Abstract
This study investigates the multifaceted phenomenon of kinesiophobia, characterized by an irrational fear of movement, particularly prevalent among individuals with chronic pain. The research delves into various factors influencing kinesiophobia, including demographic variables, psychological experiences, and physical characteristics. Employing the Tampa Scale of Kinesiophobia, the study assesses fear levels and their correlation with pain perception and functional capacity. Findings reveal a significant relationship between kinesiophobia and psychological exhaustion, reduced alertness, and self-esteem issues, particularly among athletes. Moreover, factors such as fatigue, overextension, sleep quality, and nutritional habits are identified as contributing to the manifestation of kinesiophobia. Furthermore, our study employs meticulous data preprocessing and neural network modeling, achieving an accuracy of 94.54%, to explore predictive factors such as age, gender, and fear-related attitudes. Notably, while injury history emerges as a significant predictor of kinesiophobia, gender does not exert a substantial influence. Notably, while injury history emerges as a significant predictor of kinesiophobia, gender does not exert a substantial influence. The analysis underscores the complex interplay of physical, psychological, and environmental factors in shaping kinesiophobia and highlights the importance of tailored interventions targeting fear-related attitudes and promoting well-being and rehabilitation strategies in individuals affected by this condition.
1. Introduction
Athletes encounter a variety of psychological hurdles stemming from the competitive and physically demanding nature of their profession [1,2,3]. Stress, a prevalent reaction to competition pressure or the fear of failure, emerges as one such challenge [4,5]. Emotional strain may surface when training intensity surpasses an athlete’s capacity, resulting in emotional fatigue characterized by monotony, waning enthusiasm, and diminished performance [6,7]. Psychic tension, exacerbated by intense training loads, can manifest in various forms including nervousness, emotional volatility, fatigue, sleep disturbances, diminished vigor, mood fluctuations, and headaches [6,8]. Lastly, feelings of anger and frustration can arise from the pressure to excel, along with interpersonal conflicts with teammates or coaches [9,10,11].
Kinesiophobia, an irrational dread of movement, is intricately linked to chronic pain and encompasses an array of psychological and social factors unique to each individual, which are influenced by variables such as gender, age, sporting activities, past injuries, and training methods [12]; It is noteworthy that kinesiophobia often intersects with feelings of instability, is particularly prevalent among women [13], and culminates in diminished functional mobility across daily tasks, work, and athletic pursuits. Its physiological manifestations typically include muscular atrophy, fibrosis, and impaired function [14]; which are often triggered by a heightened risk of injury or the onset of burnout [15].
Quantifying kinesiophobia often relies on tools such as the Tampa Scale of Kinesiophobia, a validated measure designed to assess both the fear of movement and its association with chronic pain recurrence [16,17,18]. This psychological state is intertwined with mental exhaustion, leading to diminished alertness and compromised reaction to movement cues, further hampering functional abilities [4,15,19,20]. Additionally, psychological factors such as self-esteem play a pivotal role as athletes compare their physiques to those of their peers, contributing to an incessant pursuit of an ideal body image, which is potentially detrimental to their well-being [15].
The impact of kinesiophobia can be seen in athletic performance, where psychological barriers may impede the optimal execution of movements critical for success. Athletes grappling with past injuries may find themselves unable to perform specific actions, which undermines team outcomes and fosters self-doubt [21]. Furthermore, fatigue arising from physical or mental exhaustion can hamper training regimens and cognitive function and is exacerbated by stressors from training or the athlete’s personal life [15,22]. Overextension, a consequence of impaired motor and psychological control, may precipitate burnout, further diminishing athletic productivity [15,23].
The significance of sleep quality and quantity cannot be overstated, with ramifications extending to athletic performance and overall health. Disruptions in sleep patterns, whether from drowsiness or insomnia, are correlated with obesity, cardiometabolic diseases, and diminished quality of life [15,24]. Similarly, muscle mass regulation, influenced by nutrition and exercise, can be disrupted by alcohol consumption, necessitating a holistic approach to athletes’ well-being [25].
In order to combat kinesiophobia, physical exercise emerges as a cornerstone intervention, aided by tools such as the Tampa Scale of Kinesiophobia. However, a multidisciplinary approach involving psychologists, nutritionists, and engineers is indispensable given the nuanced nature of each athlete’s experience and the potential comorbidities [12,26,27]. Within this framework, the Universidad del Valle de Mexico has prioritized athlete health, fostering an environment conducive to sporting excellence [28,29].
Advancements in artificial intelligence (AI) and machine learning (ML) offer promise for applications in sports medicine, particularly in injury prediction using ML models [30].
AI, which leverages computer systems to emulate human intelligence, presents opportunities for speech recognition, learning, and decision-making [31]. ML, a subset of AI, enables machines to learn from data and make predictions without explicit programming [32,33].
In the realm of sports medicine, ML models, such as neural networks, hold potential for injury prediction [34,35]. By analyzing historical data, including hydration levels, injury types, and athlete performance metrics, these models can discern patterns and forecast injury risk, empowering coaches and healthcare professionals in their injury prevention and performance enhancement efforts [30,36].
One of the objectives of this paper is to explore the primary trends contributing to kinesiophobia, such as fear, gender, injury, and age. Moreover, our contributions are as follows:
We carried out a thorough examination to identify the predictors of kinesiophobia. The analysis revealed that factors such as prior injuries, fear of becoming injured, and fear of experiencing pain play critical roles in predicting kinesiophobia.
This study found no correlation between healthy habits, such as proper nutrition and adequate rest, and kinesiophobia.
This study highlights the importance of addressing both physical and psychological factors for the prevention and treatment of kinesiophobia among athletes.
2. Materials and Methods
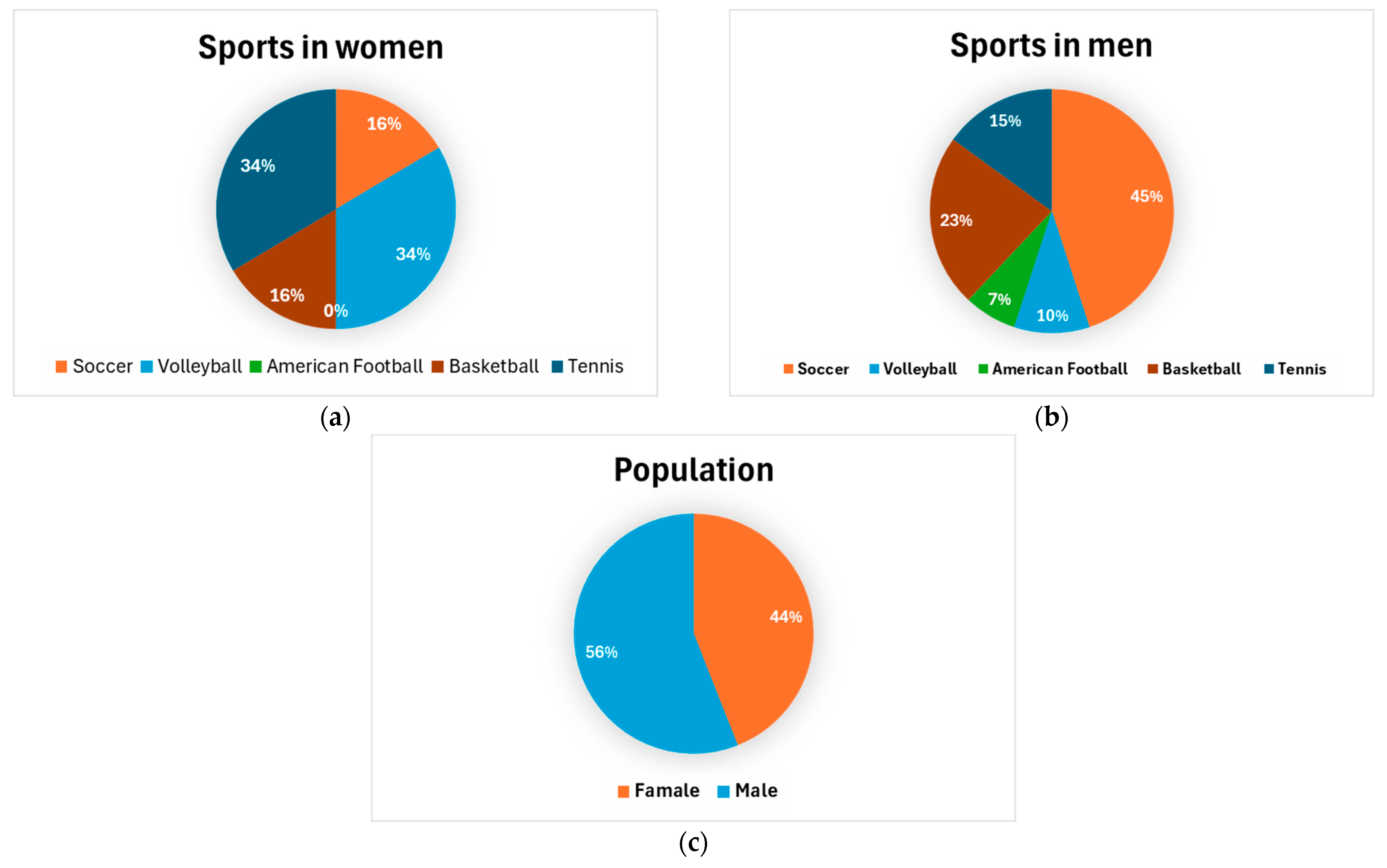
In this research, we surveyed a cohort comprising 825 athletes (364 females and 461 males) engaged in various sports activities including soccer, volleyball, American football, basketball, and tennis (Figure 1). The cohort was not divided into male and female groups so as to observe the overall behavior of the athletes irrespective of gender, with the aim of avoiding potential bias in the results and ensuring that the findings would apply to all athletes.
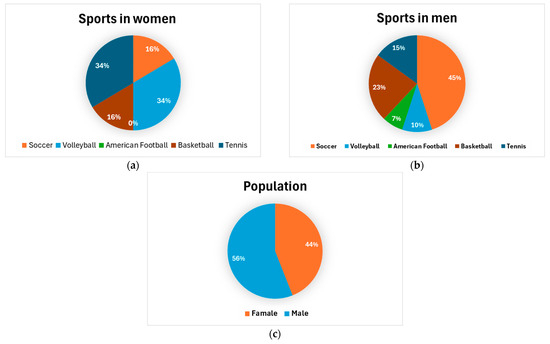
Figure 1.
(a) Percentage of sports participation among women. (b) Percentage of sports participation among men. (c) Percentage of population.
The dataset encompasses a wide array of parameters, including age, gender, daily training duration, weekly training frequency, history of ankle injury, post-injury medical interventions, participation in sports activities despite injuries, stress levels during competitions, kinesiophobia, perceived fatigue, average daily hydration, and hydration levels during specific sporting events. Structured and validated questionnaires were employed to gather data on these variables. Measurement instruments were carefully selected to ensure data reliability and validity. Additionally, we utilized the Tampa Scale of Kinesiophobia, which demonstrated a Cronbach’s alpha coefficient of 0.87, to assess the fear of movement within the context of sports injury rehabilitation [37].
Athletes were recruited through stratified random sampling at the Universidad del Valle de Mexico’s “Interlinces” event [28,29]. Before participating in the study, all athletes provided informed consent. Surveys were administered individually and privately to ensure the confidentiality of responses.
The decision was made to not divide the cohort into groups of men and women in order to observe the general behavior of athletes regardless of gender. This was done to avoid any potential bias in the results and to ensure that the findings would apply to all athletes. Furthermore, by keeping men and women in the same group, more comprehensive and representative insights into the behavior of athletes in general could be obtained.
Data Collection and Analytical Instruments
The survey responses underwent meticulous refinement in order to construct a comprehensive database that accurately portrayed the participants’ health and fitness regimens while safeguarding their privacy.
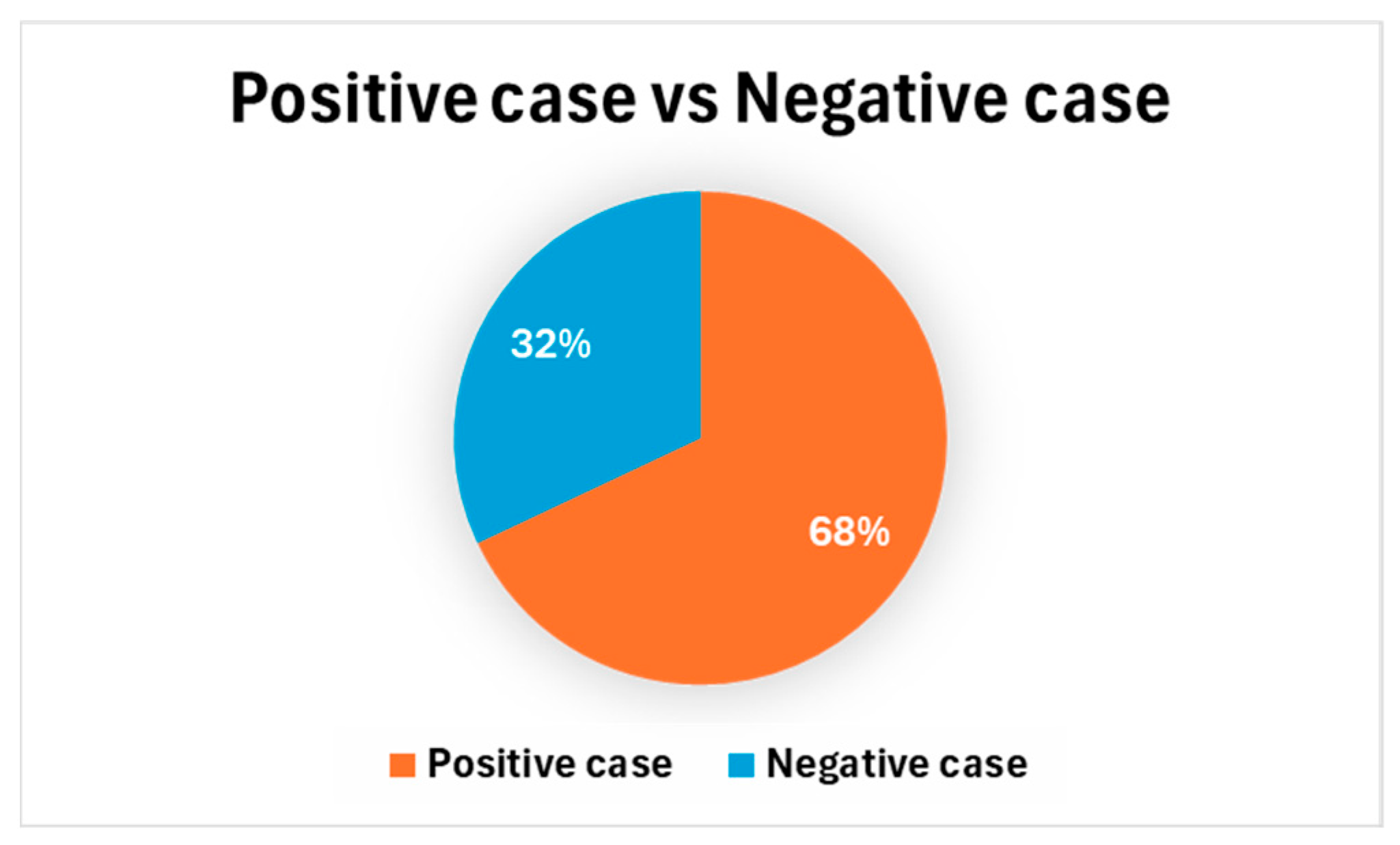
The dependent variable was divided into two categories: individuals who exhibited kinesiophobia and those who did not, with 577 positive cases (68%) and 248 negative cases (32%) as determined by the Tampa Scale of Kinesiophobia (Figure 2). MATLAB, renowned for its robust data manipulation capabilities and adeptness in implementing machine learning methodologies, including unsupervised and supervised learning techniques, served as the analytical tool of choice.
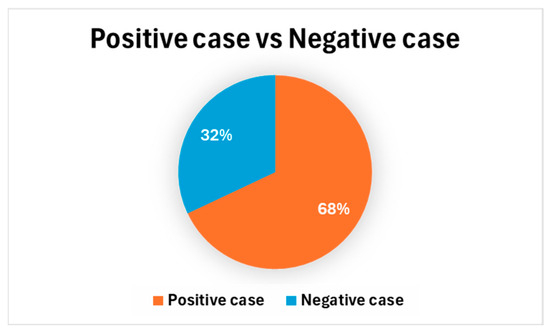
Figure 2.
Percentage of positive vs. negative cases.
3. Results of Data Training and Discussion
The development of the injury prognostication model included four pivotal components:
- Compilation of the dataset;
- Preprocessing of the data;
- Implementation of neural network models;
- Evaluation of the model.
3.1. Dataset Acquisition
Created to procure and comprehend datasets, this module facilitates the analysis of values, patterns, and trends linked with kinesiophobia among athletes, thereby substantially aiding in outcome prediction and assessment. Table 1 provides a comprehensive representation of the dataset of predictor variables and Table 2. provides a response variable.

Table 1.
Predictor variables.
Table 2.
Response variable.
3.2. Data Preprocessing
Data preprocessing, a pivotal stage in the realm of data analysis and modeling, has a significant influence on the caliber and efficacy of the results. Within the context of this study on kinesiophobia among athletes, preprocessing included a variety of tasks, ranging from purging data to readying it for machine learning algorithm application.
The initial dataset, comprising 825 surveyed athletes, underwent a meticulous debugging process to safeguard data integrity and coherence. Anomalies such as outliers, duplicates, and incongruous records were noted and duly addressed. This procedure of data cleansing is crucial to mitigate biases and inaccuracies, which could compromise subsequent analyses.
3.3. Neural Network Modeling
A comprehensive assessment of the models was carried out, and the accuracy achieved by each model is presented in Table 3.
Table 3.
Accuracy of various machine learning algorithms.
The features included age, gender (male and female), injury, deceleration injury, overuse injury, training hours, training days, overexertion, previous injuries, corrective treatment, preventive treatment, sports with injuries, non-compliance, stress injury relationship, self-esteem injury relationship, fear of injury, fear of pain, fear of increasing pain, fear of continuing sports with pain, fear of continuing training, healthy nutrition, nutritional supervision, warm-up, restful sleep, isotonic beverages, alcoholic beverages, and outcome.
Notably, the neural network model demonstrated exceptional accuracy, achieving an impressive 87.9% during testing. This indicates an outstanding ability to accurately classify athletes based on the presence or absence of kinesiophobia. Interestingly, the boosted trees and logistic regression models also exhibited high levels of accuracy, with values of 87.1% and 85.8%, respectively. These findings have significant implications for the identification and prevention of kinesiophobia in athletes.
3.3.1. Accuracy
The accuracy metric plays a pivotal role in evaluating the model’s overall performance. It is determined using Equation (1).
where:
- TPs (true positives) = 282;
- TNs (True negatives) = 342;
- FPs (False positives) = 16;
- FNs (False negatives) = 20.
In our case:
3.3.2. Recall
Recall assesses the model’s capability to accurately identify positive cases. It is calculated using Equation (3):
In our case:
3.3.3. Precision
Precision in machine learning gauges the ratio of correct positive predictions, emphasizing the model’s ability to steer clear of false positives. It is determined using Equation (5):
In our case:
3.3.4. F1-Score
The F1-score combines accuracy and recall into a unified measure. It is particularly useful in scenarios where both metrics are significant and we are striving for a balance between them. It is calculated using Equation (7):
In our case:
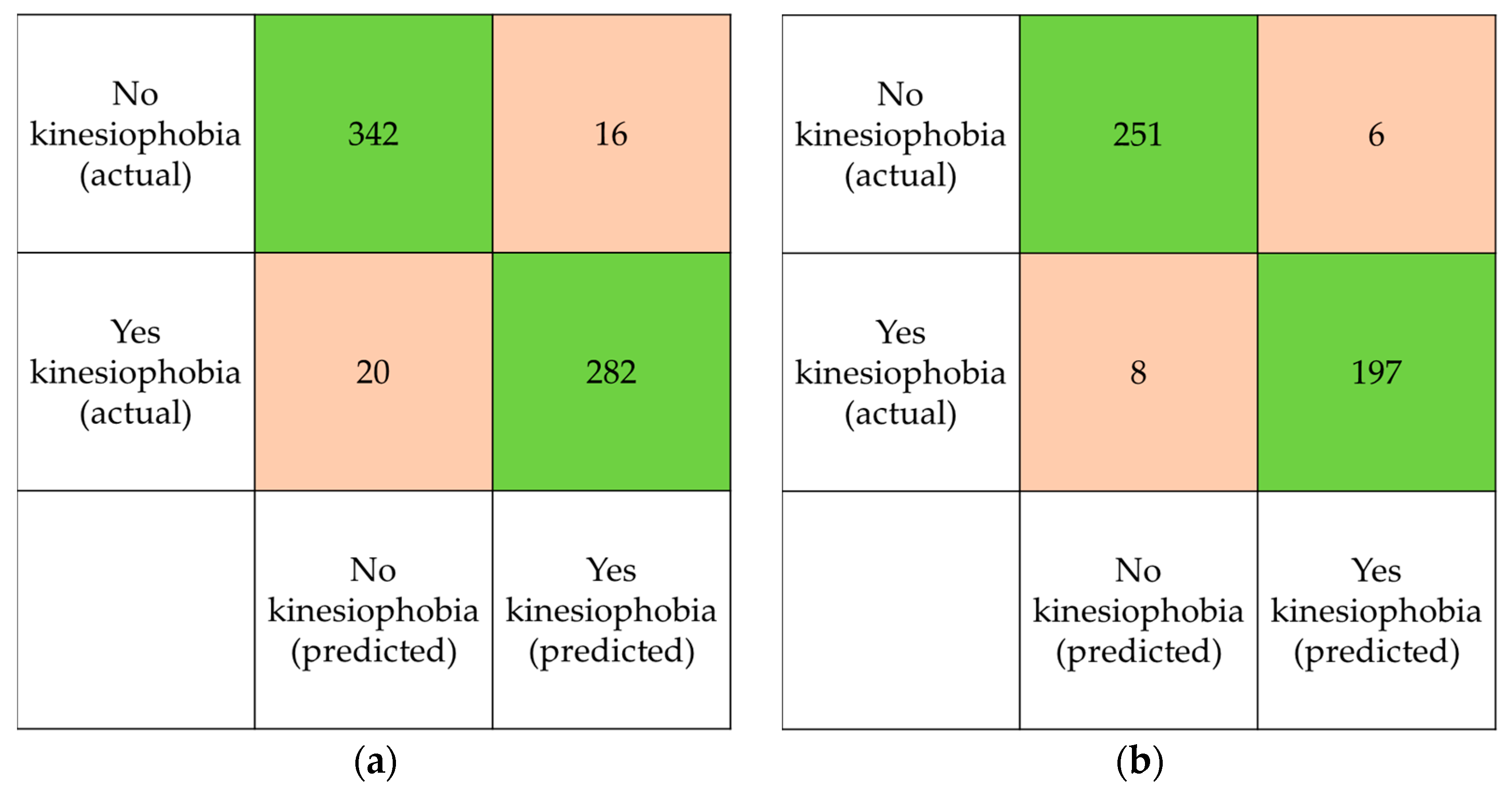
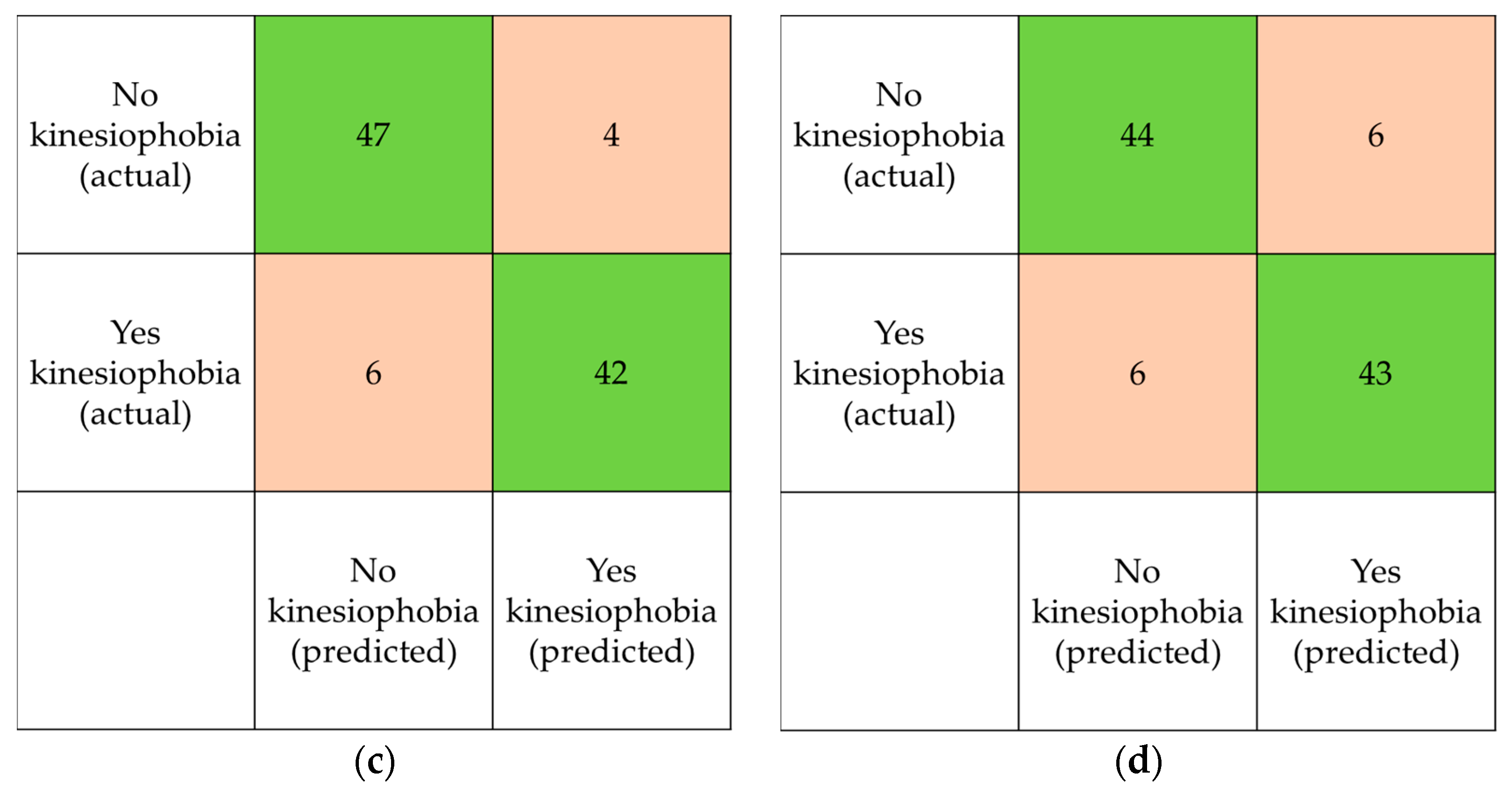
The model predictions were compared with the actual classes in these matrices to analyze their performance. Each matrix was divided into four quadrants representing the four possible combinations of predictions and actual classes: true positive (TP), false positive (FP), true negative (TN), and false negative (FN).
Starting with the overall confusion matrix (Figure 3a), we can observe that in 342 cases, the model correctly predicted the absence of kinesiophobia (TP), while in 282 cases, it correctly predicted the presence of kinesiophobia (TN). However, there are also 20 cases where the model incorrectly predicted the absence of kinesiophobia when it was present (FN), and 16 cases where it incorrectly predicted the presence of kinesiophobia when it was not present (FP).
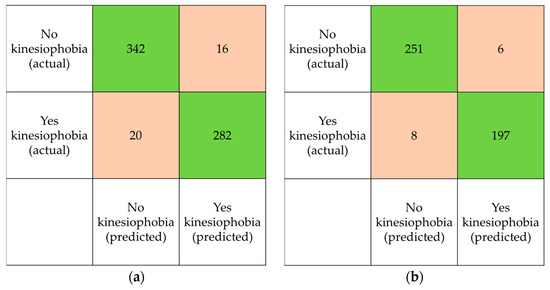
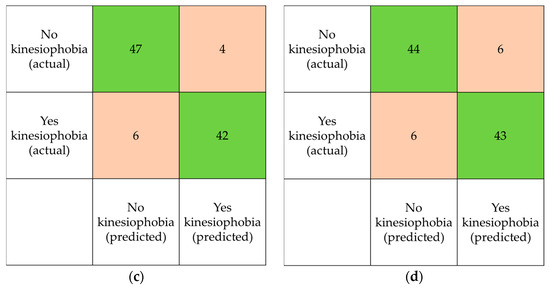
Figure 3.
Confusion matrix: (a) overall confusion matrix, (b) training set, (c) validation set, (d) validation set.
Analyzing the confusion matrix of the training set (Figure 3b), we observe that the model achieved higher accuracy in predicting the absence of kinesiophobia, with 251 cases correctly classified as negative (TP) and 197 cases correctly classified as positive (TN). However, there were also 6 cases incorrectly classified as negative (FN) and 8 cases incorrectly classified as positive (FP).
Looking at the confusion matrix of the validation set (Figure 3c), we see a similar trend to the training set, albeit with slightly lower performance. There is a higher proportion of cases correctly classified as negative (TP = 47, TN = 42), but also a higher proportion of cases incorrectly classified as positive (FP = 4) and negative (FN = 6) compared to the training set.
Finally, analyzing the confusion matrix of the test set (Figure 3d), we observe that the performance is similar to the validation set, with reasonably good accuracy in predicting the absence of kinesiophobia (TP = 44; TN = 43), but a non-negligible number of cases incorrectly classified as positive (FP = 6) and negative (FN = 6).
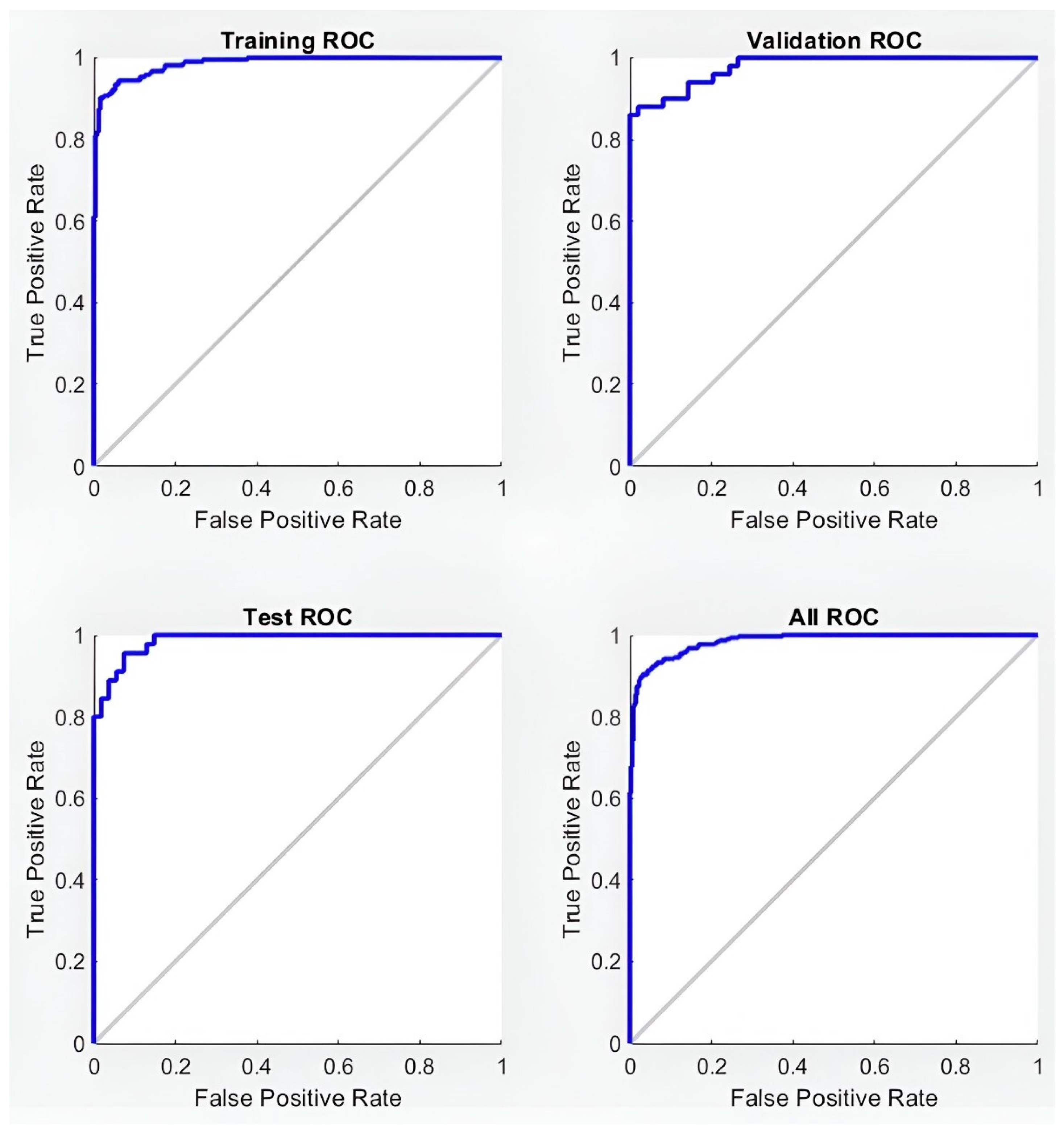
3.4. Receiver Operating Characteristics (ROC) and Area under the Curve (AUC)
The receiver operating characteristic (ROC) curve is a graphical representation of the relationship between the true positive rate (TPR), or recall, and the false positive rate (FPR) at various classification thresholds. The area under the curve (AUC) is a metric used to determine a model’s ability to distinguish between classes. In this case, as shown in Figure 4, the AUC values are 0.975 for training, 0.957 for validation, and 0.958 for the test.
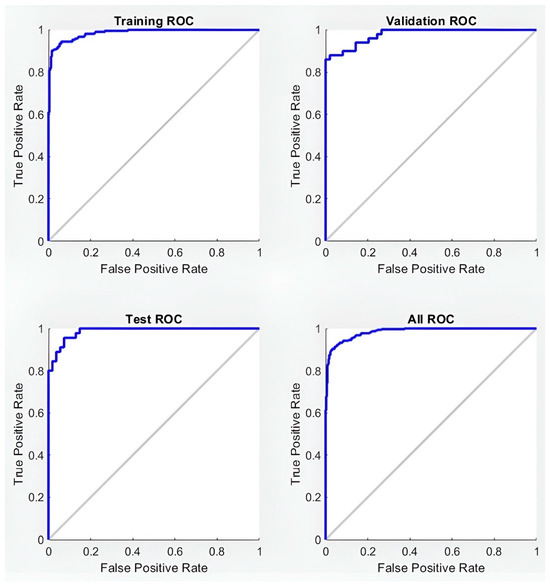
Figure 4.
Receiver operating characteristics.
3.5. Predictive Factors Analysis
In this analysis, a neural network model was employed to evaluate the relationship between the outcome variable and 14 potential predictors. Table 4 presents the estimated coefficients, providing key information about the magnitude and direction of these associations.
Table 4.
Model performance metrics.
It is important to note that positive coefficients indicate a positive association between the predictor variable and the outcome variable, while negative coefficients indicate a negative association.
3.6. Interpretation of Coefficients
Age: a positive coefficient of 0.0026624 suggests a slightly positive association between age and the outcome variable, although this association is relatively weak.
Gender (male and female): both genders have significant negative coefficients (−6.7294 for male and −6.6456 for female), indicating that gender is not a significant factor influencing kinesiophobia.
Injury: a positive coefficient of 0.94664 indicates a considerably positive association between the occurrence of injury and the outcome variable, suggesting that a previous injury increases the likelihood of kinesiophobia.
Deceleration and overuse injuries: the negative coefficients for these specific types of injuries (−0.65269 and −0.43516, respectively) suggest that they do not contribute significantly to kinesiophobia, possibly due to perceptions of less severity or quicker recovery.
Training hours and days: both variables have a positive coefficient (0.13735 and 0.080512, respectively), indicating a positive association with kinesiophobia, suggesting that more training time and greater frequency increase the risk of developing kinesiophobia.
Overexertion: with a positive coefficient of 0.29543, overexertion is positively associated with kinesiophobia, possibly due to the higher likelihood of injury and physical exhaustion.
Previous injuries: a positive coefficient of 0.030372, although weak, suggests that previous injuries may slightly influence kinesiophobia, perhaps due to fear of recurrence.
Corrective and preventive treatments: while corrective treatment has a negative coefficient (−0.69206), indicating a possible reduction in kinesiophobia, preventive treatment has a positive coefficient (0.29251), suggesting that a perceived need for preventive treatment might be associated with higher levels of kinesiophobia.
Sports with injuries: a negative coefficient of −0.6451 indicates that participating in sports with a high incidence of injuries might be associated with lower levels of kinesiophobia, possibly due to greater familiarity with and management of injuries.
Non-compliance: a positive coefficient of 0.8022 suggests that non-adherence to medical or training recommendations is positively associated with kinesiophobia.
Stress injury and self-esteem injury: both factors have a negative coefficient (−0.4922 and −0.26815, respectively), indicating that better stress management and higher self-esteem related to injuries can reduce kinesiophobia.
Fear and anxiety factors related to sports injuries: the variables “fear of injury”, “fear of pain”, “fear of increasing pain”, “fear of continuing sports with pain”, and “fear of continuing training” have high positive coefficients, indicating a strong positive association between these fears and kinesiophobia. This implies that individuals who experience greater fear of injury, pain, or continuing sports activities with pain are more likely to experience kinesiophobia.
Healthy practices: the variables “healthy nutrition”, “nutritional supervision”, “warm-up”, and “restful sleep” have negative coefficients, indicating a negative association between these healthy practices and kinesiophobia, suggesting that individuals who adopt these practices are less likely to experience kinesiophobia.
Consumption of isotonic and alcoholic beverages: while the consumption of isotonic beverages has a very low positive coefficient (0.010769), suggesting a minimal influence, the consumption of alcoholic beverages has a higher positive coefficient (0.18236), suggesting a positive association with kinesiophobia, possibly due to its negative effects on recovery and physical performance.
4. Discussion
The present analysis employed a neural network model to evaluate the relationship between kinesiophobia as the outcome variable and 14 potential predictors. The results reveal significant associations, providing a deeper understanding of the factors that influence the occurrence and severity of kinesiophobia.
4.1. Positive Factors
Positive coefficients in the model indicate a direct association with increased kinesiophobia. Notably, factors related to fear and anxiety with regard to sports injuries stand out. The variables “fear of injury” (3.5997), “fear of pain” (2.9435), “fear of increasing pain” (3.2231), “fear of continuing sports with pain” (3.8572), and “fear of continuing training” (3.5259) have the highest coefficients, suggesting a strong correlation with kinesiophobia. These findings are consistent with the literature, highlighting that the fear of pain and injuries is a critical determinant in the development of kinesiophobia.
The positive coefficient for “injury” (0.94664) is also significant, indicating that the experience of previous injuries is associated with increased kinesiophobia. This result underscores the influence of past experience on the perception of risk and fear of future injuries, which can influence the behavior of avoiding physical activity.
Additionally, the coefficients for the variables “overexertion” (0.29543) and “training Hours” (0.13735) suggest that a higher volume of training and greater effort can contribute to the development of kinesiophobia. These factors might be related to increased fatigue and the likelihood of injuries, fueling the fear of re-injury.
4.2. Negative Factors
Negative coefficients indicate an inverse relationship with kinesiophobia, suggesting that certain factors may protect against the development of this condition. “healthy nutrition” (−0.69991), “nutritional supervision” (−0.088618), “warm-up” (−0.57456), and “restful sleep” (−0.37854) are associated with a lower likelihood of experiencing kinesiophobia. These results highlight the importance of maintaining healthy lifestyle practices not only to prevent injuries but also to mitigate the fear of being injured. A comprehensive focus on health and well-being can therefore be crucial in reducing the fear of sports injuries.
The variable “corrective treatment” (−0.69206) also shows a negative association, suggesting that effective therapeutic interventions can help reduce kinesiophobia. This finding is consistent with studies demonstrating that appropriate rehabilitation of injuries and education about injuries can decrease fear and improve people’s confidence in their ability to recover and return to physical activity.
4.3. Neutral or Low Influence Factors
The factors “age” (0.0026624), “previous injuries” (0.030372), and “isotonic beverages” (0.010769) have very low coefficients, indicating minimal or no influence on kinesiophobia. This suggests that, while there may be some relationship, they are not significant determinants in the development of kinesiophobia in the studied population.
4.4. Clinical and Practical Implications
The findings of this study have important implications for the prevention and treatment of kinesiophobia. Identifying significant risk factors, such as fear of injury and pain, can guide health professionals in developing more effective intervention strategies. For example, cognitive-behavioral therapy (CBT) focused on reducing fear and anxiety around being injured could be a beneficial intervention for athletes and physically active individuals.
Moreover, healthy lifestyle practices, including adequate nutrition, proper warm-up, and restful sleep, can serve as preventive measures to decrease the incidence of kinesiophobia. These practices not only improve physical health but can also contribute to better mental and emotional health, thereby reducing the fear of injury.
5. Conclusions
The authors regard this work as highly significant, as it presents original findings indicating innovation in the field of kinesiophobia. Firstly, we employed artificial intelligence methods to predict significant trends leading to the occurrence of kinesiophobia among university athletes.
The analysis, utilizing a neural network model to explore predictive factors, revealed several key insights regarding their association with the outcome variable. Notably, the interpretation of the coefficients in Table 4 underscores the importance of discerning between positive and negative associations.
First, a positive coefficient suggests a slightly positive, albeit weak, association between age and the outcome variable. This implies that with advancing age, there may be a marginal tendency to experience kinesiophobia, although the effect size is relatively minor.
Moreover, the substantial negative coefficients for gender variables (“male” and “female”) indicate that gender per se does not significantly influence kinesiophobia. This finding suggests that, regardless of gender, individuals are equally susceptible to experiencing kinesiophobia, as indicated by the lack of a substantial association with gender.
By contrast, the variable “injury” has a notably positive coefficient, indicating a significant positive association with the outcome variable. This highlights the important contribution of previous injuries to predisposing individuals to kinesiophobia (i.e., those with a history of injuries may be more prone to developing kinesiophobia).
Furthermore, the analysis showed substantially positive associations between fear-related variables (“fear of injury”, “fear of pain”, etc.) and the outcome variable. This underscores the profound impact of fear and anxiety around sports injuries on the development of kinesiophobia. Therefore, our study is relevant, as the proposed hypothesis is accepted.
Individuals who experience heightened fear concerning injuries and pain are more likely to manifest symptoms of kinesiophobia, emphasizing the psychological dimension of strategies for injury rehabilitation and prevention.
Conversely, variables associated with healthy practices (“healthy nutrition”, “nutritional supervision”, etc.) have negative coefficients, suggesting a protective effect against kinesiophobia. This implies that adhering to healthy lifestyle practices, such as proper nutrition, adequate rest, and warm-up routines, could mitigate the risk of developing kinesiophobia.
In summary, the analysis points out the multifaceted nature of kinesiophobia, which is influenced by a myriad of factors ranging from a history of injury to psychological attitudes toward pain and fear. Understanding these predictive factors is essential in order to tailor effective interventions aimed at mitigating kinesiophobia and promoting physical rehabilitation and well-being.
6. Future Work
The authors are contemplating conducting separate follow-up investigations of a second sampling of men and women focused on predicting injuries and kinesiophobia. This will enable the development of practical applications for athletics coaches.
Author Contributions
Conceptualization, R.E.D.A. and D.P.-G.; methodology, R.E.D.A., N.R.E., D.P.-G. and C.A.G.G.; validation, M.A.O.R., C.A.G.G. and D.P.-G.; formal analysis, R.E.D.A., N.R.E. and D.P.-G.; investigation, N.R.E. and D.G.G.; data curation, D.P.-G.; writing—original draft preparation, D.P.-G. and N.R.E.; writing—review and editing, R.E.D.A. and M.A.O.R.; supervision, R.E.D.A. and D.P.-G. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by the National Vice Rector’s Office for Research, Innovation, and Business Incubator of Universidad del Valle de México.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics and Research Committee of the Universidad del Valle de México, Campus Victoria, Tamaulipas, Mexico (UVM-VIC/16/10/23-002).
Informed Consent Statement
The analyzed data were anonymized by athletes. Informed consent was obtained from all subjects during data acquisition.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We would like to express our gratitude to research Gerardo Dubcovsky for their arduous support; to Emanuel Canto Heredia from the School of Health Sciences, Campus Chihuahua, of Universidad del Valle de Mexico for their valuable contributions; and to the students Fatima Cruz Suarez and Ana Paulina Vázquez Aburto from the School of Health Sciences, Campus Lomas Verdes, of Universidad del Valle de Mexico for their valuable contributions to the database.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- van Niekerk, M.; Matzkin, E.; Christino, M.A. Psychological Aspects of Return to Sport for the Female Athlete. Arthrosc. Sports Med. Rehabil. 2023, 5, 100738. [Google Scholar] [CrossRef] [PubMed]
- Hidrus, A.B.; Kueh, Y.C.; Arifin, W.N.; Konter, E.; Kuan, G. Sports Courage in Malaysian Silat Athletes: Confirmatory Factor Analysis of the Malay Language Version. Int. J. Environ. Res. Public Health 2020, 17, 1736. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, J.H.; Greenberger, P.A. Identifying Psychological Difficulties in College Athletes. J. Allergy Clin. Immunol. Pract. 2020, 8, 2216–2219. [Google Scholar] [CrossRef]
- Sun, J.; Fan, X.; Li, H. How Do High-Performance Work Systems Affect Work Fatigue: The Mediating Effect of Job Responsibility and Role Overload. PLoS ONE 2022, 17, e0269452. [Google Scholar] [CrossRef]
- Huang, J. Identification of Sports Athletes Psychological Stress Based on K-Means Optimized Hierarchical Clustering. Comput. Intell. Neurosci. 2022, 2022, 55797. [Google Scholar] [CrossRef] [PubMed]
- Neil, R.; Hanton, S.; Mellalieu, S.D.; Fletcher, D. Competition Stress and Emotions in Sport Performers: The Role of Further Appraisals. Psychol. Sport Exerc. 2011, 12, 460–470. [Google Scholar] [CrossRef]
- Fessi, M.S.; Moalla, W. Postmatch Perceived Exertion, Feeling, and Wellness in Professional Soccer Players. Int. J. Sports Physiol. Perform. 2018, 13, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, J.W.; Herring, K.M.; Iadevito, T.L. Systemic Issues Involved in Working with Professional Sports Teams. Clin. Sports Med. 2005, 24, 929–942. [Google Scholar] [CrossRef] [PubMed]
- Vega, A.; Cabello, R.; Megías-Robles, A.; Gómez-Leal, R.; Fernández-Berrocal, P. Emotional Intelligence and Aggressive Behaviors in Adolescents: A Systematic Review and Meta-Analysis. Trauma Violence Abus. 2021, 23, 1173–1183. [Google Scholar] [CrossRef]
- Tucker, L.W.; Parks, J.B. Effects of Gender and Sport Type on Intercollegiate Athletes’ Perceptions of the Legitimacy of Aggressive Behaviors in Sport. Sociol. Sport J. 2001, 18, 403–413. [Google Scholar] [CrossRef]
- Bovolon, L.; Mallia, L.; De Maria, A.; Bertollo, M.; Berchicci, M. Modulatory Role of Sport Factors on Amateur and Competitive Athletes’ Aggressive and Antisocial Behaviors. Heliyon 2024, 10, e23321. [Google Scholar] [CrossRef] [PubMed]
- Bordeleau, M.; Vincenot, M.; Lefevre, S.; Duport, A.; Seggio, L.; Breton, T.; Lelard, T.; Serra, E.; Roussel, N.; Das Neves, J.F.; et al. Treatments for Kinesiophobia in People with Chronic Pain: A Scoping Review. Front. Behav. Neurosci. 2022, 16, 933483. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Koshino, Y.; Kawahara, D.; Akimoto, M.; Mishina, M.; Nakagawa, K.; Ishida, T.; Kasahara, S.; Samukawa, M.; Tohyama, H. Kinesiophobia, Self-Reported Ankle Function, and Sex Are Associated with Perceived Ankle Instability in College Club Sports Athletes with Chronic Ankle Instability. Phys. Ther. Sport 2023, 61, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, M.S.; Reddy, R.S. Relationship between Kinesiophobia and Ankle Joint Position Sense and Postural Control in Individuals with Chronic Ankle Instability—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 2792. [Google Scholar] [CrossRef] [PubMed]
- Alaminos-Torres, A.; Martínez-Álvarez, J.R.; Martínez-Lorca, M.; López-Ejeda, N.; Marrodán Serrano, M.D. Fatigue, Work Overload, and Sleepiness in a Sample of Spanish Commercial Airline Pilots. Behav. Sci. 2023, 13, 300. [Google Scholar] [CrossRef] [PubMed]
- Dupuis, F.; Cherif, A.; Batcho, C.; Massé-Alarie, H.; Roy, J.S. The Tampa Scale of Kinesiophobia: A Systematic Review of Its Psychometric Properties in People with Musculoskeletal Pain. Clin. J. Pain 2023, 39, 236–247. [Google Scholar] [CrossRef] [PubMed]
- French, D.J.; France, C.R.; Vigneau, F.; French, J.A.; Evans, R.T. Fear of Movement/(Re)Injury in Chronic Pain: A Psychometric Assessment of the Original English Version of the Tampa Scale for Kinesiophobia (TSK). Pain 2007, 127, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Roelofs, J.; Goubert, L.; Peters, M.L.; Vlaeyen, J.W.S.; Crombez, G. The Tampa Scale for Kinesiophobia: Further Examination of Psychometric Properties in Patients with Chronic Low Back Pain and Fibromyalgia. Eur. J. Pain 2004, 8, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Heath, M.R. Editorial Commentary: Supporting Patients Psychologically and Reducing Kinesiophobia May Improve Anterior Cruciate Ligament Reconstruction Outcomes. Arthrosc. J. Arthrosc. Relat. Surg. 2023, 39, 2056–2057. [Google Scholar] [CrossRef] [PubMed]
- Reinking, S.; Seehusen, C.N.; Walker, G.A.; Wilson, J.C.; Howell, D.R. Transitory Kinesiophobia after Sport-Related Concussion and Its Correlation with Reaction Time. J. Sci. Med. Sport 2022, 25, 20–24. [Google Scholar] [CrossRef]
- McLean, S.A.; Clauw, D.J.; Abelson, J.L.; Liberzon, I. The Development of Persistent Pain and Psychological Morbidity after Motor Vehicle Collision: Integrating the Potential Role of Stress Response Systems into a Biopsychosocial Model. Psychosom. Med. 2005, 67, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Staiano, W.; Bonet, L.R.S.; Romagnoli, M.; Ring, C. Mental Fatigue Impairs Repeated Sprint and Jump Performance in Team Sport Athletes. J. Sci. Med. Sport 2024, 27, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Font, M.M. Clinical Applications of Nuclear Medicine in the Diagnosis and Evaluation of Musculoskeletal Sports Injuries. Rev. Española Med. Nucl. Imagen Mol. (Engl. Ed.) 2020, 39, 112–134. [Google Scholar] [CrossRef]
- Silva, A.; Pinto Pinheiro, L.S.; Silva, S.; Andrade, H.; Pereira, A.G.; Rodrigues da Silva, F.; Guerreiro, R.; Barreto, B.; Resende, R.; Túlio de Mello, M. Sleep in Paralympic Athletes and Its Relationship with Injuries and Illnesses. Phys. Ther. Sport 2022, 56, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Levitt, D.E.; Luk, H.Y.; Vingren, J.L. Alcohol, Resistance Exercise, and MTOR Pathway Signaling: An Evidence-Based Narrative Review. Biomolecules 2022, 13, 2. [Google Scholar] [CrossRef]
- Salvador, E.M.E.S.; Franco, K.F.M.; Miyamoto, G.C.; Franco, Y.R.d.S.; Cabral, C.M.N. Analysis of the Measurement Properties of the Brazilian-Portuguese Version of the Tampa Scale for Kinesiophobia-11 in Patients with Fibromyalgia. Braz. J. Phys. Ther. 2021, 25, 168–174. [Google Scholar] [CrossRef] [PubMed]
- van Iersel, T.P.; Larsen van Gastel, M.; Versantvoort, A.; Hekman, K.M.C.; Sierevelt, I.N.; Broekman, B.F.P.; van den Bekerom, M.P.J.; den Arend, M.C.; Boon, F.; Versluis, E.J.; et al. The Modified Tampa-Scale of Kinesiophobia for Anterior Shoulder Instability. Arthrosc. Sports Med. Rehabil. 2023, 5, 100768. [Google Scholar] [CrossRef] [PubMed]
- Juegos Olímpicos de Tokio: Atletas UVM de México|Blog UVM. Available online: https://blog.uvm.mx/juegos-olimpicos-de-tokio-conoce-a-los-atletas-que-representan-a-mexico-y-estudian-en-uvm (accessed on 22 February 2024).
- Lo Que nos Enseñan los Deportistas del Salón de la Fama UVM|Blog UVM. Available online: https://blog.uvm.mx/lo-que-nos-ensenan-nuestros-deportistas-del-salon-de-la-fama (accessed on 22 February 2024).
- Novel, E.; Elizabeth Duarte Ayala, R.; Pérez Granados, D.; Alberto González Gutiérrez, C.; Alberto Ortega Ruíz, M.; Rojas Espinosa, N.; Canto Heredia, E. Novel Study for the Early Identification of Injury Risks in Athletes Using Machine Learning Techniques. Appl. Sci. 2024, 14, 570. [Google Scholar] [CrossRef]
- Patel, D.; Hazan, H.; Saunders, D.J.; Siegelmann, H.T.; Kozma, R. Improved Robustness of Reinforcement Learning Policies upon Conversion to Spiking Neuronal Network Platforms Applied to Atari Breakout Game. Neural Netw. 2019, 120, 108–115. [Google Scholar] [CrossRef]
- Macpherson, T.; Churchland, A.; Sejnowski, T.; DiCarlo, J.; Kamitani, Y.; Takahashi, H.; Hikida, T. Natural and Artificial Intelligence: A Brief Introduction to the Interplay between AI and Neuroscience Research. Neural Netw. 2021, 144, 603–613. [Google Scholar] [CrossRef]
- Tavanaei, A.; Ghodrati, M.; Kheradpisheh, S.R.; Masquelier, T.; Maida, A. Deep Learning in Spiking Neural Networks. Neural Netw. 2019, 111, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Díaz, M.; Aguirre, R.S.; Vásconez, J.P.; Yáñez, R.; Roby, M.; Querales, M.; Salas, R. Explainable Machine Learning Techniques to Predict Muscle Injuries in Professional Soccer Players through Biomechanical Analysis. Sensors 2023, 24, 119. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Pappalardo, L.; Cintia, P. A Narrative Review for a Machine Learning Application in Sports: An Example Based on Injury Forecasting in Soccer. Sports 2021, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Moustakidis, S.; Siouras, A.; Vassis, K.; Misiris, I.; Papageorgiou, E.; Tsaopoulos, D. Prediction of Injuries in CrossFit Training: A Machine Learning Perspective. Algorithms 2022, 15, 77. [Google Scholar] [CrossRef]
- Ferrer-Peña, R.; Gil-Martínez, A.; Pardo-Montero, J.; Jiménez-Penick, V.; Gallego-Izquierdo, T.; La Touche, R. Adaptation and Validation of the Spanish Version of the Graded Chronic Pain Scale. Reumatol. Clínica (Engl. Ed.) 2016, 12, 130–138. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).