
Deep Learning-Driven Geospatial Modeling of Elderly Care Accessibility: Disparities Across the Urban-Rural Continuum in Central China


Abstract
:1. Introduction
1.1. Spatial Accessibility and Distribution Optimization of Elderly Care Facilities from a Spatial Justice Perspective
1.2. The 15-Min City and Walkable Life Circles for Older Adults
1.3. Walkability Score and Quantitative Analysis of Street-Level Environments Factory
1.4. Literature Review
2. Study Area and Data
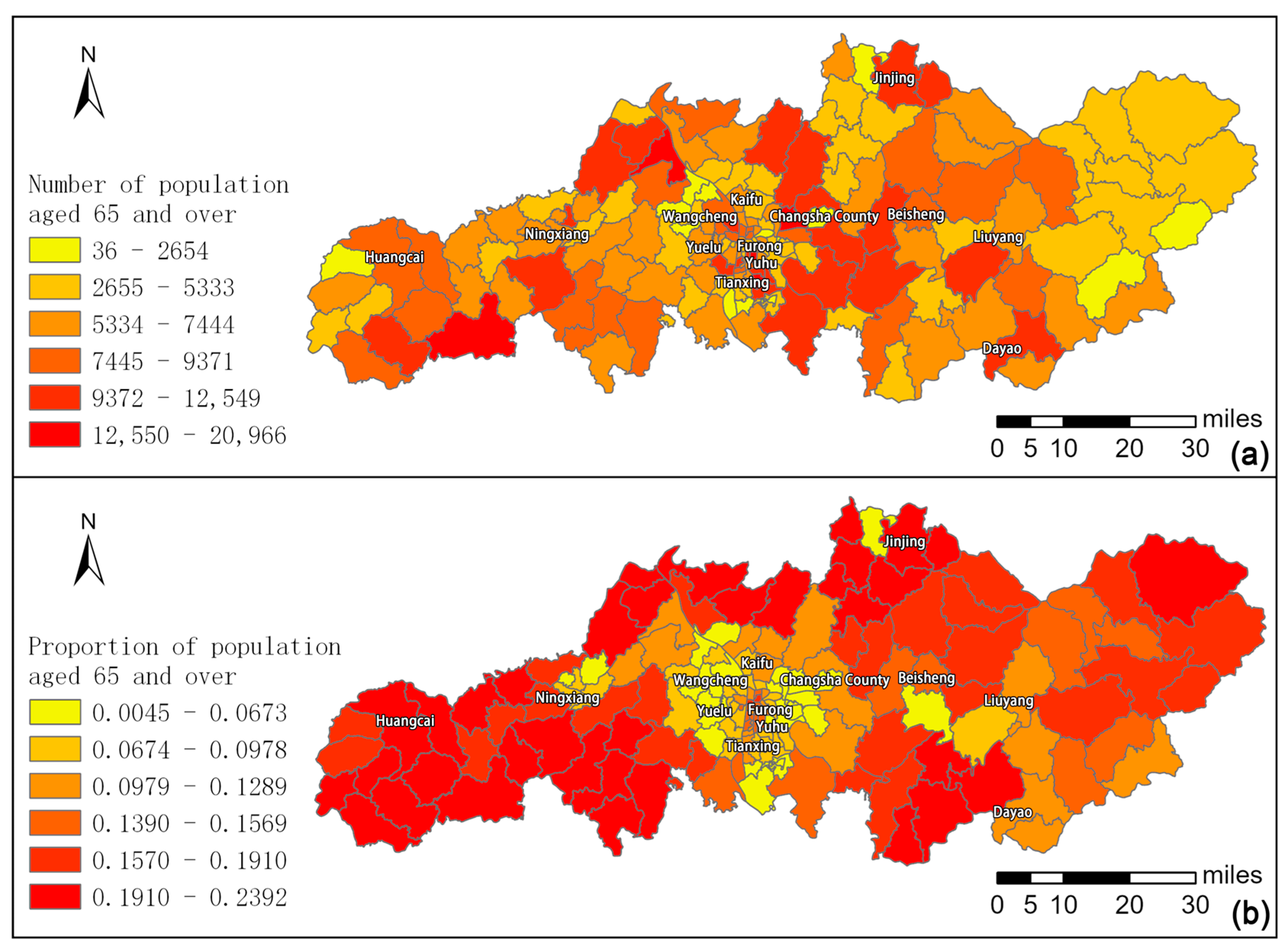
2.1. Study Area
2.2. Data
3. Method
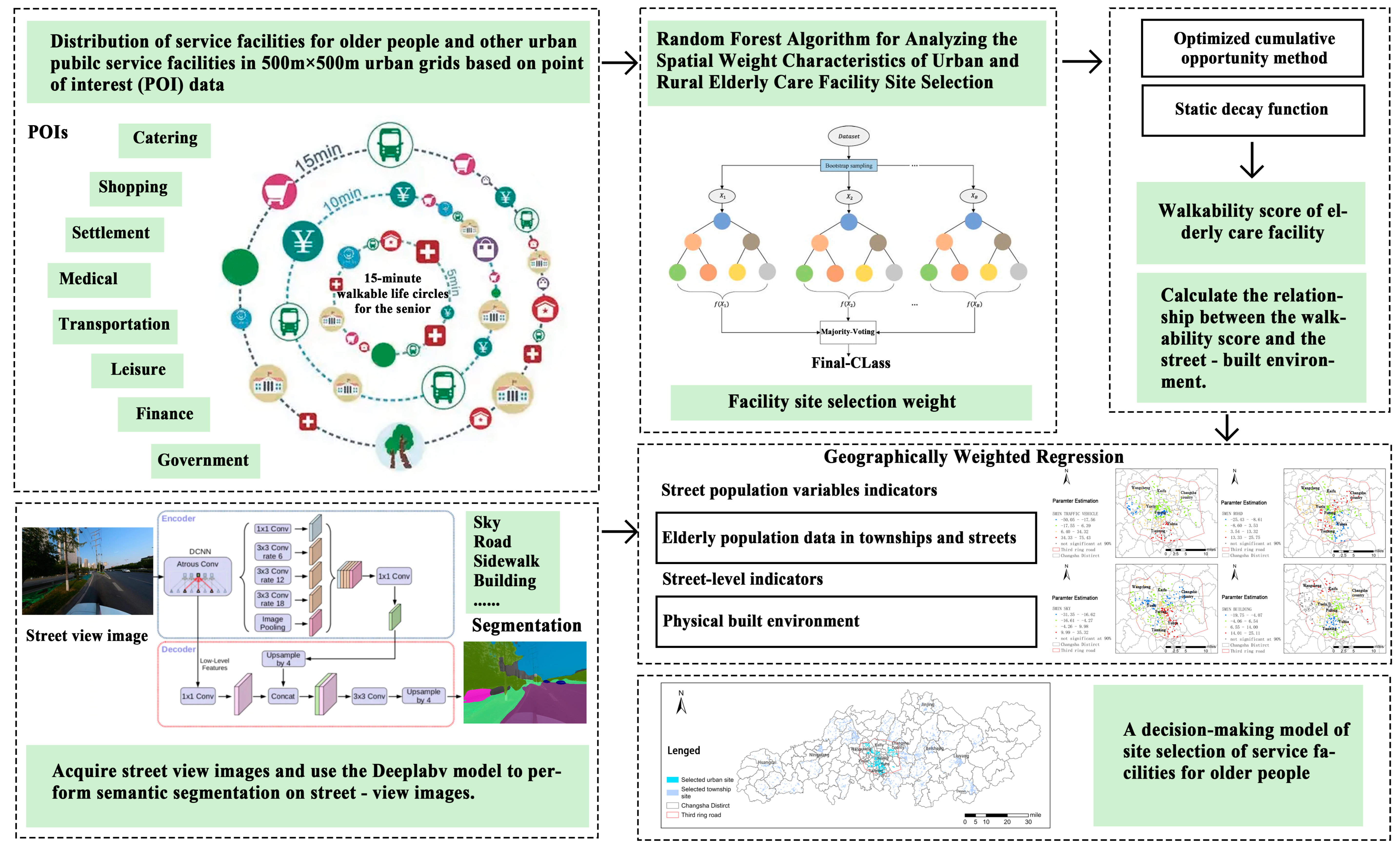
3.1. Selection of POI Facilities and Establishment of the Indicator System
3.2. Facility Grid Division and Walking Time Calculation
3.3. Evaluation of 15-min Walkability to Elderly Care Facilities
3.3.1. Machine Learning-Based Analysis of Facility Importance Weights
3.3.2. Calculation of Walkability Score Based on Optimization Cumulative Opportunity Method
3.4. Regression Model
3.4.1. Ordinary Least Squares
3.4.2. Geographically Weighted Regression (GWR)
4. Results
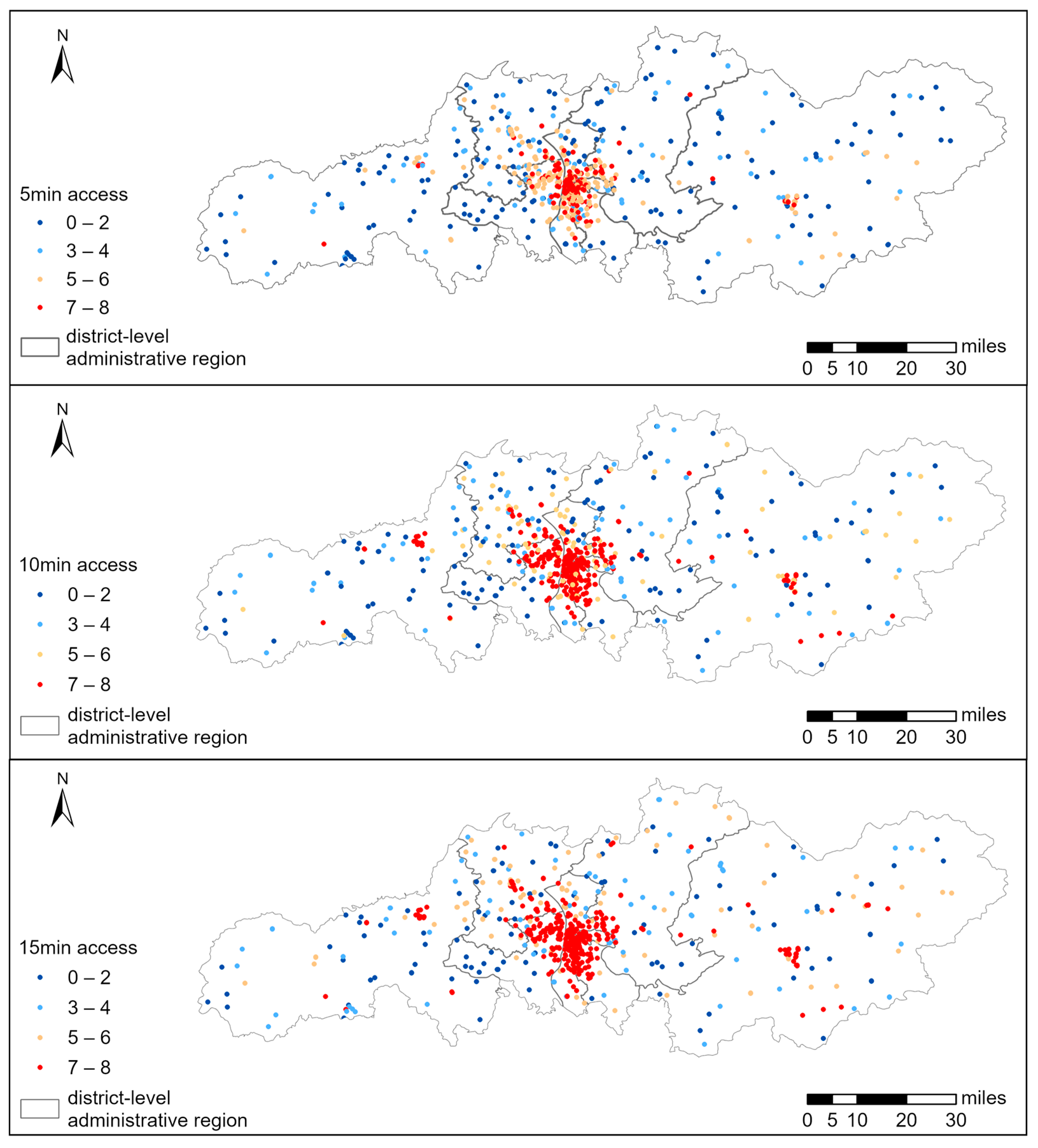
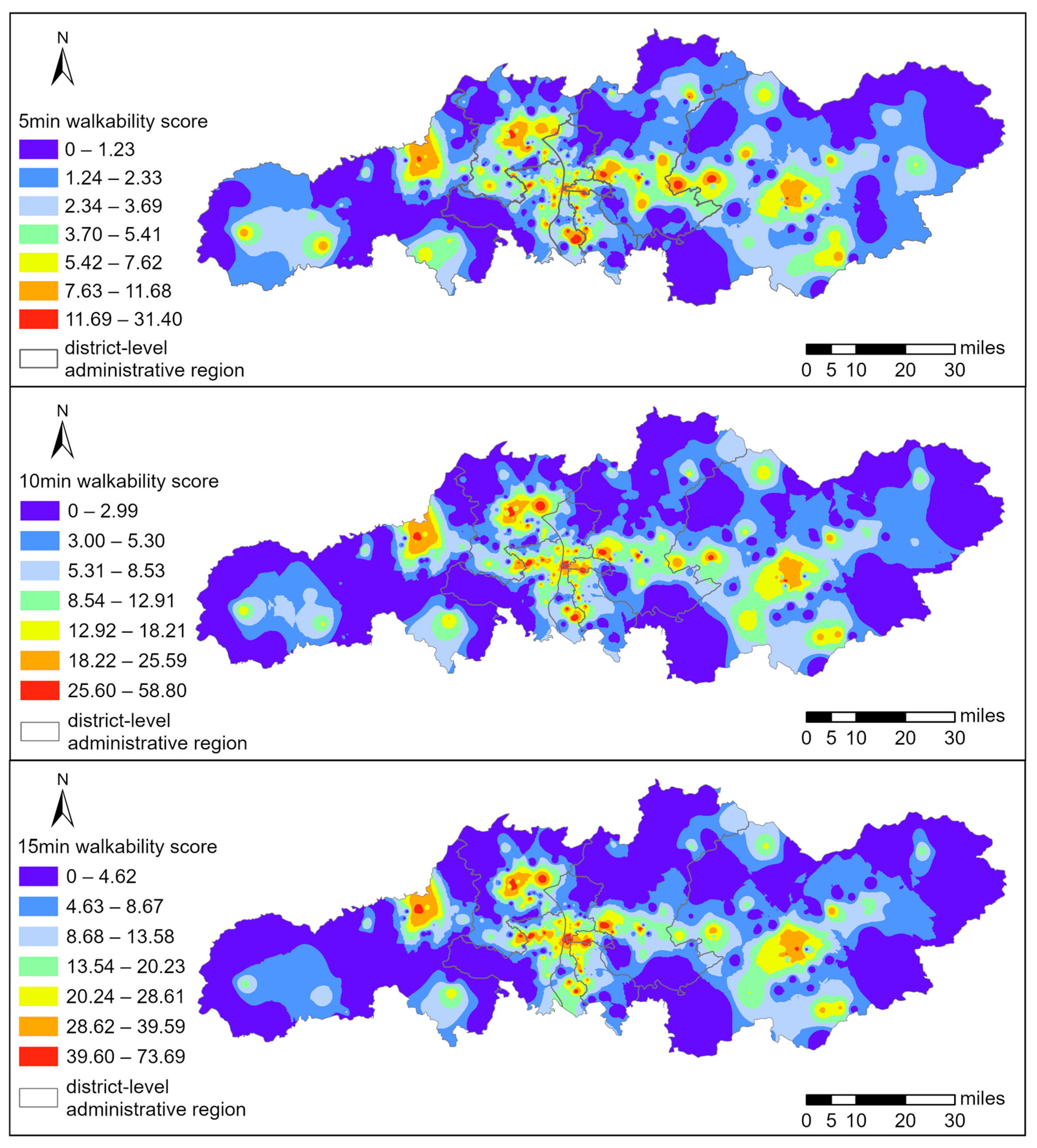
4.1. Service Accessibility for the Elderly Within 5-min, 10-min, and 15-min CLCs
4.2. Walkability Scores of Senior Care Facilities Within 5-min, 10-min, and 15-min Living Circles
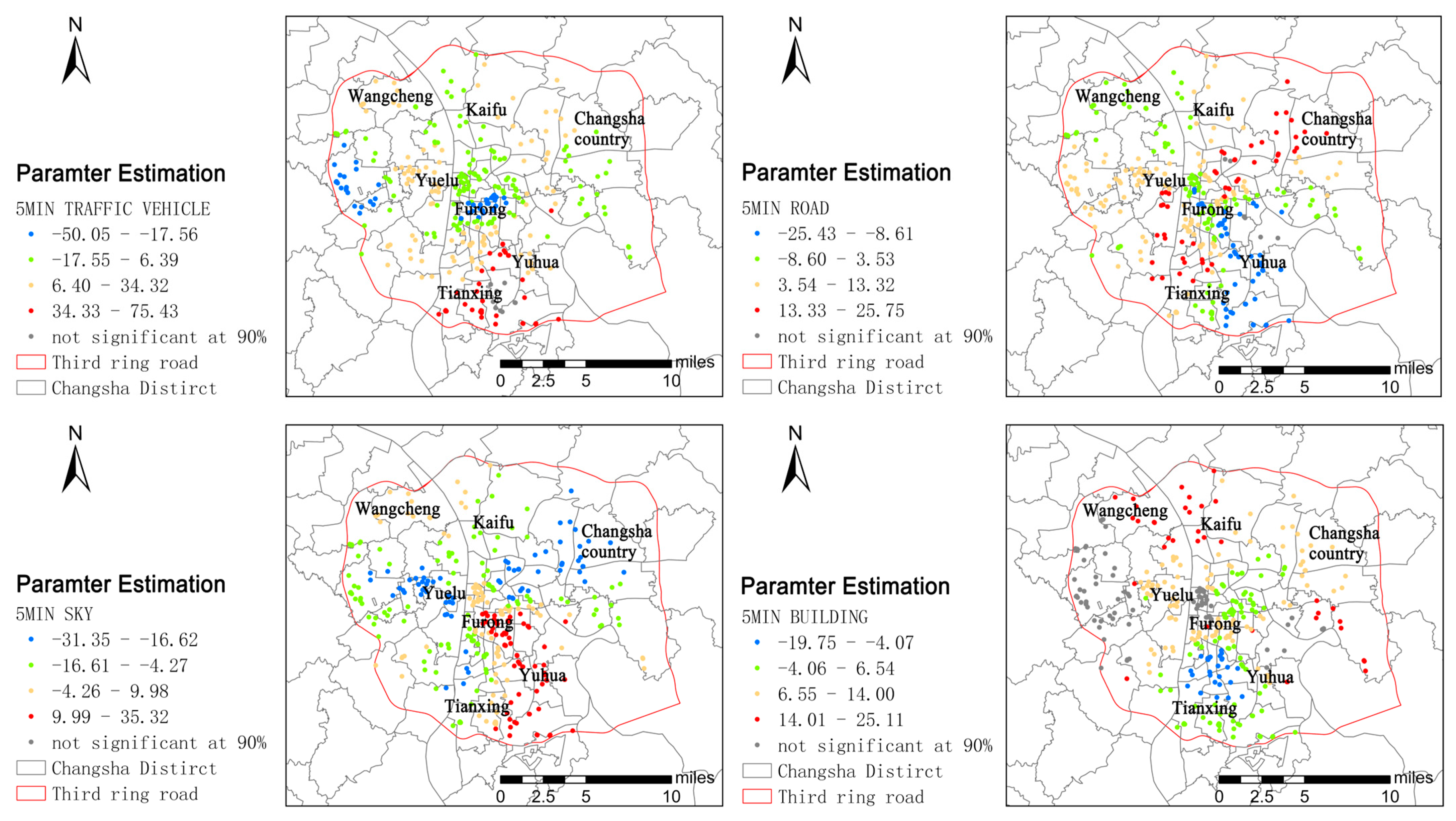
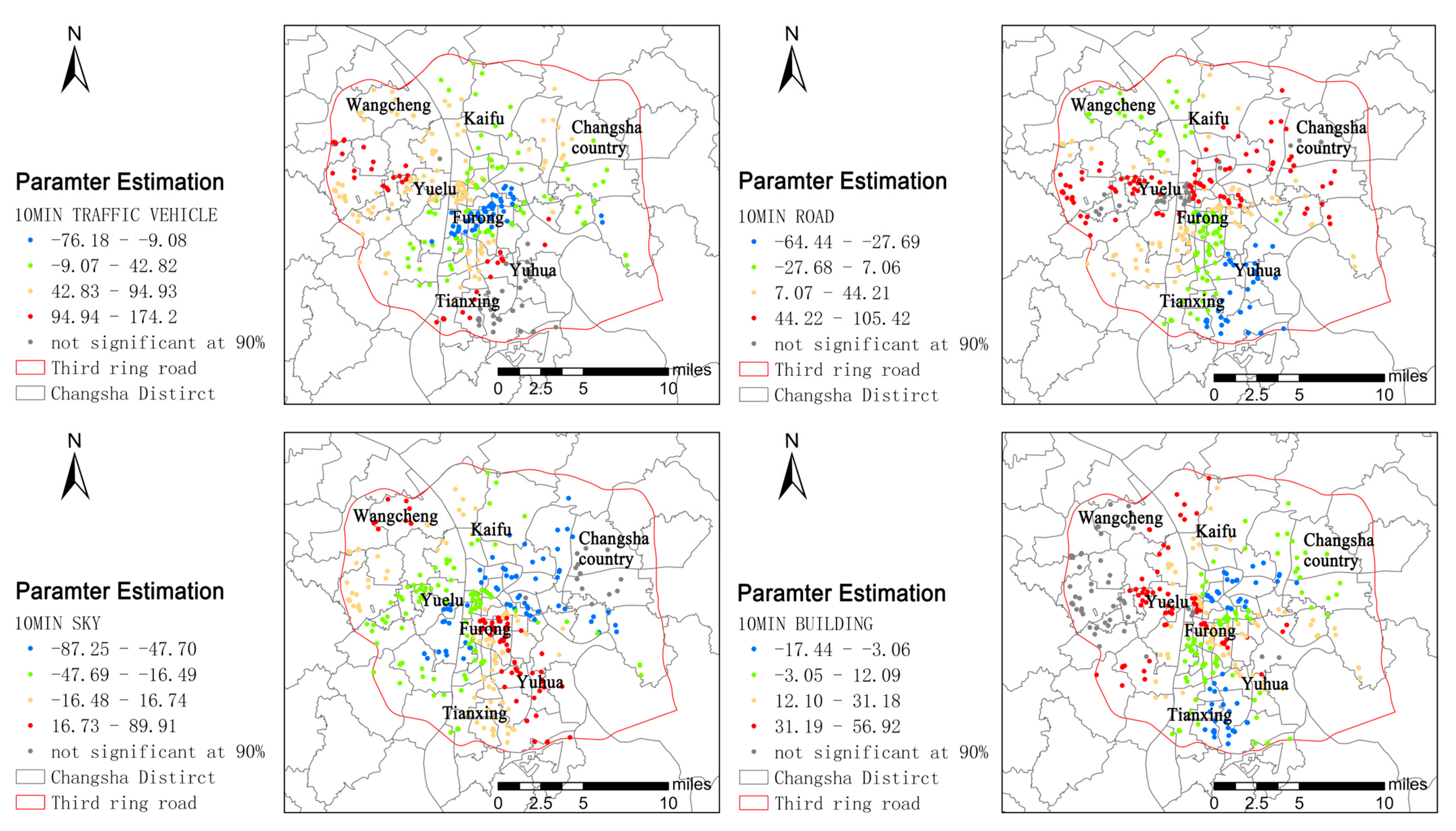
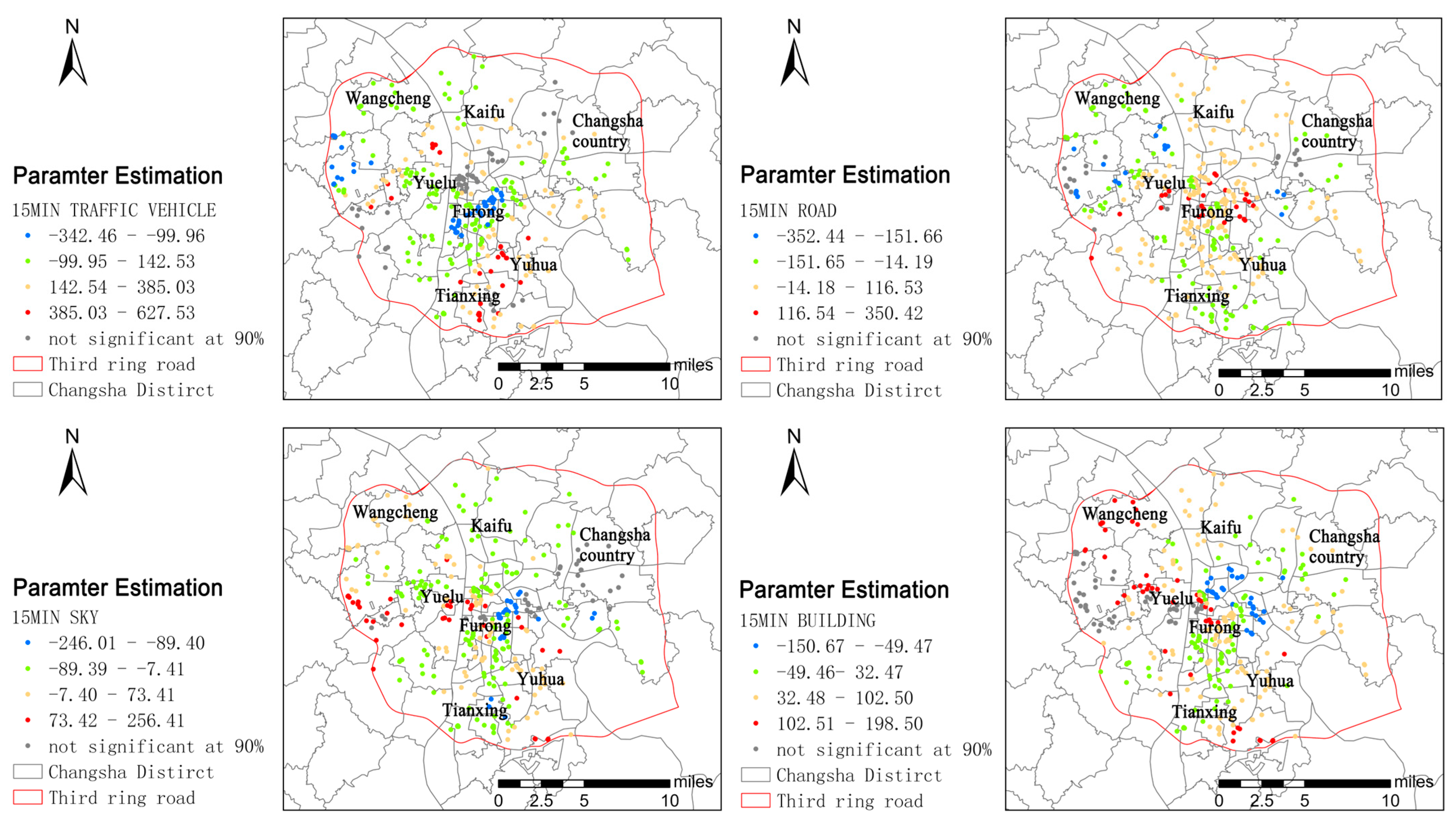
4.3. Multiple Regression Models
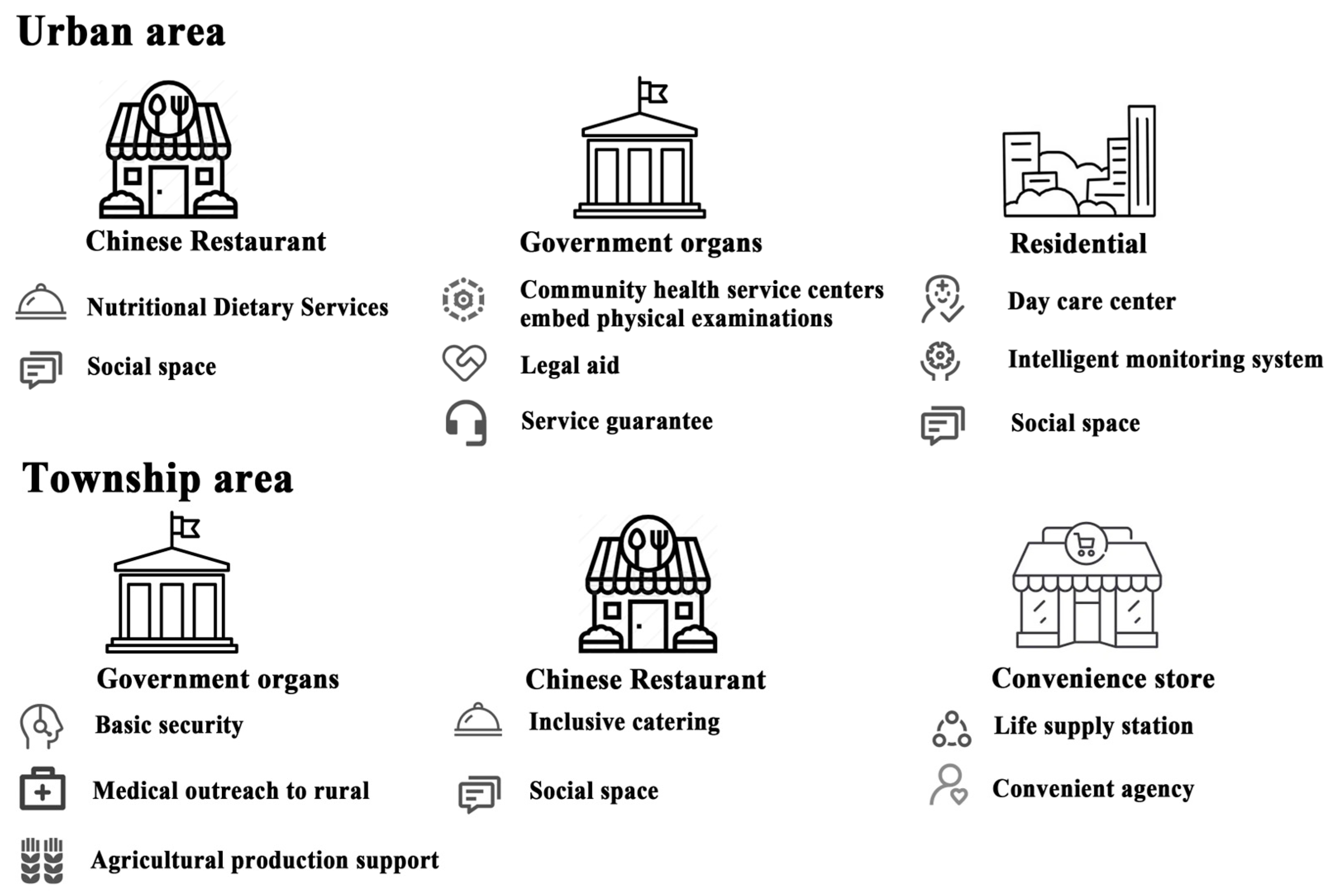
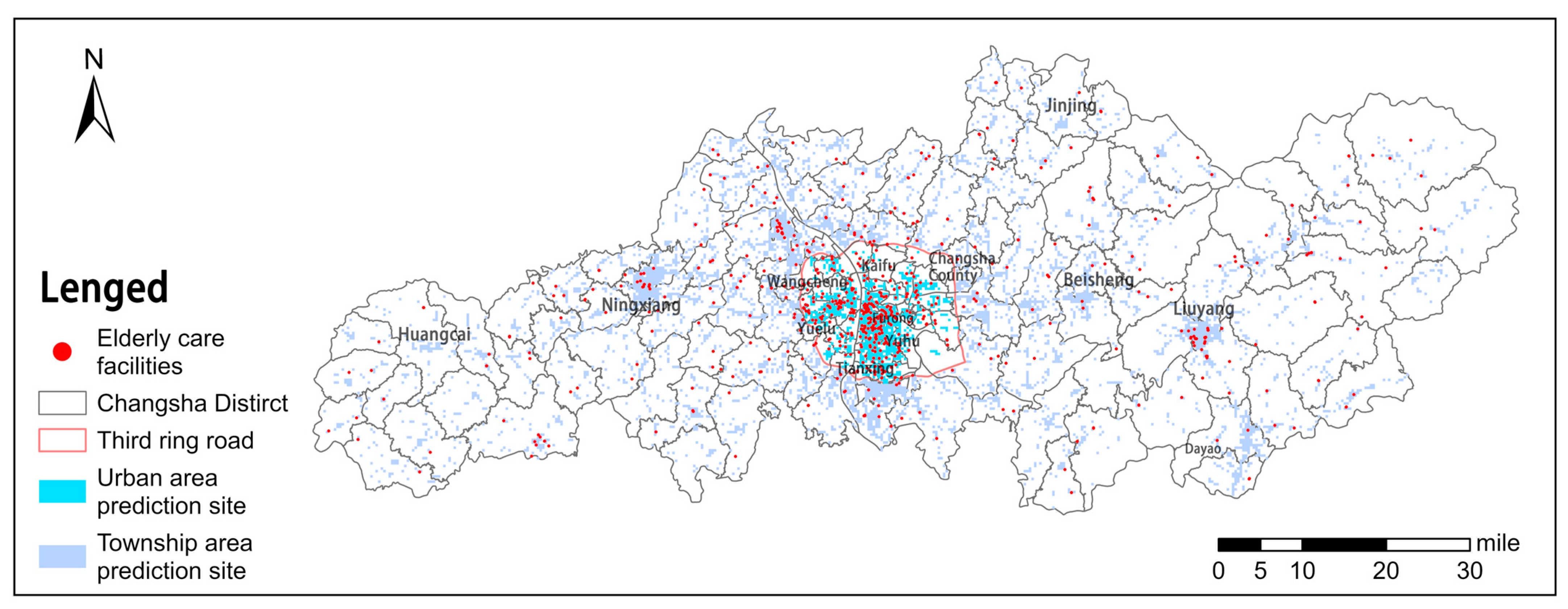
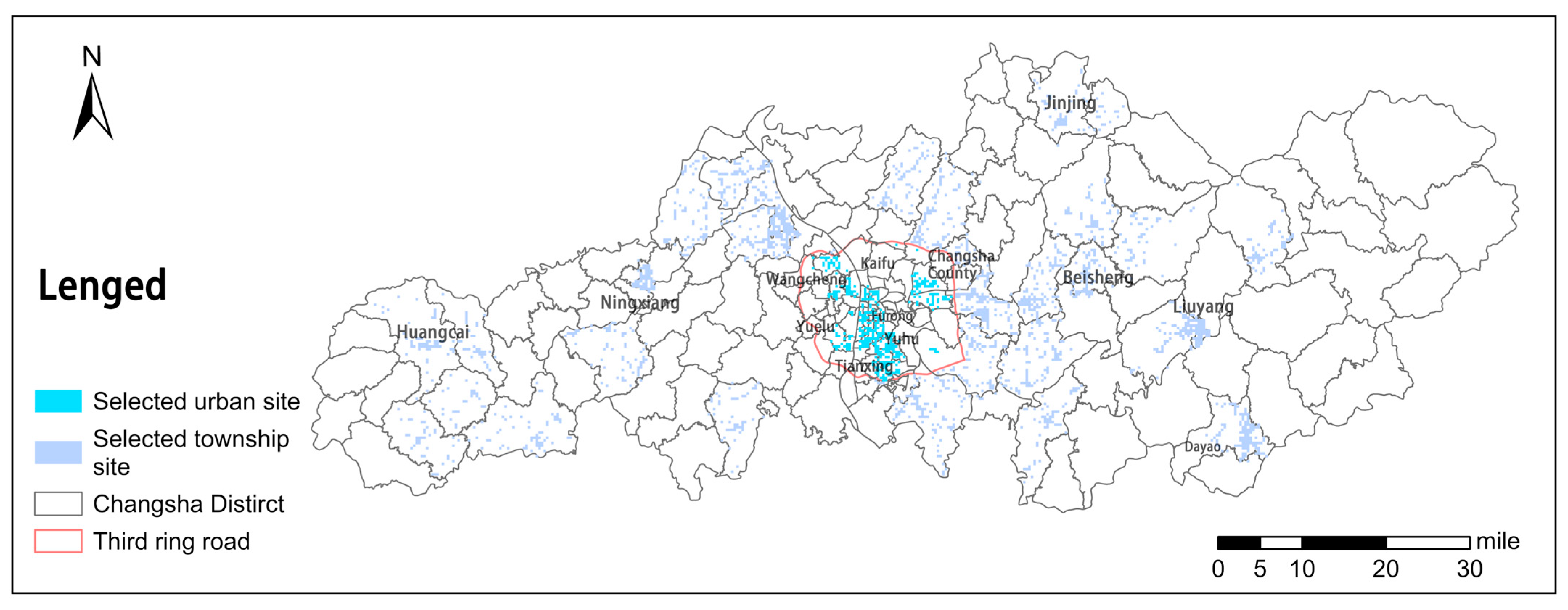
4.4. Prediction of Elderly Care Facility Locations
5. Discussion
6. Conclusions
7. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bloom, D.E.; Canning, D.; Lubet, A. Global Population Aging: Facts, Challenges, Solutions & Perspectives. Daedalus 2015, 144, 80–92. [Google Scholar] [CrossRef]
- Shie, A.J.; Wu, W.F.; Yang, M.; Wan, X.J.; Li, H.L. Design and process optimization of combined medical and elderly care services: An integrated service blueprint-TRIZ model. Front. Public Health 2022, 10, 965443. [Google Scholar] [CrossRef] [PubMed]
- United Nations Department of Economic and Social Affairs, Population Division. World Population Prospects 2024: Summary of Results (UN DESA/POP/2024/TR/NO. 9). United Nations. 2024. Available online: https://www.un.org/development/desa/pd/content/world-population-prospects-2024-summary-results (accessed on 3 February 2025).
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2020 Highlights. United Nations. 2020. Available online: https://www.un.org/development/desa/pd/content/world-population-ageing-2020-highlights (accessed on 3 February 2025).
- Wood, G.E.R.; Pykett, J.; Stathi, A. Active and healthy ageing in urban environments: Laying the groundwork for solution-building through citizen science. Health Promot. Int. 2022, 37, daac126. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ren, H.N.; Li, C. Study on the development characteristics and spatial and temporal patterns of population ageing in 31 central cities in China. Front. Public Health 2024, 12, 1341455. [Google Scholar] [CrossRef]
- Li, H.Y.; Li, R.; Cai, J.; Wang, S.L. The Spatial Equilibrium Model of Elderly Care Facilities with High Spatiotemporal Sensitivity and Its Economic Associations Study. ISPRS Int. J. Geo-Inf. 2024, 13, 268. [Google Scholar] [CrossRef]
- Wang, C.Y.; Geng, X.L. Assessing the spatial equity of the aged care institutions based on the improved potential model: A case study in Shanghai, China. Front. Public Health 2024, 12, 1428424. [Google Scholar] [CrossRef]
- Póczosová, V.; Risová, K. Considering the Preferences of Adults and Elderly Individuals While Examining the Spatial Justice of the Distribution of Urban Facilities: A Case Study of the Small Town of Fiľakovo (Slovakia). Sociologia 2023, 55, 411–433. [Google Scholar] [CrossRef]
- Moreno, C.; Allam, Z.; Chabaud, D.; Gall, C.; Pratlong, F. Introducing the "15-Minute City": Sustainability, Resilience and Place Identity in Future Post-Pandemic Cities. Smart Cities 2021, 4, 93–111. [Google Scholar] [CrossRef]
- Jiang, Z.H.; Wu, C.L.; Chung, H.Y.C. The 15-minute community life circle for older people: Walkability measurement based on service accessibility and street-level built environment—A case study of Suzhou, China. Cities 2025, 157, 105587. [Google Scholar] [CrossRef]
- Shan, J.-t.; Wu, Y.-m.; Yang, X.-l. Three-dimensional stability of two-step slope with crack considering temperature effect on unsaturated soil. Journal of Central South University 2025, 32, 1060–1079. [Google Scholar] [CrossRef]
- Yuan, J.F.; Li, L.Z.; Wang, E.D.; Skibniewski, M.J. Examining sustainability indicators of space management in elderly Facilities-a case study in China. J. Clean. Prod. 2019, 208, 144–159. [Google Scholar] [CrossRef]
- Grabowski, D.C.; Mor, V. Nursing Home Care in Crisis in the Wake of COVID-19. Jama-J. Am. Med. Assoc. 2020, 324, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-B.; Hwan-Yong, P. A Study on the Overcrowding Distribution and Location Influence Factors of Elderly Care Facilities in Seoul Metropolitan Area. J. Korean Urban Manag. Assoc. 2019, 32, 21–43. [Google Scholar] [CrossRef]
- Li, X.; Krumholz, H.M.; Yip, W.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.Y.; Mossialos, E.; Li, C.; Lu, J.P.; Su, M.; et al. Quality of primary health care in China: Challenges and recommendations. Lancet 2020, 395, 1802–1812. [Google Scholar] [CrossRef]
- Li, M.Y.; Peng, P.Y.; Zhu, H.; Ao, Y.B.; Zhou, Z.L. Exploring the equitable spatial planning on the accessibility of institutional elderly care in megacity: A study based on Chengdu, China. Sustain. Cities Soc. 2024, 117, 105998. [Google Scholar] [CrossRef]
- Waterworth, S.; Raphael, D.; Gott, M.; Arroll, B.; Benipal, J.; Jarden, A. An exploration of how community-dwelling older adults enhance their well-being. Int. J. Older People Nurs. 2019, 14, e12267. [Google Scholar] [CrossRef]
- Ahaddour, C.; van den Branden, S.; Broeckaert, B. Institutional Elderly Care Services and Moroccan and Turkish Migrants in Belgium: A Literature Review. J. Immigr. Minor. Health 2016, 18, 1216–1227. [Google Scholar] [CrossRef]
- Kalicki, A.V.; Moody, K.A.; Franzosa, E.; Gliatto, P.M.; Ornstein, K.A. Barriers to telehealth access among homebound older adults. J. Am. Geriatr. Soc. 2021, 69, 2404–2411. [Google Scholar] [CrossRef]
- Wen, C.; Albert, C.; von Haaren, C. Nature-based recreation for the elderly in urban areas: Assessing opportunities and demand as planning support. Ecol. Process. 2022, 11, 44. [Google Scholar] [CrossRef]
- Feng, S.; Chen, L.D.; Sun, R.H.; Feng, Z.Q.; Li, J.R.; Khan, M.S.; Jing, Y.C. The Distribution and Accessibility of Urban Parks in Beijing, China: Implications of Social Equity. Int. J. Environ. Res. Public Health 2019, 16, 4894. [Google Scholar] [CrossRef]
- Guida, C.; Carpentieri, G. Quality of life in the urban environment and primary health services for the elderly during the Covid-19 pandemic: An application to the city of Milan (Italy). Cities 2021, 110, 103038. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Kwan, M.P.; Wang, J.Y. Developing the 15-Minute City: A comprehensive assessment of the status in Hong Kong. Travel Behav. Soc. 2024, 34, 100666. [Google Scholar] [CrossRef]
- Guo, J.; Ling, W.H. The relationship between the mental health status and social support of the lonely elderly with government participation in the Internet context. Front. Public Health 2022, 10, 1013069. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F.; Chen, B.Y.; Yuan, H.; Wang, D.G.; Lam, W.H.K.; Li, Q.Q. Measuring temporal variation of location-based accessibility using space-time utility perspective. J. Transp. Geogr. 2018, 73, 13–24. [Google Scholar] [CrossRef]
- Liu, B.Y.; Chen, Y.; Xiao, M. The Social Utility and Health Benefits for Older Adults of Amenity Buildings in China’s Urban Parks: A Nanjing Case Study. Int. J. Environ. Res. Public Health 2020, 17, 7497. [Google Scholar] [CrossRef]
- Mao, S.; Lu, N.; Xiao, C.H. Perceived neighborhood environment and depressive symptoms among older adults living in Urban China: The mediator role of social capital. Health Soc. Care Community 2022, 30, E1977–E1990. [Google Scholar] [CrossRef]
- Li, C.; Wu, J.J.; Huang, Y. Spatial-Temporal Patterns and Coupling Characteristics of Rural Elderly Care Institutions in China: Sustainable Human Settlements Perspective. Sustainability 2023, 15, 3286. [Google Scholar] [CrossRef]
- Leigh, R.; Ogburn, W. Social Change. With Respect to Culture and Original Nature. J. Philos. 1923, 20, 526. [Google Scholar] [CrossRef]
- Cheng, T.; Liu, C.H.; Yang, H.W.; Wang, N.; Liu, Y.S. From service capacity to spatial equity: Exploring a multi-stage decision-making approach for optimizing elderly-care facility distribution in the city centre of Tianjin, China. Sustain. Cities Soc. 2022, 85, 104076. [Google Scholar] [CrossRef]
- Enssle, F.; Kabisch, N. Urban green spaces for the social interaction, health and well-being of older people-An integrated view of urban ecosystem services and socio-environmental justice. Environ. Sci. Policy 2020, 109, 36–44. [Google Scholar] [CrossRef]
- Cheng, L.; Yang, M.; De Vos, J.; Witlox, F. Examining geographical accessibility to multi-tier hospital care services for the elderly: A focus on spatial equity. J. Transp. Health 2020, 19, 100926. [Google Scholar] [CrossRef]
- Weng, M.; Ding, N.; Li, J.; Jin, X.F.; Xiao, H.; He, Z.M.; Su, S.L. The 15-minute walkable neighborhoods: Measurement, social inequalities and implications for building healthy communities in urban China. J. Transp. Health 2019, 13, 259–273. [Google Scholar] [CrossRef]
- Logan, T.M.; Hobbs, M.H.; Conrow, L.C.; Reid, N.L.; Young, R.A.; Anderson, M.J. The x-minute city: Measuring the 10, 15, 20-minute city and an evaluation of its use for sustainable urban design. Cities 2022, 131, 103924. [Google Scholar] [CrossRef]
- Dunning, R.J.; Dolega, L.; Nasuto, A.; Nurse, A.; Calafiore, A. Age and the 20-min city: Accounting for variation in mobility. Appl. Geogr. 2023, 156, 103005. [Google Scholar] [CrossRef]
- Willberg, E.; Fink, C.; Toivonen, T. The 15-minute city for all?-Measuring individual and temporal variations in walking accessibility. J. Transp. Geogr. 2023, 106, 103521. [Google Scholar] [CrossRef]
- Wu, W.; Divigalpitiya, P. Availability and Adequacy of Facilities in 15 Minute Community Life Circle Located in Old and New Communities. Smart Cities 2023, 6, 2176–2195. [Google Scholar] [CrossRef]
- Yang, Y.; Qian, Y.; Zeng, J.; Wei, X.; Yang, M. Walkability measurement of 15-minute community life circle in Shanghai. Land 2023, 12, 153. [Google Scholar] [CrossRef]
- Song, L.; Kong, X.S.; Cheng, P. Supply-demand matching assessment of the public service facilities in 15-minute community life circle based on residents’ behaviors. Cities 2024, 144, 104637. [Google Scholar] [CrossRef]
- Jin, M.J.; Deng, Q.T.; Wang, S.Y.; Wei, L.T. Equity Evaluation of Elderly-Care Institutions Based on Ga2SFCA: The Case Study of Jinan, China. Sustainability 2023, 15, 16943. [Google Scholar] [CrossRef]
- Xu, Z.; Shang, Z.Q.; Zhong, Y.F.; Han, L.Y.; Li, M.Y.; Yang, Y.H. Evaluating 15-minute walkable life circles for the senior: A case study of Jiande, China. J. Asian Archit. Build. Eng. 2024, 1–17. [Google Scholar] [CrossRef]
- Yang, Y.J.; Li, C.X.; Zhou, D. Study on the Characteristics of Community Elderly Care Service Facilities Usage and Optimization Design Based on Life Cycle Theory. Buildings 2024, 14, 3003. [Google Scholar] [CrossRef]
- Gaglione, F.; Cottrill, C.; Gargiulo, C. Urban services, pedestrian networks and behaviors to measure elderly accessibility. Transp. Res. Part D-Transp. Environ. 2021, 90, 102687. [Google Scholar] [CrossRef]
- Zhang, L.H.; Wang, L.; Wu, J.; Li, P.B.; Dong, J.L.; Wang, T.R. Decoding urban green spaces: Deep learning and google street view measure greening structures. Urban For. Urban Green. 2023, 87, 128028. [Google Scholar] [CrossRef]
- Hall, C.M.; Ram, Y. Walk score® and its potential contribution to the study of active transport and walkability: A critical and systematic review. Transp. Res. Part D-Transp. Environ. 2018, 61, 310–324. [Google Scholar] [CrossRef]
- Nagata, S.; Nakaya, T.; Hanibuchi, T.; Amagasa, S.; Kikuchi, H.; Inoue, S. Objective scoring of streetscape walkability related to leisure walking: Statistical modeling approach with semantic segmentation of Google Street View images. Health Place 2020, 66, 102428. [Google Scholar] [CrossRef]
- Koo, B.W.; Guhathakurt, S.; Botchwey, N. How are Neighborhood and Street-Level Walkability Factors Associated with Walking Behaviors? A Big Data Approach Using Street View Images. Environ. Behav. 2022, 54, 211–241. [Google Scholar] [CrossRef]
- Lee, J.; Kang, Y.; Kim, J.; Park, J. Analysis of Street View Image Object Affecting Perceived Walkability Using Machine Learning. J. Assoc. Korean Geogr. 2022, 11, 375–391. [Google Scholar] [CrossRef]
- Chen, Y.N.; Huang, X.R.; White, M. A study on street walkability for older adults with different mobility abilities combining street view image recognition and deep learning—The case of Chengxianjie Community in Nanjing (China). Comput. Environ. Urban Syst. 2024, 112, 102151. [Google Scholar] [CrossRef]
- He, X.; He, S.Y. Decoding the spatial effects of walkability on walking behavior among older adults by integrating big data and small data. Cities 2025, 156, 105537. [Google Scholar] [CrossRef]
- Marquet, O.; Hipp, J.A.; Miralles-Guasch, C. Neighborhood walkability and active ageing: A difference in differences assessment of active transportation over ten years. J. Transp. Health 2017, 7, 190–201. [Google Scholar] [CrossRef]
- Thielman, J.; Rosella, L.; Copes, R.; Lebenbaum, M.; Manson, H. Neighborhood walkability: Differential associations with self-reported transport walking and leisure-time physical activity in Canadian towns and cities of all sizes. Prev. Med. 2015, 77, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.O.; Moon, H.K.; Jeon, J.Y.; Sohn, C.M. Nutritional Management by Dietitian at Elderly Nursing Homes in Gyeonggi-do. J. Korean Diet. Assoc. 2013, 19, 400–415. [Google Scholar] [CrossRef]
- Cheng, M.; Cui, X. Spatial Optimization of Residential Care Facility Configuration Based on the Integration of Modified Immune Algorithm and GIS: A Case Study of Jing’an District in Shanghai, China. Int. J. Environ. Res. Public Health 2020, 17, 8090. [Google Scholar] [CrossRef] [PubMed]
- Balboa-Castillo, T.; Guallar-Castillón, P.; León-Muñoz, L.M.; Graciani, A.; López-García, E.; Rodríguez-Artalejo, F. Physical Activity and Mortality Related to Obesity and Functional Status in Older Adults in Spain. Am. J. Prev. Med. 2011, 40, 39–46. [Google Scholar] [CrossRef]
- Li, H.M.; Li, M.Y.; Peng, P.Y.; Long, Y.; Ao, Y.B.; Bahmani, H. Exploring non-linear effects of walking accessibility on well-being in rural older adults of Jintang County: A random forest analysis. Front. Public Health 2024, 12, 1333510. [Google Scholar] [CrossRef]
- Baldwin, R.; Chenoweth, L.; dela Rama, M.; Wang, A.Y. Does size matter in aged care facilities? A literature review of the relationship between the number of facility beds and quality. Health Care Manag. Rev. 2017, 42, 315–327. [Google Scholar] [CrossRef]
- Lin, L.J.; Zhang, L.; Geng, S.; Zhao, Y.L.; Tian, Y.Y. Research on Multi-Stage Post-Occupancy Evaluation Framework of Community Comprehensive Elderly Care Service Facilities under the Public-Private Partnership Mode-A Case Study of China. Buildings 2024, 14, 1343. [Google Scholar] [CrossRef]
- Li, Y.H.; Ran, Q.C.; Yao, S.; Ding, L.K. Evaluation and Optimization of the Layout of Community Public Service Facilities for the Elderly: A Case Study of Hangzhou. Land 2023, 12, 629. [Google Scholar] [CrossRef]
- Song, S.; Wang, D.; Zhu, W.; Wang, C. Study on the spatial configuration of nursing homes for the elderly people in Shanghai: Based on their choice preference. Technol. Forecast. Soc. Change 2020, 152, 119859. [Google Scholar] [CrossRef]
- Li, M.; Ao, Y.; Peng, P.; Bahmani, H.; Han, L.; Zhou, Z.; Li, Q. Resource allocation of rural institutional elderly care in China’s new era: Spatial-temporal differences and adaptation development. Public Health 2023, 223, 7–14. [Google Scholar] [CrossRef]
- Li, J.; Gao, X.; Qiu, Y.; Ling, Y.T. Aging-friendly cities: Investigating the effects of street usage on the psychological satisfaction of older adults in megacities. Front. Psychol. 2022, 13, 942301. [Google Scholar] [CrossRef] [PubMed]
- Changsha Municipal People’s Government (2024, October) The Changsha Home and Community Basic Elderly Care Service Improvement Action Project Has Achieved Its Expected Goals. Available online: http://www.changsha.gov.cn/zsszzzq2023/wxk/zsxw/202410/t20241021_11626786.html (accessed on 3 February 2025).
- Hunan Provincial Bureau of Statistics. (2016, September 9). Coordinated Development of Population Aging and Socio-Economy in Changsha. Hunan Statistical Information Network. Available online: https://tjj.hunan.gov.cn/tjfx/sxfx/zss_3489/201609/t20160909_3802221.html (accessed on 3 February 2025).
- McKenzie, G.; Janowicz, K.; Adams, B. A weighted multi-attribute method for matching user-generated Points of Interest. Cartogr. Geogr. Inf. Sci. 2014, 41, 125–137. [Google Scholar] [CrossRef]
- Chen, L.C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-Decoder with Atrous Separable Convolution for Semantic Image Segmentation. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018. [Google Scholar] [CrossRef]
- Cordts, M.; Omran, M.; Ramos, S.; Rehfeld, T.; Enzweiler, M.; Benenson, R.; Franke, U.; Roth, S.; Schiele, B. The cityscapes dataset for semantic urban scene understanding. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
- National Bureau of Statistics of China. Results of the 7th National Population Census. 2021. Available online: https://www.stats.gov.cn/sj/pcsj/rkpc/7rp/indexch.htm (accessed on 4 October 2024).
- Ministry of Civil Affairs of the People’s Republic of China. Planning Specification for Urban Elderly Facilities. 2017. Available online: https://www.mca.gov.cn/zt/history/18aqgly/20170500891239.html (accessed on 4 October 2024).
- Sun, X.X.; Cheng, Y.; Tao, Z.L. Spatial accessibility and equity of residential care facilities in Beijing from 2010 to 2020. Health Place 2024, 86, 103219. [Google Scholar] [CrossRef] [PubMed]
- Zuo, J.; Fan, J.H.; Huang, X.Y.; Li, C.; Luo, J.C. Classification and Spatial Differentiation of Subdistrict Units for Sustainable Urban Renewal in Megacities: A Case Study of Chengdu. Land 2024, 13, 164. [Google Scholar] [CrossRef]
- Feng, H.C.; Tang, X.X.; Zou, C. Optimizing the Layout of Service Facilities for Older People Based on POI Data and Machine Learning: Guangzhou City as an Example. Land 2024, 13, 700. [Google Scholar] [CrossRef]
- Busch, T.D.; Duarte, Y.A.; Nunes, D.P.; Lebrao, M.L.; Naslavsky, M.S.; Rodrigues, A.D.; Amaro, E. Factors associated with lower gait speed among the elderly living in a developing country: A cross-sectional population-based study. BMC Geriatr. 2015, 15, 35. [Google Scholar] [CrossRef]
- Gutiérrez-Misis, A.; Sánchez-Santos, M.T.; Banegas, J.R.; Castell, M.V.; González-Montalvo, J.I.; Otero, A. Walking speed and high blood pressure mortality risk in a spanish elderly population. J. Hum. Hypertens. 2015, 29, 566–572. [Google Scholar] [CrossRef]
- Nilsson, L. Network-Based Urban Growth-How Centrality and Accessibility to Places Shape Land Use. Ph.D. Dissertation, ProQuest Dissertations Publishing, Ann Arbor, MI, USA, 2022. [Google Scholar]
- Miller, E.J. Accessibility: Measurement and application in transportation planning. Transp. Rev. 2018, 38, 551–555. [Google Scholar] [CrossRef]
- Yang, X.L.; Huang, F. Collapse mechanism of shallow tunnel based on nonlinear Hoek-Brown failure criterion. Tunn. Undergr. Space Technol. 2011, 26, 686–691. [Google Scholar] [CrossRef]
- Kelobonye, K.; Zhou, H.; McCarney, G.; Xia, J.H. Measuring the accessibility and spatial equity of urban services under competition using the cumulative opportunities measure. J. Transp. Geogr. 2020, 85, 102706. [Google Scholar] [CrossRef]
- Singh, S.S.; Sarkar, B. Cumulative opportunity-based accessibility measurement framework in rural India. Transp. Policy 2022, 117, 138–151. [Google Scholar] [CrossRef]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically weighted regression: The analysis of spatially varying relationships. Am. J. Agric. Econ. 2004, 86, 554–556. [Google Scholar] [CrossRef]
- Elldér, E. Built environment and the evolution of the " 15-minute city: A 25-year longitudinal study of 200 Swedish cities. Cities 2024, 149, 104942. [Google Scholar] [CrossRef]
- Xing, L.J.; Chen, Q.; Liu, Y.L.; He, H.G. Evaluating the accessibility and equity of urban health resources based on multi-source big data in high-density city. Sustain. Cities Soc. 2024, 100, 105049. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Source | Url |
|---|---|---|
| The Seventh National Population Census [17,22] | National Bureau of Statistics | https://www.stats.gov.cn/ (accessed on 4 October 2024) |
| Point of interest [11,65] | Baidu Maps | https://lbsyun.baidu.com/index.php?component=index&docid=22 (accessed on 2 October 2024) |
| Street view [11] | Baidu Maps | https://map.baidu.com/ (accessed on 22 November 2024) |
| Road network data [17] | Openstreetmap | https://www.openstreetmap.org/relation/3202711 (accessed on 2 October 2024) |
| First Level Indicators | Second Level Indicators | Example |
|---|---|---|
| Catering [11,73] | Chinese Restaurant [11] | Hengdong Tu Cai Restaurant, Northeast iron pot stew |
| Dessert and beverage [11] | Modern China Tea Shop, Tea Space, Tang Dynasty Palace Peach Crispy | |
| Fast restaurant [73] | KFC, RICE MR | |
| Bakery [73] | Rosa Cake | |
| Shopping [11,17,56,73] | Supermarket [73] | Wal-mart, Le’erle Discount Wholesale Supermarket |
| Shopping mall [11] | Changsha IFS, Wanda Plaza | |
| Convenience store [17] | Lawson,7-ELEVEn | |
| Integrated market [56] | Fruit Store, Food market | |
| Bird and flower market [73] | Pet shop, Flower shop | |
| Settlement [72] | Resident [73] | Jinyuan Community |
| Transportation [17,61] | Bus station [17] | Xihu Bridge Bus Station |
| Subway station [61] | Orange Island Subway Station | |
| Medical care [11,17,19,61] | General hospital [17] | Hunan Provincial People’s Hospital |
| Specialized hospital [19] | Carnation Geriatric Hospital | |
| Clinic [19] | Wangping Clinic | |
| Pharmacy [11] | People’s Pharmacy | |
| Leisure [11,21,22] | Park and square [21,22] | Meixi Lake Park, Jiangwan Cultural Square |
| Landscape [11] | Orange County | |
| Finance [17,73] | Bank [17] | the People’s Bank of China, postal savings bank |
| ATMs [17] | China Construction Bank 24-h self-service banking | |
| Insurance [73] | China Life Insurance Company | |
| Government [11,17,73] | Government [11] | Xifu Village Committee Tianxin District Government Service Center |
| Social organization [73] | Nursery Planting Professional Cooperative |
| Study Area | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| Urban area | 0.792 | 0.814 | 0.792 | 0.785 |
| Rural area | 0.793 | 0.797 | 0.793 | 0.791 |
| First Level Indicators | Second Level Indicators | First-Level Weight | Local Weight | Global Weight |
|---|---|---|---|---|
| Catering | Chinese Restaurant | 0.3273 | 0.49021 | 0.16046 |
| Dessert and beverage | 0.27263 | 0.08924 | ||
| Fast restaurant | 0.13724 | 0.04492 | ||
| Bakery | 0.09992 | 0.03271 | ||
| Shopping | Supermarket | 0.1539 | 0.25023 | 0.03852 |
| Shopping mall | 0.07064 | 0.01087 | ||
| Convenience store | 0.37732 | 0.05808 | ||
| Integrated market | 0.18385 | 0.02830 | ||
| Bird and flower market | 0.11796 | 0.01816 | ||
| Settlement | Resident | 0.0950 | 0.09495 | |
| Transportation | Bus station | 0.0234 | 0.87539 | 0.02049 |
| Subway station | 0.12461 | 0.00292 | ||
| Medical care | General hospital | 0.1790 | 0.21525 | 0.03854 |
| Specialized hospital | 0.09776 | 0.01750 | ||
| Clinic | 0.23671 | 0.04238 | ||
| Pharmacy | 0.45028 | 0.08062 | ||
| Leisure | Park and square | 0.0148 | 0.23619 | 0.00351 |
| Landscape | 0.76381 | 0.01133 | ||
| Finance | Bank | 0.0402 | 0.37171 | 0.01495 |
| ATMs | 0.40827 | 0.01642 | ||
| Insurance | 0.22002 | 0.00885 | ||
| Government | Government | 0.1663 | 0.85744 | 0.14259 |
| Social organization | 0.14256 | 0.02371 |
| First Level Indicators | Second Level Indicators | First-Level Weight | Local Weight | Global Weight |
|---|---|---|---|---|
| Catering | Chinese Restaurant | 0.2921 | 0.58565 | 0.17109 |
| Dessert and beverage | 0.33632 | 0.09825 | ||
| Fast restaurant | 0.06644 | 0.01941 | ||
| Bakery | 0.01159 | 0.00339 | ||
| Shopping | Supermarket | 0.1877 | 0.12869 | 0.02416 |
| Shopping mall | 0.00025 | 0.00005 | ||
| Convenience store | 0.68406 | 0.12842 | ||
| Integrated market | 0.17449 | 0.03276 | ||
| Bird and flower market | 0.01251 | 0.00235 | ||
| Settlement | Resident | 0.01332 | 0.01332 | |
| Transportation | Bus station | 0.0436 | 0.96038 | 0.04183 |
| Subway station | 0.03962 | 0.00173 | ||
| Medical care | General hospital | 0.1575 | 0.16530 | 0.02604 |
| Specialized hospital | 0.02918 | 0.00460 | ||
| Clinic | 0.36262 | 0.05713 | ||
| Pharmacy | 0.44290 | 0.06978 | ||
| Leisure | Park and square | 0.0028 | 0.23619 | 0.00187 |
| Landscape | 0.76381 | 0.00095 | ||
| Finance | Bank | 0.0174 | 0.76686 | 0.01335 |
| ATMs | 0.14601 | 0.00254 | ||
| Insurance | 0.08712 | 0.00152 | ||
| Government | Government organs | 0.2855 | 0.75423 | 0.21532 |
| Social organization | 0.24577 | 0.07016 |
| Variables | Definition | Mean | Standard Deviation |
|---|---|---|---|
| Dependent variables | |||
| 5 min life circle | Walkability score of 5-min Elderly care facilities life circle for older people | 4.8555 | 4.3594 |
| 10 min life circle | Walkability score of 10-min Elderly care facilities life circle for older people | 7.6802 | 9.8110 |
| 15 min life circle | Walkability score of 15-min Elderly care facilities life circle for older people | 21.7341 | 15.4122 |
| Street level environmental variables | |||
| Road | The average proportion of road pixels to total pixels | 0.0674 | 0.0852 |
| Sidewalk | The average proportion of sidewalk pixels to total pixels | 0.0195 | 0.0259 |
| Building | The average proportion of building pixels to total pixels | 0.1041 | 0.1359 |
| Wall | The average proportion of wall pixels to total pixels | 0.0152 | 0.0270 |
| Fence | The average proportion of fence pixels to total pixels | 0.0192 | 0.0278 |
| Vegetation | The average proportion of vegetation pixels to total pixels | 0.1039 | 0.1305 |
| Terrain | The average proportion of terrain pixels to total pixels | 0.0305 | 0.0436 |
| Sky | The average proportion of sky pixels to total pixels | 0.0981 | 0.1177 |
| Person | The average proportion of person pixels to total pixels | 0.0019 | 0.0039 |
| Traffic vehicle | The average proportion of traffic vehicle pixels to total pixels | 0.0450 | 0.0707 |
| Street population variable | |||
| Elderly population | Population aged 65 and above | 6499.24 | 3029.149714 |
| 5-min | 10-min | 15-min | ||||
|---|---|---|---|---|---|---|
| Downtown | Township Areas | Downtown | Township Areas | Downtown | Township Areas | |
| Catering | 98.87% | 54.57% | 98.58% | 67.87% | 99.43% | 75.35% |
| Shopping | 89.80% | 52.08% | 96.32% | 67.04% | 97.45% | 74.24% |
| Settlement | 86.69% | 19.67% | 90.65% | 24.93% | 92.07% | 32.96% |
| Transportation | 70.26% | 27.98% | 81.87% | 47.09% | 88.95% | 55.96% |
| Medical care | 90.37% | 43.49% | 90.94% | 55.68% | 92.92% | 59.83% |
| Leisure | 31.45% | 6.37% | 46.46% | 11.36% | 57.22% | 17.73% |
| Finance | 50.71% | 18.56% | 65.44% | 26.87% | 74.50% | 36.84% |
| Government | 86.97% | 47.92% | 85.27% | 59.83% | 86.97% | 68.70% |
| Variables | 5 min Life Circle | 10 min Life Circle | 15 min Life Circle | VIF | |||
|---|---|---|---|---|---|---|---|
| Coef | p-Value | Coef | p-Value | Coef | p-Value | ||
| Intercept | 1.421 | 0.059 | 5.844 | 0.010 | 2.153 | 0.635 | |
| Street-level environmental variables | |||||||
| Road | 8.520 | 0.057 | 28.054 | 0.013 | 80.459 | 0.000 | 4.08 |
| Sidewalk | −1.569 | 0.924 | −29.486 | 0.533 | −124.315 | 0.149 | 1.60 |
| Building | 7.013 | 0.010 | 16.919 | 0.030 | 38.015 | 0.006 | 2.88 |
| Wall | −5.543 | 0.782 | −65.146 | 0.246 | −88.008 | 0.294 | 1.23 |
| Fence | 8.431 | 0.566 | 34.152 | 0.447 | 29.576 | 0.735 | 1.46 |
| Traffic | 18.315 | 0.898 | −386.299 | 0.393 | −336.588 | 0.683 | 1.70 |
| Vegetation | −4.457 | 0.148 | −5.606 | 0.436 | −15.466 | 0.224 | 1.72 |
| Terrain | −3.649 | 0.780 | −57.577 | 0.059 | −14.362 | 0.757 | 1.68 |
| Sky | −9.905 | 0.030 | −29.630 | 0.006 | −77.853 | 0.000 | 3.89 |
| Person | 151.564 | 0.107 | 517.689 | 0.081 | 1458.779 | 0.018 | 1.98 |
| Vehicle | 17.359 | 0.010 | 60.398 | 0.001 | 117.292 | 0.000 | 1.90 |
| Street population variables | |||||||
| Elderly population | 0.000 | 0.063 | 0.000 | 1.000 | 0.000 | 0.890 | 1.18 |
| R2 | 0.241 | 0.320 | 0.449 | ||||
| Adjusted R2 | 0.214 | 0.296 | 0.429 | ||||
| AICc/AIC | 1972.266 | 2505.905 | 2750.737 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Y.; Dong, T. Deep Learning-Driven Geospatial Modeling of Elderly Care Accessibility: Disparities Across the Urban-Rural Continuum in Central China. Appl. Sci. 2025, 15, 4601. https://doi.org/10.3390/app15094601
Yu Y, Dong T. Deep Learning-Driven Geospatial Modeling of Elderly Care Accessibility: Disparities Across the Urban-Rural Continuum in Central China. Applied Sciences. 2025; 15(9):4601. https://doi.org/10.3390/app15094601
Chicago/Turabian StyleYu, Yi, and Tian Dong. 2025. "Deep Learning-Driven Geospatial Modeling of Elderly Care Accessibility: Disparities Across the Urban-Rural Continuum in Central China" Applied Sciences 15, no. 9: 4601. https://doi.org/10.3390/app15094601
APA StyleYu, Y., & Dong, T. (2025). Deep Learning-Driven Geospatial Modeling of Elderly Care Accessibility: Disparities Across the Urban-Rural Continuum in Central China. Applied Sciences, 15(9), 4601. https://doi.org/10.3390/app15094601