
Pilot Study to Evaluate the Efficacy of Polynucleotide Sodium Compared to Sodium Hyaluronate and Crosslinked Sodium Hyaluronate in Patients with Knee Osteoarthritis

 , ,
, ,
Abstract
:1. Introduction
2. Methods and Materials
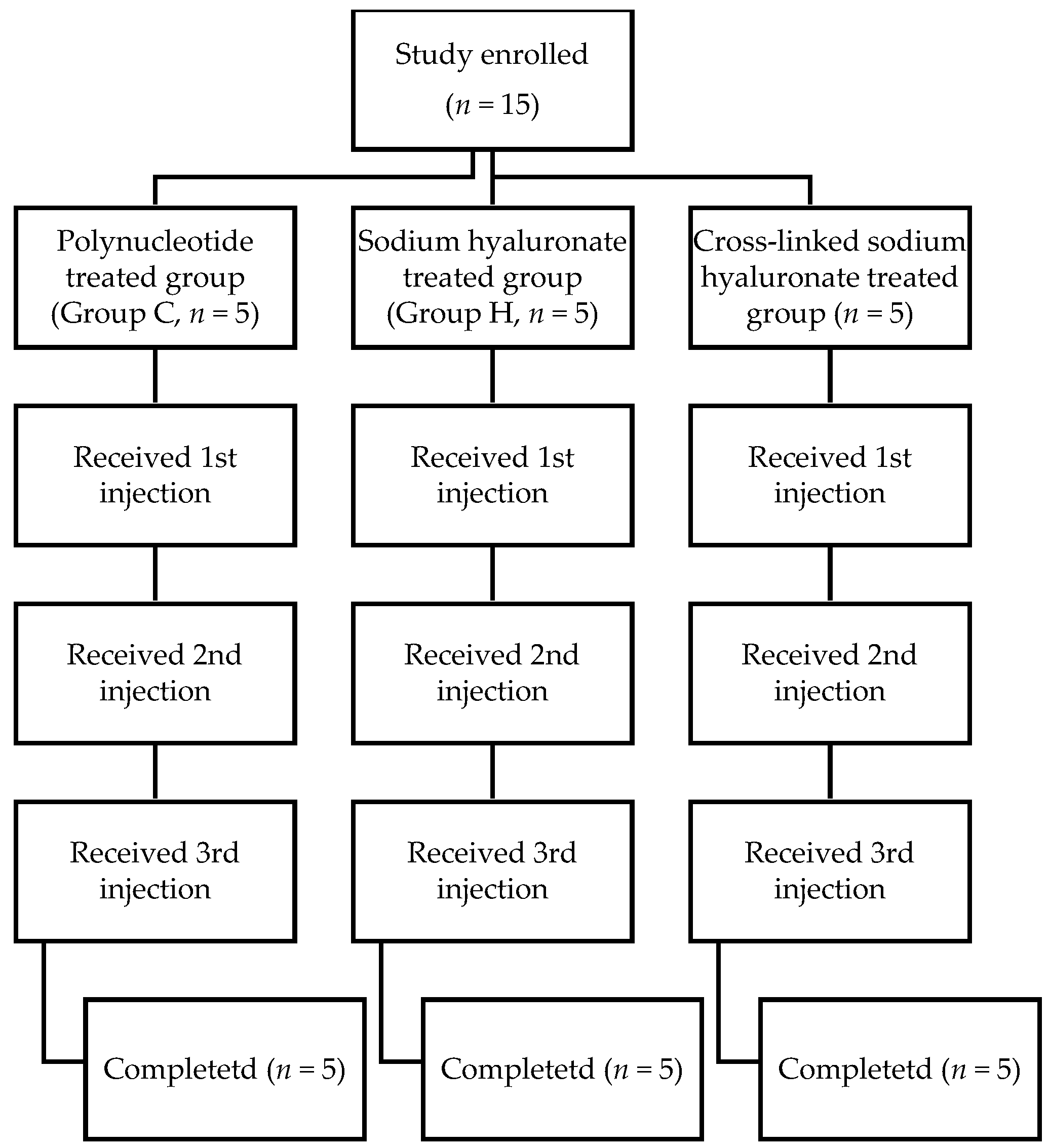
2.1. Study Design
2.2. Materials
2.3. Study Population
2.4. Experimental Intervention
2.5. Outcome Measurements
2.6. Statistical Analysis
3. Results
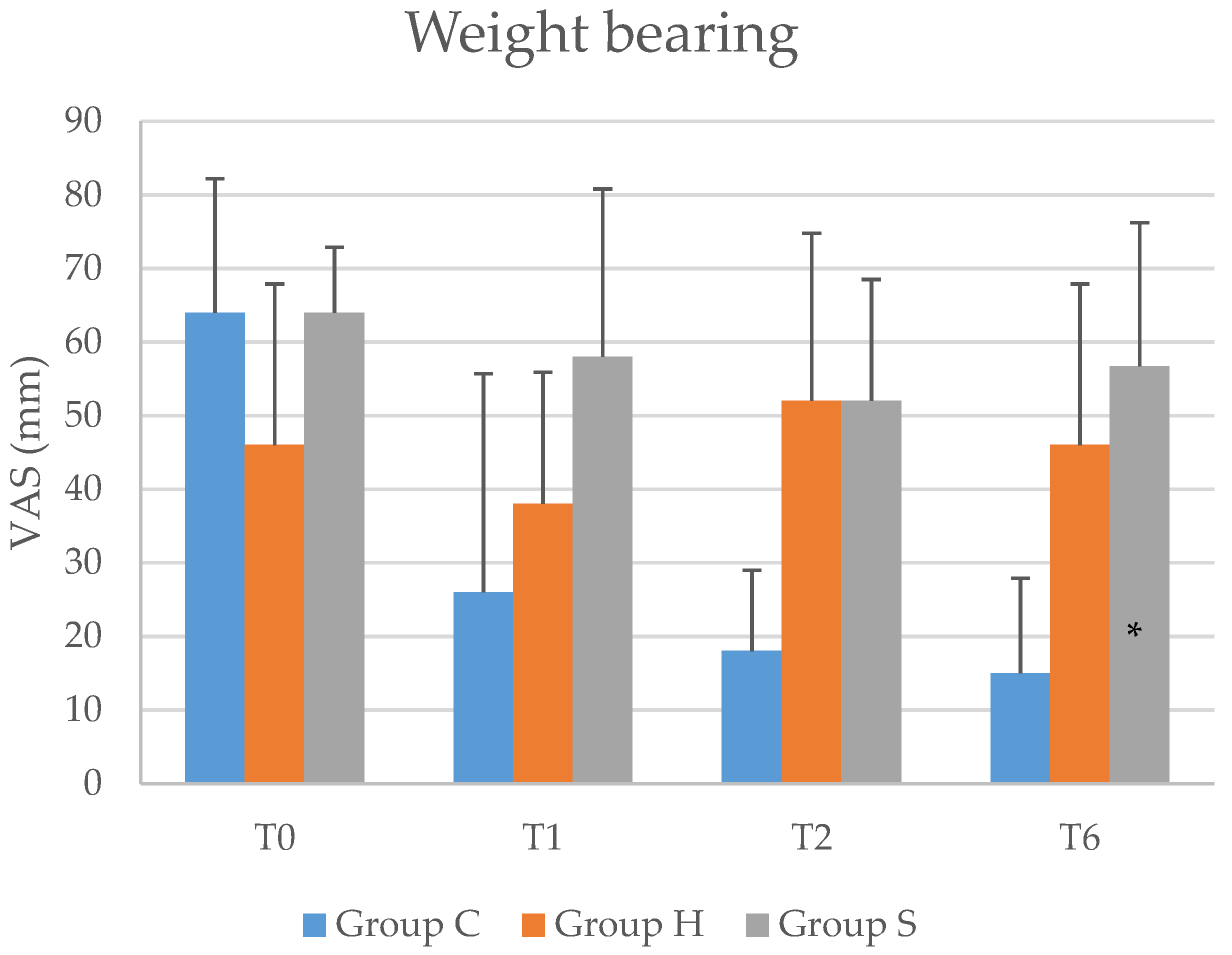
3.1. Primary Results
3.2. Secondary Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lo, G.H.; LaValley, M.; McAlindon, T.; Felson, D.T. Intra-articular hyaluronic acid in treatment of knee osteoarthritis: A meta-analysis. JAMA 2003, 290, 3115–3121. [Google Scholar] [CrossRef]
- Payne, M.W.; Petrella, R.J. Viscosupplementation effect on proprioception in the osteoarthritic knee. Arch. Phys. Med. Rehabil. 2000, 81, 598–603. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Choi, E.; Nahm, F.S.; Han, W.K.; Lee, P.-B.; Jo, J. Topical agents: A thoughtful choice for multimodal analgesia. Korean J. Anesthesiol. 2020, 73, 384–393. [Google Scholar] [CrossRef]
- Zazgyva, A.; Gergely, I.; Russu, O.M.; Roman, C.; Pop, T.S. Polynucleotides versus sodium hyaluronate in the local treatment of knee osteoarthritis. Acta Med. Transilv. 2013, 2, 260–263. [Google Scholar]
- Noh, S.-S.; Lee, J.-J.; Hwang, S.-M.; Lim, S.-Y.; Chung, I.-Y.; Choi, Y.-R. Efficacy of intra-articular sodium hyaluronate in patients with osteoarthritis of the knee. Korean J. Pain 2004, 17, 170–174. [Google Scholar] [CrossRef]
- Ha, C.-W.; Park, Y.-B.; Choi, C.-H.; Kyung, H.-S.; Lee, J.-H.; Yoo, J.D.; Yoo, J.-H.; Choi, C.-H.; Kim, C.-W.; Kim, H.-C. Efficacy and safety of single injection of cross-linked sodium hyaluronate vs. three injections of high molecular weight sodium hyaluronate for osteoarthritis of the knee: A double-blind, randomized, multi-center, non-inferiority study. BMC Musculoskelet. Disord. 2017, 18, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balazs, E.A.; Denlinger, J.L. Viscosupplementation: A new concept in the treatment of osteoarthritis. J. Rheumatol. Suppl. 1993, 39, 3–9. [Google Scholar] [PubMed]
- Mori, S.; Naito, M.; Moriyama, S. Highly viscous sodium hyaluronate and joint lubrication. Int. Orthop. 2002, 26, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Benke, M.; Shaffer, B. Viscosupplementation treatment of arthritis pain. Curr. Pain Headache Rep. 2009, 13, 440. [Google Scholar] [CrossRef]
- Curran, M.P. Hyaluronic Acid (Supartz®). Drugs Aging 2010, 27, 925–941. [Google Scholar] [CrossRef] [PubMed]
- Lester, D.K.; Zhang, K. Gait analysis of knee arthritis treated with hyaluronic acid. J. Arthroplast. 2010, 25, 1290–1294. [Google Scholar] [CrossRef]
- Rutjes, A.W.; Jüni, P.; da Costa, B.R.; Trelle, S.; Nüesch, E.; Reichenbach, S. Viscosupplementation for osteoarthritis of the knee: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Doherty, M. Efficacy paradox and proportional contextual effect (PCE). Clin. Immunol. 2018, 186, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-W.; Lue, K.-H.; Lee, H.-S.; Lin, R.-C.; Lu, K.-H. Hylan GF 20 has better pain relief and cost-effectiveness than sodium hyaluronate in treating early osteoarthritic knees in Taiwan. J. Formos. Med. Assoc. 2009, 108, 663–672. [Google Scholar] [CrossRef] [Green Version]
- Berenbaum, F.; Grifka, J.; Cazzaniga, S.; D’Amato, M.; Giacovelli, G.; Chevalier, X.; Rannou, F.; Rovati, L.C.; Maheu, E. A randomised, double-blind, controlled trial comparing two intra-articular hyaluronic acid preparations differing by their molecular weight in symptomatic knee osteoarthritis. Ann. Rheum. Dis. 2012, 71, 1454–1460. [Google Scholar] [CrossRef] [PubMed]
- Strand, V.; Baraf, H.S.; Lavin, P.; Lim, S.; Hosokawa, H. A multicenter, randomized controlled trial comparing a single intra-articular injection of Gel-200, a new cross-linked formulation of hyaluronic acid, to phosphate buffered saline for treatment of osteoarthritis of the knee. Osteoarthr. Cartil. 2012, 20, 350–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanelli, R.; Costa, P.; Rossi, S.M.P.; Benazzo, F. Efficacy of intra-articular polynucleotides in the treatment of knee osteoarthritis: A randomized, double-blind clinical trial. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 901–907. [Google Scholar] [CrossRef]
- Giarratana, L.S.; Marelli, B.M.; Crapanzano, C.; De Martinis, S.E.; Gala, L.; Ferraro, M.; Marelli, N.; Albisetti, W. A randomized double-blind clinical trial on the treatment of knee osteoarthritis: The efficacy of polynucleotides compared to standard hyaluronian viscosupplementation. Knee 2014, 21, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.; Lawrence, J. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkan, B.M.; Fidan, F.; Tosun, A.; Ardıçoğlu, Ö. Quality of life and self-reported disability in patients with knee osteoarthritis. Modern Rheumatol. 2014, 24, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.-C.; Lee, H.-S.; Yun, H.; Kim, T.-H.; Yoo, D.-H.; Kim, S. Cross-cultural adaptation and validation of Korean Western Ontario and McMaster Universities (WOMAC) and Lequesne osteoarthritis indices for clinical research. Osteoarthr. Cartil. 2001, 9, 746–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-H.; Ahn, J.; Ock, M.; Shin, S.; Park, J.; Luo, N.; Jo, M.-W. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 2016, 25, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.K.; Choi, J.H.; Jeong, J.; Kim, W.J.; Lee, D.J.; Lee, S.C.; Kim, Y.C.; Moon, J.Y. Korean version of the painDETECT questionnaire: A study for cultural adaptation and validation. Pain Pract. 2017, 17, 494–504. [Google Scholar] [CrossRef]
- Woessner, J.F.; Howell, D.S. Joint Cartilage Degradation: Basic and Clinical Aspects; Marcel Dekker: New York, NY, USA, 1993. [Google Scholar]
- De Aloe, G.; Rubegni, P.; Biagioli, M.; Taddeucci, P.; Fimiani, M. Skin graft donor site and use of polydeoxyribonucleotide as a treatment for skin regeneration: A randomized, controlled, double-blind, clinical trial. Wounds Compend. Clin. Res. Pract. 2004, 16, 258–263. [Google Scholar]
- Muratore, O.; Schito, A.P.; Cattarini, G.; Tonoli, E.; Gianoglio, S.; Schiappacasse, S.; Felli, L.; Picchetta, F.; Schito, G. Evaluation of the trophic effect of human placental polydeoxyribonucleotide on human knee skin fibroblasts in primary culture. Cell. Mol. Life Sci. CMLS 1997, 53, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Sini, P.; Denti, A.; Cattarini, G.; Daglio, M.; Tira, M.; Balduini, C. Effect of polydeoxyribonucleotides on human fibroblasts in primary culture. Cell Biochem. Funct. Cell. Biochem. Modul. Act. Agents Dis. 1999, 17, 107–114. [Google Scholar] [CrossRef]
- Thellung, S.; Florio, T.; Maragliano, A.; Cattarini, G.; Schettini, G. Polydeoxyribonucleotides enhance the proliferation of human skin fibroblasts: Involvement of A2 purinergic receptor subtypes. Life Sci. 1999, 64, 1661–1674. [Google Scholar] [CrossRef]
- Muratore, O.; Cattarini, G.; Gianoglio, S.; Tonoli, E.; Sacca, S.; Ghiglione, D.; Venzano, D.; Ciurlo, C.; Lantieri, P.; Schito, G. A human placental polydeoxyribonucleotide (PDRN) may promote the growth of human corneal fibroblasts and iris pigment epithelial cells in primary culture. New Microbiol. 2003, 26, 13–26. [Google Scholar]
- Guizzardi, S.; Galli, C.; Govoni, P.; Boratto, R.; Cattarini, G.; Martini, D.; Belletti, S.; Scandroglio, R. Polydeoxyribonucleotide (PDRN) promotes human osteoblast proliferation: A new proposal for bone tissue repair. Life Sci. 2003, 73, 1973–1983. [Google Scholar] [CrossRef]
- Saggini, R.; Di Stefano, A.; Cavezza, T.; Saladino, G.; Bellomo, R. Intrarticular treatment of osteoartropaty knee with polynucleotides: A pilot study with medium-term follow-up. J. Biol. Regul. Homeost. Agents 2013, 27, 543–549. [Google Scholar]
- Valdatta, L.; Thione, A.; Mortarino, C.; Buoro, M.; Tuinder, S. Evaluation of the efficacy of polydeoxyribonucleotides in the healing process of autologous skin graft donor sites: A pilot study. Curr. Med. Res. Opin. 2004, 20, 403–408. [Google Scholar] [CrossRef]
- Golob, M.; Marković, I.; Zovko, N.; Šakić, D.; Gudelj-Gračanin, A.; Morović-Vergles, J. Do We Pay Enough Attention to Neuropathic Pain in Knee Osteoarthritis Patients? Acta Clin. Croat. 2018, 57, 16–21. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group C (n = 5) | Group H (n = 5) | Group S (n = 5) | p-Value | |
|---|---|---|---|---|
| Age (years) | 68.0 ± 6.4 | 68.4 ± 8.2 | 67.6 ± 6.9 | 0.985 |
| Sex | 0.397 | |||
| Male | 1 (20%) | 0 (0%) | 0 (0%) | |
| Female | 4 (80%) | 5 (100%) | 5 (100%) | |
| Weight (kg) | 60.5 ± 4.8 | 64.3 ± 9.6 | 60.4 ± 11.2 | 0.747 |
| Height (cm) | 157.9 ± 4.7 | 154.7 ± 5.9 | 153.1 ± 7.7 | 0.481 |
| VAS Score (mm) | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Group C (n = 5) | T0 | 64.0 ± 18.2 | ||
| T6 | 12.0 ± 13.0 | |||
| T6–T0 | −52.0 ± 16.4 | −72.4–−31.60 | 0.006 * | |
| Group H (n = 5) | T0 | 44.0 ± 18.2 | ||
| T6 | 46.0 ± 21.9 | |||
| T6–T0 | 2.0 ± 22.8 | −26.31–30.60 | ||
| Group S (n = 5) | T0 | 64.0 ± 8.9 | ||
| T6 | 54.0 ± 19.5 | |||
| T6–T0 | −10.0 ± 26.5 | −42.85–22.85 | ||
| Post Hoc Analysis (Tukey’s HSD Test) | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Group C | Group H | −54.0 (−91.6–−16.4) | 0.006 * |
| Group S | −42.0 (−79.6–−4.4) | 0.029 * | |
| Group H | Group S | 12.0 (−25.6–49.6) | 0.680 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.Y.; Kim, Y.N.; Lee, Y.J.; Sim, S.E.; Ko, Y.R.; Shim, J.W.; Lee, K.S.; Joo, M.; Park, H.J. Pilot Study to Evaluate the Efficacy of Polynucleotide Sodium Compared to Sodium Hyaluronate and Crosslinked Sodium Hyaluronate in Patients with Knee Osteoarthritis. J. Clin. Med. 2021, 10, 1138. https://doi.org/10.3390/jcm10051138
Kim JY, Kim YN, Lee YJ, Sim SE, Ko YR, Shim JW, Lee KS, Joo M, Park HJ. Pilot Study to Evaluate the Efficacy of Polynucleotide Sodium Compared to Sodium Hyaluronate and Crosslinked Sodium Hyaluronate in Patients with Knee Osteoarthritis. Journal of Clinical Medicine. 2021; 10(5):1138. https://doi.org/10.3390/jcm10051138
Chicago/Turabian StyleKim, Ji Yeong, Yoo Na Kim, Yu Jung Lee, Sung Eun Sim, Yu Ri Ko, Jin Woo Shim, Ku Sang Lee, Mina Joo, and Hue Jung Park. 2021. "Pilot Study to Evaluate the Efficacy of Polynucleotide Sodium Compared to Sodium Hyaluronate and Crosslinked Sodium Hyaluronate in Patients with Knee Osteoarthritis" Journal of Clinical Medicine 10, no. 5: 1138. https://doi.org/10.3390/jcm10051138
APA StyleKim, J. Y., Kim, Y. N., Lee, Y. J., Sim, S. E., Ko, Y. R., Shim, J. W., Lee, K. S., Joo, M., & Park, H. J. (2021). Pilot Study to Evaluate the Efficacy of Polynucleotide Sodium Compared to Sodium Hyaluronate and Crosslinked Sodium Hyaluronate in Patients with Knee Osteoarthritis. Journal of Clinical Medicine, 10(5), 1138. https://doi.org/10.3390/jcm10051138