
Injury Patterns and Incidence in an Elite Youth Football Academy—A Prospective Cohort Study of 138 Male Athletes

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Frequency and Pattern of Injuries
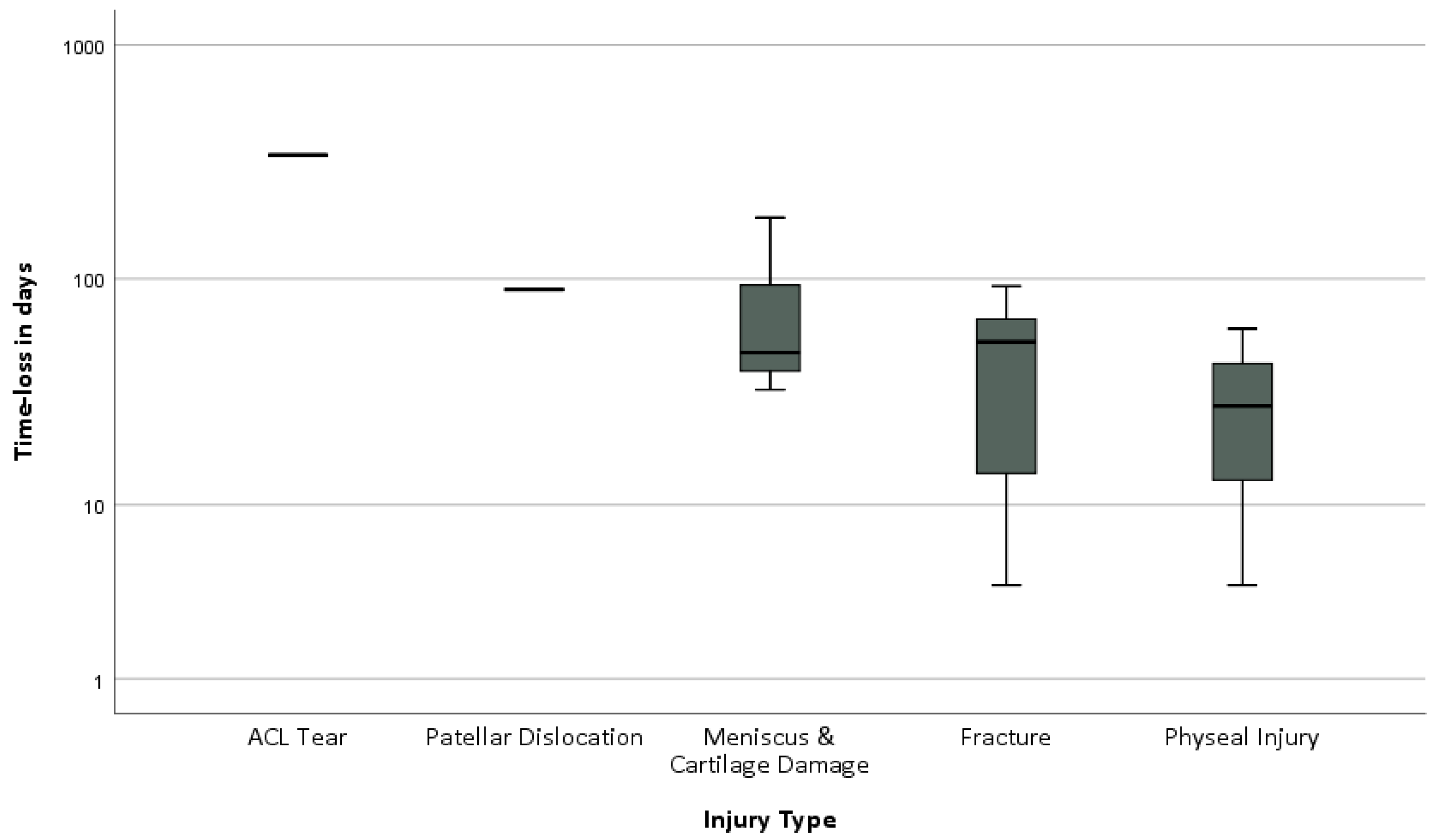
3.2. Injury Severity
3.3. Variations in Injury Incidence over the Course of a Season
3.4. Re-Injuries
4. Discussion
4.1. Frequency and Pattern of Injuries
4.2. Injury Severity
4.3. Variation in Injury Incidence over the Course of a Season
4.4. Re-Injuries
4.5. Strengths and Limitations
4.6. Future Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mountjoy, M.; Armstrong, N.; Bizzini, L.; Blimkie, C.; Evans, J.; Gerrard, D.; Hangen, J.; Knoll, K.; Micheli, L.; Sangenis, P.; et al. IOC consensus statement: “Training the elite child athlete”. Br. J. Sport Med. 2008, 42, 163–164. [Google Scholar] [CrossRef] [PubMed]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sport Med. 1992, 14, 82–99. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.D.; Hulse, M.A.; Wilkinson, C.; Hodson, A.; Gibson, M. The association football medical research programme: An audit of injuries in professional football. Br. J. Sport Med. 2001, 35, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, F.; Carling, C.; Reilly, T.; Vandewalle, H.; Church, J.; Rochcongar, P. Incidence of injuries in elite French youth soccer players: A 10-season study. Am. J. Sport Med. 2006, 34, 928–938. [Google Scholar] [CrossRef]
- Price, R.J.; Hawkins, R.D.; Hulse, M.A.; Hodson, A. The Football Association medical research programme: An audit of injuries in academy youth football. Br. J. Sport Med. 2004, 38, 466–471. [Google Scholar] [CrossRef]
- Bult, H.J.; Barendrecht, M.; Tak, I.J.R. Injury Risk and Injury Burden Are Related to Age Group and Peak Height Velocity Among Talented Male Youth Soccer Players. Orthop. J. Sport Med. 2018, 6, 2325967118811042. [Google Scholar] [CrossRef]
- Lee, I.; Jeong, H.S.; Lee, S.Y. Injury Profiles in Korean Youth Soccer. Int. J. Env. Res. Public Health 2020, 17, 5125. [Google Scholar] [CrossRef]
- Hall, E.C.R.; Larruskain, J.; Gil, S.M.; Lekue, J.A.; Baumert, P.; Rienzi, E.; Moreno, S.; Tannure, M.; Murtagh, C.F.; Ade, J.D.; et al. An injury audit in high-level male youth soccer players from English, Spanish, Uruguayan and Brazilian academies. Phys. Ther. Sport 2020, 44, 53–60. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. An audit of injuries in six english professional soccer academies. J. Sport Sci. 2018, 36, 1542–1548. [Google Scholar] [CrossRef]
- Renshaw, A.; Goodwin, P.C. Injury incidence in a Premier League youth soccer academy using the consensus statement: A prospective cohort study. BMJ Open. Sport Exerc. Med. 2016, 2, e000132. [Google Scholar] [CrossRef]
- Kemper, G.L.J.; van der Sluis, A.; Brink, M.S.; Visscher, C.; Frencken, W.G.P.; Elferink-Gemser, M.T. Anthropometric Injury Risk Factors in Elite-standard Youth Soccer. Int. J. Sport Med. 2015, 36, 1112–1117. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sport Med. 2011, 45, 553–558. [Google Scholar] [CrossRef]
- Jones, S.; Almousa, S.; Gibb, A.; Allamby, N.; Mullen, R.; Andersen, T.E.; Williams, M. Injury Incidence, Prevalence and Severity in High-Level Male Youth Football: A Systematic Review. Sport Med. 2019, 49, 1879–1899. [Google Scholar] [CrossRef] [PubMed]
- Jaber, A.; Weishorn, J.; Berrsche, G.; Ott, H.; Bangert, Y. Injury Profile among Elite Youth Male Football Players in a German Academy. Int. J. Sport Med. 2021, 43, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br. J. Sport Med. 2006, 40, 193. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Bahr, R.; Ekstrand, J. Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br. J. Sport Med. 2005, 39, 340–346. [Google Scholar] [CrossRef]
- Bowen, L.; Gross, A.S.; Gimpel, M.; Li, F.X. Accumulated workloads and the acute:chronic workload ratio relate to injury risk in elite youth football players. Br. J. Sport Med. 2017, 51, 452–459. [Google Scholar] [CrossRef]
- Tears, C.; Chesterton, P.; Wijnbergen, M. The elite player performance plan: The impact of a new national youth development strategy on injury characteristics in a premier league football academy. J. Sport Sci. 2018, 36, 2181–2188. [Google Scholar] [CrossRef]
- Materne, O.; Chamari, K.; Farooq, A.; Weir, A.; Hölmich, P.; Bahr, R.; Greig, M.; McNaughton, L.R. Injury incidence and burden in a youth elite football academy: A four-season prospective study of 551 players aged from under 9 to under 19 years. Br. J. Sport Med. 2021, 55, 493–500. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Ekstrand, J. Injuries in Swedish elite football--a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand. J. Med. Sci. Sport 2005, 15, 118–125. [Google Scholar] [CrossRef]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of Injury Incidences in Male Professional Adult and Elite Youth Soccer Players: A Systematic Review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Cezarino, L.G.; Grüninger, B.; Scattone Silva, R. Injury Profile in a Brazilian First-Division Youth Soccer Team: A Prospective Study. J. Athl. Train. 2020, 55, 295–302. [Google Scholar] [CrossRef] [PubMed]
- van der Sluis, A.; Elferink-Gemser, M.T.; Brink, M.S.; Visscher, C. Importance of Peak Height Velocity Timing in Terms of Injuries in Talented Soccer Players. Int. J. Sport Med. 2015, 36, 327–332. [Google Scholar] [CrossRef]
- Faude, O.; Rößler, R.; Junge, A. Football injuries in children and adolescent players: Are there clues for prevention? Sport Med. 2013, 43, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Krutsch, W.; Lehmann, J.; Jansen, P.; Angele, P.; Fellner, B.; Achenbach, L.; Krutsch, V.; Nerlich, M.; Alt, V.; Loose, O. Prevention of severe knee injuries in men’s elite football by implementing specific training modules. Knee Surg. Sport Traumatol. Arthrosc. 2020, 28, 519–527. [Google Scholar] [CrossRef]
- Rosado-Portillo, A.; Chamorro-Moriana, G.; Gonzalez-Medina, G.; Perez-Cabezas, V. Acute Hamstring Injury Prevention Programs in Eleven-a-Side Football Players Based on Physical Exercises: Systematic Review. J. Clin. Med. 2021, 10, 2029. [Google Scholar] [CrossRef]
- Al Attar, W.S.A.; Soomro, N.; Sinclair, P.J.; Pappas, E.; Sanders, R.H. Effect of Injury Prevention Programs that Include the Nordic Hamstring Exercise on Hamstring Injury Rates in Soccer Players: A Systematic Review and Meta-Analysis. Sport Med. 2017, 47, 907–916. [Google Scholar] [CrossRef]
- Schuermans, J.; Danneels, L.; Van Tiggelen, D.; Palmans, T.; Witvrouw, E. Proximal Neuromuscular Control Protects Against Hamstring Injuries in Male Soccer Players: A Prospective Study With Electromyography Time-Series Analysis During Maximal Sprinting. Am. J. Sport Med. 2017, 45, 1315–1325. [Google Scholar] [CrossRef]
- van de Hoef, P.A.; Brink, M.S.; Huisstede, B.M.A.; van Smeden, M.; de Vries, N.; Goedhart, E.A.; Gouttebarge, V.; Backx, F.J.G. Does a bounding exercise program prevent hamstring injuries in adult male soccer players?—A cluster-RCT. Scand. J. Med. Sci. Sport 2019, 29, 515–523. [Google Scholar] [CrossRef]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sport Med. 2016, 50, 731–737. [Google Scholar] [CrossRef]
- O’Brien, J.; Finch, C.F. A systematic review of core implementation components in team ball sport injury prevention trials. Inj. Prev. 2014, 20, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Materne, O.; Chamari, K.; Farooq, A.; Tabben, M.; Weir, A.; Holmich, P.; Bahr, R.; Greig, M.; McNaughton, L.R. Shedding light on incidence and burden of physeal injuries in a youth elite football academy: A 4-season prospective study. Scand. J. Med. Sci. Sport 2022, 32, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Tagliero, A.J.; Desai, V.S.; Kennedy, N.I.; Camp, C.L.; Stuart, M.J.; Levy, B.A.; Dahm, D.L.; Krych, A.J. Seventeen-Year Follow-up After Meniscal Repair With Concomitant Anterior Cruciate Ligament Reconstruction in a Pediatric and Adolescent Population. Am. J. Sport Med. 2018, 46, 3361–3367. [Google Scholar] [CrossRef]
- Zebis, M.K.; Aagaard, P.; Andersen, L.L.; Hölmich, P.; Clausen, M.B.; Brandt, M.; Husted, R.S.; Lauridsen, H.B.; Curtis, D.J.; Bencke, J. First-time anterior cruciate ligament injury in adolescent female elite athletes: A prospective cohort study to identify modifiable risk factors. Knee Surg. Sport Traumatol. Arthrosc. 2022, 30, 1341–1351. [Google Scholar] [CrossRef]
- Sandon, A.; Söderström, T.; Stenling, A.; Forssblad, M. Can Talented Youth Soccer Players Who Have Undergone Anterior Cruciate Ligament Reconstruction Reach the Elite Level? Am. J. Sport Med. 2021, 49, 384–390. [Google Scholar] [CrossRef]
- Della Villa, F.; Hägglund, M.; Della Villa, S.; Ekstrand, J.; Waldén, M. High rate of second ACL injury following ACL reconstruction in male professional footballers: An updated longitudinal analysis from 118 players in the UEFA Elite Club Injury Study. Br. J. Sport Med. 2021, 55, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, A.J.; Whitaker, J.R.; Collofello, B.S.; Wilson, B.R.; Unger, R.Z.; Ireland, M.L.; Johnson, D.L.; Jacobs, C.A. Secondary Injuries After Pediatric Anterior Cruciate Ligament Reconstruction: A Systematic Review With Quantitative Analysis. Am. J. Sport Med. 2021, 49, 1086–1093. [Google Scholar] [CrossRef]
- Silvers-Granelli, H.; Mandelbaum, B.; Adeniji, O.; Insler, S.; Bizzini, M.; Pohlig, R.; Junge, A.; Snyder-Mackler, L.; Dvorak, J. Efficacy of the FIFA 11+ Injury Prevention Program in the Collegiate Male Soccer Player. Am. J. Sport Med. 2015, 43, 2628–2637. [Google Scholar] [CrossRef]
- Ekstrand, J.; Spreco, A.; Windt, J.; Khan, K.M. Are Elite Soccer Teams’ Preseason Training Sessions Associated With Fewer In-Season Injuries? A 15-Year Analysis From the Union of European Football Associations (UEFA) Elite Club Injury Study. Am. J. Sport Med. 2020, 48, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Sonesson, S.; Lindblom, H.; Hägglund, M. Higher age and present injury at the start of the season are risk factors for in-season injury in amateur male and female football players-a prospective cohort study. Knee Surg. Sport Traumatol. Arthrosc. 2023, 31, 4618–4630. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injury incidence and distribution in elite football--a prospective study of the Danish and the Swedish top divisions. Scand. J. Med. Sci. Sport 2005, 15, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Holme, I. Risk factors for sports injuries—A methodological approach. Br. J. Sport Med. 2003, 37, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Schmoor, C.; Sauerbrei, W.; Schumacher, M. Sample size considerations for the evaluation of prognostic factors in survival analysis. Stat. Med. 2000, 19, 441–452. [Google Scholar] [CrossRef]
- Ekstrand, J.; Spreco, A.; Bengtsson, H.; Bahr, R. Injury rates decreased in men’s professional football: An 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br. J. Sport Med. 2021, 55, 1084–1091. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Previous injury as a risk factor for injury in elite football: A prospective study over two consecutive seasons. Br. J. Sport Med. 2006, 40, 767–772. [Google Scholar] [CrossRef]
- Obërtinca, R.; Hoxha, I.; Meha, R.; Lama, A.; Bimbashi, A.; Kuqi, D.; Shabani, B.; Meyer, T.; der Fünten, K.A. Efficacy of Multi-Component Exercise-Based Injury Prevention Programs on Injury Risk Among Footballers of All Age Groups: A Systematic Review and Meta-analysis. Sport Med. 2023, 53, 837–848. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Terminology | Description |
|---|---|
| Muscle | |
| Tear | Injuries with structural damage or complete muscle rupture, corresponding to grades IIIa, b and IV according to Müller-Wohlfahrt et al. |
| Strain | Injuries with functional damage, corresponding to grade II according to Müller-Wohlfahrt et al. |
| Functional Muscle disorder | Injuries involving functional disorders without structural damage to the musculature (e.g., neuromuscular disorders or fatigue-related muscular disorders) |
| Bone | |
| Physeal injury | Physeal injuries other than physeal fractures (e.g., apophysitis) |
| Mature Bone | |
| Fracture | All fractures of mature bones caused by trauma |
| Other Bone injury | Structural bone damage such as bone marrow oedema, stress fractures or periostitis |
| Ligament | |
| Sprain/Ligament injury | Strained or torn ligaments responsible for joint stability |
| Others | |
| Concussion | Mild traumatic brain injury resulting from head impact or acceleration-deceleration forces |
| Skin lesion | Mechanical or thermal damage causing a disruption of the skin barrier. |
| Other injury | Acute functional impairment without diagnosis of specific tissue pathology |
| Non-specific overuse | Slow-onset functional impairment reported without diagnosis of specific tissue pathology |
| Age Groups | Total Players | Age (years, SD) | Stature (cm, SD) | Body Mass (kg, SD) | BMI (kg/m2, SD) | League |
|---|---|---|---|---|---|---|
| U-12 | 15 | 11.8 (0.4) | 148.1 (7,1) | 42.1 (5.5) | 19.2 (1.9) | Kreisklasse A |
| U-13 | 18 | 12.7 (0.5) | 156.7 (7.2) | 44.7 (6.1) | 18.2 (1.8) | Landesliga Rhein-Neckar |
| U-14 | 20 | 13.5 (0.5) | 161.4 (7.0) | 48.3 (5.9) | 18.5 (1.8) | Oberliga Baden-Württemberg |
| U-15 | 21 | 14.6 (0.5) | 168.5 (7.3) | 55.4 (6.1) | 19.5 (2.0) | Regionalliga Süd |
| U-16 | 22 | 15.7 (0.5) | 173.8 (6.4) | 62.5 (6.2) | 20.7 (1.7) | Oberliga Baden-Württemberg |
| U-17 | 21 | 16.6 (0.5) | 176.7 (5.2) | 69.8 (6.7) | 22.4 (1.6) | Bundesliga |
| U-19 | 21 | 18.0 (0.8) | 181.7 (7.8) | 75.1 (7.5) | 22.7 (2.1) | Bundesliga |
| All Teams | 138 | 14.9 (2.1) | 166.7 (6.9) | 56.8 (6.3) | 20.4 (1.8) |
| Injury Location | Frequency n (%) | 4–7 Days | 8–28 Days | >28 Days |
|---|---|---|---|---|
| Head/Neck | 5 (5) | 2 (4) | 3 (7) | - |
| Shoulder/Clavicula | 2 (2) | 2 (4) | - | - |
| Ellbow | 1 (1) | - | 1 (2) | - |
| Forearm | 3 (3) | 1 (2) | 1 (2) | 1 (5) |
| Hand | 4 (4) | 3 (7) | - | 1 (5) |
| Trunk | 3 (3) | 1 (2) | 2 (5) | - |
| Hip/Pelvis | 5 (5) | - | 2 (5) | 3 (14) |
| Thigh | 26 (24) | 15 (33) | 9 (21) | 2 (10) |
| Knee | 21 (19) | 5 (11) | 10 (23) | 6 (29) |
| Lower leg/Calf | 6 (6) | 3 (7) | 3 (7) | - |
| Ankle | 22 (20) | 9 (20) | 11 (26) | 2 (10) |
| Foot/Toe | 11 (10) | 4 (9) | 1 (2) | 6 (29) |
| Overall | 109 (100%) | 45 | 43 | 21 |
| Diagnosis | Frequency n (%) | Total Time-Loss (Days) | Median Time-Loss (IQ 25th–75th) |
|---|---|---|---|
| Head and neck | 5 (4.6%) | 44 | 10 (4.5–12.5) |
| Concussion | 2 (1.8%) | 21 | 10.5 (10–10.5) |
| Nasal bone fracture | 2 (1.8%) | 18 | 9 (4–9) |
| Cut | 1 (0.9%) | 5 | 5 (5–5) |
| Upper Limb | 10 (9.2%) | 225 | 7 (4.75–31.75) |
| AC-Contusion | 1 (0.9%) | 4 | 4 (4–4) |
| Shoulder Contusion | 1 (0.9%) | 5 | 5 (5–5) |
| Ellbow Contusion | 1 (0.9%) | 8 | 8 (8–8) |
| Forearm Contusion | 1 (0.9%) | 7 | 7 (7–7) |
| Forearm Fracture | 2 (1.8%) | 91 | 45.5 (45–46) |
| Hand Contusion | 2 (1.8%) | 11 | 5.5 (5–6) |
| Hand/Finger sprain | 1 (0.9%) | 6 | 6 (6–6) |
| Hand/Finger fracture | 1 (0.9%) | 93 | 93 (93–93) |
| Trunk | 3 (2.8%) | 42 | 11 (5.0–11) |
| Overuse unspecific pathology | 2 (1.8%) | 37 | 18.5 (11–18.5) |
| Functional muscle disorder | 1 (0.9%) | 5 | 5 (5–5) |
| Hip and Pelvis | 5 (4.6%) | 176 | 36 (13.5–58.5) |
| Physeal injury (avulsion) | 2 (1.8%) | 68 | 34 (12–34) |
| Physeal injury (apophysitis) | 2 (1.8%) | 97 | 48.5 (36–48.5) |
| Gluteal strain | 1 (0.9%) | 15 | 15 (15–15) |
| Thigh | 26 (23.9%) | 317 | 6.0 (4–32.5) |
| Torn Hamstrings | 5 (4.6%) | 140 | 23.0 (13–44) |
| Torn Quadriceps | 1 (0.9%) | 15 | 15 (15–15) |
| Thigh Contusion | 3 (2.8%) | 15 | 5 (4–5) |
| Adductor strain | 5 (4.6%) | 56 | 11 (5.0–17.5) |
| Hamstring strain | 4 (3.7%) | 17 | 4 (4–4.75) |
| Quadrizeps strain | 8 (7.3%) | 74 | 6 (4–13) |
| Knee | 21 (19.3%) | 929 | 14 (7.5–38) |
| Knee Sprain/Ligament | 9 (8.3%) | 103 | 10 (4–16) |
| Meniscus and Cartilage Damage | 3 (2.8%) | 264 | 48 (33–48) |
| Physeal injury (apophysitis) | 7 (6.4%) | 133 | 14 (8–28) |
| Patellar dislocation | 1 (0.9%) | 90 | 90 (90–90) |
| Torn ACL | 1 (0.9%) | 339 | 339 (339–339) |
| Lower leg and calf | 6 (5.5%) | 47 | 7.5 (5.75–9.75) |
| Functional muscle disorder | 1 (0.9%) | 12 | 12 (12–12) |
| Torn Calf muscle | 1 (0.9%) | 8 | 8 (8–8) |
| Calf muscles strain | 3 (2.7%) | 20 | 6 (5–6) |
| Calf Cut | 1 (0.9%) | 7 | 7 (7–7) |
| Foot and Ankle | 33 (30.3%) | 752 | 14 (5–31) |
| Ankle Sprain/Ligament | 19 (17.4%) | 295 | 13.0 (7–19) |
| Ankle contusion | 1 (0.9%) | 4 | 4 (4–4) |
| Ankle fracture | 1 (0.9%) | 57 | 57 (57–57) |
| Ankle Stress injury | 1 (0.9%) | 5 | 5 (5–5) |
| Physeal injury (apophysitis) | 2 (1.8%) | 88 | 44 (39–44) |
| Foot/Toes fracture | 4 (3.7%) | 185 | 56 (17–65.8) |
| Foot Contusion | 3 (2.8%) | 96 | 4 (4–4) |
| Foot sprain | 2(1.8%) | 22 | 11 (4–11) |
| Mean (SD) | |||
| Total | 109 (100%) | 2536 | 23.3 (40.1) |
| Injury Type | Total n (%) | 4–7 Days n (%) | 8–28 Days n (%) | >28 Days n (%) |
|---|---|---|---|---|
| Ligament sprain | 31 (28) | 13 (29) | 17 (40) | 1 (5) |
| Muscle strain | 21 (19) | 14 (31) | 7 (16) | - |
| Physeal injury | 13 (12) | 1 (2) | 6 (14) | 6 (29) |
| Contusion | 13 (12) | 11 (24) | 1 (2) | 1 (5) |
| Fracture | 10 (9) | 2 (4) | 2 (5) | 6 (29) |
| Muscle tear | 7 (6) | - | 5 (12) | 2 (10) |
| Meniscus and Cartilage lesion | 3 (3) | - | - | 3 (14) |
| Functional muscle disorder | 2 (2) | 1 (2) | 1 (2) | - |
| Concussion | 2 (2) | - | 2 (5) | - |
| Cut | 2 (2) | 2 (4) | - | - |
| ACL tear | 1 (1) | - | - | 1 (5) |
| Dislocation | 1 (1) | - | - | 1 (5) |
| Stress injury | 1 (1) | 1 (2) | - | - |
| Other overuse | 2 (2) | - | 2 (5) | - |
| Injury Type | Incidence n (%) | Incidence/1000 h | Incidence/Squad-Season * | Incidence/Squad-Season ** | Mean Time-Loss (95%-KI) | Training/Match-Ratio |
|---|---|---|---|---|---|---|
| Ligament sprain | 31 (28) | 0.7 | 4.4 | 5.6 | 13.8 (8.9–18.6) | 1.6 |
| Muscle strain | 21 (19) | 0.5 | 3.0 | 3.8 | 8.7 (5.6–11.7) | 6 |
| Physeal injury | 13 (12) | 0.3 | 1.9 | 2.4 | 29.7 (18.2–41.2) | 5.5 |
| Contusion | 13 (12) | 0.3 | 1.9 | 2.4 | 11.5 (0–25.5) | 1.2 |
| Fracture | 10 (9) | 0.2 | 1.4 | 1.8 | 44.4 (21.9–66.9) | 0.67 |
| Torn Muscle | 7 (6) | 0.2 | 1.0 | 1.3 | 16 (13–43) | 0.75 |
| Meniscus and Cartilage | 3 (3) | 0.1 | 0.4 | 0.6 | 88 (0–293) | - |
| Functional muscle disorder | 2 (2) | 0.1 | 0.3 | 0.4 | 8.5 (0–53.0) | 1 |
| Concussion | 2 (2) | 0.1 | 0.3 | 0.4 | 10.5 (4.2–16.9) | 1 |
| Cut | 2 (2) | 0.1 | 0.3 | 0.4 | 6 (0–18.7) | 1 |
| ACL tear | 1 (1) | 0.05 | 0.1 | 0.2 | 339 | - |
| Dislocation | 1 (1) | 0.05 | 0.1 | 0.2 | 90 | - |
| Stress injury | 1 (1) | 0.05 | 0.1 | 0.2 | 5 | - |
| Other overuse | 2 (2) | 0.1 | 0.3 | 0.4 | 18.5 (0–113.8) | - |
| Overall | 109 (100) | 2.6 | 15.6 | 19.7 | 23.3 (15.7–30.9) | 1.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weishorn, J.; Jaber, A.; Zietzschmann, S.; Spielmann, J.; Renkawitz, T.; Bangert, Y. Injury Patterns and Incidence in an Elite Youth Football Academy—A Prospective Cohort Study of 138 Male Athletes. J. Clin. Med. 2023, 12, 6138. https://doi.org/10.3390/jcm12196138
Weishorn J, Jaber A, Zietzschmann S, Spielmann J, Renkawitz T, Bangert Y. Injury Patterns and Incidence in an Elite Youth Football Academy—A Prospective Cohort Study of 138 Male Athletes. Journal of Clinical Medicine. 2023; 12(19):6138. https://doi.org/10.3390/jcm12196138
Chicago/Turabian StyleWeishorn, Johannes, Ayham Jaber, Severin Zietzschmann, Jan Spielmann, Tobias Renkawitz, and Yannic Bangert. 2023. "Injury Patterns and Incidence in an Elite Youth Football Academy—A Prospective Cohort Study of 138 Male Athletes" Journal of Clinical Medicine 12, no. 19: 6138. https://doi.org/10.3390/jcm12196138