
Rate of Torque Development Scaling Factor Decreased Following a 6-Week Unilateral Isometric Training Using Electrostimulation or Voluntary Contractions
 , ,
, ,  , , , and
, , , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
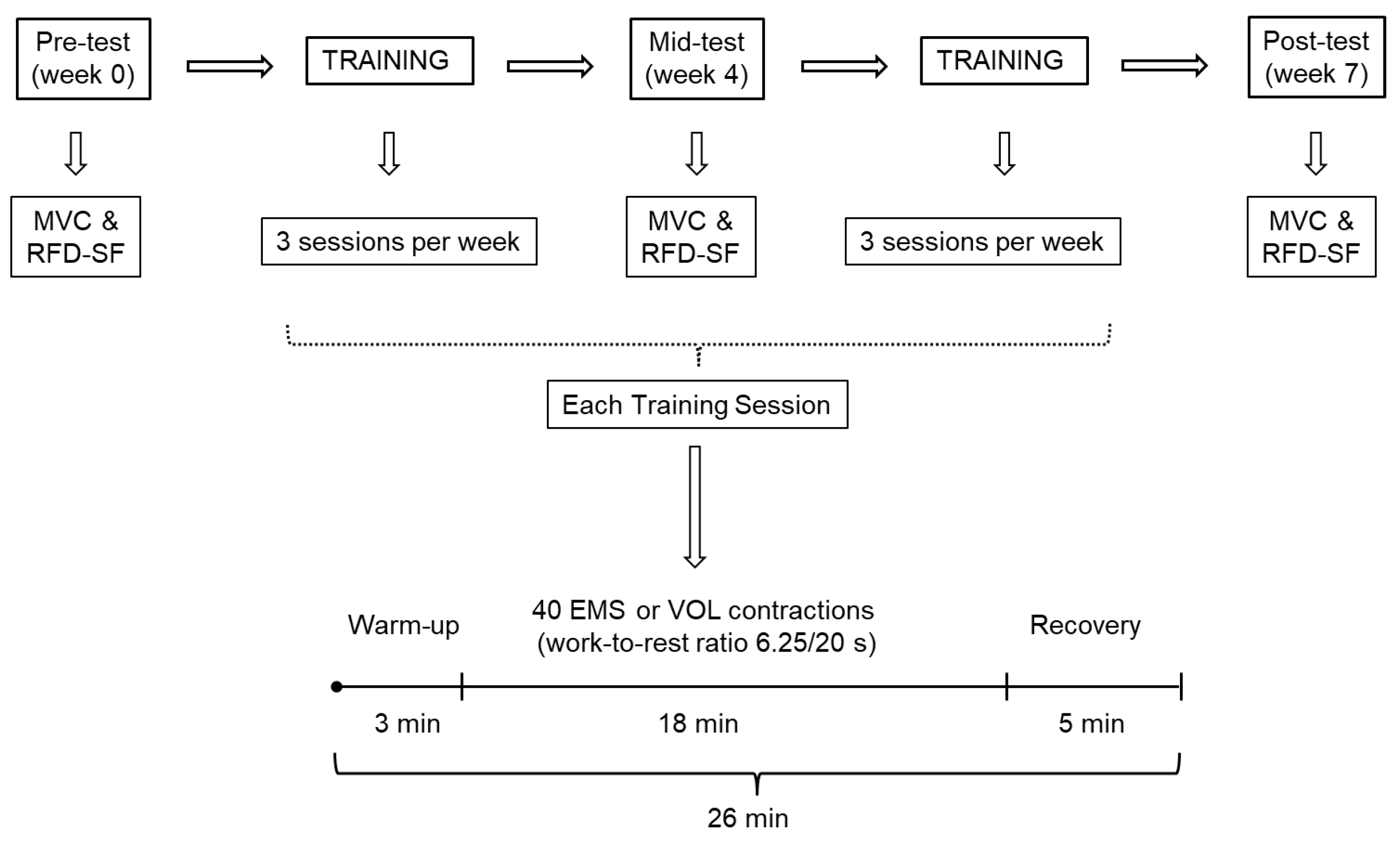
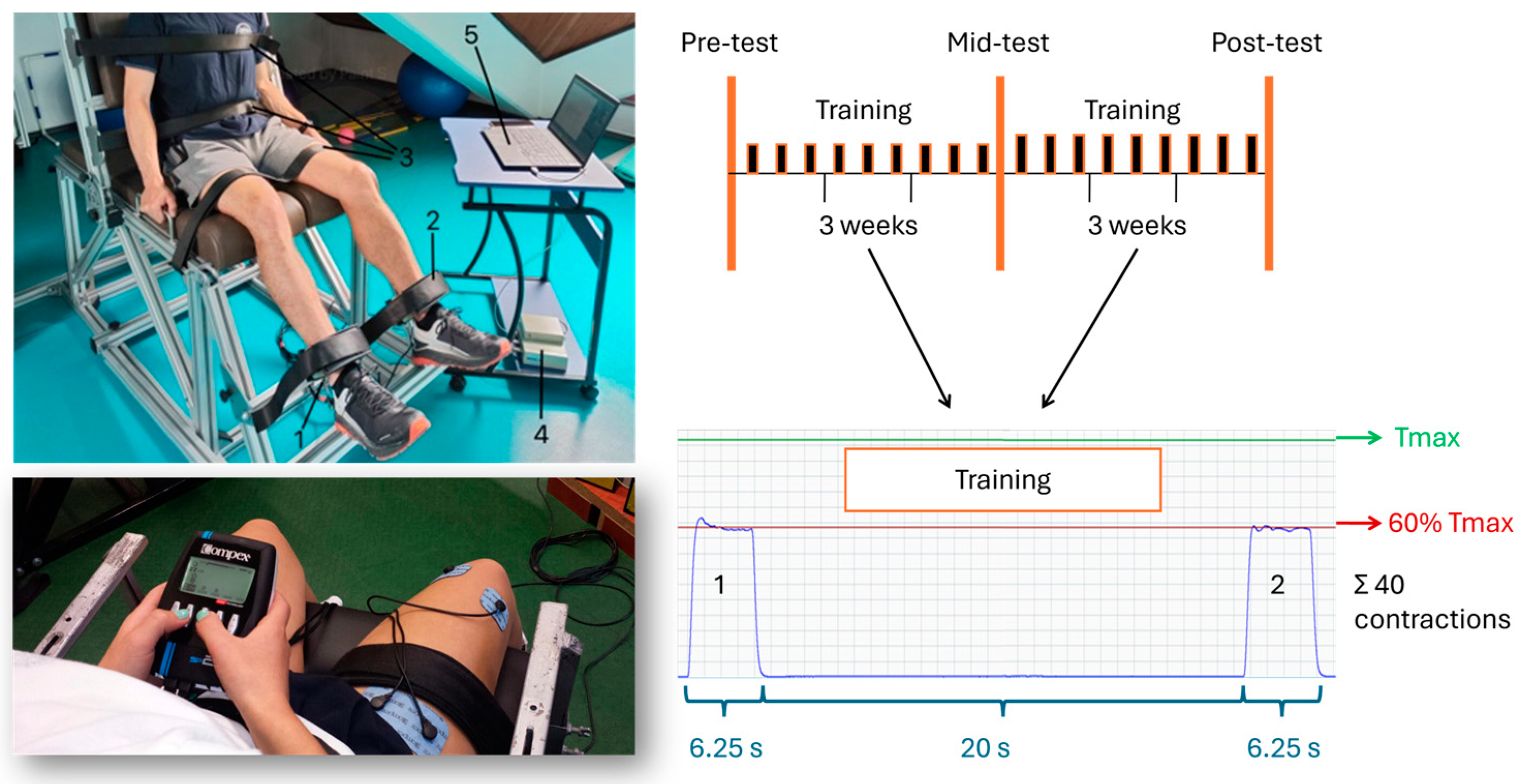
2.1. Study Design
2.2. Subjects
2.3. Testing Procedures
2.4. Training Procedures
2.5. Statistical Analyses
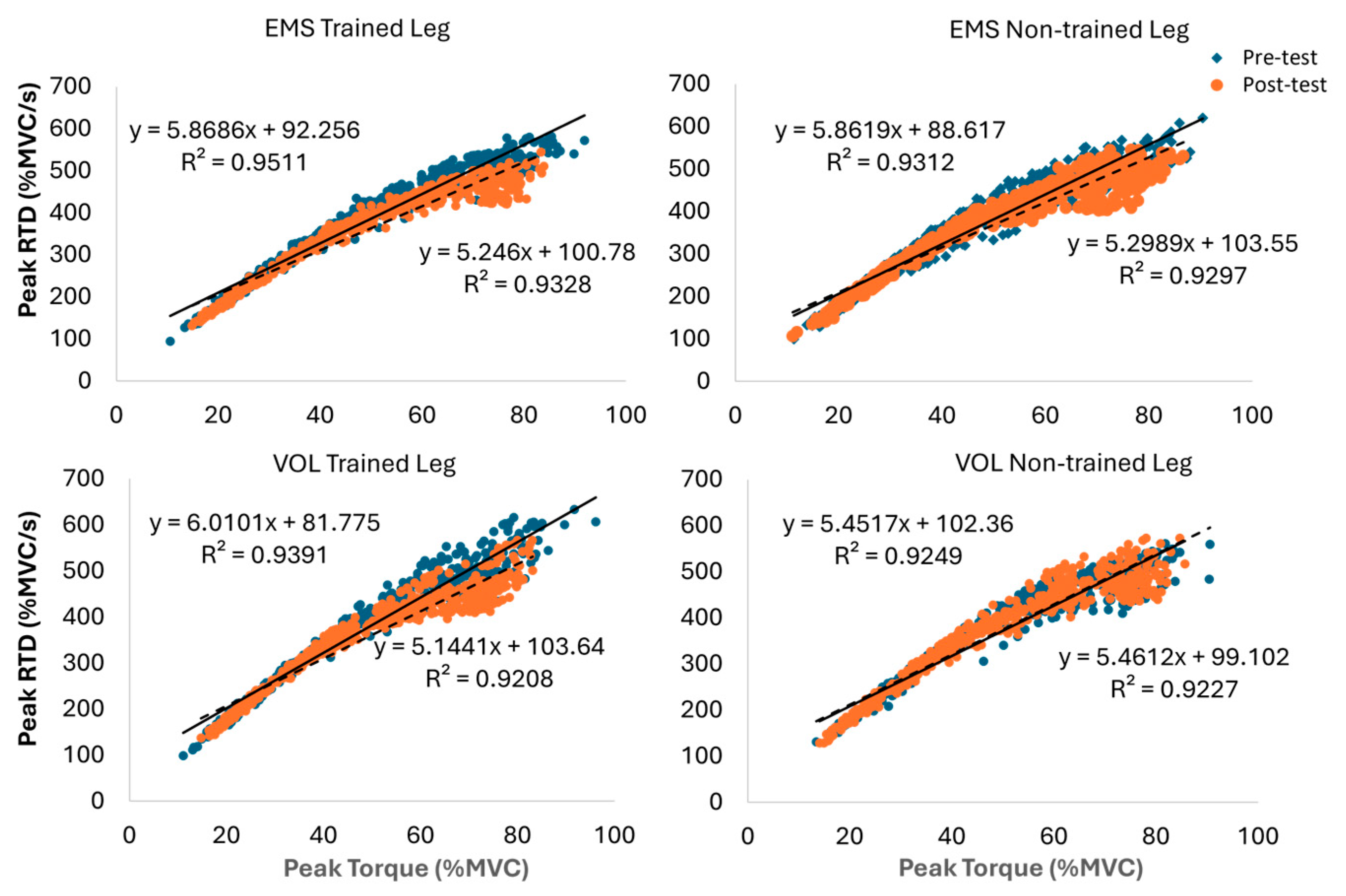
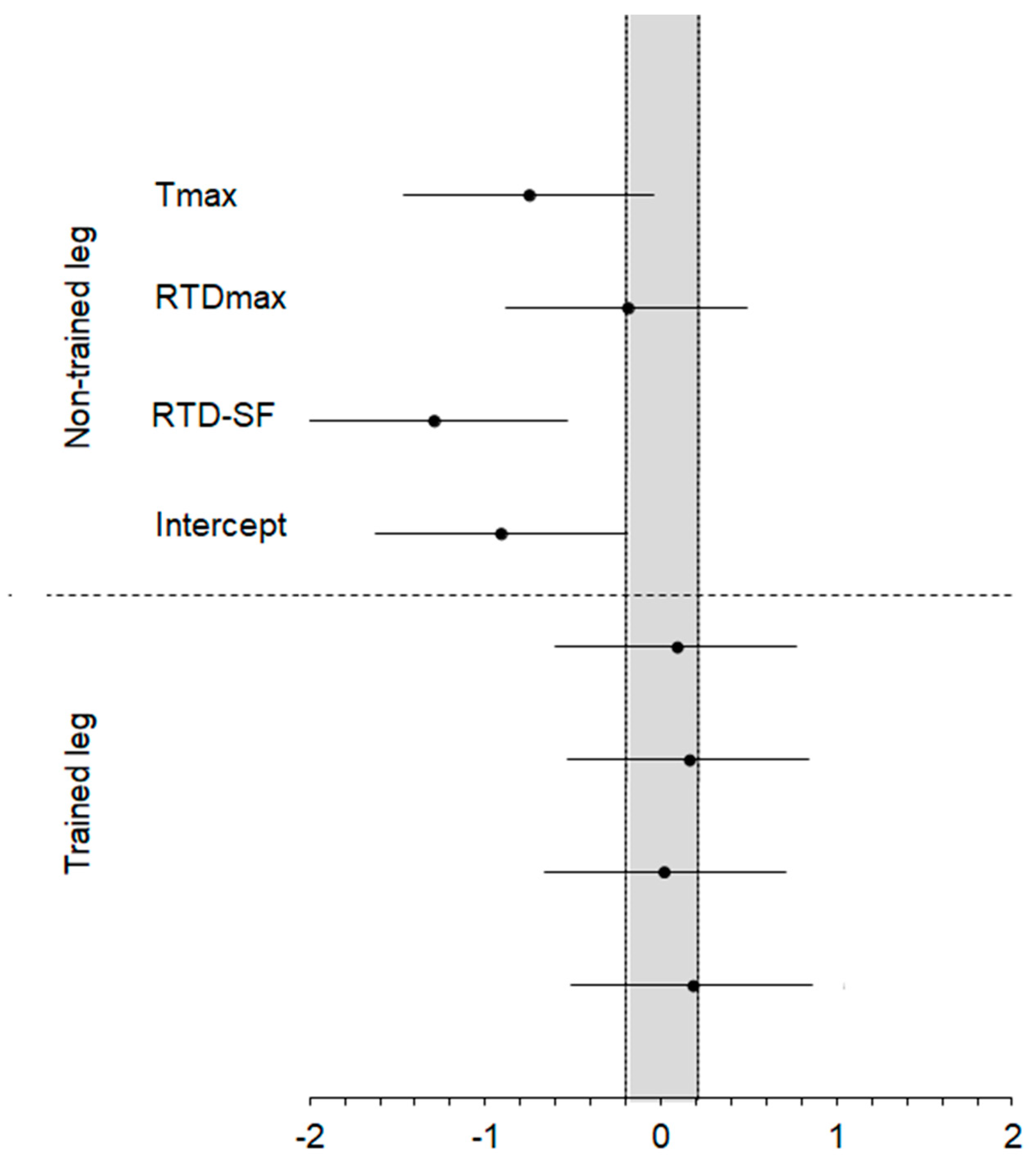
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellumori, M.; Jaric, S.; Knight, C.A. The Rate of Force Development Scaling Factor (RFD-SF): Protocol, Reliability, and Muscle Comparisons. Exp. Brain Res. 2011, 212, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Kozinc, Ž.; Smajla, D.; Šarabon, N. The Rate of Force Development Scaling Factor: A Review of Underlying Factors, Assessment Methods and Potential for Practical Applications. Eur. J. Appl. Physiol. 2022, 122, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, O.M.; Mirkov, D.M.; Kadija, M.; Nedeljkovic, A.; Jaric, S. Asymmetries in Explosive Strength Following Anterior Cruciate Ligament Reconstruction. Knee 2014, 21, 1039–1045. [Google Scholar] [CrossRef]
- Mirkov, D.M.; Knezevic, O.M.; Maffiuletti, N.A.; Kadija, M.; Nedeljkovic, A.; Jaric, S. Contralateral Limb Deficit after ACL-Reconstruction: An Analysis of Early and Late Phase of Rate of Force Development. J. Sports Sci. 2017, 35, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Blazevich, A.J.; Wilson, C.J.; Alcaraz, P.E.; Rubio-Arias, J.A. Effects of Resistance Training Movement Pattern and Velocity on Isometric Muscular Rate of Force Development: A Systematic Review with Meta-Analysis and Meta-Regression. Sports Med. 2020, 50, 943–963. [Google Scholar] [CrossRef] [PubMed]
- Uygur, M.; de Freitas, P.B.; Barone, D.A. Rate of Force Development and Relaxation Scaling Factors Are Highly Sensitive to Detect Upper Extremity Motor Impairments in Multiple Sclerosis. J. Neurol. Sci. 2020, 408, 116500. [Google Scholar] [CrossRef] [PubMed]
- Smajla, D.; Knezevic, O.M.; Mirkov, D.M.; Šarabon, N. Interlimb Asymmetries and Ipsilateral Associations of Plantar Flexors and Knee Extensors Rate-of-Force Development Scaling Factor. Symmetry 2020, 12, 1522. [Google Scholar] [CrossRef]
- Šarabon, N.; Knezevic, M.O.; Mirkov, M.D.; Smajla, D. Introduction of Dynamic Rate-of-Force Development Scaling Factor in Progressive Drop Jumps. J. Biomech. 2020, 110, 109980. [Google Scholar] [CrossRef] [PubMed]
- Casartelli, N.C.; Lepers, R.; Maffiuletti, N.A. Assessment of the Rate of Force Development Scaling Factor for the Hip Muscles. Muscle Nerve 2014, 50, 932–938. [Google Scholar] [CrossRef]
- Mathern, R.M.; Anhorn, M.; Uygur, M. A Novel Method to Assess Rate of Force Relaxation: Reliability and Comparisons with Rate of Force Development across Various Muscles. Eur. J. Appl. Physiol. 2019, 119, 291–300. [Google Scholar] [CrossRef]
- Stefanović, Ž.; Kukić, F.; Knežević, O.M.; Šarabon, N.; Mirkov, D.M. Evaluation of the Reduced Protocol for the Assessment of Rate of Force Development Scaling Factor. Symmetry 2023, 15, 1590. [Google Scholar] [CrossRef]
- Bellumori, M.; Uygur, M.; Knight, C.A. High-Speed Cycling Intervention Improves Rate-Dependent Mobility in Older Adults. Med. Sci. Sports Exerc. 2017, 49, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, T.G.C.; Donato, S.V.S.; Lima, K.C.A.; Uygur, M.; Pereira, R.V.; de Freitas, P.B. Age- And Sex-Related Differences in the Maximum Muscle Performance and Rate of Force Development Scaling Factor of Precision Grip Muscles. Motor Control 2020, 24, 274–290. [Google Scholar] [CrossRef] [PubMed]
- Bellumori, M.; Jaric, S.; Knight, C.A. Age-Related Decline in the Rate of Force Development Scaling Factor. Motor Control 2013, 17, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Boccia, G.; Dardanello, D.; Brustio, P.R.; Tarperi, C.; Festa, L.; Zoppirolli, C.; Pellegrini, B.; Schena, F.; Rainoldi, A. Neuromuscular Fatigue Does Not Impair the Rate of Force Development in Ballistic Contractions of Submaximal Amplitudes. Front. Physiol. 2018, 9, 1503. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, T.; Poulin-Charronnat, B.; Bard, P.; Lepers, R. Effect of Mental Fatigue on Hand Force Production Capacities. PLoS ONE 2024, 19, e0298958. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.L.; Culvenor, A.G.; Juhl, C.B.; Berg, B.; Bricca, A.; Filbay, S.R.; Holm, P.; Macri, E.; Urhausen, A.P.; Ardern, C.L.; et al. OPTIKNEE 2022: Consensus Recommendations to Optimise Knee Health after Traumatic Knee Injury to Prevent Osteoarthritis. Br. J. Sports Med. 2022, 56, 1393–1405. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Maffiuletti, N. Neural Adaptations to Electrical Stimulation Strength Training. Eur. J. Appl. Physiol. 2011, 111, 2439–2449. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Scott, K.; Lambert, J.; Hamilton, G.; Tracy, J. Cross-Education of Muscle Strength Is Greater with Stimulated than Voluntary Contractions. Motor Control 1999, 3, 205–219. [Google Scholar] [CrossRef]
- Zhou, S.; Oakman, A.; Davie, A.J. Effects of Unilateral Voluntary and Electromyostimulation Training on Muscular Strength on the Contralateral Limb. Hong Kong J. Sports Med. Sports Sci. 2002, XIV, 1–11. [Google Scholar]
- Sonnery-Cottet, B.; Saithna, A.; Quelard, B.; Daggett, M.; Borade, A.; Ouanezar, H.; Thaunat, M.; Blakeney, W.G. Arthrogenic Muscle Inhibition after ACL Reconstruction: A Scoping Review of the Efficacy of Interventions. Br. J. Sports Med. 2019, 53, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Colson, S.S.; Martin, A.; Van Hoecke, J. Effects of Electromyostimulation versus Voluntary Isometric Training on Elbow Flexor Muscle Strength. J. Electromyogr. Kinesiol. 2009, 19, e311–e319. [Google Scholar] [CrossRef] [PubMed]
- Filipovic, A.; Kleinode, H.; Dorman, U.; Meste, J. Electromyostimulation-a Systematic Review of the Influence of Training Regimens and Stimulation Parameters on Effectiveness in Electromyostimulation Training of Selected Strength Parameters. J. Strength Cond. Res. 2011, 25, 3218–3238. [Google Scholar] [CrossRef] [PubMed]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation-a Systematic Review of the Effects of Different Electromyostimulation Methods on Selected Strength Parameters in Trained and Elite Athletes. J. Strength Cond. Res. 2012, 26, 2600–2614. [Google Scholar] [CrossRef] [PubMed]
- Natsume, T.; Ozaki, H.; Kakigi, R.; Kobayashi, H.; Naito, H. Effects of Training Intensity in Electromyostimulation on Human Skeletal Muscle. Eur. J. Appl. Physiol. 2018, 118, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- Oakman, A.; Zhou, S.; Davie, A. Cross-Education Effect Observed in Voluntary and Electromyostimulation Strength Training. In Proceedings of the 17 International Symposium on Biomechanics in Sports, Perth, Australia, 30 June–6 July 1999; pp. 401–404. [Google Scholar]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, P.; Dyhre-Poulsen, P. Increased Rate of Force Development and Neural Drive of Human Skeletal Muscle Following Resistance Training. J. Appl. Physiol. 2002, 93, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.L.; Aagaard, P. Influence of Maximal Muscle Strength and Intrinsic Muscle Contractile Properties on Contractile Rate of Force Development. Eur. J. Appl. Physiol. 2006, 96, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Mastalerz, A.; Sadowski, J. The Effect of Unilateral Training on Contralateral Limb Power in Young Women and Men. Biol. Sport 2020, 37, 443. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Carroll, T. Cross Education: Possible Mechanisms for the Contralateral Effects of Unilateral Resistance Training. Sports Med. 2007, 37, 1–14. [Google Scholar] [CrossRef]
- Benito-Martínez, E.; Senovilla-Herguedas, D.; de la Torre-Montero, J.; Martínez-Beltrán, M.; Reguera-García, M.; Alonso-Cortés, B. Local and Contralateral Effects after the Application of Neuromuscular Electrostimulation in Lower Limbs. Int. J. Environ. Res. Public Health 2020, 17, 9028. [Google Scholar] [CrossRef]
- Kadri, M.A.; Noé, F.; Nouar, M.B.; Paillard, T. Effects of Training Programs Based on Ipsilateral Voluntary and Stimulated Contractions on Muscle Strength and Monopedal Postural Control of the Contralateral Limb. Eur. J. Appl. Physiol. 2017, 117, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Gondin, J.; Cozzone, P.; Bendahan, D. Is High-Frequency Neuromuscular Electrical Stimulation a Suitable Tool for Muscle Performance Improvement in Both Healthy Humans and Athletes? Eur. J. Appl. Physiol. 2011, 111, 2473–2487. [Google Scholar] [CrossRef] [PubMed]
- Green, L.A.; Gabriel, D.A. The Effect of Unilateral Training on Contralateral Limb Strength in Young, Older, and Patient Populations: A Meta-Analysis of Cross Education. Phys. Ther. Rev. 2018, 23, 238–249. [Google Scholar] [CrossRef]
- Hester, G.M.; Magrini, M.A.; Colquhoun, R.J.; Barrera-Curiel, A.; Estrada, C.A.; Olmos, A.A.; Bailly, A.R.; Ha, P.L.; Defreitas, J.M. Cross-Education: Effects of Age on Rapid and Maximal Voluntary Contractile Characteristics in Males. Eur. J. Appl. Physiol. 2019, 119, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A. Physiological and Methodological Considerations for the Use of Neuromuscular Electrical Stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Gondin, J.; Guette, M.; Ballay, Y.; Martin, A. Electromyostimulation Training Effects on Neural Drive and Muscle Architecture. Med. Sci. Sports Exerc. 2005, 37, 1291–1299. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kozinc, Ž.; Šarabon, N. Inter-Limb Asymmetries in Volleyball Players: Differences between Testing Approaches and Association with Performance. J. Sports Sci. Med. 2020, 19, 745. [Google Scholar] [PubMed]
- Lum, D.; Barbosa, T. Brief Review: Effects of Isometric Strength Training on Strength and Dynamic Performance. Int. J. Sports Med. 2019, 40, 363–375. [Google Scholar] [CrossRef]
- Rhea, M.R.; Alvar, B.A.; Burkett, L.N.; Ball, S.D. A Meta-Analysis to Determine the Dose Response for Strength Development. Med. Sci. Sports Exerc. 2003, 35, 456–464. [Google Scholar] [CrossRef]
- Kanehisa, H.; Nagareda, H.; Kawakami, Y.; Akima, H.; Masani, K.; Kouzaki, M.; Fukunaga, T. Effects of Equivolume Isometric Training Programs Comprising Medium or High Resistance on Muscle Size and Strength. Eur. J. Appl. Physiol. 2002, 87, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, B.; Holzinger, S.; Soleimani, M.; Pelzer, T.; Stening, J.; Pfeiffer, M. Neuromuscular Responses to 14 Weeks of Traditional and Daily Undulating Resistance Training. Int. J. Sports Med. 2015, 36, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Szeto, G.; Strauss, G.; Domenico, G.; Lai, H. The Effect of Training Intensity on Voluntary Isometric Strength Improvement. Aust. J. Physiother. 1989, 35, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Speicher, U.; Kleinöder, H. Effektitvitätsprüfung Klassischer Und Moderner Krafttrainingsverfahren—Differentielle Kraftdiagnostik Und Moderne Trainingsregulation. F.I.T-Wissenschaftsmag. Dtsch. Sporthochsch. Köln 2009, 14, 20–23. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EMS | VOL | ANOVA | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | % Change | Cohen’s d | Pre-Test | Post-Test | % Change | Cohen’s d | F-Value Time | F-Value Group | F-Value Time × Group | |
| Trained leg | |||||||||||
| Tmax (Nm/kg) | 15.7 ± 2 | 20.2 ± 3.5 | 29.3 | 2.12 | 16.6 ± 2.2 | 21.4 ± 3.4 | 28.8 | 2.11 | 82.0 ** | 0.9 | 0.0 |
| RTD (Nm/kg/s) | 83 ± 13 | 93 ± 17 | 12.3 | 0.92 | 85 ± 18 | 97 ± 15 | 16.6 | 1.10 | 16.4 ** | 0.1 | 0.2 |
| RTD-SF | 6.0 ± 0.6 | 5.1 ± 0.7 | −14.6 | 1.10 | 5.9 ± 0.8 | 5.0 ± 0.6 | −14.9 | 1.01 | 25.1 ** | 0.1 | 0.0 |
| Intercept | 0.9 ± 0.18 | 1.07 ± 0.21 | 22.5 | 0.78 | 0.86 ± 0.29 | 1.08 ± 0.17 | 24.9 | 0.72 | 12.5 ** | 0.0 | 0.1 |
| Non-trained leg | |||||||||||
| Tmax (Nm/kg) | 17 ± 1.9 | 19 ± 3.6 | 11.9 | 0.76 | 19.2 ± 2.8 | 19.4 ± 2.9 | 2.2 | 0.20 | 3.28 | 1.4 | 2.1 |
| RTD (Nm/kg/s) | 87 ± 16 | 89 ± 20 | 2 | 0.34 | 96 ± 18 | 94 ± 18 | −0.6 | 0.01 | 0.04 | 0.9 | 0.4 |
| RTD-SF | 5.9 ± 0.6 | 5.1 ± 0.5 † | −12.6 | 0.76 | 5.5 ± 0.6 | 5.4 ± 0.7 | −0.1 | 0.20 | 6.35 * | 0.0 | 5.5 * |
| Intercept | 0.94 ± 0.25 | 1.10 ± 0.17 | 16.6 | 0.60 | 1.02 ± 0.17 | 0.99 ± 0.24 | −2.2 | 0.25 | 1.13 | 0.0 | 2.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knežević, O.M.; Šarabon, N.; Garcia-Ramos, A.; Majstorović, N.; Milanović, S.D.; Filipović, S.R.; Mirkov, D.M. Rate of Torque Development Scaling Factor Decreased Following a 6-Week Unilateral Isometric Training Using Electrostimulation or Voluntary Contractions. Appl. Sci. 2024, 14, 6485. https://doi.org/10.3390/app14156485
Knežević OM, Šarabon N, Garcia-Ramos A, Majstorović N, Milanović SD, Filipović SR, Mirkov DM. Rate of Torque Development Scaling Factor Decreased Following a 6-Week Unilateral Isometric Training Using Electrostimulation or Voluntary Contractions. Applied Sciences. 2024; 14(15):6485. https://doi.org/10.3390/app14156485
Chicago/Turabian StyleKnežević, Olivera M., Nejc Šarabon, Amador Garcia-Ramos, Nikola Majstorović, Sladjan D. Milanović, Saša R. Filipović, and Dragan M. Mirkov. 2024. "Rate of Torque Development Scaling Factor Decreased Following a 6-Week Unilateral Isometric Training Using Electrostimulation or Voluntary Contractions" Applied Sciences 14, no. 15: 6485. https://doi.org/10.3390/app14156485