
Effects of Functional Fatigue Protocol and Visual Information on Postural Control in Patients with Chronic Ankle Instability

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Participants
2.3. Experimental Procedure
2.4. Static Postural Control
2.5. Functional Fatigue Protocol
2.6. Data Analysis
2.7. Statistical Analysis
3. Results
3.1. Static Postural Control
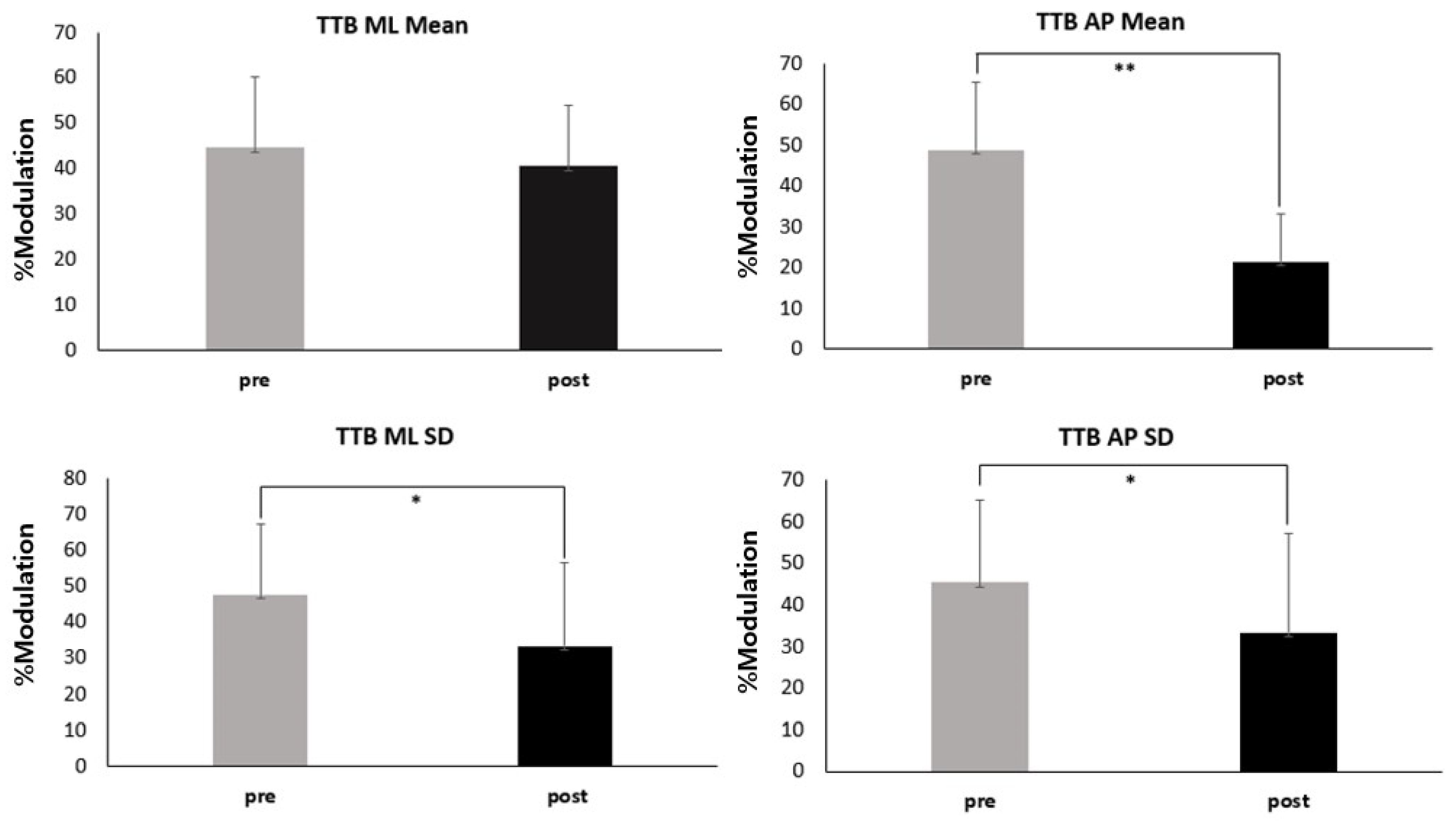
3.2. Visual Reliance
4. Discussion
5. Clinical Implications
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C. The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014, 44, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Herzog, M.M.; Kerr, Z.Y.; Marshall, S.W.; Wikstrom, E.A. Epidemiology of ankle sprains and chronic ankle instability. J. Athl. Train. 2019, 54, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-I.; Houtenbos, S.; Lu, Y.-H.; Mayer, F.; Wippert, P.-M. The epidemiology of chronic ankle instability with perceived ankle instability—A systematic review. J. Foot Ankle Res. 2021, 14, 41. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.L.; Fourchet, F.; Fong, D.; Hertel, J.; Hiller, C.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the international ankle consortium. J. Orthop. Sports Phys. Ther. 2013, 43, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Ha, S.; Chae, S.; Jeong, H.S.; Lee, S.Y. Altered biomechanics in individuals with chronic ankle instability compared with copers and controls during gait. J. Athl. Train. 2022, 57, 760–770. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.A.; Pietrosimone, B.G.; Gribble, P.A. Muscle activation during landing before and after fatigue in individuals with or without chronic ankle instability. J. Athl. Train. 2016, 51, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J. Athl. Train. 2002, 37, 364–375. [Google Scholar] [PubMed]
- Kim, K.-M.; Hart, J.M.; Saliba, S.A.; Hertel, J. Modulation of the fibularis longus Hoffmann reflex and postural instability associated with chronic ankle instability. J. Athl. Train. 2016, 51, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Grooms, D.; Appelbaum, G.; Onate, J. Neuroplasticity following anterior cruciate ligament injury: A framework for visual-motor training approaches in rehabilitation. J. Orthop. Sports Phys. Ther. 2015, 45, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Bleakley, C.M.; Caulfield, B.M.; Docherty, C.L.; Fourchet, F.; Fong, D.T.-P.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; McKeon, P.O.; et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br. J. Sports Med 2016, 50, 1496–1505. [Google Scholar] [CrossRef]
- Winter, D.A.; Patla, A.E.; Prince, F.; Ishac, M.; Gielo-Perczak, K. Stiffness control of balance in quiet standing. J. Neurophysiol. 1998, 80, 1211–1221. [Google Scholar] [CrossRef]
- Wikstrom, E.A.; Naik, S.; Lodha, N.; Cauraugh, J.H. Balance capabilities after lateral ankle trauma and intervention: A meta-analysis. In Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews; Centre for Reviews and Dissemination (UK): York, UK, 2009. [Google Scholar]
- Munn, J.; Sullivan, S.J.; Schneiders, A.G. Evidence of sensorimotor deficits in functional ankle instability: A systematic review with meta-analysis. J. Sci. Med. Sport 2010, 13, 2–12. [Google Scholar] [CrossRef]
- Hiller, C.E.; Nightingale, E.J.; Lin, C.-W.C.; Coughlan, G.F.; Caulfield, B.; Delahunt, E. Characteristics of people with recurrent ankle sprains: A systematic review with meta-analysis. Br. J. Sports Med. 2011, 45, 660–672. [Google Scholar] [CrossRef]
- Song, K.; Burcal, C.J.; Hertel, J.; Wikstrom, E.A. Increased visual use in chronic ankle instability: A meta-analysis. Med. Sci. Sports Exerc. 2016, 48, 2046–2056. [Google Scholar] [CrossRef]
- Holmes, A.; Delahunt, E. Treatment of common deficits associated with chronic ankle instability. Sports Med. 2009, 39, 207–224. [Google Scholar] [CrossRef]
- McKeon, P.O.; Booi, M.J.; Branam, B.; Johnson, D.L.; Mattacola, C.G. Lateral ankle ligament anesthesia significantly alters single limb postural control. Gait Posture 2010, 32, 374–377. [Google Scholar] [CrossRef]
- Knapp, D.; Lee, S.Y.; Chinn, L.; Saliba, S.A.; Hertel, J. Differential ability of selected postural-control measures in the prediction of chronic ankle instability status. J. Athl. Train. 2011, 46, 257–262. [Google Scholar] [CrossRef]
- Song, K.; Rhodes, E.; Wikstrom, E.A. Balance training does not alter reliance on visual information during static stance in those with chronic ankle instability: A systematic review with meta-analysis. Sports Med. 2018, 48, 893–905. [Google Scholar] [CrossRef]
- Kim, K.M. Higher visual reliance during single-leg balance bilaterally occurring following acute lateral ankle sprain: A potential central mechanism of bilateral sensorimotor deficits. Gait Posture 2020, 78, 26–29. [Google Scholar] [CrossRef]
- Gribble, P.A.; Hertel, J.; Denegar, C.R.; Buckley, W.E. The effects of fatigue and chronic ankle instability on dynamic postural control. J. Athl. Train. 2004, 39, 321–329. [Google Scholar]
- Gribble, P.A.; Hertel, J. Effect of lower-extremity muscle fatigue on postural control. Arch. Phys. Med. Rehabil. 2004, 85, 589–592. [Google Scholar] [CrossRef]
- Lane, J.; Bansbach, H.; Connaboy, C.; Darnell, M.; Keenan, K.A.; Lovalekar, M.T.; Nagai, T.; Allison, K.F. The Effect of Loaded Fatigue on Loaded Postural Stability; University of Pittsburgh: Bradford, PA, USA, 2018. [Google Scholar]
- Bizid, R.; Margnes, E.; François, Y.; Jully, J.L.; Gonzalez, G.; Dupui, P.; Paillard, T. Effects of knee and ankle muscle fatigue on postural control in the unipedal stance. Eur. J. Appl. Physiol. 2009, 106, 375–380. [Google Scholar] [CrossRef]
- Gimmon, Y.; Riemer, R.; Oddsson, L.; Melzer, I. The effect of plantar flexor muscle fatigue on postural control. J. Electromyogr. Kinesiol. 2011, 21, 922–928. [Google Scholar] [CrossRef]
- Steib, S.; Zech, A.; Hentschke, C.; Pfeifer, K. Fatigue-induced alterations of static and dynamic postural control in athletes with a history of ankle sprain. J. Athl. Train. 2013, 48, 203–208. [Google Scholar] [CrossRef]
- Reimer, R.C., III; Wikstrom, E.A. Functional fatigue of the hip and ankle musculature cause similar alterations in single leg stance postural control. J. Sci. Med. Sport 2010, 13, 161–166. [Google Scholar] [CrossRef]
- Jones, C.M.; Griffiths, P.C.; Mellalieu, S.D. Training load and fatigue marker associations with injury and illness: A systematic review of longitudinal studies. Sports Med. 2017, 47, 943–974. [Google Scholar] [CrossRef]
- Cortes, N.; Greska, E.; Kollock, R.; Ambegaonkar, J.; Onate, J.A. Changes in lower extremity biomechanics due to a short-term fatigue protocol. J. Athl. Train. 2013, 48, 306–313. [Google Scholar] [CrossRef]
- Martin, R.L.; Irrgang, J.J.; Burdett, R.G.; Conti, S.F.; Van Swearingen, J.M. Evidence of validity for the Foot and Ankle Ability Measure (FAAM). Foot Ankle Int. 2005, 26, 968–983. [Google Scholar] [CrossRef]
- Ross, S.E.; Guskiewicz, K.M.; Gross, M.T.; Yu, B. Assessment tools for identifying functional limitations associated with functional ankle instability. J. Athl. Train. 2008, 43, 44–50. [Google Scholar] [CrossRef]
- Lee, S.C.; Kim, C.Y.; Jeong, H.S.; Lee, S.Y.; Kim, S. Effect of functional fatigue protocol on static and dynamic postural control of lower extremities. Int. J. Appl. Sports Sci. 2018, 29, 603–612. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Kim, H. Lower Extremity Neuromechanics During a Forward-Side Jump Following Functional Fatigue in Patients with Ankle Instability; Brigham Young University: Provo, UT, USA, 2015. [Google Scholar]
- Hertel, J.; Buckley, W.E.; Denegar, C.R. Serial testing of postural control after acute lateral ankle sprain. J. Athl. Train. 2001, 36, 363–368. [Google Scholar]
- van Wegen, E.E.; van Emmerik, R.E.; Wagenaar, R.C.; Ellis, T. Stability boundaries and lateral postural control in Parkinson’s disease. Mot. Control 2001, 5, 254–269. [Google Scholar] [CrossRef]
- Song, K.; Kang, T.K.; Wikstrom, E.A.; Jun, H.-P.; Lee, S.Y. Effects of reduced plantar cutaneous sensation on static postural control in individuals with and without chronic ankle instability. J. Sci. Med. Sport 2017, 20, 910–914. [Google Scholar] [CrossRef]
- Hertel, J.; Olmsted-Kramer, L.C. Deficits in time-to-boundary measures of postural control with chronic ankle instability. Gait Posture 2007, 25, 33–39. [Google Scholar] [CrossRef]
- Hertel, J.; Olmsted-Kramer, L.C.; Challis, J.H. Time-to-boundary measures of postural control during single leg quiet standing. J. Appl. Biomech. 2006, 22, 67–73. [Google Scholar] [CrossRef]
- Wikstrom, E.A.; Song, K.; Pietrosimone, B.G.; Blackburn, J.T.; Padua, D.A. Visual utilization during postural control in anterior cruciate ligament-deficient and–reconstructed patients: Systematic Reviews and Meta-Analyses. Arch. Phys. Med. Rehabil. 2017, 98, 2052–2065. [Google Scholar] [CrossRef]
- Cohen, J. Statistical power analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Thompson, C.; Schabrun, S.; Romero, R.; Bialocerkowski, A.; van Dieen, J.; Marshall, P. Factors contributing to chronic ankle instability: A systematic review and meta-analysis of systematic reviews. Sports Med. 2018, 48, 189–205. [Google Scholar] [CrossRef]
- Gribble, P.A.; Tucker, W.S.; White, P.A. Time-of-day influences on static and dynamic postural control. J. Athl. Train. 2007, 42, 35–41. [Google Scholar]
- Corbin, D.M.; Hart, J.M.; McKeon, P.O.; Ingersoll, C.D.; Hertel, J. The effect of textured insoles on postural control in double and single limb stance. J. Sport. Rehabil. 2007, 16, 363–372. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J. Diminished plantar cutaneous sensation and postural control. Percept. Mot. Skills 2007, 104, 56–66. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J. Spatiotemporal postural control deficits are present in those with chronic ankle instability. BMC Musculoskelet. Disord. 2008, 9, 76. [Google Scholar] [CrossRef]
- Simpson, J.D.; Rendos, N.K.; Stewart, E.M.; Turner, A.J.; Wilson, S.J.; Macias, D.M.; Chander, H.; Knight, A.C. Bilateral spatiotemporal postural control impairments are present in participants with chronic ankle instability. Phys. Ther. Sport 2019, 39, 1–7. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Postural control strategies during single limb stance following acute lateral ankle sprain. Clin. Biomech. 2014, 29, 643–649. [Google Scholar] [CrossRef]
- Koldenhoven, R.M.; Feger, M.A.; Fraser, J.J.; Hertel, J. Variability in center of pressure position and muscle activation during walking with chronic ankle instability. J. Electromyogr. Kinesiol. 2018, 38, 155–161. [Google Scholar] [CrossRef]
- Woods, C.; Hawkins, R.D.; Maltby, S.; Hulse, M.; Thomas, A.; Hodson, A.; Football Association Medical Research Programme. The Football Association Medical Research Programme: An audit of injuries in professional football—Analysis of hamstring injuries. Br. J. Sports Med. 2004, 38, 36–41. [Google Scholar] [CrossRef]
- Gabbett, T.J. Incidence, site, and nature of injuries in amateur rugby league over three consecutive seasons. Br. J. Sports Med. 2000, 34, 98–103. [Google Scholar] [CrossRef]
- Pinto, M.; Kuhn, J.E.; Greenfield, M.L.V.; Hawkins, R.J. Prospective analysis of ice hockey injuries at the Junior A level over the course of one season. Clin. J. Sport Med. 1999, 9, 70–74. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | CAI (n = 28) |
|---|---|
| Age (years) | 24.07 ± 2.62 |
| Height (cm) | 166.87 ± 7.45 |
| Body mass (kg) | 61.81 ± 17.09 |
| Foot length (cm) | 22.96 ± 1.66 |
| Foot width (cm) | 8.86 ± 1.21 |
| Resting heart rate | 95 ± 7.53 |
| IdFAI | 18.26 ± 3.82 |
| FAAM ADL | 79.09 ± 9.34 |
| FAAM Sports | 67.83 ± 11.83 |
| Variables | Value |
|---|---|
| Rep. time (s) | 44.30 ± 7.05 |
| HR | 184.80 ± 6.34 |
| RPE | 17.73 ± 1.35 |
| MVJH (cm) | 39.00 ± 16.46 |
| Eyes Open | Eyes Closed | ANOVA | F | Effect Size (95% CI) | p | |||
|---|---|---|---|---|---|---|---|---|
| Measures (s) | Pre-Fatigue | Post-Fatigue | Pre-Fatigue | Post-Fatigue | ||||
| TTB ML Mean of minima | 3.4 ± 0.76 | 3 ± 0.34 | 1.78 ± 0.46 | 1.74 ± 0.43 | Fatigue Effect | 7.826741 | 0.6 (0.055 to 0.360) | 0.009 |
| Condition Effect | 201.0951 | 0.98 (1.221 to 1.634) | <0.001 | |||||
| Fatigue × Condition Interaction | 7.81124 | 0.009 | ||||||
| TTB AP Mean of minima | 9.99 ± 1.43 | 4.53 ± 0.91 | 4.92 ± 1.1 | 4.79 ± 0.94 | Fatigue Effect | 426.7928 | 0.45 (2.518 to 3.074) | <0.001 |
| Condition Effect | 81.72411 | 0.52 (1.860 to 2.953) | ||||||
| Fatigue × Condition Interaction | 240.4783 | |||||||
| TTB ML SD on minima | 2.9 ± 1.17 | 2.45 ± 1.16 | 1.59 ± 0.83 | 1.56 ± 0.63 | Fatigue Effect | 63.98371 | 0.57 (−0.040 to 0.515) | 0.091 |
| Condition Effect | 2.563906 | 0.96 (0.696 to 1.499) | <0.001 | |||||
| Fatigue × Condition Interaction | 12.21461 | 0.176 | ||||||
| TTB AP SD on minima | 6.11 ± 1.23 | 2.69 ± 0.53 | 3.33 ± 0.94 | 3.19 ± 0.83 | Fatigue Effect | 46.88057 | 0.54 (1.531 to 1.963) | <0.001 |
| Condition Effect | 106.8657 | 0.33 (0.717 to 1.629) | ||||||
| Fatigue × Condition Interaction | 364.4761 | |||||||
| %Modulation | Pre-Fatigue | Post-Fatigue | t | 95% CI | d | p |
|---|---|---|---|---|---|---|
| TTB ML Mean of minima | 44.59 ± 15.64 | 40.52 ± 13.57 | 1.61 | (−0.078 to 0.681) | 0.28 | 0.119 |
| TTB AP Mean of minima | 48.7 ± 16.54 | 21.37 ± 11.65 | 7.604 | (0.899 to 1.962) | 1.91 | <0.001 |
| TTB ML SD on minima | 49.17 ± 18.23 | 34.73 ± 24.66 | 3.033 | (0.168 to 0.969) | 0.66 | 0.05 |
| TTB AP SD on minima | 44.95 ± 20.02 | 22.67 ± 12.83 | 4.441 | (0.401 to 1.266) | 1.33 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Kim, H.; Song, K.; Yoon, S.; Hong, E.J.; Jeon, H.G.; Oh, K.U.; Lee, S.Y. Effects of Functional Fatigue Protocol and Visual Information on Postural Control in Patients with Chronic Ankle Instability. Appl. Sci. 2024, 14, 4445. https://doi.org/10.3390/app14114445
Kim K, Kim H, Song K, Yoon S, Hong EJ, Jeon HG, Oh KU, Lee SY. Effects of Functional Fatigue Protocol and Visual Information on Postural Control in Patients with Chronic Ankle Instability. Applied Sciences. 2024; 14(11):4445. https://doi.org/10.3390/app14114445
Chicago/Turabian StyleKim, Kyungeon, Hyunsoo Kim, Kyeongtak Song, Suji Yoon, Eun Ji Hong, Hyung Gyu Jeon, Kyoung Uk Oh, and Sae Yong Lee. 2024. "Effects of Functional Fatigue Protocol and Visual Information on Postural Control in Patients with Chronic Ankle Instability" Applied Sciences 14, no. 11: 4445. https://doi.org/10.3390/app14114445
APA StyleKim, K., Kim, H., Song, K., Yoon, S., Hong, E. J., Jeon, H. G., Oh, K. U., & Lee, S. Y. (2024). Effects of Functional Fatigue Protocol and Visual Information on Postural Control in Patients with Chronic Ankle Instability. Applied Sciences, 14(11), 4445. https://doi.org/10.3390/app14114445