Abstract
Immunizations during pregnancy are an important aspect of perinatal care. Although the influenza vaccine during pregnancy is safe, vaccination rates are low. According to research data, one of the reasons for the low vaccination rates among pregnant women is that they do not receive a clear recommendation from healthcare providers. This study aims to record the knowledge and attitudes about influenza vaccination and investigate healthcare professionals’ recommendations during the perinatal period. A cross-sectional study was conducted with convenience sampling in Athens, Greece. Our purposive sample included 240 midwives, Ob/Gs, and pediatricians. Data were collected using an appropriate standardized questionnaire with information about demographics, attitudes towards influenza vaccination, and knowledge about the influenza virus and peripartum vaccination. Statistical analysis was conducted using IBM SPSS-Statistics version 26.0. This study identifies the reasons for the lack of vaccine uptake including a wide range of misconceptions or lack of knowledge about influenza infection, lack of convenient access to get vaccinated, etc. Misconceptions about influenza and influenza vaccines could be improved by better education of healthcare workers. Continuing professional education for health professionals is necessary to improve the level of knowledge, prevent negative beliefs, and promote preventive and therapeutic practices.
1. Introduction
In December 2019, a new disease known as coronavirus disease 2019 (COVID-19) emerged as a major world threat. The pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has exposed vulnerable populations to an unprecedented global health crisis. Initially, the ability of SARS-CoV-2 to spread in the population was considered to be similar to that of the influenza virus [1]. Of note, the influenza A virus (novel H1N1 subtype) was first identified in April 2009 with the WHO raising the influenza pandemic alert to its highest level in June 2009. Since then, seasonal influenza continues to be a major worldwide health hazard [2].
Seasonal influenza is an acute respiratory illness caused by a group of RNA viruses (A, B, and C) [3]. The most common symptoms are those of the upper respiratory tract, such as cough, sore throat, and runny nose, which are also associated with general symptoms such as fever, headaches, myalgia, and weakness. Influenza can also cause severe complications including viral pneumonia and death, which occurs most frequently in certain groups of patients with underlying chronic illnesses classified as high-risk [4]. The CDC and the World Health Organization have added pregnant women to the high-risk groups for severe influenza illness [5].
Influenza during the perinatal period may therefore be associated with adverse maternal and prenatal outcomes due to the physiological changes and immune adaptations that occur during pregnancy [6]. A systematic review and meta-analysis of observational studies showed that there was a higher risk for hospitalization in pregnant versus non-pregnant women infected with influenza [7]. Interestingly, the risk of hospitalization was higher in the third trimester of pregnancy [8]. Ethnic minority background, obesity, diabetes mellitus or chronic cardiac or pulmonary disease, advanced maternal age (≥35 years), living in increased socioeconomic deprivation and working in healthcare or other public-facing occupations are important risk factors for more severe illness and pregnancy complications [9,10].
In addition to the adverse maternal outcomes, many studies have shown that influenza may also lead to neonatal complications such as preterm delivery, low birth weight, and occasionally neonatal death [11]. In a recent Korean study, children born to women with influenza were at an increased risk of preterm birth and low birth weight irrespective of gestational age [11]. Some studies observed an association between maternal fever and other congenital anomalies (e.g., congenital heart defects and orofacial clefts) [12,13]. The best protection against influenza during pregnancy is vaccination. Immunization during pregnancy is a significant aspect of perinatal care. Influenza vaccination is vital in every influenza season to help reduce the impact of respiratory illness on the community, and the overburdened healthcare system, as the battle against the COVID-19 pandemic continues. The WHO has emphasized that pregnant women are the highest priority group for influenza vaccination and has thus recommended their vaccination. The CDC Advisory Committee on Immunization Practices recommends that all women who are or might be pregnant, or are in their postpartum period, during the influenza season should receive any licensed, age-appropriate, recommended inactivated influenza vaccine or the recombinant quadrivalent influenza vaccine, regardless of trimester [14].
Several studies conducted by the CDC and its partners support the safety of the flu vaccine for pregnant people and their babies. Some retrospective studies evaluating maternal safety found no correlation between influenza vaccines and maternal adverse events. More recently, three systematic studies published by the WHO did not detect an increased risk of miscarriage, fetal death, mortality, preterm birth, or congenital anomalies among pregnant women who received the flu vaccine [15,16,17]. Maternal vaccination can also protect a newborn from influenza after birth (due to maternal antibodies that pass to the developing fetus through the placenta during gestation). Breastfeeding women can also get a shot to protect themselves from the flu. Vaccination reduces parents’ risk of getting sick and passing the flu on to their babies, thus shielding their offspring from infection. This is particularly significant for children younger than 6 months old since they are too young to receive a flu vaccine themselves [18].
Despite the recommendations for vaccination against influenza during pregnancy, vaccination rates remain low due to concerns about the safety of the vaccine and fear of genetic abnormalities [19]. Unbiased maternal care providers (MCPs), obstetrician–gynecologists, and midwives should be distinctively located to increase maternal vaccination acceptance. According to studies, one of the reasons for the low vaccination rates among pregnant women is that they do not receive a clear recommendation from maternity care providers [20]. Other comparable studies have also noted that health professionals were more likely to recommend vaccination in pregnancy if they would personally have received the influenza vaccines of their own free will and/or if they as healthcare workers had the influenza vaccine shots [21,22,23].
Most countries strongly recommend that healthcare workers be vaccinated seasonally against influenza to protect themselves and their patients. Ongoing assessment of influenza vaccine effectiveness is critical to inform public health policy. Public health messaging should highlight the overall benefit of influenza vaccines so as to avoid an unprecedented disruption in healthcare systems around the globe.
As the Coronavirus Disease 2019 (COVID-19) pandemic still causes life-threatening conditions, and the 2022–2023 influenza season epidemic comes to an early start in the European region, this study aims to record the knowledge and attitudes about influenza vaccination and explore healthcare professionals’ recommendations during the perinatal period.
2. Materials and Methods
A cross-sectional survey was conducted from November 2020 to January 2021. A total of 240 health professionals attended the study from different scientific fields, e.g., midwives, obstetricians–gynecologists, and pediatricians, practicing in two of the largest public maternity hospitals in Athens, Greece.
Self-administered questionnaires were originally distributed either online or in a paper-and-pen format in person or through the mail. The study was initially designed with the questionnaires distributed in paper-and-pen format. The rapid increase in the COVID-19 pandemic crisis in Greece, with repeated lockdowns following research approval in September 2020, and the extremely limited number (only twenty) of hard copies collected so far, forced the authors to turn to scientific associations in order to amass participants through informative emails. Thus, the questionnaire was distributed by word-of-mouth to professionals working in the reference hospitals but also by sharing the research with the respective associations of each scientific field (the Hellenic Midwives’ Association and The Medical Association of Athens). The scientific associations informed their members via email of this research and shared the study questionnaire’s link with them. Consequently, two hundred and twenty questionnaires were administered exclusively online.
All questions were standardized so that all respondents received the same questions with identical wording. The COVID-19 pandemic has proven relentlessly challenging for healthcare workers and has strained the healthcare system in Greece in unprecedented ways. Limitations in staffing, high workload, heightened levels of somatic symptoms, and burnout led the researchers of this study to send the questionnaires by mail. This method was considered preferable due to time efficiency; further, respondents would not feel pressured and could answer when they had time, giving more accurate answers.
The questionnaire was divided into three sections and was administered online and distributed via email. Section 1 included items on socio-demographics (age, gender) and practice characteristics (occupation/specialty, section of work, educational level). Section 2 included items on knowledge about the flu and modes of transmission (what is influenza, how it is caused, etc.). Section 3 included knowledge of the influenza vaccine (recommendations and guidelines about vaccination). The response rate was 80%. The questionnaires were sent to three hundred health professionals and, ultimately, two hundred and forty were returned fully completed.
Participation in the survey was voluntary. A short paragraph was included at the beginning of the questionnaire to inform participants of the study’s objectives and their responses’ confidentiality. All participants gave informed consent. Data were collected anonymously and participants had the right to access their answers and withdraw from the research whenever they wished to. The study protocol was approved by the Research Ethics Boards of participating institutions (Clinical Research and Ethics Committee of ELENA VENIZELOU & ALEXANDRA Hospital, T59-Μ10/16-09-2020). The authors declare that the study procedures were followed according to the regulations established by the Clinical Research and Ethics Committee and the Helsinki Declaration of the World Medical Association.
Continuous variables are presented as mean (standard deviation). The normal distribution of variables was assessed using the Kolmogorov–Smirnov test due to the study’s sample size (˃70). The Kolmogorov–Smirnov test is a nonparametric goodness-of-fit test and is used to determine whether two distributions differ, or whether an underlying probability distribution differs from a hypothesized distribution.
All continuous variables were not normally distributed; therefore, their comparison was performed using an unpaired non-parametric two-tailed Mann–Whitney test on variables with two groups and the Kruskal–Wallis test on variables with three or more groups. Categorical variables were examined using Fisher’s exact or chi-square tests and are shown as absolute numbers (frequency percent); p-values under 0.05 were defined as significant. Statistical analysis was conducted using IBM SPSS-Statistics version 26.0 (IBM, Armonk, NY, USA).
3. Results
A total of 240 maternity care providers fully responded to the questionnaire. The mean age of the participants was 38.96 ± 9.56 years. As regards the occupation and specialty, 191 (79.6%) were midwives and 49 (20.4%) were medical doctors, of whom 27 (11.3%) were obstetricians–gynecologists and 22 (9.2%) were pediatricians. More than half (54.2%) of our population was working in public hospitals, 80 (33.3%) were working in private clinics and 30 (12.5) had their own private practices.
Regarding the educational level, 138 (57.5%) of the participants had bachelor’s degrees, 91 (37.9%) had master’s degrees, and 11 (4.6%) were Ph.D. holders. The mean amount of work experience was 11.45 ± 8.48 years (the characteristics of the study population are summarized in Table 1).

Table 1.
Demographics of the study population.
A total of 228 (95%) responders noted that the flu is a viral contagious infection affecting the respiratory system; 88 (36.7%) responders answered that it is caused by RNA viruses; and 63 (26.2%) replied that the types that cause the disease are A, B, and C. Most of the participants (221, 92.1%) mentioned that the flu is more serious than the common cold. Regarding the question “Which of the following is the official influenza crisis response plan?”, 17 (7.1%) respondents chose PERSEUS, 2 (0.8%) selected SOSTRATOS, 33 (13.8%) picked ARTEMIS, and 2 (0.8%) chose ATHENA. With reference to the questions about the transmission of the flu, the majority of participants gave the right answers (Data on the knowledge of health professionals about the flu and the ways of transmission is summarized in Table 2).
Table 2.
Healthcare professionals’ knowledge about the flu and methods of transmission and prevention.
Numerous healthcare providers in our study (117, 73.8%) stated that they are aware of the guidelines of the Hellenic National Public Health Organization regarding flu vaccination, and more than half (150, 62.5%) mentioned that they are up to date on the developments surrounding the flu vaccine. The vast majority of our sample (233, 97.1%) declared that they are aware that the Hellenic National Public Health Organization recommends influenza vaccination for healthcare professionals; nonetheless, a great number (109, 45.4%) had not been vaccinated against the seasonal flu during the 2020 to 2021 season. Regarding the population groups in which vaccination is required, the most frequent answer was pregnant women (187 participants, 77.9%). Remarkably, 137 (57.1%) of our participants answered that vaccination is recommended throughout pregnancy, and 103 participants (42.9%) replied that vaccination is suggested either in the 1st or the 2nd, or in the 3rd trimester of pregnancy, or they did not know the correct answer.
The protection of their family appeared as the strongest motive for getting the vaccine (189 responders, 79.1%), followed by intending to protect their pregnant patients (173 responders, 73.3%), and themselves (172 responders, 72%). Concerns about side effects prevent a high percentage (118 respondents, 49.2%) from getting the vaccine, followed by the statement that the vaccine is not readily available (106 respondents, 44.2%). Almost all of the study’s population recommend the flu shot during pregnancy (227 respondents, 94.6%).
Furthermore, most participants were certain that the SARS-CoV-2 pandemic will increase influenza virus vaccine recommendations and vaccination rates (204 responders, 85%). Finally, the most recommended strategies regarding the promotion of flu vaccination were better informing health professionals about the vaccine and its recommendations (212 participants, 88.3%), vaccine information campaigns in the general population (120 participants, 50%), and an automatic vaccination reminder system (151 participants, 62.9%) (Data on health professionals’ knowledge of the influenza vaccine is summarized in Table 3).
Table 3.
Health professionals’ knowledge of the influenza vaccine.
Association between Responders’ Characteristics and Knowledge about the Flu Vaccine
Most responders who mentioned that they were up to date on the developments surrounding the flu vaccine were obstetricians–gynecologists (p = 0.016); nevertheless, those who knew that the flu vaccine is recommended for the general population were midwives (p = 0.021) (Figure 1).
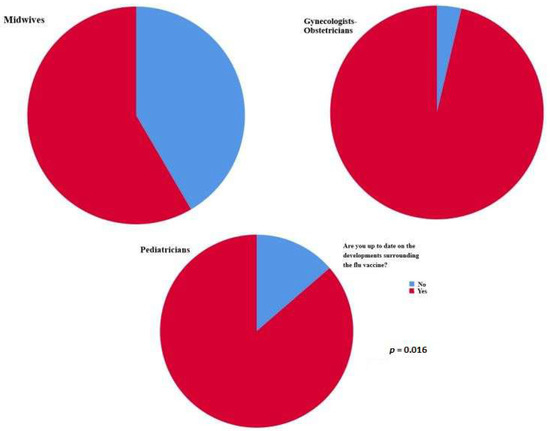
Figure 1.
Most responders who mentioned that they were up to date on the developments surrounding the flu vaccine were obstetricians–gynecologists (p = 0.016).
Pediatricians in our sample declared that vaccination is allowed for children older than six months (p = 0.01). Midwife participants answered that vaccination is recommended throughout the entire pregnancy (p = 0.02) (Figure 2).
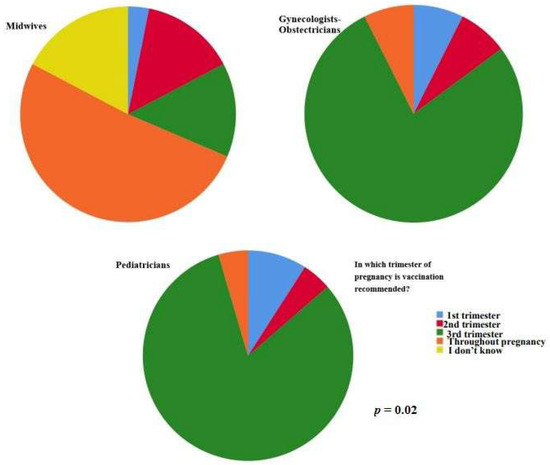
Figure 2.
Midwife participants answered that vaccination is recommended throughout the entire pregnancy (p = 0.02).
Table 4 summarizes the associations between occupation/specialty and knowledge about the flu vaccine.
Table 4.
Associations between occupation/specialty and knowledge about the flu vaccine.
Remarkably, the respondents who stated that the vaccination is recommended through the entire pregnancy and those who had gotten the flu vaccine during the 2020–2021 season had their own private settings (p = 0.03 and p = 0.39, respectively).
Regarding work experience, the participants who recommended the flu vaccine had greater work experience (11.73 ± 8.54 years vs. 6.71 ± 5.79 years, p = 0.026) (Figure 3).

Figure 3.
The participants who recommended the flu vaccine had greater work experience (11.73 ± 8.54 years vs. 6.71 ± 5.79 years, p = 0.026).
Table 5 summarizes the associations of the section of work and years of service with knowledge about the flu vaccine.
Table 5.
Associations of sections of work and years of service with knowledge about the flu vaccine.
Moreover, a statistically significant number of our study population mentioned that they were aware of the guidelines of the Hellenic National Public Health Organization regarding flu vaccination, they were up to date on the developments surrounding the flu vaccine, knew that the Hellenic National Public Health Organization recommends influenza vaccination for healthcare professionals and the ones that recommend the flu vaccine were attending a statistically higher number of conferences/seminars/workshops per year (p = 0.013, p = 0.01, p = 0.02, and p = 0.013, respectively). Table 6 summarizes the relationships between the number of conferences/seminars/workshops attended per year and flu vaccine knowledge.
Table 6.
Associations between the number of attended conferences/seminars/workshops per year and the knowledge about the flu vaccine.
Finally, of great interest is the finding that there was a statistically significant difference in the proportion of participants who were vaccinated against the flu among the participants who recommended the vaccine (57.7% vaccinated vs. 42.3% unvaccinated, p = 0.01) (Figure 4).
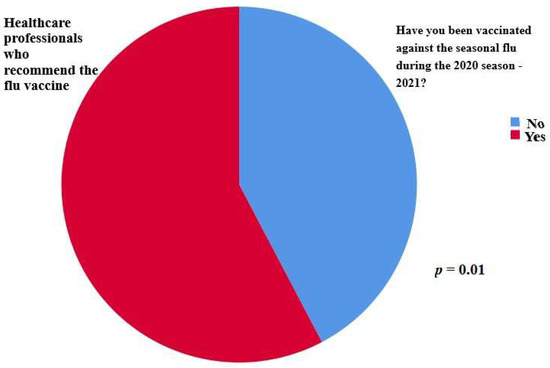
Figure 4.
A statistically significant difference was observed in the proportion of participants who were vaccinated against the flu among the participants who recommended the vaccine (57.7% vaccinated vs. 42.3% unvaccinated, p = 0.01).
Similarly, the participants who were aware of the guidelines of the Hellenic National Public Health Organization regarding flu vaccination and those who were up to date on the developments surrounding the flu vaccine remained more likely to be vaccinated against the seasonal flu during the 2020–2021 season (p = 0.002, and p = 0.011, respectively).
In addition, there was a statistically significant association between the number of healthcare professionals who recommended the vaccine and the number of healthcare professionals who had been informed about the flu vaccine (p = 0.01). Moreover, there was a statistically significant association between the number of healthcare professionals who recommended the vaccine and the number of healthcare professionals who were aware of the Hellenic National Public Health Organization guidelines regarding flu vaccination (p = 0.044). Table 7 summarizes the associations between information about the flu vaccine and vaccine recommendation/vaccination of healthcare professionals.
Table 7.
Associations between information about the flu vaccine and vaccine recommendation/vaccination of the healthcare professionals.
4. Discussion
Vaccination during pregnancy remains a national and international priority for maintaining perinatal health. Understanding healthcare providers’ knowledge about flu vaccination and attitudes toward vaccine acceptance is important in explaining current vaccination attainment levels among pregnant women. The purpose of this study was to identify reasons for the lack of vaccine uptake, which possibly includes a wide range of misconceptions or a lack of knowledge about influenza infection or the flu vaccine.
Due to the Hellenic National Public Health Organization in Greece, since 2015, there has been a gradual increase in staff vaccination coverage in both hospitals and Primary Health Care Centers [24]. In our sample, influenza vaccine coverage of healthcare providers was 54.6%, comparable to the percentage found by Vishram et al. in a UK study (58%) [25]. The majority of our sample (186, 77.5%) was unaware of the National Operational Plan to deal with an influenza pandemic, the so-called “ARTEMIS” plan. This was a thought-provoking finding because this plan is the same as the one for managing the COVID-19 pandemic in Greece.
While obstetricians–gynecologists in our research stated that they were up to date on the developments surrounding the flu vaccine, those who correctly replied that the vaccination is recommended throughout the entire pregnancy were the participant midwives. A similar cross-sectional study conducted among midwives practicing in Paris showed that they were aware that vaccination against influenza is recommended during pregnancy (190/208, 91%) and can be administered during any trimester (155/208, 82%). Equally, in our study, 57.1% of the participants knew that flu vaccination is recommended throughout pregnancy, and the majority of those who gave the correct answer were midwives.
The health professionals participating in this study who recommended the flu vaccine during pregnancy had many years of work experience in maternity care. Similarly, in a UK survey, the more experienced a maternity care provider, the more confident they were in advice-giving regarding influenza vaccination [25].
In our study, it was found that the majority of healthcare professionals who recommend the vaccine had been informed about the flu vaccine, and they were also aware of the guidelines of the Hellenic National Public Health Organization regarding flu vaccination. This was a similar finding to a study at a regional hospital in the northeast of the Republic of Ireland where a correlation between healthcare professionals’ awareness of guidelines and flu vaccine recommendations was proved [22]. A cross-sectional survey among French midwives practicing in public and private sectors also demonstrated that a higher level of knowledge and the existence of a vaccination protocol against influenza were associated with higher offer and prescription rates [21].
Our responders who recommend the flu vaccine attended a statistically higher number of conferences/seminars/workshops annually. Ongoing professional education is vital to update healthcare providers’ knowledge in crucial scientific areas of interest so as to improve their ability to serve their clients.
Despite the fact that most of our sample declared that they were aware of the Hellenic National Public Health Organization influenza vaccination recommendation for healthcare professionals (233, 97.1%), a great proportion (109, 45.4%) had not been vaccinated against the seasonal flu during the 2020–2021 season. Furthermore, it is worth mentioning that in our study, 73.8% of our participants were fully cognizant of the guidelines of the Hellenic National Public Health Organization regarding flu vaccination and 62.5% were up to date on the developments surrounding the flu vaccine. This finding was analogous to another study in which the majority (95%) of healthcare professionals were aware of the health service executive guidelines on immunization; nonetheless, more than 75% of them did not receive the influenza vaccinations themselves and had no plans to receive it [22].
Worries about side effects were most commonly cited as the reason for not being vaccinated (118, 49.2%). This fact possibly explains the low rate of vaccination among our participants. This was also found in another study in England where 43% of healthcare professionals answered that concerns about side effects or personal illness/allergy were the reasons for not accepting influenza vaccination [25]. In a cross-sectional survey among midwives in Paris, the most frequent reason for non-vaccination was “not being worried about catching influenza” (33%) [21]. Studies consistently advise that when recommendations for influenza vaccination during pregnancy originate directly from a woman’s obstetrician–gynecologist or midwife and if the vaccine is available in the health professional’s office, the odds of vaccine acceptance and receipt are 5-fold to 50-fold higher [26,27]. Thus, it is critically important that all maternity care providers recommend and advocate for the influenza vaccine.
As in former studies, the present study had its own limitations. First, this research had a cross-sectional design meaning the study was conducted in a specific time period. Therefore, the timing of the snapshot is not guaranteed to be representative and the study cannot be used to analyze behavior over a period of time.
Another limitation of our research is the relatively small sample size which may affect the generalizability of our results. This study was carried out amid the COVID-19 pandemic and consequently, numerous factors, such as irregular and long working hours, shift-working system, role ambiguity, role conflict, and cancellation of their annual leave, operated as deterrents for the more massive participation of health workers. However, those who eventually participated in the survey completed the entire questionnaire, with no missing data. This study was not very flexible as researchers were generally confined to a single instrument for collecting data. Depth was also a problem with this survey. Research questions were standardized; thus, it often seemed difficult to ask anything other than general questions that a broad range of health professionals would understand.
Likewise, another limitation is convenience sampling, which proved efficient and simple to implement under the pandemic circumstances; however, the sample lacks clear generalizability. The last limitation was the unbalanced number of maternity care professionals. The vast majority of participants in our research were midwives (191 (79.6%)). This may have caused the study results to be more influenced by midwives’ views and to reflect mainly their knowledge and attitudes. Studies, where the professional distribution is equal or close, are required in the future.
Although the findings should be interpreted with caution, this study has several strengths. The results contribute to our understanding of three different groups of maternity care professionals (obstetricians–gynecologists, pediatricians, and midwives) who have been found to experience difficulty in dealing with many issues during the COVID-19 pandemic. More specifically, our research is the only one that studied these three specialties compared to other studies during the COVID-19 pandemic. As there are limited data on influenza vaccination uptake and determinants of uptake in obstetric populations, our research embraces the gap of knowledge and attitudes of primary maternity care providers on that issue, as influenza during pregnancy can be potentially life-threatening.
Even though our survey was conducted during the COVID-19 pandemic, it is noteworthy that the attitudes and knowledge on influenza vaccination among healthcare professionals were similar to those found in other studies conducted before the COVID-19 pandemic.
Notwithstanding the relatively limited sample, this work offers valuable insights into how maternity care professionals that have been at the frontline in the fight against the COVID-19 crisis are actively involved in providing good quality maternity care while managing this crisis.
This study has provided a deeper insight into an increasing necessity for personal and professional interventions that can strengthen the personal empowerment of maternity health professionals concerning influenza vaccination. Evidence-based information will guarantee a well-informed health workforce, leading to quality maternity services. Information delivery methods about the benefits of vaccination during pregnancy should be improved to increase the likelihood that someone will act on it [28]. Future health promotion campaigns may use the information in this study to address the concerns in support of influenza vaccination so as to improve vaccination uptake, following the new influenza A virus outbreak globally.
5. Conclusions
This study outlined reasons for the lack of vaccine uptake among health professionals working in maternity care, which mostly included a wide range of misconceptions or lack of knowledge about influenza infection or convenient access to vaccinations. There was a statistically significant difference in the percentage of participants from different scientific areas who responded that vaccination is recommended throughout the entire pregnancy, with midwives exhibiting the highest percentage. Given that the central role of Ob/Gs and midwives in the context of primary maternity care is prevention with the intention of improving maternal health and promoting safe motherhood, misconceptions about influenza and influenza vaccines should be improved by better educating healthcare workers. Health professional associations should ease the process of delivering information on perinatal vaccination to the end user in a way that is most likely to be understood and most likely to be acted upon. Strategies such as vaccine information campaigns in the general population and better-informing health professionals about the vaccine and its recommendations would help in the promotion of flu vaccination, as the European Commission has already published a communication on preparing for the autumn and winter 2022–2023 to help countries prepare their response to an expected increase of COVID-19 and influenza.
Author Contributions
Conceptualization, C.T. and A.L.; data curation, C.T.; formal analysis, V.Ε.G., C.T. and A.S.; funding acquisition, A.S. and C.T.; investigation, C.T., A.S. and P.P.; methodology, A.L., C.T.; project administration, C.T.; supervision, A.L., A.B. and G.D.; validation, A.S.; writing—original draft, C.T. and A.S.; writing—review and editing, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
The APCs will be paid by the Special Account for Research Grants, University of West Attica, Athens, Greece.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by ELENA VENIZELOU & ALEXANDRA HOSPITAL Clinical Research and Ethics Committee, T59-Μ10/16-09-2020 (protocol code T59-M10—16 September 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available; however, they are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef] [PubMed]
- Girard, M.P.; Tam, J.S.; Assossou, O.M.; Kieny, M.P. The 2009A (H1N1) influenza virus pandemic: A review. Vaccine 2010, 28, 4895–4902. [Google Scholar] [CrossRef] [PubMed]
- Neumann, G.; Noda, T.; Kawaoka, Y. Emergence and pandemic potential of swine-origin H1N1 influenza virus. Nature 2009, 459, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Loeb, M.; Singh, P.K.; Fox, J.; Russell, M.L.; Pabbaraju, K.; Zarra, D.; Wong, S.; Neupane, B.; Webby, R.; Fonseca, K. Longitudinal study of influenza molecular viral shedding in Hutterite communities. J. Infect. Dis. 2012, 206, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.; Cutland, C.; Jones, S.; Hugo, A.; Madimabe, R.; Simões, E.A.F.; Weinberg, A.; Madhi, S.A. Duration of infant protection against influenza illness conferred by maternal immunization: Secondary Analysis of a Randomized Clinical Trial. JAMA Pediatr. 2016, 170, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Gaunt, G.; Ramin, K. Immunological tolerance of the human fetus. Am. J. Perinatol. 2001, 18, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Mertz, D.; Geraci, J.; Winkup, J.; Gessner, B.D.; Ortiz, J.R.; Loeb, M. Pregnancy as a risk factor for severe outcomes from influenza virus infection: A systematic review and meta-analysis of observational studies. Vaccine 2017, 35, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, D.J.; Honein, M.A.; Rasmussen, S.A.; Williams, J.L.; Swerdlow, D.L.; Biggerstaff, M.S.; Lindstrom, S.; Louie, J.K.; Christ, C.M.; Bohm, S.R.; et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet 2009, 374, 451–458. [Google Scholar] [CrossRef]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population-based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef]
- Mertz, D.; Kim, T.H.; Johnstone, J.; Lam, P.P.; Science, M.; Kuster, S.P.; Fadel, S.A.; Tran, D.; Fernandez, E.; Bhatnagar, N.; et al. Populations at risk for severe or complicated influenza illness: Systematic review and meta-analysis. BMJ 2013, 347, f5061. [Google Scholar] [CrossRef]
- Fell, D.; Savitz, D.; Kramer, M.; Gessner, B.; Katz, M.; Knight, M.; Luteijn, J.; Marshall, H.; Bhat, N.; Gravett, M.; et al. Maternal influenza and birth outcomes: Systematic review of comparative studies. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 48–59. [Google Scholar] [CrossRef]
- Song, J.Y.; Park, K.V.; Han, S.W.; Choi, M.J.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Oh, M.-J.; Cho, G.J. Paradoxical long-term impact of maternal influenza infection on neonates and infants. BMC Infect. Dis. 2020, 20, 502. [Google Scholar] [CrossRef]
- Moretti, M.E.; Bar-Oz, B.; Fried, S.K.G. Maternal hyperthermia and the risk for neural tube defects in offspring: Systematic review and meta-analysis. Epidemiology 2005, 16, 216–219. [Google Scholar] [CrossRef]
- Center of Disease Control and Prevention (CDC). Key Facts about Seasonal Flu Vaccine. 2020. Available online: https://www.cdc.gov/flu/prevent/keyfacts.htm (accessed on 16 December 2020).
- Fell, D.B.; Platt, R.; Lanes, A.; Wilson, K.; Kaufman, J.; Basso, O.; Buckeridge, D. Fetal death and preterm birth associated with maternal influenza vaccination: Systematic review. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 17–26. [Google Scholar] [CrossRef]
- Fell, D.B.; Sprague, A.E.; Liu, N.; Yasseen, A.S.; Wen, S.-W.; Smith, G.; Walker, M.C. H1N1 influenza vaccination during pregnancy and fetal and neonatal outcomes. Am. J. Public Health 2012, 102, e33–e40. [Google Scholar] [CrossRef]
- McMillan, M.; Porritt, K.; Kralik, D.; Costi, L.; Marshall, H. Influenza vaccination during pregnancy: A systematic review of fetal death, spontaneous abortion, and congenital malformation safety outcomes. Vaccine 2015, 33, 2108–2117. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Center for Immunization and Respiratory Diseases (NCIRD). Available online: https://www.cdc.gov/ncird/index.html (accessed on 30 October 2022).
- Yuen, C.Y.; Tarrant, M. A comprehensive review of influenza and influenza vaccination during pregnancy. J. Perinat. Neonatal Nurs. 2014, 28, 261–270. [Google Scholar] [CrossRef]
- Adeyanju, G.C.; Engel, E.; Koch, L.; Ranzinger, T.; Shahid, I.B.M.; Head, M.G.; Eitze, S.; Betsch, C. Determinants of influenza vaccine hesitancy among pregnant women in Europe: A systematic review. Eur. J. Med. Res. 2021, 26, 116. [Google Scholar] [CrossRef]
- Loubet, P.; Nguyen, C.; Burnet, E.; Launay, O. Influenza vaccination of pregnant women in Paris, France: Knowledge, attitudes and practices among midwives. PLoS ONE 2019, 14, e0215251. [Google Scholar] [CrossRef]
- Ugezu, C.; Essajee, M. Exploring patients’ awareness and healthcare professionals’ knowledge and attitude to pertussis and influenza vaccination during the antenatal periods in Cavan Monaghan general hospital. Hum. Vaccines Immunother. 2018, 14, 978–983. [Google Scholar] [CrossRef]
- Lu, A.B.; Halim, A.A.; Dendle, C.; Kotsanas, D.; Giles, M.L.; Wallace, E.M.; Buttery, J.P.; Stuart, R.L. Influenza vaccination uptake among pregnant women and maternal care providers is suboptimal. Vaccine 2012, 30, 4055–4059. [Google Scholar] [CrossRef] [PubMed]
- Influenza and Seasonal Influenza. Available online: https://eody.gov.gr/wp-content/uploads/2020/10/antigripikos-emvoliasmos-prosopikou-2020-2021-1.pdf (accessed on 20 March 2020).
- Vishram, B.; Letley, L.; Van Hoek, A.J.; Silverton, L.; Donovan, H.; Adams, C.; Green, D.; Edwards, A.; Yarwood, J.; Bedford, H.; et al. Vaccination in pregnancy: Attitudes of nurses, midwives and health visitors in England. Hum. Vaccines Immunother. 2018, 14, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, I.B.; Jamieson, D.J.; Rasmussen, S.A.; D’Angelo, D.; Goodman, D.; Kim, H. Correlates of seasonal influenza vaccine coverage among pregnant women in Georgia and Rhode Island. Obstet. Gynecol. 2010, 116, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Shavell, V.I.; Moniz, M.H.; Gonik, B.; Beigi, R.H. Influenza immunization in pregnancy: Overcoming patient and health care provider barriers. Am. J. Obstet. Gynecol. 2012, 207, S67–S74. [Google Scholar] [CrossRef]
- Sarantaki, A.; Kalogeropoulou, V.E.; Taskou, C.; Nanou, C.; Lykeridou, A. COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 2055. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).