
A Systematic Review of Osteotomies to Correct Hallux Valgus in the First Metatarsal




Abstract
Featured Application
Abstract
1. Introduction
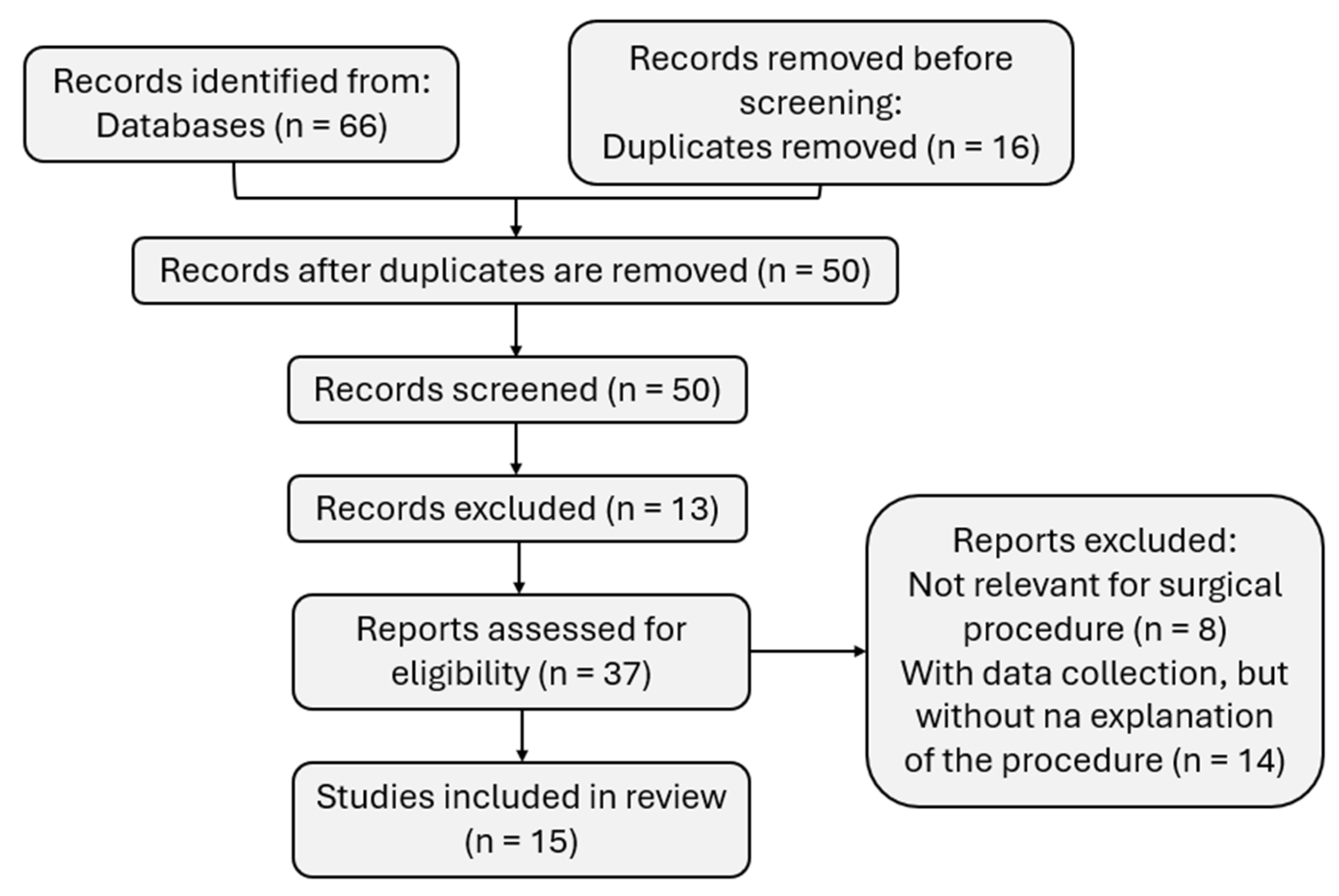
2. Materials and Methods
3. Results
3.1. Basal Closing Wedge Osteotomy
3.1.1. Procedure and Analysis
3.1.2. Follow-up and Biomechanical Analysis
3.2. Distal Chevron Metatarsal Osteotomy
3.2.1. Procedure and Analysis
3.2.2. Follow-up and Biomechanical Analysis
3.3. Proximal Metatarsal Osteotomy
3.3.1. Procedure and Analysis
3.3.2. Follow-up and Biomechanical Analysis
3.4. Proximal Oblique-Domed Osteotomy
3.4.1. Procedure and Analysis
3.4.2. Follow-up and Biomechanical Analysis
3.5. Proximal Spherical Metatarsal Osteotomy
3.5.1. Procedure and Analysis
3.5.2. Follow-up and Biomechanical Analysis
3.6. Rotational Scarf Osteotomy
3.6.1. Procedure and Analysis
3.6.2. Follow-up and Biomechanical Analysis
3.7. Mitchell Osteotomy
3.7.1. Procedure and Analysis
3.7.2. Follow-up and Biomechanical Analysis
4. Discussion
4.1. Analysis of Procedures and Results
4.2. Limitations on Review
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, S.-S.; Kim, J.H.; Kim, S.; Jung, E.Y.; Ryu, D.J.; Lee, D.K.; Wang, J.H. Avoiding Overcorrection to Increase Patient Satisfaction After Open Wedge High Tibial Osteotomy. Am. J. Sports Med. 2022, 50, 2453–2461. [Google Scholar] [CrossRef] [PubMed]
- Nix, S.; Smith, M.; Vicenzino, B. Prevalence of hallux valgus in the general population: A systematic review and meta-analysis. J. Foot Ankle Res. 2010, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- Perera, A.; Mason, L.; Stephens, M. The pathogenesis of hallux valgus. J. Bone Jt. Surg. 2011, 93, 1650–1661. [Google Scholar] [CrossRef] [PubMed]
- Alkhalifah, K.M.; Almotiri, M.M.; Alharbi, A.E.; Alrashidi, A.; Aldhali, I.K.; Alsaqry, O.S.; Alharbi, K.H.; Almogbil, I. A Systematic Review and Meta-Analysis of the Prevalence of Hallux Valgus in the General Population. Cureus 2023, 15, e42739. [Google Scholar] [CrossRef]
- Nguyen, J.K.; Sullivan, M.; Alpuerto, B.B., 2nd; Mueller, S.; Sly, N. A radiographic analysis of the abnormal hallux interphalangeus angle range: Considerations for surgeons performing Akin osteotomies. J. Orthop. Surg. 2019, 27, 2309499019841093. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, A.; Chen, J. Minimally Invasive Chevron Akin Osteotomy for Hallux Valgus Correction. JBJS Essent. Surg. Tech. 2024, 14, e22. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, S.; Watanabe, K.; Katayose, M.; Yamatsu, K.; Teramoto, A.; Ogihara, N. Three-dimensional morphological variations in the calcaneus and talus in relation to the hallux valgus angle. Ann. Anat. Anat. Anz. 2023, 247, 152053. [Google Scholar] [CrossRef] [PubMed]
- Yokozuka, M.; Okazaki, K. Characteristics of hindfoot morphology and ankle range of motion in young women with hallux valgus. J. Foot Ankle Res. 2023, 16, 64. [Google Scholar] [CrossRef]
- Sharma, J.; Aydogan, U. Algorithm for Severe Hallux Valgus Associated with Metatarsus Adductus. Foot Ankle Int. 2015, 36, 1499–1503. [Google Scholar] [CrossRef] [PubMed]
- Steadman, J.; Barg, A.; Saltzman, C.L. First Metatarsal Rotation in Hallux Valgus Deformity. Foot Ankle Int. 2021, 42, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Trnka, H.-J.; Mühlbauer, M.; Zembsch, A.; Hungerford, M.; Ritschl, P.; Salzer, M. Basal Closing Wedge Osteotomy for Correction of Hallux Valgus and Metatarsus Primus Varus: 10- To 22-Year Follow-up. Foot Ankle Int. 1999, 20, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, H.S.; Jeong, J.-J.; Seo, D.-K.; Kee, T.; So, S.; Choi, Y.R. Distal chevron metatarsal osteotomy is a viable treatment option for hallux valgus with metatarsus adductus—Multicentre retrospective study. Int. Orthop. 2021, 45, 2261–2270. [Google Scholar] [CrossRef] [PubMed]
- Makabe, K.; Matsumoto, T.; Tanaka, S.; Uchida, Y.; Nagase, Y.; Nishikawa, T. Comparison of short-term outcomes after distal metatarsal telescoping osteotomy and scarf osteotomy for hallux valgus in patients with rheumatoid arthritis. Foot Ankle Surg. Tech. Rep. Cases 2023, 3, 100254. [Google Scholar] [CrossRef]
- Kernozek, T.W.; Sterriker, S.A. Chevron (Austin) distal metatarsal osteotomy for hallux valgus: Comparison of pre- and post-surgical characteristics. Foot Ankle Int. 2002, 23, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Saro, C.; Andrén, B.; Felländer-Tsai, L.; Lindgren, U.; Arndt, A. Plantar pressure distribution and pain after distal osteotomy for hallux valgus: A prospective study of 22 patients with 12-month follow-up. Foot 2007, 17, 84–93. [Google Scholar] [CrossRef][Green Version]
- Haddad, R.J., Jr. Hallux valgus and metatarsus primus varus treated by bunionectomy and proximal metatarsal osteotomy. South. Med. J. 1975, 68, 684–686. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Suh, Y.M.; Yeom, J.W.; Suh, J.S. Comparison of Postoperative Height Changes of the Second Metatarsal among 3 Osteotomy Methods for Hallux Valgus Deformity Correction. Foot Ankle Int. 2017, 38, 20–26. [Google Scholar] [CrossRef]
- Nyska, M.; Liberson, A.; McCabe, C.; Linge, K.; Klenerman, L. Plantar foot pressure distribution in patients with Hallux valgus treated by distal soft tissue procedure and proximal metatarsal osteotomy. Foot Ankle Surg. 1998, 4, 35–41. [Google Scholar] [CrossRef]
- Kraus, J.; Ziegele, M.J.; Wang, M.; Law, B. First Tarsometatarsal Joint Loading After Sequential Correction of Hallux Valgus Using a Proximal Opening Wedge Metatarsal Osteotomy and Distal Soft Tissue Procedure. Foot Ankle Orthop. 2021, 6, 24730114211026934. [Google Scholar] [CrossRef] [PubMed]
- Takao, M.; Komatsu, F.; Oae, K.; Miyamoto, W.; Uchio, Y.; Ochi, M.; Matsushita, T. Proximal oblique-domed osteotomy of the first metatarsal for the treatment of hallux valgus associate with flat foot: Effect to the correction of the longitudinal arch of the foot. Arch. Orthop. Trauma Surg. 2007, 127, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Takakura, Y.; Kumai, T.; Sugimoto, K.; Taniguchi, A.; Hattori, K. Proximal spherical metatarsal osteotomy for the foot with severe hallux valgus. Foot Ankle Int. 2008, 29, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Larholt, J.; Kilmartin, T.E. Rotational scarf and akin osteotomy for correction of hallux valgus associated with metatarsus adductus. Foot Ankle Int. 2010, 31, 220–228. [Google Scholar] [CrossRef]
- Dhukaram, V.; Hullin, M.G.; Kumar, C.S. The Mitchell and Scarf Osteotomies for Hallux Valgus Correction: A Retrospective, Comparative Analysis Using Plantar Pressures. J. Foot Ankle Surg. 2006, 45, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, F.O.L.; Verburg, H.; Reininga, I.; van Raaij, T. Chevron versus Mitchell osteotomy in hallux valgus surgery: A comparative study. J. Foot Ankle Surg. 2015, 54, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Imakiire, A.; Katori, Y.; Masaoka, T.; Koizumi, R. Clinical results of modified Mitchell’s osteotomy for hallux valgus augmented with oblique lesser metatarsal osteotomy. J. Orthop. Surg. 2005, 13, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Melai, T.; Ijzerman, T.H.; Schaper, N.C.; de Lange, T.L.; Willems, P.J.; Meijer, K.; Lieverse, A.G.; Savelberg, H.H. Calculation of plantar pressure time integral, an alternative approach. Gait Posture 2011, 34, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Arin-Bal, G.; Livanelioglu, A.; Leardini, A.; Belvedere, C. Correlations between plantar pressure and postural balance in healthy subjects and their comparison according to gender and limb dominance: A cross-sectional descriptive study. Gait Posture 2024, 108, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Wilczyński, J.; Paprocki, M. Correlations between foot defects and balance reactions among young school-children. Med. Stud. Stud. Med. 2020, 36, 265–272. [Google Scholar]
- National Institute for Health; Care Research Global Health Research Unit on Global Surgery. Reducing the environmental impact of surgery on a global scale: Systematic review and co-prioritization with healthcare workers in 132 countries. Br. J. Surg. 2023, 110, 804–817. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms |
|---|---|
| PubMed Science Direct Sage Journals | (“pressure distribution”[All Fields] AND (“osteotomy$”[Title] AND “hallux valgus”[Title])) OR ((“foot”[Title] OR “metatarsus”[Title]) AND “osteotomy$”[Title] AND “hallux valgus”[Title])data |
| Ref. | Number of Participants/Cases | Follow-up Duration | Procedure | Summary |
|---|---|---|---|---|
| [12] | Forty-two patients (60 feet) | ≥10 years | Basal Closing Wedge Osteotomy | The article analyzes the results obtained with the procedure for at least ten years and the disadvantages and complications of the long-term process for correcting HVâ and metatarsus primus varus. |
| [13] | Thirty-eight patients (45 feet) | ≥1 years | Distal Chevron Metatarsal Osteotomy | The article analyzes whether the procedure is viable for treating HVâ with metatarsus adductus. |
| [14] | Forty-five patients (47 feet) | ------ | Telescopic Osteotomy, and Scarf Osteotomy | The article compares the short-term results after telescopic osteotomy of the distal MT and scarf osteotomy for hallux valgus in patients with rheumatoid arthritis. |
| [15] | Twenty-five patients | ≥1 years | Chevron Distal Metatarsal Osteotomy | The article compares pre- and post-surgical characteristics of Chevron distal MT osteotomy for hallux valgus. |
| [16] | Twenty-two patients | ≤1 year | Distal Osteotomy | The article analyzes plantar pressure distribution and pain after distal osteotomy for hallux valgus. |
| [17] | Sixteen feet | =3 years | Proximal Metatarsal Osteotomy | The article analyzes the procedure and results for treating HVâ and metatarsus primus varus. |
| [18] | ------ | ≥1 years | Proximal Chevron Metatarsal Osteotomy (PCMO), Scarf Osteotomy, and Distal Chevron Metatarsal Osteotomy (DCMO) | The article compares post-operative changes in the height of the second MT between three osteotomy methods for correcting hallux valgus deformity. |
| [19] | Twenty patients (29 feet) | ------ | Proximal Metatarsal Osteotomy | The article analyzes foot plantar pressure distribution in patients with hallux valgus treated by distal soft tissue procedure and proximal MT osteotomy. |
| [20] | Five fresh-frozen cadaveric below-knee specimens | ------ | Proximal Opening Wedge Metatarsal Osteotomy | The article reviews the first tarsometatarsal joint loading after sequential hallux valgus correction using a proximal opening wedge MT osteotomy and distal soft tissue procedure. |
| [21] | Twenty-two patients (27 feet) | ≥2 years | Proximal Oblique Domed Osteotomy | The article analyzes the procedure for treating HVâ associated with a flat foot. |
| [22] | Thirty-seven patients (48 feet) | >2 years <8 | Proximal Spherical Metatarsal Osteotomy | The article reviews the procedure for treating severe HVâ. |
| [23] | Twenty-seven patients (38 feet) | =5 years | Rotational Scarf Osteotomy | The article analyzes the procedure for correcting HVâ associated with the MT adductus. |
| [24] | Twenty-eight patients | >1 years <5 | Mitchell and Scarf Osteotomies | The article takes a retrospective, comparative analysis using plantar pressures from the Mitchell and scarf osteotomies for hallux valgus correction. |
| [25] | Eighty-four patients | ------ | Chevron and Mitchell Osteotomy | The article compares Chevron versus Mitchell osteotomy in hallux valgus surgery. |
| [26] | Fifty-three patients (93 feet) | ≥5 years | Modified Mitchell Osteotomy and Oblique Lesser Metatarsal Osteotomy | The article presents the clinical results of modified Mitchell osteotomy for augmented hallux valgus with oblique lesser MT osteotomy. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, M.; Roseiro, L.; Cortesão Seiça, E.; Amaro, A.M. A Systematic Review of Osteotomies to Correct Hallux Valgus in the First Metatarsal. Appl. Sci. 2024, 14, 3043. https://doi.org/10.3390/app14073043
Santos M, Roseiro L, Cortesão Seiça E, Amaro AM. A Systematic Review of Osteotomies to Correct Hallux Valgus in the First Metatarsal. Applied Sciences. 2024; 14(7):3043. https://doi.org/10.3390/app14073043
Chicago/Turabian StyleSantos, M., L. Roseiro, E. Cortesão Seiça, and A. M. Amaro. 2024. "A Systematic Review of Osteotomies to Correct Hallux Valgus in the First Metatarsal" Applied Sciences 14, no. 7: 3043. https://doi.org/10.3390/app14073043
APA StyleSantos, M., Roseiro, L., Cortesão Seiça, E., & Amaro, A. M. (2024). A Systematic Review of Osteotomies to Correct Hallux Valgus in the First Metatarsal. Applied Sciences, 14(7), 3043. https://doi.org/10.3390/app14073043