Abstract
The coronavirus disease 2019 (COVID-19) pandemic is related to psychological distress. Such distress depends on various factors. We previously reported that hemodialysis patients have more psychological distress than peritoneal dialysis patients among patients on dialysis in the COVID-19 pandemic era. However, no study has reported how psychological distress related to the COVID-19 pandemic depends on renal function in the entire group of chronic kidney disease (CKD) patients. Therefore, the objective of this study was to investigate psychological distress and concerns related to COVID-19 according to CKD stage. This was a cross-sectional study that included 397 CKD patients who visited a hospital from August 2020 to November 2020. Patients responded to questionnaires covering depression (9-item Patient Health Questionnaire, PHQ-9), anxiety (7-item Generalized Anxiety Disorder, GAD-7), psychological impact of event (22-item Impact of Event Scale-Revised, IES-R), insomnia (7-item Insomnia severity Index, ISI), concerns, and precautionary measures about COVID-19. According to eGFR and dialysis status, patients were divided into three groups: (1) patients with CKD stage 1~2, (2) patients with CKD stage 3~5 without dialysis, and (3) dialysis patients. The higher the CKD stage, the higher the GAD-7 (p = 0.009) and the ISI score (p = 0.001). When patients with CKD stage 1~2 and CKD stage 3~5 (with or without dialysis) were compared, PHQ-9 (p = 0.026), GAD-7 (p = 0.010), and ISI score (p = 0.002) were higher in the CKD stage 3~5 group. However, when comparing those with and without dialysis, only the ISI score (p = 0.008) showed a significant difference. More severe kidney dysfunction in CKD patients was associated with more psychological distress during the COVID-19 pandemic. Therefore, as CKD stage increases, more attention should be paid to the mental care of these patients.
1. Introduction
The outbreak of novel coronavirus, called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was initially reported to the World Health Organization (WHO) in December 2019. In March 2020, WHO declared that coronavirus disease 2019 (COVID-19) could be characterized as a pandemic, since this viral infection had spread rapidly to a number of countries [1]. As of 11 November 2020, the cumulative number of confirmed cases in Korea was 27,799, which was 441.1 per 100,000 population [2]. SARS-CoV-2 virus can affect the respiratory tract, gastrointestinal system, liver, heart, central nervous system, and kidney. It can lead to multiorgan failure [3]. Patients with older age and medical comorbidities are more likely to become infected, with worse outcomes [4].
The period of widespread occurrence of infectious diseases, such as COVID-19, may be closely related to psychological distress and symptoms of mental illness even in the general public without a psychiatric problem [5]. From the following sentence, psychological distress associated with the period of the COVID-19 pandemic will be referred to as “COVID-19-related psychological distress” for convenience. COVID-19-related psychological distress is caused not only by concerns about its infection, but also by large-scale isolation and overall socioeconomic problems [6]. Previous studies revealed the psychological impact of the period of the COVID-19 pandemic on anxiety, depressive symptoms, and sleep quality. Such an impact depends on age, gender, job status, specific physical symptoms (e.g., myalgia, dizziness, coryza), and preexisting psychiatric illness [7,8,9,10]. In addition, comorbidities, such as hypertension, diabetes mellitus, asthma, eczema, migraine, ischemic heart disease, and stroke, can affect mental health [8].
Likewise, one study suggested that older patients with chronic kidney disease (CKD) are more likely to develop psychiatric problems related to COVID-19 than other older patients without CKD [11]. A similar study was conducted on children with CKD [12]. As a result, children with CKD had more COVID-19-related anxiety than those without CKD [12]. Whether these results can be equally applied to general adults has not been confirmed. There are studies showing high levels of anxiety and depression in general adult-age patients receiving renal replacement therapy during the COVID-19 pandemic [13,14]. However, these studies did not include all CKD patients. They only included patients who underwent renal replacement therapy.
Other similar studies have reported the relationship between CKD and psychiatric problems before the COVID-19 pandemic. A study from western Rajasthan reported that 66% and 61% of CKD patients undergoing hemodialysis had depressive disorder and anxiety disorder, respectively [15]. One study observed that there is a direct linear correlation between CKD or ESRD and insomnia [16]. Specifically, a worsening CKD is directly associated with worsened insomnia [16]. It might be due to differences in comorbidities and individual perception of health caused by CKD. There are studies showing that the prevalence of inflammation and oxidant stress increases in CKD patients, leading to psychological distress, such as depression [17,18]. However, these studies were mainly conducted on dialysis patients. CKD patients not on dialysis, especially CKD stage 1~2 patients, were often excluded from these studies. We have previously reported psychological distress associated with COVID-19 in dialysis patients [19]. In that study, we compared hemodialysis (a procedure where a dialysis machine and a special filter called an artificial kidney, or a dialyzer, are used to clean one’s blood, performed 2–3 times a week at the hospital) patients and peritoneal dialysis (a treatment for kidney failure that uses the lining of the abdomen to filter one’s blood inside the body and can be practiced daily at home) patients and observed that hemodialysis patients had more psychological distress related to COVID-19. A limitation of that study was that there was no comparison with non-dialysis patients.
In order to overcome that limitation of the previous study, we added stage 1~5 non-dialysis CKD patients to dialysis patients in the previous study and tried to compare the degree of psychological distress according to their CKD stage. We hypothesized that the worse the patient’s renal function, the greater the psychological stress related to COVID-19.
2. Methods
2.1. Subjects
This was a cross-sectional, observational study of patients who received outpatient treatment at Nephrology Department of Soonchunhyang University Hospital Cheonan. The study protocol was approved by the Institutional Review Board of Soonchunhyang University Cheonan Hospital (No. 2020-07-029). All patients provided written informed consent before enrollment.
A survey was conducted from 17 August 2020 to 28 November 2020 when the monthly number of COVID-19 diagnosis cases had increased in Korea. A total of 397 patients with CKD defined by 2012 Kidney Disease: Improving Global Outcomes (KDIGO) guidelines who visited the Nephrology Department at Soonchunhyang University Cheonan were selected. Among patients selected for this study, patients with dialysis were included in the previous study [19]. Dialysis patients were taken part from August 2020 to September 2020. Although there is a slight difference in the timing, this period from August 2020 to November 2020 is when the number of confirmed COVID-19 patients was continuously maintained between 20,000 and 30,000, with little difference in incidence according to time.
Among them, those aged under 18 or above 90 years were excluded. Patients who could not complete the questionnaire due to cognitive degradation or illiteracy were excluded. Patients with any acute illness, hospitalization within three months, or a history of COVID-19 infection were also excluded.
Subjects were divided into three groups. First, according to Kidney Disease Outcomes Quality Initiative (KDOQI) definitions, non-dialysis patients were divided into two groups: stage 1–2 CKD patients with eGFR ≥ 60 mL/min and stage 3–5 CKD patients with eGFR < 60 mL/min according to eGFR calculated by Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. Patients with dialysis, including both peritoneal dialysis and hemodialysis, were used as the third group.
2.2. Survey Development
We investigated the medical history and laboratory data of patients at the time the questionnaires were administered by reviewing medical records. Their medical records included age and sex, diabetes mellitus or hypertension, statin intake, visit interval, and laboratory data.
To measure psychological distress, the same questionnaire as in the prior study was used [19]. The 9-item Patient Health Questionnaire (PHQ-9) [20] indicating the degree of depression, the 7-item Generalized Anxiety Disorder scale (GAD-7) [21] indicating the degree of anxiety, the 22-item Impact of Event Scale-Revised (IES-R) [22] indicating the degree of psychological impact of events, and the 7-item Insomnia severity Index (ISI) [23] indicating the degree of insomnia were used. Each questionnaire was scored. The severity was divided into normal, mild, moderate, and severe according to each score (PHQ-9: 0–8, 9–14, 15–19, 20–27; GAD-7: 0–4, 5–9, 10–14, 15–21; IES-R: 0–8, 9–25, 26–43, 44–88; and ISI: 0–7, 8–14, 15–21, 22–28).
To evaluate psychological distress related to COVID-19, a questionnaire was conducted on concerns and precautionary measures related to COVID-19 [8,19]. Concerns about COVID-19 included four questions. Precautionary measures related to COVID-19 included six questions. To determine whether time spent at home was related to psychological distress in CKD patients, correlation between each questionnaire score and time spent at home was analyzed.
2.3. Statistical Analysis
Jonckheere–Terpstra test [24] was used to confirm the tendency of demographic and psychological characteristics for patients with stage 1~2 CKD, patients with stage 3~5 CKD, and dialysis patients. Linear-by-linear association was used for categorical data. Student’s t-test was used to compare psychological characteristics between two groups (dialysis patients vs. non-dialysis CKD patients, CKD stage 3~5 patients (with or without dialysis) vs. CKD stage 1~2 patients). Logistic regression was utilized to exclude confounding factors such as HTN, DM, age, and sex. All statistical analyses were performed using SPSS version 26 (SPSS, Inc., Chicago, IL, USA). The significance level was set at p-value < 0.05.
3. Results
3.1. Patient Characteristics
We included a total of 397 CKD patients who visited Soonchunhyang University Cheonan Hospital from 17 August 2020 to 28 November 2020 during the COVID-19 pandemic. These patients were divided into three groups: patients with stage 1~2 CKD (eGFR ≥ 60mL/min, n = 111), non-dialytic patients with stage 3~5 CKD (eGFR < 60 mL/min, n = 138), and patients on dialysis (n = 148).
Baseline characteristics of study participants are presented in Table 1. The mean age of patients was 53.5 years for patients on dialysis, 60.3 years for patients with stage 3~5 CKD, and 51.2 years for patients with stage 1~2 CKD (p = 0.199). Gender ratio in patients on dialysis was similar to that in patients with stage 3~5 CKD and patients with stage 1~2 CKD (p = 0.366). The median visit interval became shorter as renal function deteriorated (15.0 days for patients on dialysis, 79.0 days for patients with stage 3~5 CKD, and 127.3 days for patients with stage 1~2 CKD, p < 0.001).

Table 1.
Baseline characteristics of study subjects.
The poorer the kidney function, the higher the prevalence of diabetes mellitus (DM) and hypertension (HTN). In total, 141 (35.25%) patients were diagnosed and treated with DM, including 55 (37.26%) in the group of dialysis patients, 63 (45.65%) in the group of patients with stage 3~5 CKD, and 23 (20.72%) in the group of patients with stage 1~2 CKD (p = 0.014). A total of 181 (71.83%) patients had HTN, including 124 (83.78%) in the group of dialysis patients, 115 (83.33%) in the group of patients with stage 3~5 CKD, and 65 (58.56%) in the group of patients with stage 1~2 CKD (p < 0.001).
Laboratory data were compared among the three CKD groups. Hemoglobin and hematocrit tended to lessen as kidney function deteriorated. Hb and Hct were around 14.07 g/dL and 41.63% in patients with stage 1~2 CKD, 11.87 g/dL and 35.50% in patients with stage 3~5 CKD, and 10.61 g/dL and 31.06% in dialysis patients, respectively. Potassium tended to be increased as kidney function deteriorated (4.33 mmol/L in patients with stage 1~2 CKD vs. 4.62 mmol/L in patients with stage 3~5 CKD vs. 4.54 mmol/L in dialysis patients, p < 0.001). Albumin tended to be less as kidney function deteriorated (4.49 g/dL in patients with stage 1~2 CKD vs. 4.24 g/dL in patients with stage 3~5 CKD vs. 3.94 g/dL in dialysis patients, p < 0.001). However, cholesterol and statin intake according to renal function showed no trend.
3.2. Psychological Measurements
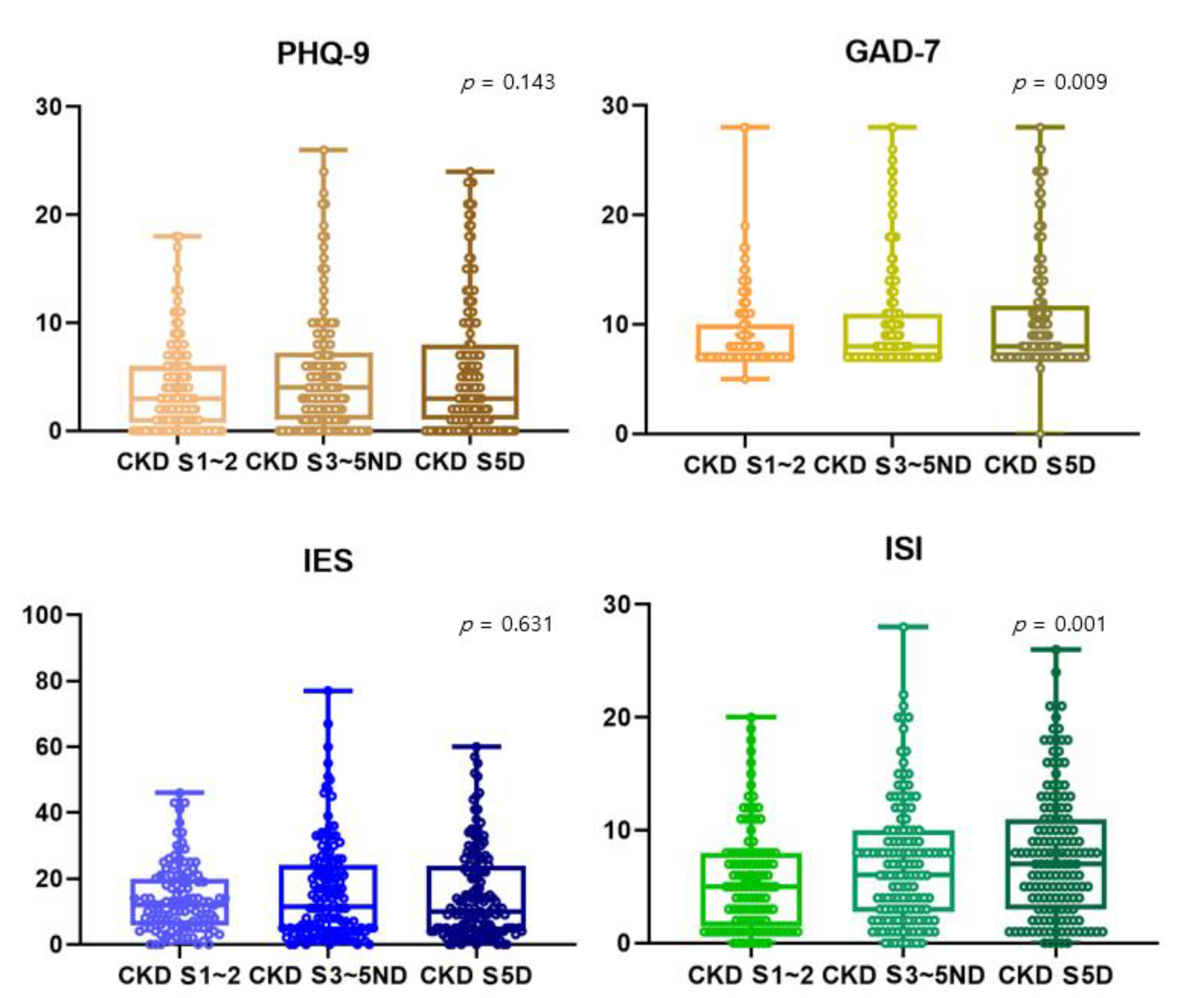
In Figure 1, all scores reflecting depression (PHQ-9), anxiety (GAD-7), stress (IES-R), and insomnia (ISI) tended to be higher as kidney function deteriorated. However, PHQ-9 and IES-R showed no statistically significant trend. GAD-7 score reflecting anxiety was around 10.51 for dialysis patients, 10.21 for patients with stage 3~5 CKD, and 9.00 for patients with stage 1~2 CKD (p = 0.009). ISI score reflecting insomnia was around 7.88 for dialysis patients, 7.01 for patients with stage 3~5 CKD, and 5.62 for patients with stage 1~2 CKD (p = 0.001) (Figure 1).
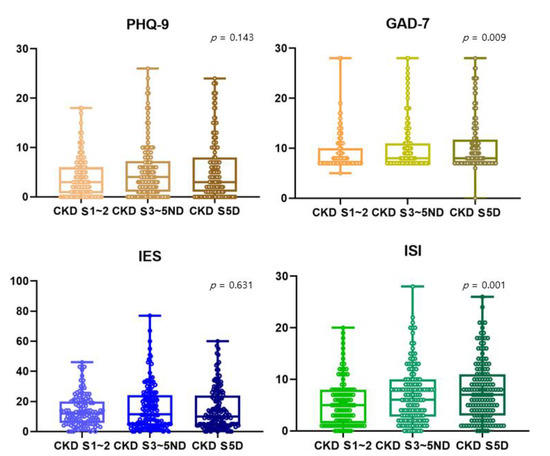
Figure 1.
Comparison of scores of PHQ-9, GAD-7, IES-R, and ISI among stage 1~2 CKD patients, stage 3~5 non-dialytic CKD patients, and dialysis patients. The Jonckheere–Terpstra test was used to see if there was a statistical significance for the tendency. The higher the CKD stage, the higher the anxiety (9.00 ± 3.69 vs. 10.21 ± 4.87 vs. 10.51 ± 5.19, p-value = 0.009) and insomnia (5.62 ± 4.58 vs. 7.01 ± 5.45 vs. 7.88 ± 5.74, p-value = 0.001) scores. CKD S5D, chronic kidney disease stage 5 dialysis; S3~5ND, stage 3~stage 5 non-dialysis; S1~2, stage 1~stage 2; PHQ-9, the 9-item Patient Health Questionnaire; GAD-7, the 7-item Generalized Anxiety Disorder scale; IES-R, the 22-item impact of Event Scale-Revised; ISI, insomnia severity index.
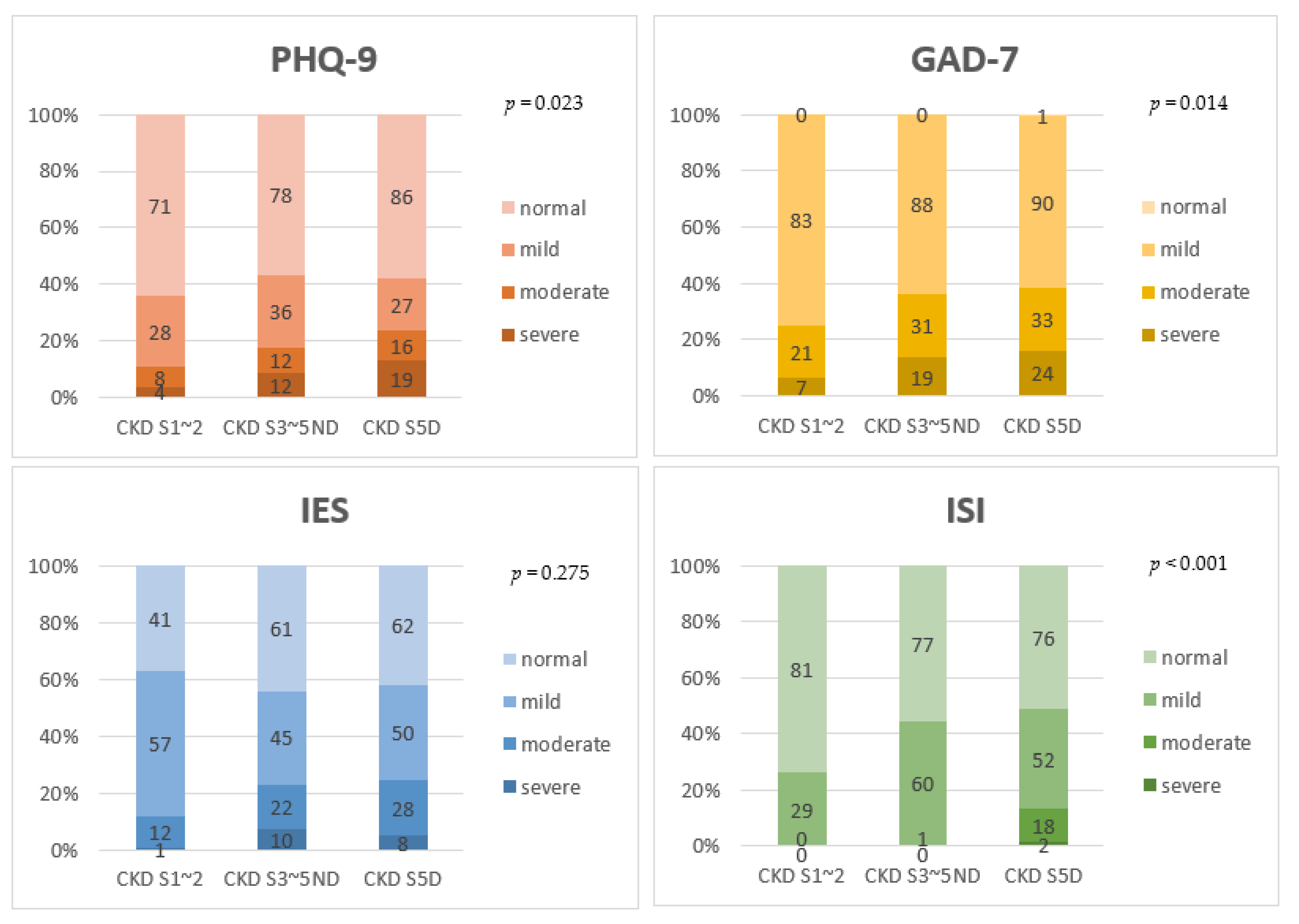
In terms of severity, the proportion of patients who scored high on PHQ-9, GAD-7, and ISI showed a tendency to increase as the renal function worsened (Figure 2). About 10.8% of patients with stage 1~2 CKD, 17.4% of patients with stage 3~5 CKD, and 23.6% of dialysis patients reported moderate to severe depression (p = 0.023). About 25.2% of patients with stage 1~2 CKD, 36.3% of patients with stage 3~5 CKD, and 38.5% of dialysis patients reported moderate to severe anxiety (p = 0.014). About 26.4% of patients with stage 1~2 CKD, 44.2% of patients with stage 3~5 CKD, and 48.7% of dialysis patients reported insomnia. Among the entire CKD cohort, only two patients in the dialysis group had severe insomnia (p < 0.001).
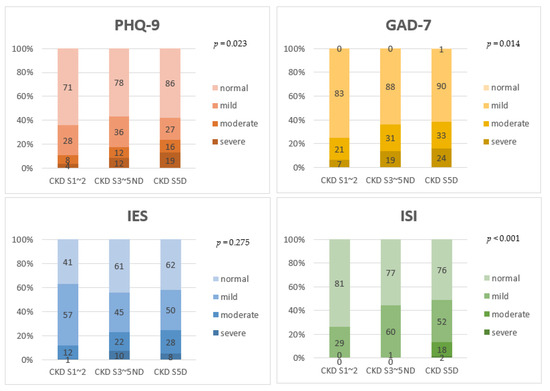
Figure 2.
Comparison of severity of PHQ-9, GAD-7, IES-R, and ISI among stage 1~2 CKD patients, stage 3~5 non-dialytic CKD patients, and dialysis patients. The linear-by-linear association test was used to see if there was a statistical significance for the tendency. As CKD stage increased, the proportion of patients with severe depression, anxiety, and insomnia also increased. CKD S5D, chronic kidney disease stage 5 dialysis; S3~5ND, stage 3~stage 5 non-dialysis; S1~2, stage 1~stage 2; PHQ-9, the 9-item Patient Health Questionnaire; GAD-7, the 7-item Generalized Anxiety Disorder scale; IES-R, the 22-item impact of Event Scale-Revised; ISI, insomnia severity index.
Logistic regression was performed to exclude confounding factors, such as HTN, DM, age, and sex. The outcome was set as a score in PHQ-9, IES-R, and ISI, corresponding to mild to severe depression, psychological impact of events, and insomnia, respectively. Since the number of normal patients based on the GAD-7 score was too small (n = 1), patients with moderate to severe anxiety were analyzed for outcomes. As a result, there was no statistical association between confounding factors (such as HTN, DM, age, and sex) and psychological distress, except that male gender was 0.607-times (p = 0.027) less likely to have moderate to severe anxiety than female gender. However, there was a significant association between CKD stage and anxiety (p = 0.013). Compared to patients with stage 1~2 CKD, patients with stage 3~5 CKD without dialysis and dialysis patients were 2.119-times (p = 0.016) and 2.341-times (p = 0.004) more likely to have moderate to severe anxiety, respectively. There was a significant association between CKD stage and insomnia (p < 0.001). Compared to patients with stage 1~2 CKD, patients with stage 3~5 CKD without dialysis and dialysis patients were 2.535-times (p = 0.002) and 3.019-times (p < 0.001) more likely to have mild to severe insomnia, respectively (Table 2).
Table 2.
Associations between psychological distress and baseline characteristics of study subjects.
When patients with stage 3~5 CKD were grouped into one group based on eGFR, regardless of dialysis statues, and compared with stage 1~2 CKD patients, PHQ-9, GAD-7, IES-R, and ISI scores were higher in the group of patients with stage 3~5 CKD. There were statistically significant differences in PHQ-9, GAD-7, ISI score, and severity among patient groups. PHQ-9 score was around 5.40 for patients with stage 3~5 CKD and 4.01 for patients with stage 1~2 CKD (p = 0.026). GAD-7 score was around 10.37 for patients with stage 3~5 CKD and 9.00 for patients with stage 1~2 CKD (p = 0.010). ISI score was around 7.45 for patients with stage 3~5 CKD and 5.62 for patients with stage 1~2 CKD (p = 0.002) (Table 3).
Table 3.
Comparison of score and severity of questionnaires covering mental health status between CKD stage 1~2 and CKD stage 3~5 with or without dialysis.
Similarly, when patients with stage 1~5 CKD without dialysis were grouped into one group and compared with dialysis patients, all questionnaire scores were higher in dialysis patients. However, there was no statistically significant difference, except for ISI score and severity (Supplementary Table S1).
3.3. Concerns and Precautionary Measures about COVID-19
Concerns and precautionary measures about COVID-19 in dialysis patients, stage 3~5 non-dialysis CKD patients, and stage 1~2 CKD patients are shown in Table 4. There was no statistically significant difference in concerns about COVID-19 in each group. Concerns about coming into contact with COVID-19 and concerns about the ability of doctors to diagnose were relatively low in all three groups. On the other hand, concerns about dying if infected with COVID-19 and concerns about other families were high.
Table 4.
Comparison of concerns and precautionary measures for 2019 coronavirus disease (COVID-19) in CKD patients.
Most patients answered that they followed precautions against COVID-19, especially covering mouth when coughing or sneezing and wearing a mask, regardless of the presence or absence of symptoms. There were no significant differences in precautionary measures for COVID-19 in each group, except for hours stayed at home per day to avoid COVID-19. Dialysis patients replied that they stayed at home for about 15.92 h per day, while stage 3~5 non-dialysis CKD patients and stage 1~2 CKD patients reported that they stayed at home for about 14.18 h per day and 13.00 h per day, respectively (p < 0.001).
As a result of the correlation study between each questionnaire score and the time spent at home, all questionnaire scores showed positive correlations with time stayed at home, although correlation coefficients were not large. Only the correlation between PHQ-9 score, suggesting depression, and time stayed at home showed statistical significance (p = 0.004) (Supplementary Figure S1).
When patients with stage 3~5 CKD, with or without dialysis, were compared with stage 1~2 CKD patients, results were similar to results when all three groups were compared (Table 5). However, when stage 1~5 CKD patients without dialysis were compared with dialysis patients, there was a difference in the perceived likelihood of contracting COVID-19 during the current outbreak. A larger percentage of non-dialysis CKD patients responded that they were likely to contract COVID-19 during the current outbreak (very likely: 1.6% vs. 0.7%; somewhat likely: 1.6% vs. 2.7%) (p = 0.042) (Supplementary Table S2).
Table 5.
Comparison of concerns and precautionary measures for 2019 coronavirus disease (COVID-19) between CKD stage 1~2 and CKD stage 3~5 patients with or without dialysis.
4. Discussion
In this study, we investigated psychological stress, including depression, anxiety, psychological impact of events, and insomnia, in the era of the COVID-19 pandemic for the entire group of CKD patients. In the present study, it was observed that anxiety and insomnia worsened as CKD stage increased for all CKD patients, including those with CKD stage 1~2. The same result was confirmed even after adjusting other confounding factors, such as HTN, DM, age, and sex. In the case of depression, it showed no statistically significant difference between those without dialysis and those with dialysis. However, it was significantly different between those with stage 1~2 CKD (eGFR ≥ 60 mL/min) and those with stage 3~5 CKD (eGFR < 60 mL/min).
To see if psychological distress answered by patients through questionnaires in this study was related to COVID-19, we investigated COVID-19-related concerns and precautionary measurements. As a result, concerns about dying if infected with COVID-19 and concerns about other families were high. Precautionary measures of covering mouth when coughing or sneezing and wearing mask, regardless of the symptoms, were followed by most patients. There were no significant differences according to CKD stage. Therefore, anxiety and insomnia, which worsen as the CKD stage increases, are more likely due to differences in comorbidities, chronic inflammation, oxidant stress, and individual perception of health caused by CKD, rather than differences in responses due to COVID-19. In many cases, the prevalence of chronic inflammation and oxidant stress increases as the CKD stage increases, but since there are individual differences, it may also act as a confounding factor for COVID-19-related psychological distress [17,18].
The time spent at home increased as the CKD stage increased. Dialysis modality may affect the number of hours that patients spend at home. Of the 148 dialysis patients who participated in the study, 78 patients on hemodialysis needed to spend time away from home and 70 patients on peritoneal dialysis needed to stay at home in order to perform their treatments. The time spent at home had a correlation with PHQ-9 score. It is currently unclear whether CKD patients are staying home longer because they are depressed or whether they are depressed because they have been at home for longer due to their concerns about COVID-19.
Because subjects in this study were only CKD patients, we were unable to compare psychological stress or COVID-19-related concerns and precautionary measurements with people with normal renal function. In simple comparison with a study conducted on the general public in China’s COVID-19 epidemic area, several concerns were more prevalent in CKD patients, including concerns about other family members being diagnosed with COVID-19 infection (75.2% in general public vs. 86.1% in CKD patients) and unlikely to survive if infected with COVID-19 (30.8% in general public vs. 45.4% in CKD patients) [8]. However, since these comparisons did not consider differences according to the study area or demographic characteristics of subjects, additional comparative studies on patients with normal renal function are needed.
In addition to the above, this study has other limitations. First, we were unable to assess an individual’s psychological condition before the outbreak due to sudden occurrence of the COVID-19 outbreak. Since there were no data before COVID-19, we could not know how much impact COVID-19 had on psychological distress. In a study conducted on hemodialysis patients in 2010, 1417 patients completed PHQ-9 assessment and 238 (17%) patients showed moderate to severe depression [25]. In comparison, in this study, moderate to severe depression was observed in a relatively large proportion (about 23%) of dialysis patients and about 18% of all CKD patients, regardless of stage. It is difficult to make a simple comparison with previous studies. Thus, follow-up studies are needed after the COVID-19 pandemic has passed. Second, scales used in this study were self-reported measures. PHQ-9, GAD-7, IES-R, and ISI might fail to fully reflect depression, anxiety, psychological impact, and insomnia in CKD patients. Constructed questions might not reflect all COVID-19-related concerns, although we tried to overcome these limitations by using reliable and validated instruments widely used in other studies [8]. COVID-19-related concerns were constructed with reference to a prior research study conducted in China [8].
5. Conclusions
Although this study showed that anxiety and insomnia increased with increasing CKD stage, whether this had a direct correlation with COVID-19 is unclear. However, previous studies reported that patients with psychological problems, such as anxiety and insomnia, are vulnerable to COVID-19-related stress [9,26]. One study suggested that depression and anxiety can be associated with suicide, fatigue, sleep disorder, and pain in CKD patients with hemodialysis [27]. Therefore, as CKD stage increases, more attention should be paid to not only physical care, but also mental care for these patients.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/article/10.3390/jcm11164776/s1, Figure S1: Hours stayed at home to avoid COVID-19 and PHQ-9, GAD-7, IES, and ISI scores of patients were compared through correlation analysis. All showed positive correlations, although their correlation coefficients were not large. Only the correlation between PHQ-9 suggesting depression and time stayed at home showed a statistical significance. PHQ-9, the 9-item Patient Health Questionnaire; GAD-7, the 7-item Generalized Anxiety Disorder scale; IES-R, the 22-item impact of Event Scale-Revised; ISI, insomnia severity index; Table S1: Comparison of score and severity of questionnaires covering mental health status between non-dialytic CKD and dialysis CKD patients; Table S2: Comparison of concerns and precautionary measures for 2019 coronavirus disease (COVID-19) between non-dialytic CKD and dialysis CKD patients.
Author Contributions
Conceptualization, E.Y.L., J.-S.K. and K.-M.L.; methodology, E.Y.L., J.-S.K. and K.-M.L.; data analysis and visualization, E.Y.L., N.J.C., S.P., H.W.G. and K.-M.L.; data curation, E.Y.L., N.J.C., S.P., H.W.G. and K.-M.L.; funding acquisition, E.Y.L.; writing—original draft preparation, E.Y.L., J.-S.K. and K.-M.L.; writing—review and editing: E.Y.L., S.H., N.J.C., S.P., H.W.G. and K.-M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a National Research Foundation (NRF) of Korea grant funded by the Korean Government (Ministry of Science and ICT) (2020R1A2C2003438) and the Soonchunhyang University Research Fund.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Soonchunhyang University Hospital Cheonan (approval reference no. 2020-07-029).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The authors confirm that the data supporting the findings are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-MentalHealth-2020.1 (accessed on 18 March 2020).
- Coronavirus Disease 2019 (COVID-19) Gyeonggi Daily Report—217 Data as Reported by 11 November 2020. Available online: http://www.gidcc.or.kr/gypd-type/covid-19-daily-reports/ (accessed on 11 November 2020).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Chen, N. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; Mckyer, E.L.J.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Research 2020, 9, 636. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Khan, F.A.; Shanmugam, G.N.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Chan, A.S.W.; Ho, J.M.C.; Li, J.S.F.; Tam, H.L.; Tang, P.M.K. Impacts of COVID-19 Pandemic on Psychological Well-Being of Older Chronic Kidney Disease Patients. Front. Med. 2020, 8, 666973. [Google Scholar] [CrossRef]
- Erfidan, G.; Özyurt, G.; Arslansoyu-Çamlar, S.; Özdemir-Şimşek, Ö.; Başaran, C.; Alaygut, D.; Mutlubaş, F.; Kasap-Demir, B. Is COVID-19 Related Anxiety Higher in Children With Chronic Kidney Disease Than Healthy Children? Pediatr. Int. 2021, 64, e14887. [Google Scholar]
- Gadia, P.; Awasthi, A.; Jain, S.; Koolwal, G.D. Depression and anxiety in patients of chronic kidney disease undergoing haemodialysis: A study from western Rajasthan. J. Fam. Med. Prim. Care 2020, 9, 4282–4286. [Google Scholar]
- Hanly, P. Sleep disorders and end-stage renal disease. Curr. Opin. Pulm. Med. 2008, 14, 543–550. [Google Scholar] [CrossRef]
- Lee, J.; Steel, J.; Roumelioti, M.E.; Erickson, S.; Myaskovsky, L.; Yabes, J.G.; Rollman, B.L.; Weisbord, S.; Unruh, M.; Jhamb, M. Psychosocial impact of COVID-19 pandemic on patients with end-stage kidney disease on hemodialysis. Kidney360 2020, 1, 1390–1397. [Google Scholar] [CrossRef]
- Barutcu, A.D.; Aydin, S.E.; Velioglu, A.; Tuglular, S. The association between perceived stress with sleep quality, insomnia, anxiety and depression in kidney transplant recipients during Covid-19 pandemic. PLoS ONE 2021, 16, e0248117. [Google Scholar] [CrossRef]
- Oberg, B.P.; McMenamin, E.; Lucas, F.L.; McMonagle, E.; Morrow, J.; Ikizler, T.A.; Himmelfarb, J. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004, 65, 1009–1016. [Google Scholar] [CrossRef]
- Dantzer, R.; O’Connor, J.C.; Lawson, M.A.; Kelley, K.W. Inflammation-associated depression: From serotonin to kynurenine. Psychoneuroendocrinology 2011, 36, 426–436. [Google Scholar] [CrossRef]
- Yu, J.Y.; Kim, J.S.; Hong, C.M.; Lee, K.Y.; Cho, N.J.; Park, S.; Gil, H.W.; Lee, E.Y. Psychological distress of patients with end-stage kidney disease undergoing dialysis during the 2019 coronavirus disease pandemic: A cross-sectional study in a University Hospital. PLoS ONE 2021, 16, e0260929. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Wiliams, J.B. Patient Health Questionnaire Primary Care Study Group. Valiation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary evaluation of mental disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Beck, J.G.; Grant, D.M.; Read, J.P.; Clapp, J.D.; Coffey, S.F.; Miller, L.M.; Palyo, S.A. The impact of event scale-revised: Psychometric properties in a sample of motor vehicle accident survivors. J. Anxiety Disord. 2008, 22, 187–198. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Jonckheere, A.R. A Distribution-Free k-Sample Test Against Ordered Alternatives. Biometrika 1954, 41, 133–145. [Google Scholar] [CrossRef]
- Belayev, L.Y.; Mor, M.K.; Sevick, M.A.; Shields, A.M.; Rollman, B.L.; Palevsky, P.M.; Arnold, R.M.; Fine, M.J.; Weisbord, S.D. Longitudinal associations of depressive symptoms and pain with quality of life in patients receiving chronic hemodialysis. Hemodial. Int. 2015, 19, 216–224. [Google Scholar] [CrossRef]
- Colodro-Conde, L.; Couvy-Duchesne, B.; Zhu, G.; Coventry, W.L.; Byrne, E.M.; Gordon, S.; Wright, M.J.; Montgomery, G.W.; Madden, P.A.F.; Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium; et al. A direct test of the diathesis–stress model for depression. Mol. Psychiatry 2018, 23, 1590–1596. [Google Scholar] [CrossRef]
- Chen, C.K.; Tsai, Y.C.; Hsu, H.J.; Wu, I.W.; Sun, C.Y.; Chou, C.C.; Lee, C.C.; Tsai, C.R.; Wu, M.S.; Wang, L.J. Depression and suicide risk in hemodialysis patients with chronic renal failure. Psychosomatics 2010, 51, 528. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).