

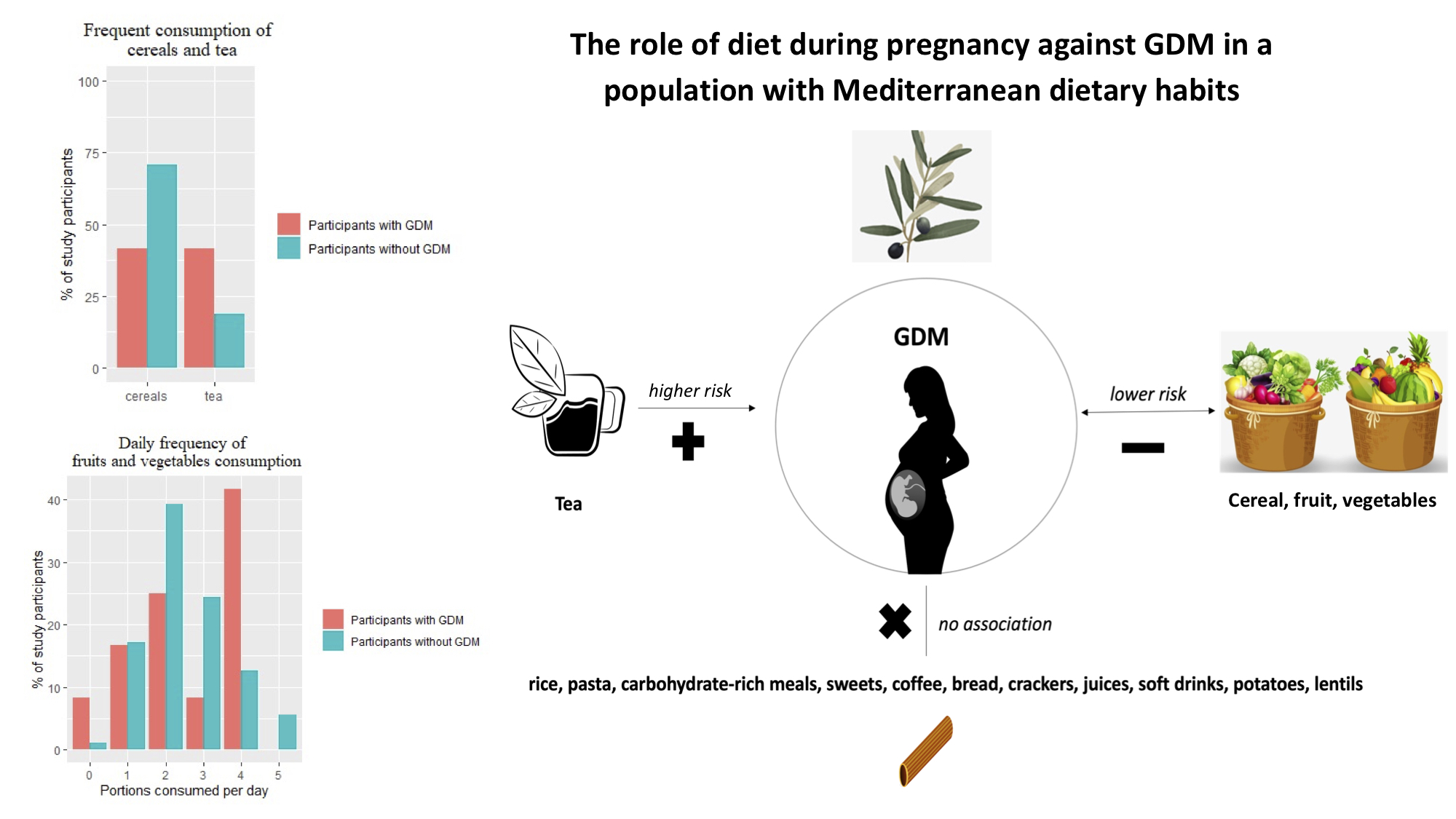
The Role of Diet during Pregnancy in Protecting against Gestational Diabetes Mellitus in a Population with Mediterranean Dietary Habits: A Cross-Sectional Study
 , , and
, , and 
Abstract

1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Diabetes Association 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef]
- Guariguata, L.; Linnenkamp, U.; Beagley, J.; Whiting, D.R.; Cho, N.H. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res. Clin. Pract. 2014, 103, 176–185. [Google Scholar] [CrossRef]
- Metzger, B.E. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- Group, H.S.C.R. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Int. J. Gynecol. Obstet. 2002, 78, 69–77. [Google Scholar] [CrossRef]
- Metzger, B.E.; Contreras, M.; Sacks, D.A.; Watson, W.; Dooley, S.L.; Foderaro, M.; Niznik, C.; Bjaloncik, J.; Catalano, P.M.; Dierker, L.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Wah Cheung, N.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C.; et al. Associations of diet and physical activity with risk for gestational diabetes mellitus: A Systematic review and meta-analysis. Nutrients 2018, 10, 698. [Google Scholar] [CrossRef]
- Karamanos, B.; Thanopoulou, A.; Anastasiou, E.; Assaad-Khalil, S.; Albache, N.; Bachaoui, M.; Slama, C.B.; El Ghomari, H.; Jotic, A.; Lalic, N.; et al. Relation of the Mediterranean diet with the incidence of gestational diabetes. Eur. J. Clin. Nutr. 2014, 68, 8–13. [Google Scholar] [CrossRef]
- Tieu, J.; Shepherd, E.; Middleton, P.; Crowther, C.A. Dietary advice interventions in pregnancy for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 8–41. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Zaragoza-Martí, A.; Ruiz-Ródenas, N.; Herranz-Chofre, I.; Sánchez-SanSegundo, M.; Delgado, V.D.; Hurtado-Sánchez, J.A. Adherence to the Mediterranean Diet in Pregnancy and Its Benefits on Maternal-Fetal Health: A Systematic Review of the Literature. Front. Nutr. 2022, 9, 813942. [Google Scholar] [CrossRef] [PubMed]
- Biagi, C.; Di Nunzio, M.; Bordoni, A.; Gori, D.; Lanari, M. Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients 2019, 11, 997. [Google Scholar] [CrossRef] [PubMed]
- Bédard, A.; Northstone, K.; John Henderson, A.; Shaheen, S.O. Mediterranean diet during pregnancy and childhood respiratory and atopic outcomes: Birth cohort study. Eur. Respir. J. 2020, 55, 1901215. [Google Scholar] [CrossRef] [PubMed]
- Petrakos, G.; Panagopoulos, P.; Koutras, I.; Kazis, A.; Panagiotakos, D.; Economou, A.; Kanellopoulos, N.; Salamalekis, E.; Zabelas, A. A comparison of the dietary and total intake of micronutrients in a group of pregnant Greek women with the Dietary Reference Intakes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 127, 166–171. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2017. [Google Scholar]
- Yoshida, K.; Bohn, J. Tableone: Create “Table 1” to describe baseline characteristics. 2015. Available online: https://cran.r-project.org/package=tableone (accessed on 8 September 2022).
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Package Version 2.2.9; Northwestern University: Evanston, IL, UAS, 2022; Available online: https://CRAN.R-project.org/package=psych (accessed on 8 September 2022).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Kathleen, M.; Rasmussen, K.; Yaktine, A. Institute of Medicine and National Research Council. In Weight Gain during Pregnancy: Reexamining the Guidelines; National Academy Press: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, S.; Solomon, C.G.; Hu, F.B. Dietary fiber intake, dietary glycemic load, and the risk for gestational diabetes mellitus. Diabetes Care 2006, 29, 2223–2230. [Google Scholar] [CrossRef]
- Bao, W.; Bowers, K.; Tobias, D.K.; Olsen, S.F.; Chavarro, J.; Vaag, A.; Kiely, M.; Zhang, C. Prepregnancy low-carbohydrate dietary pattern and risk of gestational diabetes mellitus: A prospective cohort study. Am. J. Clin. Nutr. 2014, 99, 1378–1384. [Google Scholar] [CrossRef]
- Bao, W.; Bowers, K.; Tobias, D.K.; Hu, F.B.; Zhang, C. Prepregnancy dietary protein intake, major dietary protein sources, and the risk of gestational diabetes mellitus: A prospective cohort study. Diabetes Care 2013, 36, 2001–2008. [Google Scholar] [CrossRef]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary patterns during pregnancy are associated with risk of gestational diabetes mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef]
- Hinkle, S.N.; Gleason, J.L.; Yisahak, S.F.; Zhao, S.K.; Mumford, S.L.; Sundaram, R.; Grewal, J.; Grantz, K.L.; Zhang, C. Assessment of Caffeine Consumption and Maternal Cardiometabolic Pregnancy Complications. JAMA Netw. Open 2021, 4, e2133401. [Google Scholar] [CrossRef]
- Kolb, H.; Martin, S.; Kempf, K. Coffee and Lower Risk of Type 2 Diabetes: Arguments for a Causal Relationship. Nutrients 2021, 13, 1144. [Google Scholar] [CrossRef]
- Santos, R.M.M.; Lima, D.R.A. Coffee consumption, obesity and type 2 diabetes: A mini-review. Eur. J. Nutr. 2016, 55, 1345–1358. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, N.; White, H. Systematic review of randomised controlled trials of the effects of caffeine or caffeinated drinks on blood glucose concentrations and insulin sensitivity in people with diabetes mellitus. J. Hum. Nutr. Diet. 2013, 26, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Spafford, C.; Graham, T.E.; Smith, G.N. Acute caffeine ingestion and glucose tolerance in women with or without gestational diabetes mellitus. J. Obstet. Gynaecol. Can. 2009, 31, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Bunker, M.L.; McWilliams, M. Caffeine content of common beverages. J. Am. Diet. Assoc. 1979, 74, 28–32. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Moderate caffeine consumption during pregnancy. Committee Opinion No. 462. Obstet. Gynecol. 2010, 116, 467–468. [Google Scholar] [CrossRef]
- van Woudenbergh, G.J.; Kuijsten, A.; Drogan, D.; van der A, D.L.; Romaguera, D.; Ardanaz, E.; Amiano, P.; Barricarte, A.; Beulens, J.W.J.; Boeing, H.; et al. Tea consumption and incidence of type 2 diabetes in Europe: The EPIC-InterAct case-cohort study. PLoS ONE 2012, 7, e36910. [Google Scholar] [CrossRef]
- Higdon, J.V.; Frei, B. Tea catechins and polyphenols: Health effects, metabolism, and antioxidant functions. Crit. Rev. Food Sci. Nutr. 2003, 43, 89–143. [Google Scholar] [CrossRef]
- Hinkle, S.N.; Laughon, S.K.; Catov, J.M.; Olsen, J.; Bech, B.H. First trimester coffee and tea intake and risk of gestational diabetes mellitus: A study within a national birth cohort. BJOG 2015, 122, 420–428. [Google Scholar] [CrossRef]
- Marshall, N.E.; Abrams, B.; Barbour, L.A.; Catalano, P.; Christian, P.; Friedman, J.E.; Hay, W.W.; Hernandez, T.L.; Krebs, N.F.; Oken, E.; et al. The importance of nutrition in pregnancy and lactation: Lifelong consequences. Am. J. Obstet. Gynecol. 2022, 226, 607–632. [Google Scholar] [CrossRef] [PubMed]
- Fedullo, A.L.; Schiattarella, A.; Morlando, M.; Raguzzini, A.; Toti, E.; De Franciscis, P.; Peluso, I. Mediterranean Diet for the Prevention of Gestational Diabetes in the Covid-19 Era: Implications of Il-6 In Diabesity. Int. J. Mol. Sci. 2021, 22, 1213. [Google Scholar] [CrossRef] [PubMed]
- Assaf-Balut, C.; García De La Torre, N.; Durán, A.; Fuentes, M.; Bordiú, E.; Del Valle, L.; Familiar, C.; Ortolá, A.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef]
- Hernandez, T.L.; Mande, A.; Barbour, L.A. Nutrition therapy within and beyond gestational diabetes. Diabetes Res. Clin. Pract. 2018, 145, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful dietary patterns and type 2 diabetes mellitus risk among women with a history of gestational diabetes mellitus. Arch. Intern. Med. 2012, 172, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Zhang, C.; Chavarro, J.; Bowers, K.; Rich-Edwards, J.; Rosner, B.; Mozaffarian, D.; Hu, F.B. Prepregnancy adherence to dietary patterns and lower risk of gestational diabetes mellitus. Am. J. Clin. Nutr. 2012, 96, 289–295. [Google Scholar] [CrossRef]
- Chatzi, L.; Leventakou, V.; Vafeiadi, M.; Koutra, K.; Roumeliotaki, T.; Chalkiadaki, G.; Karachaliou, M.; Daraki, V.; Kyriklaki, A.; Kampouri, M.; et al. Cohort Profile: The Mother-Child Cohort in Crete, Greece (Rhea Study). Int. J. Epidemiol. 2017, 46, 1392–1393k. [Google Scholar] [CrossRef]
- Tsarna, E.; Reedijk, M.; Birks, L.E.; Guxens, M.; Ballester, F.; Ha, M.; Jiménez-Zabala, A.; Kheifets, L.; Lertxundi, A.; Lim, H.R.; et al. Associations of Maternal Cell-Phone Use During Pregnancy with Pregnancy Duration and Fetal Growth in 4 Birth Cohorts. Am. J. Epidemiol. 2019, 188, 1270–1280. [Google Scholar] [CrossRef]
- Pandolfini, C.; Clavenna, A.; Cartabia, M.; Campi, R.; Bonati, M. National, longitudinal NASCITA birth cohort study to investigate the health of Italian children and potential influencing factors. BMJ Open 2022, 12, e063394. [Google Scholar] [CrossRef]
- Rothman, K.J.; Gallacher, J.E.J.; Hatch, E.E. Why representativeness should be avoided. Int. J. Epidemiol. 2013, 42, 1012. [Google Scholar] [CrossRef]
- Banerjee, A.; Chitnis, U.B.; Jadhav, S.L.; Bhawalkar, J.S.; Chaudhury, S. Hypothesis testing, type I and type II errors. Ind. Psychiatry J. 2009, 18, 127. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| All Study Participants | Number of Study Participants with Missing Data | Study Participants without GDM | Study Participants with GDM | |||
|---|---|---|---|---|---|---|
| Mean (SD)/N (%) | N (%) | Mean (SD)/N (%) | Mean (SD)/N (%) | p-Value 1 | ||
| Maternal age (mean (SD)) | 31.53 (4.43) | 0 (0.0%) | 31.45 (4.43) | 32.75 (4.54) | 0.39 | |
| Pre-gestational BMI (mean (SD)) | 22.81 (3.75) | 0 (0.0%) | 22.70 (3.63) | 24.39 (5.08) | 0.20 | |
| Gestational weight gain (mean (SD)) | 13.46 (6.94) | 0 (0.0%) | 13.69 (6.63) | 10.00 (10.32) | <0.01 | |
| Weight gain below IOM target range n (%) | 61 (31.6%) | 0 (0.0%) | 54 (29.8%) | 7 (58.3%) | 0.08 | |
| Weight gain within IOM target range n (%) | 65 (33.7%) | 0 (0.0%) | 61 (33.7%) | 4 (33.3%) | 1.00 | |
| Weight gain above IOM target range n (%) | 67 (34.7%) | 0 (0.0%) | 66 (36.5%) | 1 (8.3%) | 0.10 | |
| Gravidity status n (%) | 0 | 124 (64.2%) | 0 (0.0%) | 114 (63.0%) | 10 (83.3%) | 0.03 |
| 1 | 43 (22.3%) | 43 (23.8%) | 0 (0.0%) | |||
| 2 | 18 (9.3%) | 17 (9.4%) | 1 (8.3%) | |||
| 3 | 6 (3.1%) | 6 (3.3%) | 0 (0.0%) | |||
| 4 | 2 (1.0%) | 1 (0.6%) | 1 (8.3%) | |||
| Parity status n (%) | 0 | 143 (74.1%) | 0 (0.0%) | 133 (73.5%) | 10 (83.3%) | 0.22 |
| 1 | 45 (23.3%) | 44 (24.3%) | 1 (8.3%) | |||
| 2 | 5 (2.6%) | 4 (2.2%) | 1 (8.3%) | |||
| Number of prior vaginal births n (%) | 0 | 155 (80.3%) | 0 (0.0%) | 145 (80.1%) | 10 (83.3%) | 0.21 |
| 1 | 34 (17.6%) | 33 (18.2%) | 1 (8.3%) | |||
| 2 | 4 (2.1%) | 3 (1.7%) | 1 (8.3%) | |||
| Number of prior caesarian sections n (%) | 0 | 174 (90.2%) | 0 (0.0%) | 162 (89.5%) | 12 (100.0%) | 0.50 |
| 1 | 19 (9.8%) | 19 (10.5%) | 0 (0.0%) | |||
| Smoking before pregnancy n (%) | No | 108 (56.0%) | 0 (0.0%) | 103 (56.9%) | 5 (41.7%) | 0.47 |
| Yes | 85 (44.0%) | 78 (43.1%) | 7 (58.3%) | |||
| Smoking during pregnancy n (%) | No | 170 (88.1%) | 0 (0.0%) | 158 (87.3%) | 12 (100.0%) | 0.39 |
| Yes | 23 (11.9%) | 23 (12.7%) | 0 (0.0%) | |||
| Passive smoking at home during pregnancy n (%) | No | 105 (54.4%) | 0 (0.0%) | 97 (53.6%) | 8 (66.7%) | 0.56 |
| Yes | 88 (45.6%) | 84 (46.4%) | 4 (33.3%) | |||
| Gestational diabetes mellitus n (%) | 12 (6.2%) | 0 (0.0%) | 0 (0.0%) | 12 (100.0%) | NA | |
| Pregnancy-induced hypertension n (%) | 7 (3.6%) | 0 (0.0%) | 5 (2.8%) | 2 (16.7%) | 0.09 | |
| Gestational age at birth (mean (SD)) | 38.53 (1.38) | 0 (0.0%) | 38.54 (1.40) | 38.42 (1.16) | 0.56 | |
| Birthweight in gr (mean (SD)) | 3075.12 (499.66) | 26 (13.5%) | 3060.73 (500.51) | 3327.78 (433.84) | 0.12 | |
| Neonate’s sex n (%) | Female | 88 (52.4%) | 25 (13.0%) | 82 (51.6%) | 6 (66.7%) | 0.59 |
| Male | 80 (47.6%) | 77 (48.4%) | 3 (33.3%) | |||
| Sample Size | 193 | 181 | 12 | |||
| Crude p-Value | Adjusted p-Value | |
|---|---|---|
| Carbohydrate-rich meal consumption frequency | 0.22 | 0.26 |
| Fruit and vegetable consumption frequency | 0.07 | 0.04 |
| Sweet consumption frequency | 0.21 | 0.33 |
| Soft drink consumption frequency | 0.67 | 0.75 |
| Coffee consumption frequency | 0.43 | 0.33 |
| Crude Analysis | Adjusted Analysis | |||
|---|---|---|---|---|
| Odds Ratio (OR) | p-Value | Odds Ratio (OR) | p-Value | |
| Frequent consumption of cereals | 0.30 | 0.045 | 0.35 | 0.095 |
| Frequent consumption of rice | 0.60 | 0.39 | 0.70 | 0.57 |
| Frequent consumption of pasta | 0.64 | 0.53 | 0.66 | 0.56 |
| Frequent consumption of bread and crackers | 1.52 | 0.54 | 1.55 | 0.53 |
| Frequent consumption of potatoes | 1.24 | 0.75 | 1.30 | 0.71 |
| Frequent consumption of lentils | 2.48 | 0.25 | 2.50 | 0.25 |
| Frequent consumption of tea | 3.09 | 0.067 | 3.97 | 0.035 |
| Frequent consumption of juices | 0.50 | 0.26 | 0.56 | 0.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsarna, E.; Eleftheriades, A.; Tsomi, E.; Ziogou, G.; Vakas, P.; Panoskaltsis, T.; Christopoulos, P. The Role of Diet during Pregnancy in Protecting against Gestational Diabetes Mellitus in a Population with Mediterranean Dietary Habits: A Cross-Sectional Study. J. Clin. Med. 2023, 12, 1857. https://doi.org/10.3390/jcm12051857
Tsarna E, Eleftheriades A, Tsomi E, Ziogou G, Vakas P, Panoskaltsis T, Christopoulos P. The Role of Diet during Pregnancy in Protecting against Gestational Diabetes Mellitus in a Population with Mediterranean Dietary Habits: A Cross-Sectional Study. Journal of Clinical Medicine. 2023; 12(5):1857. https://doi.org/10.3390/jcm12051857
Chicago/Turabian StyleTsarna, Ermioni, Anna Eleftheriades, Efthymia Tsomi, Georgia Ziogou, Panagiotis Vakas, Theodoros Panoskaltsis, and Panagiotis Christopoulos. 2023. "The Role of Diet during Pregnancy in Protecting against Gestational Diabetes Mellitus in a Population with Mediterranean Dietary Habits: A Cross-Sectional Study" Journal of Clinical Medicine 12, no. 5: 1857. https://doi.org/10.3390/jcm12051857
APA StyleTsarna, E., Eleftheriades, A., Tsomi, E., Ziogou, G., Vakas, P., Panoskaltsis, T., & Christopoulos, P. (2023). The Role of Diet during Pregnancy in Protecting against Gestational Diabetes Mellitus in a Population with Mediterranean Dietary Habits: A Cross-Sectional Study. Journal of Clinical Medicine, 12(5), 1857. https://doi.org/10.3390/jcm12051857