of experience
![Applsci 13 03807 i001]()
With more than five years of experience
• Hospital Manager
![Applsci 13 03807 i001]()
Facilities and Equipment Services
![Applsci 13 03807 i001]()
Superintendent/Director
![Applsci 13 03807 i001]()
Other, which one?
• Other
![Applsci 13 03807 i001]()
What?
2. Identification
2.1. Area of expertise and project development:
3. The proposed Hospital Building Method is a Design Support that consists of three levels to position the selected assessment criteria. Thus the fifty-seven Indicators presented are grouped into twenty-two Categories, framed into five Areas.
3.1. Considering the following tables show the indicators of each category, define the relative importance that each INDICATOR should present in the statement scale.
The criteria are in the form of statements; the evaluator should verify if each of the statements is consistent with the indicator that is being evaluated through a five-level scale (Likert scale):
1—Not important
2—Slightly important
3—Neutral
4—Important
5—Very important
Appendix A.2. Environmental Area
Total primary energy consumption during the use phase to promote the reduction of energy consumption in healthcare buildings.
Amount of energy produced in the building through renewable sources to reward renewable energy consumption by incorporating systems that enable clean energy. The use of renewable energy allows the reduction of greenhouse gas emissions and other pollutants. It contributes to the conservation of global resources of fossil fuels and the development of technologies that will enable their exploitation, additionally resulting in a reduction in the life cycle costs of the building.
Several beds are available per square meter of the built area to recognise the efficient use of the built space.
Waterproofing Index to promote soil permeability in urban areas to ensure aquifer recharge and decrease peak flow in stormwater drainage systems. The impermeable areas can majorly impact ecosystems as the ground covered by constructions, streets, and other occupations reduces the soil surface available to support natural habitats and perform rainwater absorption. The increased area of impermeable soil has a negative effect on sustainable development, and the most common are nature conservation and the absence of flood control.
Percentage of intervention areas previously contaminated or built to reward the choice of location of these buildings in areas previously contaminated or constructed once. The primary solution to slow the destruction of natural habitats and wildlife they support and prevent the loss of soil suitability is reuse.
Protection of the site’s ecological and natural resources aims to implement measures to preserve the ecological and natural resources of the building construction site. The ecological value is affected by the type of existing flora and fauna and their interactions, the number of different species, vegetation strata, and water courses.
Potential development of the surroundings by rewarding the rehabilitation of deteriorated or/and abandoned surrounding areas. The principle to be adopted when studying the implementation of a building is to minimise the impacts on the ecology of the site or, where possible, contribute to its improvement.
Percentage of the green area occupied by native plants aiming to promote the integration of pre-existing native plants and the planting of local plants in green spaces. Native plants are the ones that belong to a place where they live for many generations, which is different from an introduced plant, which is a specie that resulted from subsequent introductions. The spontaneous plants grow in a community with other species, providing protection and nourishment, but at the same time, they can interfere with the natural habitat, competing with native plants.
Measurements to reduce the production of Solid Construction and Demolition Waste, and a percentage is destined for reuse or recycling to promote the reduction of waste production and reward its recycling.
Percentage of the cost of reused products and materials with recycled content to promote its usage from the construction site or outside, specific for each material type within its components. The reuse of building materials or elements that result from the end of a building’s life cycle consists of using them incorporated into new materials for construction or rehabilitation.
The building’s performance at the level of this parameter is evaluated by the value of the Potential of the Building’s Conditions for Promoting the Separation of Solid Waste (PRSU), which results from criteria related to the indoor and outdoor existing conditions for the deposition and storage of household waste and usually composed of organic material, paper, cardboard, plastic, glass, metals, infectious, pathological, sharps, and chemicals, among others.
The annual volume of water consumed per square meter inside the building aims to promote reducing water consumption, depending on the efficiency of devices and the average consumption patterns. The quality of water supply, drainage and wastewater treatment strongly impact public health. Due to reducing drinking water supplies, as opposed to increasing consumption, it is necessary to take measures to make its use more efficient.
Percentage reduction of drinking water consumption rewarding the use of effluents and systems that reduce the unnecessary consumption of potable water. As a precious resource and quality of life, potable water should be used only for functions that require all its qualities. However, it is currently used in applications that can be satisfied with recycled or lower-quality water.
Separation of contaminated effluents and local wastewater treatment gives space for premises in the building for wastewater treatment and an appropriate contaminated effluent drainage system. Hospital effluents can be classified into household effluents (kitchens, laundries and toilets) and specifically hospital effluents (from analyses, patient care and medicines). Hospital wastewater is classified according to the Generic Recommendations for Hospital Wastewater Management into groups that should be treated appropriately and differentiated according to their category.
Appendix A.3. Sociocultural and functional
The efficiency of natural ventilation indoors promotes the existence of conditions that allow natural ventilation of the interior space of the building to the exclusive detriment of mechanical ventilation. The levels of indoor air renewal must be guaranteed, safeguarding its quality and reducing occupant exposure to indoor pollutants. The primary influence for the natural ventilation is the depth of the floor drawings plans. Also, courtyards and inner courts favour. When natural ventilation strategy is conceived correctly, this can be as effective as a mechanical ventilation system, with all the advantages associated with the fact that there is no power consumption.
Weight the per cent of low Volatile Organic Compounds (VOC) finishing materials aiming the reward of using materials that do not cause occupant health problems. Several studies reveal the connection between high VOC Sick Building Syndrome (SBS) concentrations. Some examples are formaldehyde, benzene, toluene and xylene. Inside the buildings, the primary sources are products derived from wood produced through adhesives and used as solvents in paints mainly based on synthetic, adhesives, carpeting and polyurethane foams. These compounds are often accidentally released into the atmosphere and are responsible for significant environmental impacts.
Average annual thermal comfort level to ensure the conditions within the healthcare providers to meet occupant needs. The thermal environment of the interior spaces has physical and psychological effects on its occupants and is of great importance in building design. When designing a building, creating a microclimate in the interior spaces, despite the weather conditions outside, essentially responds to the needs and expectations of occupants. The climate in Brazil is divided into five sub-types – equatorial, semi-arid, highland tropical, and subtropical – and during much of the year, it is necessary to use a cooling system to maintain indoor temperatures within a comfortable range. This situation explains that most buildings produce large amounts of thermal energy.
This item measures the contribution of natural lighting to the proper lighting of the interior environment by promoting the adoption of criteria to improve the visual comfort of occupants through the appropriate use of natural lighting, which will contribute to the recovery of patients and the reduction of energy consumption inside the building. Natural lighting is one factor in conditioning the environment’s quality. It has to provide a comfortable visual interior environment, through the minimum energy consumption (artificial lighting). The increasing importance of aspects related to the environment, sustainable development and interior comfort, has contributed to natural light’s leading role in the healing process.
The average level of sound insulation aims to promote the option for constructive solutions that improve the acoustic comfort of patients and team works. Considering the problems that noise causes in humans, society must be aware and take necessary measures to preserve the health of building occupants. Thus, those responsible for building design must develop techniques to provide acoustic comfort conditions, creating a suitable environment for the activities developed.
The possibility of room control of temperature and openings (windows) to encourage the installation of systems that guarantee indoor air quality (IAQ) conditions at a reduced level of energy consumption, while preventing the sprawl of diseases. The increasing efficiency of natural ventilation and preventing the solar incidence are linked with the requirements of IAQ and thermal comfort, as well as to the potential for reducing energy consumption.
Proper implementation and orientation of the building, considering the territorial and landscape framing of the place, promoting the quality of the interior environment to promote, and reward a building implementation and orientation that allows the good use of solar radiation in the different heating and cooling stations and the appropriate use of wind for natural ventilation.
To evaluate the existence and accessibility, by users, to activities, living, leisure, and outdoor spaces by aiming for living spaces that provide the well-being of patients and work teams.
The maximisation of the usable floor area inside the building and reduction of the total construction area by promoting the adoption of space design forms and construction solutions that facilitate the optimisation of the construction area, reducing the environmental impacts associated with the floor area, and increasing the efficiency.
The need for spatial solutions that contributes to the versatility of the area, analysing the level of flexibility, allowing the increase in and adaptation to the continuous need for alteration of spatial functions into rewarding the option for a design that promotes the flexibility of spaces, so that it can adapt to different operations according to the diverse needs of everyday life.
Appendix A.4. Economy
The value of initial investment cost per square meter of the total construction area to promote the design of sustainable buildings whose initial investment is at least equivalent to conventional buildings.
The risk of corruption is transversal. Good practices management helps to prevent situations of infractions and, therefore, it is essential to identify the risks of deviation from good practices and their consequences in terms of management. Reducing corruption is necessary for strengthening democratic institutions, promoting relations between citizens and public or private administration, economic development and growth, and the regular functioning of markets. The problem of corruption is associated with many situations, which spoil the functioning of institutions and markets, such as abuse of power, bribery, embezzlement, influence peddling, economic participation in business, and concussion. All of these constitute related crimes, and there is an undue advantage or compensation to be obtained. Sustainable purchase policies aim to identify risks, resources, actions, and responsibilities to mitigate them, as well as the implementation, monitoring, evaluation, and reporting process. The risk can be defined as an event that, if it occurs, will have a negative impact on the achievement of the organisation’s mission and objectives. Missed opportunities can also be considered a risk.
| Corruption Avoiding Plan |
| ID | Description | Evaluation |
| Not Important | Slightly Important | Neutral | Important | Very Important |
| I39 | Sustainable purchase policies | ![Applsci 13 03807 i001]() | ![Applsci 13 03807 i001]() | ![Applsci 13 03807 i001]() | ![Applsci 13 03807 i001]() | ![Applsci 13 03807 i001]() |
Appendix A.5. Technical
Assessment of building systems and components throughout the different life cycle phases to identify a properly planned commissioning process that ensures the proper functioning of all building systems and components.
Adopting a Sustainable Management Plan aims to reward the existence of an Environmental Management System to ensure the design and construction phase lasts throughout the use phase.
Monitor and evaluate infection control by promoting adequate cleaning, disinfection, decontamination, and sterilisation of all areas, equipment, and instruments of the hospital.
The indicator below evaluates measures to ensure occupant safety by limiting the risk of hatching and fire hazards, favour the action of firefighters whenever their intervention is necessary, and provide means for users to initiate combat measures before the firefighter’s arrival.
Assessment of the durability and required level of maintenance of finishing materials and other constituents of building elements to benefit the use of durable materials suitable for their intended use, reducing the complexity and periodicity of maintenance.
Availability and content of the Building’s User Manual by rewarding guidelines for occupants to use it efficiently. Regardless of the design of a building, its efficiency and operating costs are strongly influenced by the daily behaviour of its users. With guidance and access to information, these can best use the systems. On the other hand, malfunctioning can lead to discomfort and operating, and maintenance costs differ from those estimated, resulting in a waste of resources.
Availability and content of the Building’s Maintenance and Management Manual by ensuring the proper maintenance for better use and preservation and increasing its useful life.
The public transport accessibility index aims to promote and value solutions that meet most building users’ travel needs through urban transportation services.
The potential of the building’s sustainable mobility conditions is to provide facilities which encourage building users to travel using low-carbon modes of transport, by stimulating the usage of bicycles and pedestrian accessibility, minimising individual journeys, and using vehicles with less environmental impact.
4. Considering the proposed Method presented above, are there any indicators that still need to be delivered and that you think should be addressed? Which? Justify.
5. Considering the proposed Method presented above, is there any indicator that could be eliminated? Which? Justify.
Comments:
Thanks for the collaboration!




 With less than five years of experience
With less than five years of experience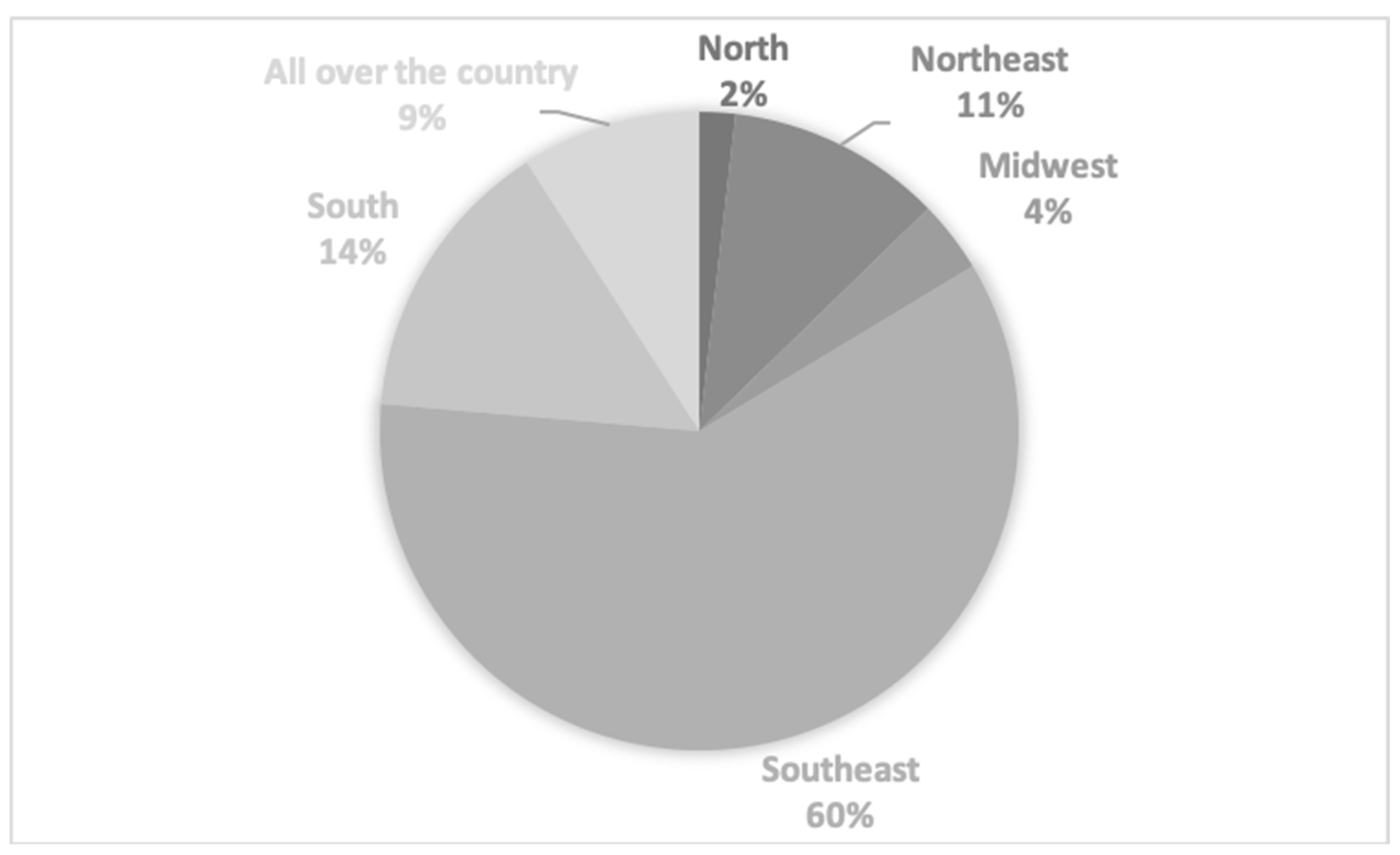




{kind=link}
{kind=link}
{kind=link}
{kind=link}