
3D Printing Approach in Maxillofacial Surgery in Iran: An Evaluation Using the Non-Adoption, Abandonment, Scale-Up, Spread, and Sustainability (NASSS) Framework

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
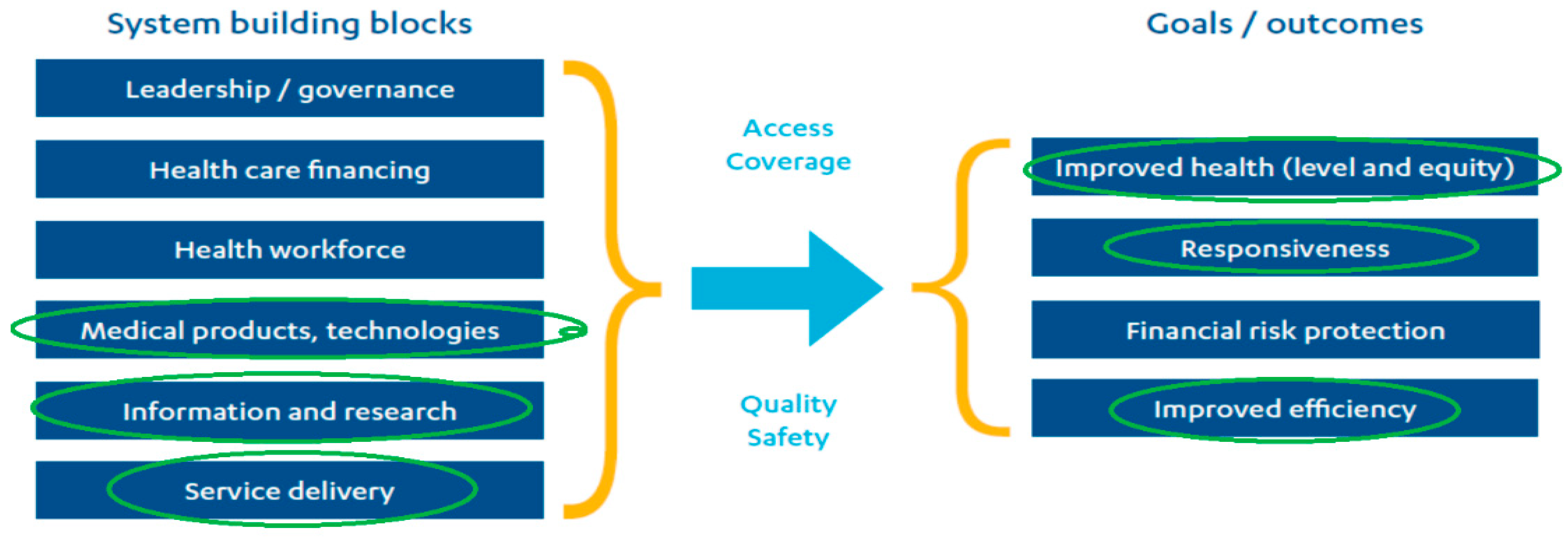
3.1. WHO Framework
3.1.1. System Building Blocks
Service Delivery
Health Information Systems
Medicinal Products and Technology
3.1.2. Outcomes
Improve Health
Responsiveness
Improve Efficiency
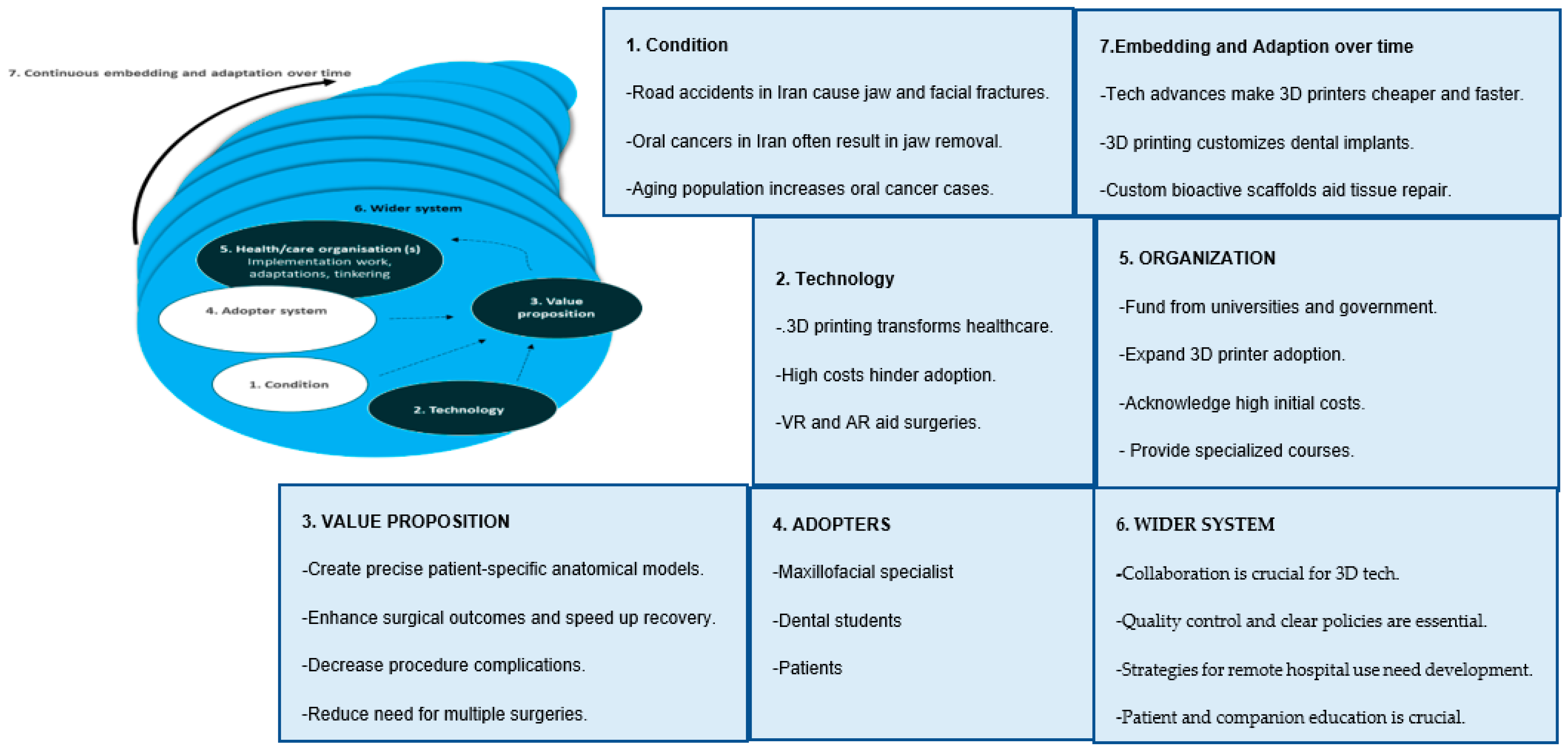
3.2. NASSS Framework
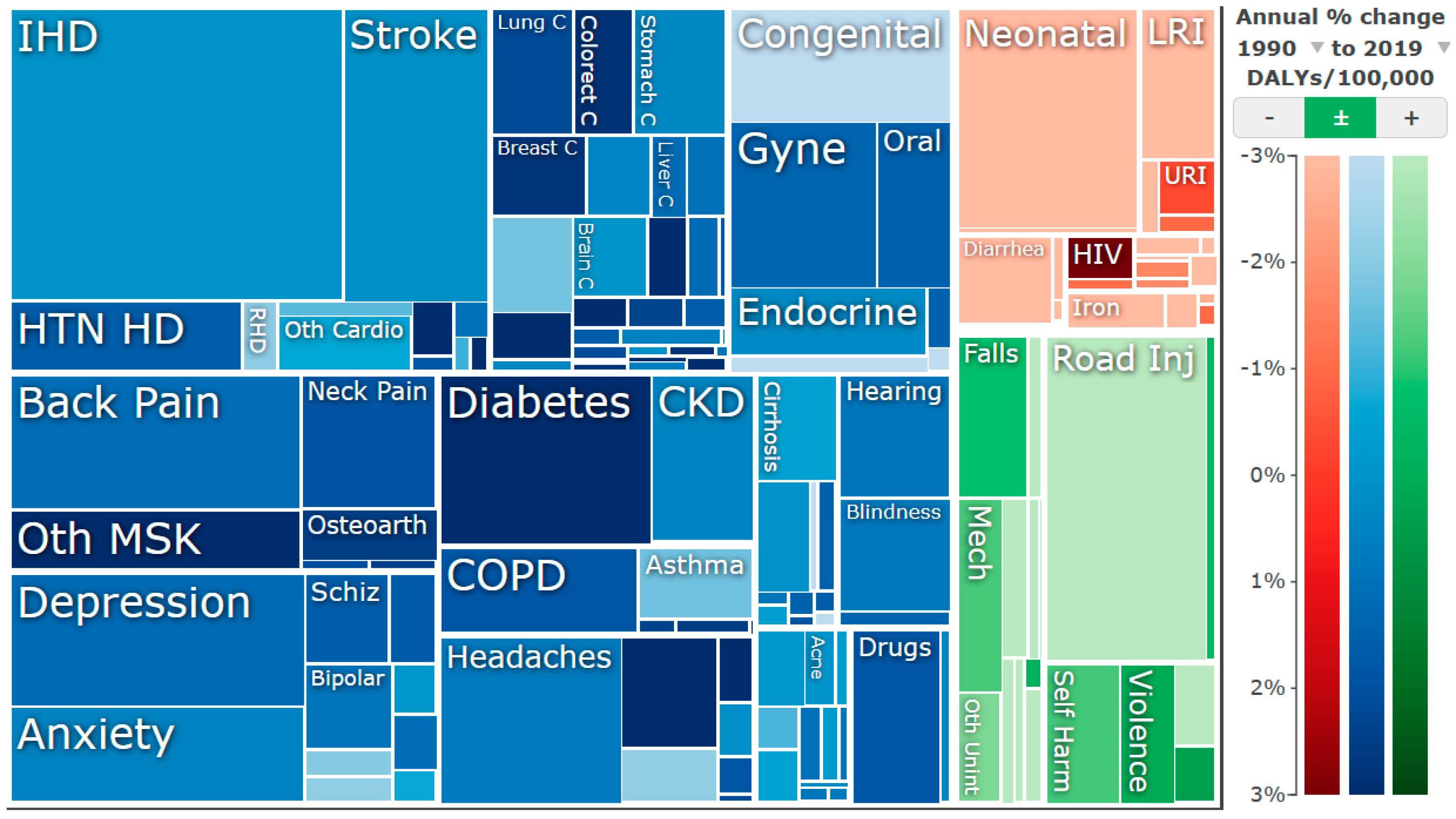
3.2.1. Condition
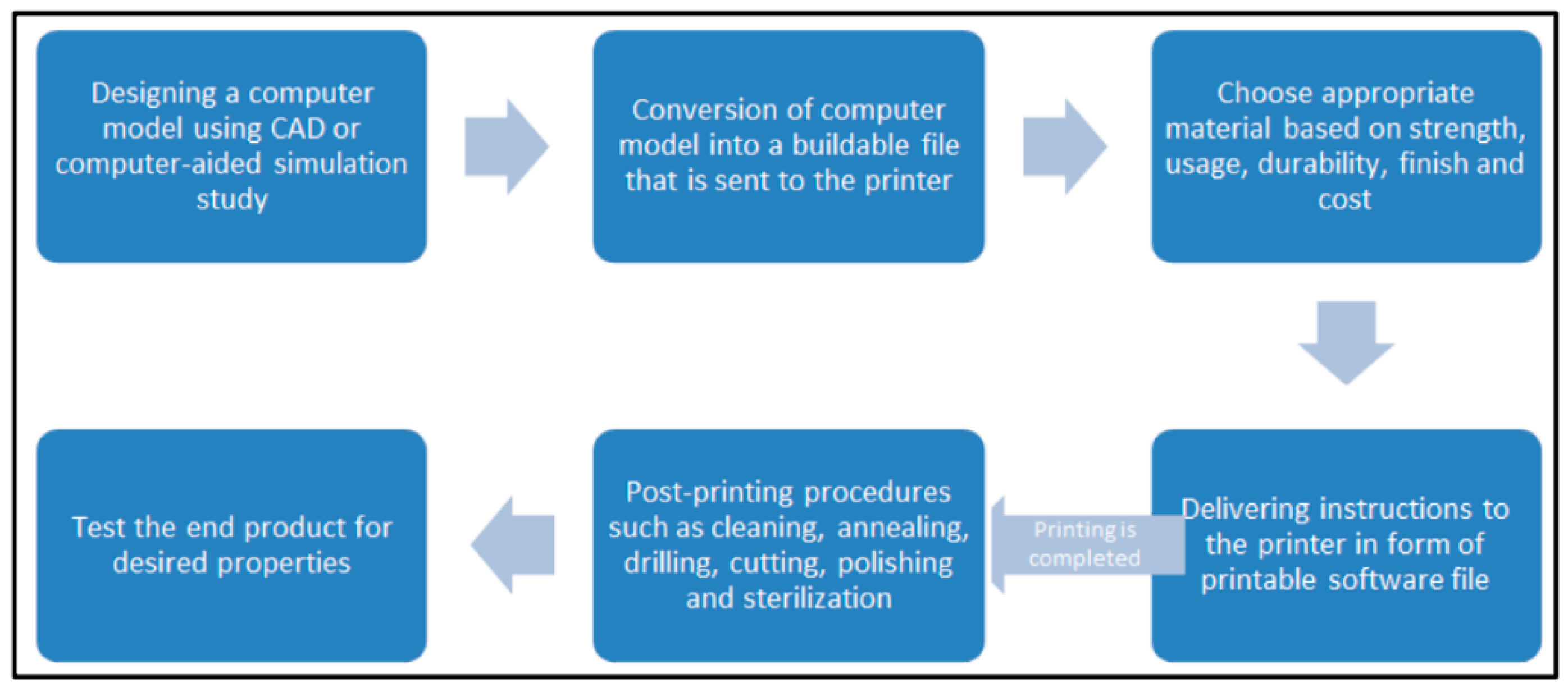
3.2.2. Technology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stereolithography (SLA) | Fused Deposition Modeling (FDM) | Selective Laser Sintering (SLS) | |
|---|---|---|---|
| Materials for printing |
|
|
|
| Approximate Accuracy | 50 to 55 μm | 35 to 40 μm | 45 to 50 μm |
3.2.3. Value Proposition
3.2.4. Adopters
3.2.5. Organization(s)
3.2.6. Wider System
Political/Policy Context
Regulatory/Legal Issues
Sociocultural Context
3.2.7. Embedding and Adaption over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Turek, P.; Pakla, P.; Budzik, G.; Lewandowski, B.; Przeszłowski, Ł.; Dziubek, T.; Wolski, S.; Frańczak, J. Procedure Increasing the Accuracy of Modelling and the Manufacturing of Surgical Templates with the Use of 3D Printing Techniques, Applied in Planning the Procedures of Reconstruction of the Mandible. J. Clin. Med. 2021, 10, 5525. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Abimbola, S. The NASSS Framework—A Synthesis of Multiple Theories of Technology Implementation. Stud. Health Technol. Inform. 2019, 263, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Hushie, M.; Suhuyini Salifu, R.; Seidu, I. Strengthening International Health Security by Embedding the Role of Civil Society Organizations in National Health Systems: Lessons from the 2014–2016 West Africa Ebola Response. In Contemporary Developments and Perspectives in International Health Security—Volume 1; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Abimbola, S.; Patel, B.; Peiris, D.; Patel, A.; Harris, M.; Usherwood, T.; Greenhalgh, T. The NASSS framework for ex post theorisation of technology-supported change in healthcare: Worked example of the TORPEDO programme. BMC Med. 2019, 17, 233. [Google Scholar] [CrossRef] [PubMed]
- Stilgoe, J.; Owen, R.; Macnaghten, P. Developing a framework for responsible innovation. Res. Policy 2013, 42, 1568–1580. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’Court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J. Med. Internet Res. 2017, 19, e367. [Google Scholar] [CrossRef]
- Winter, P.D.; Chico, T.J.A. Using the Non-Adoption, Abandonment, Scale-Up, Spread, and Sustainability (NASSS) Framework to Identify Barriers and Facilitators for the Implementation of Digital Twins in Cardiovascular Medicine. Sensors 2023, 23, 6333. [Google Scholar] [CrossRef]
- World Health Organisation. 2020. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 5 January 2021).
- James, H.M.; Papoutsi, C.; Wherton, J.; Greenhalgh, T.; Shaw, S.E. Spread, scale-up, and sustainability of video consulting in health care: Systematic review and synthesis guided by the NASSS framework. J. Med. Internet Res. 2021, 23, e23775. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’Court, C.; Hinder, S.; Procter, R.; Shaw, S. Analysing the role of complexity in explaining the fortunes of technology programmes: Empirical application of the NASSS framework. BMC Med. 2018, 16, 66. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.D.; Hamovitch, E.; Gatov, E.; MacKinnon, M.; Samawi, L.; Boateng, R.; Thorpe, K.E.; Barwick, M. The NASSS (Non-Adoption, Abandonment, Scale-Up, Spread and Sustainability) framework use over time: A scoping review. medRxiv 2023, 2023-11. [Google Scholar] [CrossRef]
- Everybody Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; WHO: Geneva, Switzerland, 2007.
- World Health Organization. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Louvrier, A.; Marty, P.; Barrabé, A.; Euvrard, E.; Chatelain, B.; Weber, E.; Meyer, C. How useful is 3D printing in maxillofacial surgery? Journal of Stomatology, Oral and Maxillofacial Surgery. J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 230–235. [Google Scholar]
- Meyer-Szary, J.; Luis, M.S.; Mikulski, S.; Patel, A.; Schulz, F.; Tretiakow, D.; Fercho, J.; Jaguszewska, K.; Frankiewicz, M.; Pawłowska, E.; et al. The Role of 3D Printing in Planning Complex Medical Procedures and Training of Medical Professionals—Cross-Sectional Multispecialty Review. J. Clin. Med. 2022, 19, 3331. [Google Scholar] [CrossRef]
- Zoabi, A.; Redenski, I.; Oren, D.; Kasem, A.; Zigron, A.; Daoud, S.; Moskovich, L.; Kablan, F.; Srouji, S. 3D printing and virtual surgical planning in oral and maxillofacial surgery. J. Clin. Med. 2022, 11, 2385. [Google Scholar] [CrossRef]
- Pourabbasi, A.; Akbari, H.; Akhvan, A.A.; Haghdoost, A.A.; Kheiry, Z.; Dehnavieh, R.; Rahimi, H.; Larijani, B. Analysis of Iran’s National Medical Education Evolution and Innovation Plan using the Michelle and Scott’s model of policymaking. J. Adv. Med. Educ. Prof. 2019, 7, 20–26. [Google Scholar] [CrossRef]
- Ballard, D.H.; Mills, P.; Duszak, R., Jr.; Weisman, J.A.; Rybicki, F.J.; Woodard, P.K. Medical 3D printing cost-savings in orthopedic and maxillofacial surgery: Cost analysis of operating room time saved with 3D printed anatomic models and surgical guides. Acad. Radiol. 2020, 27, 1103–1113. [Google Scholar] [CrossRef]
- World Life Expectancy (n.d.). Oral Cancer in Iran. Available online: http://worldlifeexpectancy.com/iran-oral-cancer (accessed on 14 April 2023).
- Azami, R.; Hosseini, S.M.; Alimohammadzadeh, K.; Jafari, M.; Bahadori, M.K. International Sanctions and the Procurement of Medical Equipment in Iran: A Qualitative Study. Med. J. Islam. Repub. Iran 2021, 35, 180. [Google Scholar] [CrossRef] [PubMed]
- Keyhan, S.O.; Jahangirnia, A.; Fallahi, H.R.; Navabazam, A.; Ghanean, S. Three-dimensional printer-assisted reduction genioplasty; surgical guide fabrication. J. Clin. Diagn. Res. JCDR 2016, 10, ZD25–ZD27. [Google Scholar]
- Keyhan, S.O.; Fallahi, H.R.; Azari, A.; Cheshmi, B. Early Assessment of Computer-Assisted Malarplasty: A Novel Methodology for Both Reduction and Augmentation. Aesthetic Plast. Surg. 2019, 43, 329–337. [Google Scholar] [CrossRef]
- Doshmangir, L.; Bazyar, M.; Majdzadeh, R.; Takian, A. So Near, So Far: Four Decades of Health Policy Reforms in Iran, Achievements and Challenges. Arch. Iran. Med. 2019, 22, 592–605. [Google Scholar]
- Institute for Health Metrics and Evaluation. GBD Compare. [Online] Healthdata.org. 2019. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 17 February 2024).
- iPleaders. What Are the Legal Issues Related to 3D Printing in Medicine and Healthcare. 2021. Available online: https://blog.ipleaders.in/what-are-the-legal-issues-related-to-3d-printing-in-medicine-and-healthcare/?amp=1 (accessed on 14 April 2023).
- Arabion, H.R.; Tabrizi, R.; Aliabadi, E.; Gholami, M.; Za, K. A Retrospective Analysis of Maxillofacial Trauma in Shiraz, Iran: A 6-Year- Study of 768 Patients (2004–2010). J. Craniofacial Surg. 2014, 25, 404–407. [Google Scholar]
- Najafi, S.; Khayamzadeh, M.; Ghavamabad, A.J.; Moradi, F.; Bafrouii, S.D. A 5 year Epidemiological Study on Oral and Pharyngeal Cancers from Cancer Registration Centers in Tehran. J. Iran. Med. Counc. 2018, 1, 63–68. [Google Scholar]
- Mesgarzadeh, A.H.; Shahamfar, M.; FeiziAzar, S.; Shahamfar, J. Analysis of the pattern of maxillofacial fractures in north western of Iran: A retrospective study. J. Emerg. Trauma Shock. 2011, 4, 48–52. [Google Scholar] [CrossRef]
- Noureldin, M.G.; Dessoky, N.Y. 3D Printing: Towards the Future of Oral and Maxillofacial Surgery. Acta Sci. Dent. Sci. 2020, 4, 107–112. [Google Scholar] [CrossRef]
- Jones, A.; Griffin, J. 3D Printing and the Right to Privacy: Proposals for a Regulatory Framework. Eur. J. Law Technol. 2020, 11. Available online: https://ejlt.org/index.php/ejlt/article/view/743 (accessed on 14 April 2023).
- Madeleine, P. The Integration of 3D Printing in Hospitals. 3Dnatives. 2022. Available online: https://www.3dnatives.com/en/the-integration-of-3d-printing-in-hospitals-190920224/amp (accessed on 14 April 2023).
- Hadad, H.; Boos Lima, F.B.; Shirinbak, I.; Porto, T.S.; Chen, J.E.; Guastaldi, F.P. The impact of 3D printing on oral and maxillofacial surgery. J. 3D Print. Med. 2023, 7, 3DP007. [Google Scholar] [CrossRef]
- Sarkarat, F.; Tofighi, O.; Jamilian, A.; Fateh, A.; Abbaszadeh, F. Are Virtually Designed 3D Printed Surgical Splints Accurate Enough for Maxillary Reposition as an Intermediate Orthognathic Surgical Guide. J. Maxillofac. Oral Surg. 2023, 22, 861–872. [Google Scholar] [CrossRef]
- Gupta, H.; Bhateja, S.; Arora, G. 3D printing and its applications in oral and maxillofacial surgery. Natl. J. Maxillofac. Surg. 2019, 13 (Suppl. S1), S203–S211. [Google Scholar]
- Kamio, T.; Onda, T. Fused Deposition modeling 3d printing in Oral and Maxillofacial surgery: Problem and solutions. Cureus 2022, 14, e28906. [Google Scholar] [CrossRef]
- First Maxillofacial Surgery with 3D Printer in Iran. Financial Tribune. 7 February 2015. Available online: https://financialtribune.com/articles/people/16945/first-maxillofacial-surgery-with-3d-printer-in-iran (accessed on 17 February 2024).
- Wang, X.; Shujaat, S.; Shaheen, E.; Jacobs, R. Accuracy of desktop versus professional 3D prnters for maxillofacial model production. A systematic review and meta-analysis. J. Dent. 2021, 112, 103741. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.F.; Alfi, D.; Alfi, J.; Huang, A.T. The Use of Patient-Specific Implants in Oral and Maxillofacial Surgery. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 593–600. [Google Scholar] [CrossRef]
- Abbasi, A.J.; Azari, A.; Mohebbi, S.Z.; Javani, A. Mandibular Rami Implant: A New Approach in Mandibular Reconstruction. J. Oral Maxillofac. Surg. 2017, 75, 2550–2558. [Google Scholar] [CrossRef]
- Oberoi, G.; Nitsch, S.; Edelmayer, M.; Janjic, K.; Müller, A.S.; Agis, H. 3D Printing-Encompassing the Facets of Dentistry. J. Clin. Med. 2018, 7, 451. [Google Scholar] [CrossRef] [PubMed]
- Pillai, S.; Upadhyay, A.; Khayambashi, P.; Farooq, I.; Sabri, H.; Tarar, M.; Lee, K.T.; Harb, I.; Zhou, S.; Wang, Y.; et al. Dental 3D-Printing: Transferring Art from the Laboratories to the Clinics. Polymers 2021, 13, 157. [Google Scholar] [CrossRef] [PubMed]
- Ostaș, D.; Almășan, O.; Ileșan, R.R.; Andrei, V.; Thieringer, F.M.; Hedeșiu, M.; Rotar, H. Point-of-care virtual surgical planning and 3D printing in oral and cranio-maxillofacial surgery: A narrative review. J. Clin. Med. 2022, 11, 6625. [Google Scholar] [CrossRef] [PubMed]
- Martelli, N.; Serrano, C.; van den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef] [PubMed]
- RegDesk (n.d.). Iran Medical Device Regulations. Available online: https://www.regdesk.co/resource-library/iran/amp/ (accessed on 14 April 2023).
- Khorrami, F.; Ahmadi, M.; Alizadeh, A.; Roozbeh, N.; Mohseni, S. Information needs assessment of medical equipment offices based on Critical Success Factors (CSF) and Business System Planning (BSP) methods. J. Med. Life 2015, 8, 1–7. [Google Scholar]
- irimc.org (n.d.). IRI Medical Council > Regulations > Dentistry Education. Available online: https://irimc.org/en/Regulations/Dentistry-Education (accessed on 14 April 2023).
- Petrova, I.; Dzhongova, E.; Georgieva, V. Applications of 3D printing in oral and maxillofacial surgery. Scr. Sci. Med. Dent. 2022, 8, 14–21. [Google Scholar] [CrossRef]
- Jamilian, A.; Showkatbakhsh, R.; Behnaz, M.; Ghassemi, A.; Kamalee, Z.; Perillo, L. Tooth-borne distraction osteogenesis versus conventional Le Fort I in maxillary advancement of cleft lip and palate patients. Minerva Stomatol. 2018, 67, 117–124. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farjaminejad, R.; Farjaminejad, S.; Nucci, L.; d’Apuzzo, F.; Grassia, V.; Majidi, K.; Jamilian, A. 3D Printing Approach in Maxillofacial Surgery in Iran: An Evaluation Using the Non-Adoption, Abandonment, Scale-Up, Spread, and Sustainability (NASSS) Framework. Appl. Sci. 2024, 14, 3075. https://doi.org/10.3390/app14073075
Farjaminejad R, Farjaminejad S, Nucci L, d’Apuzzo F, Grassia V, Majidi K, Jamilian A. 3D Printing Approach in Maxillofacial Surgery in Iran: An Evaluation Using the Non-Adoption, Abandonment, Scale-Up, Spread, and Sustainability (NASSS) Framework. Applied Sciences. 2024; 14(7):3075. https://doi.org/10.3390/app14073075
Chicago/Turabian StyleFarjaminejad, Rosana, Samira Farjaminejad, Ludovica Nucci, Fabrizia d’Apuzzo, Vincenzo Grassia, Korosh Majidi, and Abdolreza Jamilian. 2024. "3D Printing Approach in Maxillofacial Surgery in Iran: An Evaluation Using the Non-Adoption, Abandonment, Scale-Up, Spread, and Sustainability (NASSS) Framework" Applied Sciences 14, no. 7: 3075. https://doi.org/10.3390/app14073075