Abstract
Background: Chronic hepatitis B (CHB) and non-alcoholic fatty liver disease (NAFLD) are significant causes of chronic liver disease, potentially leading to liver cirrhosis and hepatocellular carcinoma. Moreover, the coexistence of CHB and NAFLD is increasingly common, although the relationship between NAFLD and inactive CHB infection remains poorly understood. Objectives: This study aimed to investigate the prevalence of NAFLD among patients with inactive CHB, identify risk factors for NAFLD, and determine predictors of significant fibrosis in these patients. Methods: This single-center cross-sectional study targeted patients with inactive CHB at Sultan Qaboos University Hospital from January 2010 to November 2021. Results: A total of 425 patients with inactive CHB were identified, of which 53.1% were male and 62.6% were aged 40–60 years. The prevalence of NAFLD was 47.8%. Various independent factors were associated with NAFLD, including type 2 diabetes mellitus, elevated low-density lipoprotein levels, high hemoglobin levels, low platelet counts, and normal alpha-fetoprotein levels. Significant associations were noted between NAFLD and significant fibrosis, with 10.5% of CHB patients with NAFLD exhibiting significant fibrosis compared to 1.4% of those without NAFLD. Other significant parameters included male gender, increased age, high alanine transaminase levels, elevated hemoglobin, and decreased platelet levels. Conclusions: The high prevalence of NAFLD in patients with inactive CHB and its associations with increased fibrosis and cirrhosis risk underscore the need for comprehensive management strategies for these patients.
1. Introduction
Chronic hepatitis B (CHB) infection is a global health concern, affecting an estimated 257.5 million people worldwide [1]. In Oman, the prevalence of CHB carriers is approximately 2.5% [2]. Inactive CHB infection, also termed hepatitis B e-antigen (HBeAg)-negative CHB infection, is diagnosed based on specific criteria: the presence of HBeAg antibodies (anti-HBeAg), undetectable or low hepatitis B virus (HBV) DNA levels, and normal alanine transaminase (ALT) levels [3]. Non-alcoholic fatty liver disease (NAFLD) is another rising liver concern globally [4]. Among Asian individuals with CHB, the prevalence of NAFLD ranges from 14% to 67%, similar to the rates in Western countries [5,6]. In Oman, the prevalence of NAFLD increased from 8.9% in 1990 to 19.5% in 2017, with an estimated annual rise of 2.12% [7]. Another study in Oman reported an even higher prevalence of 67.3% [8].
Over the past few decades, the obesity epidemic has led to NAFLD becoming one of the most significant chronic liver diseases both regionally and globally, particularly given its association with insulin resistance [9,10,11]. Indeed, experts have proposed replacing the term with metabolic dysfunction-associated fatty liver disease (MASLD) to better reflect the metabolic underpinnings of the disease [12]. Unlike NAFLD, which necessitates the exclusion of other causes of liver disease, a diagnosis of MASLD requires evidence of steatosis and at least one metabolic risk factor like obesity or insulin resistance [12]. This new terminology has already been adopted in the latest guidelines from the American Association of the Study of Liver Disease [13].
Various imaging techniques can be used to diagnose NAFLD, such as ultrasonography, computed tomography, and magnetic resonance imaging, while transient elastography can be utilized to assess hepatic fibrosis. Liver biopsy remains an option when other diagnostic methods are inconclusive [14]. While most individuals with NAFLD have no inflammation, those with both fat and inflammation in the liver―a condition known as non-alcoholic steatohepatitis (NASH)―face an increased risk of fibrosis and cirrhosis [14]. As the prevalence of NAFLD rises, so does its cooccurrence with inactive CHB infection [15,16]. While the detrimental effects of active CHB on the liver are well understood, the potential interaction between NAFLD and inactive CHB warrants further investigation. The relationship between these conditions remains unclear, with some research suggesting their coexistence may worsen liver damage and increase the risk of cirrhosis and fibrosis [17].
The current study, the first of its kind in the region, aimed to determine the prevalence of NAFLD among patients with inactive CHB, identify associated risk factors, and determine predictors of significant fibrosis. Understanding local disease patterns is crucial, particularly considering the rising obesity rates that predispose individuals to NAFLD, which can lead to liver cirrhosis and complications such as hepatocellular carcinoma (HCC) and the need for liver transplantation. Examining the interaction between NAFLD and inactive CHB can influence patient management, treatment strategies, and liver disease prognosis. This knowledge has the potential to improve patient outcomes, tailor treatment approaches, and optimize healthcare resource allocation.
2. Materials and Methods
This single-center, cross-sectional study enrolled adult patients diagnosed with inactive CHB between January 2010 and November 2021. All participants received regular follow-up care at the Sultan Qaboos University Hospital (SQUH), a tertiary hospital in Muscat, Oman. The inclusion criteria encompassed all adult individuals diagnosed with inactive CHB according to the guidelines of the European Association for the Study of the Liver (EASL) [3]. These criteria included serum anti-HBeAg positivity, undetectable or low levels of HBV DNA (<2000 IU/mL) by polymerase chain reaction testing, and normal ALT levels based on the standard cut-off values. Additionally, the study included some patients diagnosed with inactive CHB who had HBV DNA levels >2000 IU/mL (usually <20,000 IU/mL) accompanied by persistently normal ALT and low fibrosis, according to the EASL guidelines [3]. Participants with missing essential data, such as laboratory or imaging results, were excluded from the study.
The necessary sample size was estimated based on the anticipated prevalence of NAFLD among patients with inactive CHB, aiming for an absolute precision of 5% and a 95% confidence level, resulting in a required sample size of 334. Ultimately, a total of 425 patients with inactive CHB were included in the study. These patients were categorized into case or control groups based on the presence or absence of NAFLD. Ultrasound findings were used to diagnose NAFLD according to the EASL criteria, with evidence of steatosis by imaging or histology after the exclusion of secondary causes, such as increased alcohol intake, viral hepatitis, or steroid use [18].
The relevant data were extracted from the patients’ electronic medical records using the hospital information system at SQUH (TrakCare, InterSystems Corp., Cambridge, MA, USA). Baseline data included demographic characteristics such as age, gender, weight, height, and body mass index (BMI), as well as any medical history of hypertension (HTN), type 2 diabetes mellitus (T2DM), dyslipidemia, or metabolic syndrome (MetS). The latter condition was defined as the presence of any three of the following criteria: central or visceral obesity (waist circumference of ≥102 cm or ≥40 inches in males and ≥88 cm or ≥35 inches in females), elevated triglycerides (≥150 mg/dL or ≥1.7 mmol/L or specific treatment), reduced high-density lipoprotein cholesterol levels (<1.04 mmol/L or <40 mg/dL in males and <1.29 mmol/L or <50 mg/dL in females or specific treatment), elevated blood pressure (BP)(systolic BP of ≥130 mmHg or diastolic BP of ≥85 mmHg or specific treatment for HTN), and elevated fasting plasma glucose (≥5.6 mmol/L or ≥100 mg/dL or previously diagnosed T2DM) [19,20].
Laboratory data included the hepatitis B surface antigen, HBeAg, anti-hepatitis B e-antigen, hepatitis B surface antibody, hepatitis B core antibody, HBV viral load, alpha-fetoprotein (AFP), gamma-glutamyl transferase, alkaline phosphatase, ALT, aspartate aminotransferase (AST), hemoglobin (Hb), platelet (PLT) count, high-density lipoprotein (HDL), total cholesterol, triglycerides, low-density lipoprotein (LDL), and glycated Hb levels. Systolic and diastolic BP readings were also documented. Liver ultrasonography with simultaneous two-dimensional shear wave elastography was performed using the GE LOGIQ E9 XDclear 2.0 ultrasound machine (GE Healthcare, Milwaukee, WI, USA) every six months as part of the routine HCC screening. The ultrasound findings were used to assess for NAFLD and any signs of cirrhosis. The Fibrosis-4 (FIB-4) index, a validated, non-invasive scoring system based on laboratory tests, was used to estimate the degree of liver fibrosis, aiding in the decision of whether a liver biopsy was necessary [21]. FIB-4 index scores were calculated using the MDCalc (MDCalc Calculator. Retrieved from https://www.mdcalc.com/calc/2200/fibrosis-4-fib-4-index-liver-fibrosis (accessed on 26 June 2023)).
Collected data were analyzed using the Statistical Package for the Social Sciences (SPSS) software, version 26 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as percentages and frequencies, while continuous variables were reported as either means with standard deviations or medians with interquartile ranges, as appropriate. Prevalence was expressed as a proportion with a 95% confidence interval (CI). Crude associations were evaluated using odds ratio (OR), a chi-squared test, and a Mann–Whitney U test. Multivariate analysis was conducted using logistic binary regression, including variables from the initial analysis with a p-value < 0.20. To address potential multicollinearity issues, the Variance Inflation Factor (VIF) was calculated for each predictor variable. Variables with a VIF greater than 10 were considered to exhibit multicollinearity and were excluded from the final model. The level of statistical significance was set at p < 0.05.
This study received ethical approval from the institutional Medical Research and Ethics Committee of the College of Medicine and Health Sciences at Sultan Qaboos University. All study procedures were conducted in accordance with the principles of the revised Helsinki Declaration.
3. Results
Of the 425 patients with inactive CHB infection enrolled in the study, the majority were male (53.1%) and 40–60 years old (62.6%). The mean BMI was 29.14 ± 6.32 kg/m2, with 75.6% classified as overweight or obese. In terms of comorbidities, MetS was present in 14.6% of participants, while 14.6% and 12.5% had T2DM and HTN, respectively. Dyslipidemia was documented in 16.9% of cases. Detectable HBV DNA levels exceeding 2000 IU/mL were found in 5.6% of patients, while elevated AFP levels were noted in 14.5%. Liver enzymes were mildly elevated, with 6.9% and 3.1% of patients showing increased ALT and AST levels, respectively. Additional baseline characteristics of the study population are summarized in Table 1.

Table 1.
General characteristics of the study sample.
The prevalence of NAFLD was 47.8% (95% CI: 43.1–52.5%). Overall, the prevalence of NAFLD was higher in male patients (55.6%, 95% CI: 49.1–62.1%) compared to female patients (39.2%, 95% CI: 32.4–46.0%). Moreover, a higher prevalence was noted among older patients. Interestingly, the prevalence of NAFLD was similar between patients with and without MetS. Table 2 presents a detailed comparison of NAFLD prevalence according to gender, age, and MetS status.
Table 2.
Prevalence of NAFLD according to the subgroup.
Various factors were found to be associated with NAFLD, as shown in Table 3. Gender was significantly correlated (p < 0.001), with female patients being 0.52 times less likely to develop NAFLD than males (95% CI: 0.35–0.76). Additionally, significant associations were observed between NAFLD and both LDL levels (OR: 6.187, 95% CI: 3.22–11.90; p < 0.001) and HBV DNA levels (OR: 0.223, 95% CI: 0.082–0.609; p = 0.002). Figure 1a–c display the frequency of NAFLD according to gender, LDL, and HBV DNA groups.
Table 3.
Associations between NAFLD and various factors.
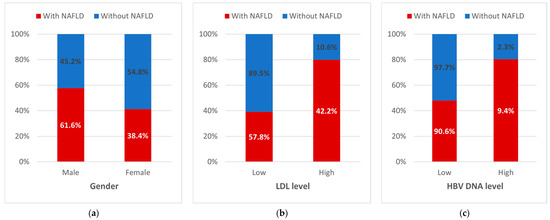
Figure 1.
Distribution of NAFLD cases by (a) gender, (b) LDL level, and (c) HBV DNA level. HBV: hepatitis B virus; LDL: low-density lipoprotein; NAFLD: non-alcoholic fatty liver disease.
Furthermore, patients with high ALT levels were significantly more likely to have NAFLD (OR: 10.846, 95% CI: 3.229–36.425) compared to those with normal levels. Conversely, high levels of AFP significantly reduced the likelihood of NAFLD (OR: 0.277, 95% CI: 0.148–0.521; p < 0.001). Significant correlations were also found between NAFLD and both the Hb level and PLT count (p < 0.001 each). However, in the multivariate regression analysis, only T2DM, high LDL levels, normal AFP levels, elevated Hb levels, and lower PLT counts remained independent predictors of NAFLD. Specifically, the likelihood of NAFLD was 2.606 times higher for patients with T2DM (95% CI: 1.091–6.225) and 4.204 times higher for patients with elevated LDL levels (95% CI: 1.936–9.126). Table 4 details the results of the multivariate analysis.
Table 4.
Multivariate analysis showing the relationships between NAFLD and various parameters (n = 279).
As per their FIB-4 index scores, most patients (94.3%) were classified as unlikely to have significant fibrosis (score < 1.3; 95% CI: 92.1–9 6.5%). A smaller proportion (4.7%) had scores indicating possible fibrosis (score 1.3–2.67; 95% CI: 2.7–6.7%), while only 0.9% were classified as having advanced fibrosis (score > 2.67; 95% CI: 0–1.8%). The overall prevalence of significant fibrosis, indicated by a FIB-4 index score greater than 1.3, was 5.7% (95% CI: 3.5–7.9%), with cirrhosis observed in 3.3% of cases (95% CI: 1.6–5.0%). The preliminary analysis revealed a significant association between NAFLD and significant fibrosis, with 10.5% of the NAFLD group exhibiting significant fibrosis compared to only 1.4% of patients without NAFLD (OR: 8.564, 95% CI: 2.51–29.18; p < 0.001). Moreover, there was a strong association between NAFLD and cirrhosis, with NAFLD patients being 15.15 times more likely to have cirrhosis (95% CI: 1.96–116.66; p = 0.001).
Table 5 outlines the associations between various factors and the fibrosis status based on the patients’ FIB-4 index scores. Gender showed a significant correlation with fibrosis, with female patients being less likely to develop significant fibrosis (OR: 0.356, 95% CI: 0.138–0.915) compared to males. High ALT levels also demonstrated a significant association with fibrosis (OR: 5.44; 95% CI: 1.97–15.00). Additionally, increased age, elevated Hb levels, and decreased PLT counts were significantly associated with fibrosis status.
Table 5.
Associations between fibrosis status and various factors.
4. Discussion
Chronic liver diseases like CHB and NAFLD carry considerable risks, potentially leading to life-threatening consequences such as liver cirrhosis and HCC [22,23]. In particular, NAFLD has emerged as the most prevalent chronic liver disease globally [10]. Despite the increasingly common coexistence of CHB and NAFLD [17], the relationship between NAFLD and inactive CHB infection remains poorly understood. This study aimed to investigate the prevalence of NAFLD in patients with inactive CHB, its associated risk factors, and predictors of fibrosis in this population.
In our study, 53.1% of participants were male. This is consistent with other studies, including those involving long-term vaccinated individuals, which have similarly reported higher rates of CHB infection in males compared to females [24,25]. This gender disparity is largely attributed to the influence of sex hormones. Testosterone can suppress certain immune responses, potentially hindering the effective control of HBV, whereas estrogen is known to have a protective effect against the virus [26]. Furthermore, men may engage more frequently in high-risk behaviors, such as intravenous drug use and sexual relations with multiple partners, thereby increasing their likelihood of HBV exposure [27].
In terms of age distribution, the majority (62.6%) of CHB patients in our study were between 40 and 60 years old. This demographic pattern can be attributed to the widespread availability of the HBV vaccine in Oman. Starting in August 1990, the vaccine was recommended for newborns, followed by school-based campaigns targeting adolescents aged 11–18 years from 2000 to 2005 (i.e., the 1982–1990 birth cohorts) [28]. Despite these efforts, achieving full vaccination coverage across the population took time, potentially leaving some individuals susceptible to infection. Furthermore, infection rates remained elevated among individuals born before the introduction of the vaccine but within the catch-up campaign period. This is partly due to many individuals in this group receiving the vaccine without prior screening for HBV infection [28]. The prolonged duration of the catch-up campaigns could also have contributed to increased infection risk among unvaccinated children exposed to infected family members.
Our study also indicated that 75.6% of patients with inactive CHB infection were overweight or obese, a finding of significant concern amid the global rise in obesity [29]. In 2021, over half of the Omani population was overweight or obese, with 30% having a BMI over 30 kg/m2 [30]. Various factors, such as lifestyle changes, sedentary behavior, urbanization, and socioeconomic status, contribute to these high rates [30,31]. This trend is particularly concerning among CHB patients, as obesity may exacerbate metabolic comorbidities and liver disease progression [32,33]. This may stem from several factors, including reduced physical activity and metabolic disturbances associated with liver disease [33]. While a direct link between CHB and obesity remains unclear, the presence of obesity in CHB patients reflects broader societal trends influenced by factors like poor diet and physical inactivity [32]. Although CHB itself does not cause obesity, its interaction with obesity can significantly impact liver disease outcomes [32,33,34,35].
In our study, MetS was present in 14.6% of participants overall, with a similar prevalence (14.8%) among those with NAFLD. Factors such as ethnicity, age, gender, lifestyle, and other population characteristics influence the prevalence of MetS in CHB patients. In Oman, the MetS prevalence ranges widely from 21% in healthy adults to 45.9% in prediabetic populations [36,37,38]. While the MetS rate in our study was lower than that of the general population, international studies suggest that individuals with CHB may face a higher risk of MetS [39,40]. Nonetheless, the precise relationship between MetS and CHB infection remains complex and inconclusive [41]. Some studies suggest a potential link, while others do not find a significant association [42,43]. Evidence indicates that HBV might influence metabolic profiles and MetS development, although the findings vary [39]. In HBV patients, those with MetS often exhibit higher viral loads, with high and low extremes of cholesterol levels correlating with higher HBV DNA levels, indicating a potential interaction with lipid metabolism [44]. Moreover, CHB infection can lead to various liver diseases, indirectly impacting metabolic health [45]. Conversely, a large Taiwanese study reported an inverse association between CHB infection and MetS development, even after adjusting for the BMI, suggesting unique metabolic influences compared to other liver diseases [35]. Thus, while some evidence suggests an interaction between HBV and metabolic factors, the association with MetS remains uncertain.
In addition, 14.6% of our patients were affected by T2DM, which is lower than the 20.4% prevalence observed among HBV-infected patients in Egypt [46]. In Oman, the prevalence of diabetes varies, with age-adjusted rates ranging from 10.4% to 21.1% [47]. The International Diabetes Federation reported an 11.8% prevalence of T2DM among adults in Oman in 2021, below that found in the HBV population [48]. In contrast, a large, community-based study from 2017 showed an overall T2DM prevalence of 15.7%, with prediabetes at 11.8% [49]. Additionally, 35.1% of Omani men have been reported to have impaired fasting glucose, a precursor to T2DM [47]. The relationship between CHB infection and T2DM is complex. A meta-analysis by Cai et al. indicated that HBV-infected patients have a higher risk of developing T2DM compared to non-HBV-infected patients, although the researchers did not differentiate the stages of HBV infection [50]. Chronic inflammation caused by HBV infection may contribute to insulin resistance and impaired glucose metabolism, key factors in T2DM development [51]. This relationship is influenced by age, ethnicity, duration of HBV infection, and other risk factors like obesity or a family history of T2DM [52].
Overall, the prevalence of NAFLD in our study was 47.8%, aligning with rates reported in studies of CHB patients from Iran and Malaysia (46.8% and 47.9%, respectively) [53,54]. The high prevalence of obesity and elevated BMI in the general Omani population likely contribute to this high prevalence of NAFLD among individuals with inactive CHB infection [31]. However, the occurrence of NAFLD in our population was still lower than that of the general Omani population (67.3%) [8]. This finding supports the literature suggesting that CHB patients have a lower prevalence of NAFLD due to the virus impairing fat formation in the liver [55]. We also identified several factors associated with the development of NAFLD in our univariate analysis, including male gender, high LDL levels, high HBV DNA levels, normal AFP levels, high ALT levels, high Hb levels, and low PLT counts. However, in the multivariate analysis, only T2DM, high LDL levels, high Hb levels, decreased PLT counts, and normal AFP levels remained independent factors associated with NAFLD.
Our study showed that male gender was not an independent risk factor for NAFLD. This finding contrasts with other studies that have identified male gender as significantly associated with liver steatosis among both CHB and non-CHB patients [56,57,58,59]. Two systematic reviews and meta-analyses corroborate that the male gender is a strong risk factor for hepatic steatosis in CHB patients, consistent with the general population [56,57]. Moreover, the prevalence of NAFLD tends to be higher in males, regardless of the presence of inactive CHB infection [60]. This may be attributed to the protective effect of estrogen against hepatic steatosis or fat accumulation in the liver [61].
However, we identified significant relationships between NAFLD and both high LDL levels and T2DM, aligning with previous studies [40,45,48,62]. This is due to the underlying pathogenesis, insulin resistance, which contributes to both NAFLD and T2DM [63,64,65]. Additionally, the LDL receptor, implicated in HBV infection, presumably acts as a viral attachment receptor, thereby altering the LDL levels in inactive CHB [66]. Moreover, HBV may modify hepatic cholesterol metabolism by increasing LDL receptor expression and 3-hydroxy-3-methylglutaryl-coenzyme A reductase via the pre-S1 domain of the viral envelope [67,68]. Given that low HDL cholesterol levels predict poor outcomes in patients with HBV-related liver failure and decompensated cirrhosis [69,70], these findings emphasize the relevance of monitoring lipid values in individuals with inactive CHB.
We also observed independent associations between NAFLD and both low PLT counts and high Hb levels. The etiology of a low PLT count in NAFLD remains unclear, with the proposed factors including hypersplenism, bone marrow hypoplasia, decreased peripheral blood cell survival, and thrombopoietin insufficiency [71,72,73,74]. High Hb levels in CHB patients, as observed in other studies [75,76,77,78], may be due to chronic inflammation, insulin resistance, and hypoxia-induced erythropoietin production. Coexisting conditions such as obesity and MetS may also contribute to elevated Hb levels [79]. Our research also showed a crude association between high ALT levels and NAFLD, although this did not hold in the multivariate analysis. Indeed, ALT, a surrogate marker for liver inflammation, is typically normal in mild cases of NAFLD and inactive CHB [80,81]. Elevated ALT levels indicate the need for further assessment of the hepatitis activity or the progression of NAFLD to more severe forms, such as NASH or liver fibrosis [82]. These results suggest that ALT may act as a cofactor, rather than an independent factor, for NAFLD.
Intriguingly, we observed that patients with inactive CHB and normal AFP levels exhibited a higher prevalence of NAFLD compared to those with high AFP levels. This finding offers a novel perspective on the relationship between AFP levels and NAFLD in patients with inactive CHB, contrary to the prevailing understanding linking elevated AFP levels with hepatic steatosis development [83,84,85,86,87]. For instance, Xu et al. suggested that AFP may act as a cofactor in NAFLD development, albeit not an independent factor [83]. Other researchers have reported a correlation between serum AFP levels and NAFLD grade, with higher AFP levels potentially indicating more severe NAFLD, even though liver enzymes ALT and AST do not show such correlations [86]. Additionally, elevated AFP levels have been associated with the histopathological findings in NAFLD patients, suggesting a potential link between AFP levels and liver pathology [85]. However, our study presents an interesting deviation from these established patterns.
This discrepancy suggests that the mechanisms underlying NAFLD in the context of inactive CHB might differ from those in other hepatic conditions. Several hypotheses could explain our findings. In inactive CHB, normal AFP levels may indicate a less aggressive disease state, allowing for the development of NAFLD without the concurrent increase in AFP typically seen in more active or advanced liver disease. Alternatively, the metabolic profile of patients with inactive CHB might differ in ways that influence both AFP production and lipid metabolism, leading to this unique association. Our findings underscore the need for further research to elucidate the pathophysiological mechanisms linking the AFP levels and NAFLD in inactive CHB. Understanding these interactions could have significant implications for patient management, potentially guiding more tailored and effective treatment strategies. Given the mixed findings in the literature regarding AFP and NAFLD, our study contributes to a more nuanced understanding of liver disease progression in specific patient populations, highlighting the importance of context in interpreting biomarker data.
In our study, substantial links were found between NAFLD and fibrosis or cirrhosis, particularly in patients with inactive CHB, with an increased risk in NASH patients [88,89,90]. The joint existence of NAFLD and CHB accelerates disease progression due to metabolic abnormalities, oxidative stress, and chronic inflammation. Variable fibrosis prevalence exists based on disease severity, individual characteristics, and additional risk factors. The major determinants identified include gender, age, ALT and Hb levels, and PLT counts, with women, especially premenopausal, presenting lower fibrosis risks, potentially due to sex hormone influence [91,92,93,94,95,96,97]. A heightened risk exists for postmenopausal women. Age is another significant contributor, with susceptibility increasing due to prolonged virus exposure [98,99]. Elevated ALT and Hb levels were found to connect to escalated liver inflammation and possible red blood cell turnover and systemic inflammation, linking to fibrosis [100,101,102,103,104,105].
High ALT levels were also significantly associated with fibrosis in our study, consistent with the literature findings that link ALT with increased hepatic inflammation and fibrosis [100]. Studies across various populations have shown that patients with elevated ALT levels have significantly higher odds of fibrosis, reinforcing the utilization of ALT measurements as a reliable marker for liver fibrosis in CHB patients [101,102]. Elevated Hb levels have also been associated with higher fibrosis stages, suggesting a potential link between increased red blood cell turnover and liver fibrosis, although studies confirming this association are scarce [103,104]. Potential mechanisms by which elevated Hb levels might contribute to liver fibrosis include increased red blood cell turnover and the resultant heme oxygenase activity, leading to the production of profibrotic cytokines and growth factors. Elevated Hb might also reflect the underlying systemic inflammation and oxidative stress, which contribute to fibrosis progression [103]. However, studies on NAFLD patients have reported conflicting results regarding this association [75,105].
Finally, we found decreased PLT counts to be significantly associated with fibrosis in our population. Thrombocytopenia, defined as a PLT count of less than 150 × 103 per µL, is frequently seen in advanced liver disease and can indicate portal hypertension and splenic sequestration, both common in liver fibrosis. The pathophysiology behind this association involves the role of PLTs in liver regeneration and repair. Yang et al. showed that the PLT count could predict significant liver fibrosis in patients with CHB infection [106]. Huang et al. also confirmed that a decreased peripheral PLT count is associated with liver fibrosis in both chronic hepatitis B and C patients, highlighting the commonality of this marker across different hepatitis infections [107]. A comprehensive review by Parikh et al. emphasized the importance of the PLT count as a non-invasive marker for assessing liver fibrosis in CHB patients, thereby aiding in the early detection and management of fibrosis, potentially improving patient outcomes [108]. Overall, the consistent association between thrombocytopenia and liver fibrosis underscores the importance of monitoring PLT counts in CHB patients to effectively assess and manage the fibrosis risk.
Our study has several limitations that should be considered when interpreting the results. Firstly, the cross-sectional design precludes the establishment of causality between NAFLD and fibrosis in patients with inactive CHB. Longitudinal studies are needed to confirm these findings and understand the temporal relationship between these conditions. Secondly, our study was conducted at a single center, which may limit the generalizability of the results to other populations. The sample population was primarily drawn from patients attending SQUH, and regional variations in disease prevalence and risk factors may not be fully captured. Thirdly, the reliance on non-invasive methods for diagnosing NAFLD and fibrosis, such as ultrasonography and FIB-4 score, may introduce measurement biases compared to histological confirmation via liver biopsy. Lastly, potential confounding factors, such as lifestyle habits and detailed metabolic profiles, were not comprehensively assessed, which could influence the observed associations. Future research should address these limitations by incorporating multicenter cohorts, prospective designs, and comprehensive data collection to enhance our understanding of the interplay between NAFLD and CHB infection.
5. Conclusions
Our study highlights the significant impact of NAFLD on the risk of fibrosis among inactive CHB patients. The high prevalence of NAFLD in this population and its association with increased fibrosis and cirrhosis risk underscore the need for comprehensive management strategies that address both conditions concurrently. Moreover, we identified several key factors independently associated with NAFLD, including T2DM, high LDL and Hb levels, low PLT counts, and normal AFP levels. In turn, significant fibrosis was associated with male gender, increasing age, and high ALT levels. These findings emphasize the importance of closely monitoring and managing metabolic factors and liver health in patients with inactive CHB to prevent disease progression. Future studies should examine how the MASLD criteria, including the presence of metabolic risk factors, refine our understanding of the link between inactive CHB and liver disease progression. This revised terminology reflects the growing recognition of the metabolic underpinnings of this condition, potentially offering a more nuanced understanding of how liver disease develops in patients with inactive CHB.
Author Contributions
Conceptualization, S.A.A.-B.; methodology, S.A.A.-B., A.S.A.B. and H.H.A.S.; validation, S.A.A.-B., A.S.A.B. and H.H.A.S.; formal analysis, S.A.A.-B., A.S.A.B., H.H.A.S. and A.M.A.A.; investigation, S.A.A.-B.; A.S.A.B., H.H.A.S. and D.A.M.; resources, S.A.A.-B.; data curation, A.S.A.B. and D.A.M.; writing—original draft preparation, A.S.A.B. and H.H.A.S.; writing—review and editing, S.A.A.-B., A.S.A.B., H.H.A.S. and A.M.A.A.; visualization, S.A.A.-B.; supervision, S.A.A.-B.; project administration, S.A.A.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Research and Ethics Committee of the College of Medicine and Health Sciences, Sultan Qaboos University in March 2022 (protocol code: MREC#691).
Informed Consent Statement
Patient consent was waived, because the study did not involve the collection of identifying information.
Data Availability Statement
Data supporting the reported results are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Polaris Observatory Collaborators. Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: A modelling study. Lancet Gastroenterol. Hepatol. 2023, 8, 879–907. [Google Scholar] [CrossRef] [PubMed]
- Al Awaidy, S.T.; Al Naamani, K.; Sathyanarayana, G.; AlKalban, A.; Kamath, B.R.; Al Sinani, S.; Said, E.; Omer, H.; Al Mehrzi, A.; Mahomed, O. Epidemiological characteristics of hepatitis B positive patients in Oman between 2009 and 2019: A retrospective cohort study. Acad. J. Gastroenterol. Hepatol. 2021, 3, 2021. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef] [PubMed]
- Farrell, G.C.; Wong, V.W.; Chitturi, S. NAFLD in Asia-as common and important as in the West. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.G.; Kim, S.U.; Wong, V.W. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef]
- Ge, X.; Zheng, L.; Wang, M.; Du, Y.; Jiang, J. Prevalence trends in non-alcoholic fatty liver disease at the global, regional and national levels, 1990-2017: A population-based observational study. BMJ Open 2020, 10, e036663. [Google Scholar] [CrossRef] [PubMed]
- Al Mutori, H.; Al Rudaini, M.; Omar, A.F.; Anwar, S.; Selim, Y.; Yaseen, B. Nonalcoholic fatty liver disease among obese patients in Oman. Revis. Bionatura 2022, 7, 42. [Google Scholar] [CrossRef]
- Alswat, K.; Aljumah, A.A.; Sanai, F.M.; Abaalkhail, F.; Alghamdi, M.; Al Hamoudi, W.K.; Al Khathlan, A.; Al Quraishi, H.; Al Rifai, A.; Al Zaabi, M.; et al. Nonalcoholic fatty liver disease burden—Saudi Arabia and United Arab Emirates, 2017–2030. Saudi J. Gastroenterol. 2018, 24, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Sangro, P.; de la Torre Aláez, M.; Sangro, B.; D’Avola, D. Metabolic dysfunction-associated fatty liver disease (MAFLD): An update of the recent advances in pharmacological treatment. J. Physiol. Biochem. 2023, 79, 869–879. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.R.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023, 78, 1966–1986. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Neuschwander-Tetri, B.A.; Loomba, R.; Rinella, M.E. Metabolic dysfunction-associated steatotic liver disease: Update and impact of new nomenclature on the American Association for the Study of Liver Diseases practice guidance on nonalcoholic fatty liver disease. Hepatology 2024, 79, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Tourkochristou, E.; Assimakopoulos, S.F.; Thomopoulos, K.; Marangos, M.; Triantos, C. NAFLD and HBV interplay—Related mechanisms underlying liver disease progression. Front. Immunol. 2022, 13, 965548. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C.J.; Alkhalifah, M.; Afsar, H.; Pappachan, J.M. Metabolic dysfunction-associated fatty liver disease and chronic viral hepatitis: The interlink. Pathogens 2024, 13, 68. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Li, H.; Zhang, Y.; Zhang, J.; Cao, Z. Hepatitis B virus infection combined with nonalcoholic fatty liver disease: Interaction and prognosis. Heliyon 2023, 9, e13113. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. Obes. Facts 2016, 9, 65–90. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, J.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef]
- Kim, B.K.; Kim, D.Y.; Park, J.Y.; Ahn, S.H.; Chon, C.Y.; Kim, J.K.; Paik, Y.H.; Lee, K.S.; Park, Y.N.; Han, K.H. Validation of FIB-4 and comparison with other simple noninvasive indices for predicting liver fibrosis and cirrhosis in hepatitis B virus-infected patients. Liver Int. 2010, 30, 546–553. [Google Scholar] [CrossRef]
- Ginzberg, D.; Wong, R.J.; Gish, R. Global HBV burden: Guesstimates and facts. Hepatol. Int. 2018, 12, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Lyu, X.; Liu, K.; Chen, Y.; Wang, Z.; Yao, J.; Cai, G.; Jiang, Z.; Wang, Z.; Jiang, J.; Gu, H. Analysis of risk factors associated with the development of hepatocellular carcinoma in chronic HBV-infected Chinese: A meta-analysis. Int. J. Environ. Res. Public Health 2016, 13, 604. [Google Scholar] [CrossRef]
- Liu, M.; Li, L.; Zhao, J.; Ungvarim, G.S.; Ng, C.H.; Duan, Z.; Zheng, S.J.; Xiang, Y.T. Gender differences in demographic and clinical characteristics in patients with HBV-related liver diseases in China. PeerJ 2022, 10, e13828. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.H.; Chen, P.J.; Yeh, S.H. Gender disparity in chronic hepatitis B: Mechanisms of sex hormones. J. Gastroenterol. Hepatol. 2015, 30, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.; Goulder, P.; Matthews, P.C. Sexual dimorphism in chronic hepatitis B virus (HBV) infection: Evidence to inform elimination efforts. Wellcome Open Res. 2022, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Al Awaidy, S.T.; Bawikar, S.P.; Al Busaidy, S.S.; Al Mahrouqi, S.; Al Baqlani, S.; Al Obaidani, I.; Alexander, J.; Patel, M.K. Progress toward elimination of hepatitis B virus transmission in Oman: Impact of hepatitis B vaccination. Am. J. Trop. Med. Hyg. 2013, 89, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; Abraham, J.P. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Oman Obesity Briefing Book Launched. Available online: https://www.moh.gov.om/en/-/--1562 (accessed on 5 July 2024).
- Al-Riyami, A.A.; Afifi, M.M. Prevalence and correlates of obesity and central obesity among Omani adults. Saudi Med. J. 2003, 24, 641–646. [Google Scholar]
- Thin, K.N.; Tran, A.; Li, J.; Lee, E.Y.; Yang, H.; Rui, F.; Stave, C.D.; Cheung, R.C.; Nguyen, M.H. Increased risk of liver-related outcomes in chronic hepatitis B patients with metabolic syndrome: A systematic review and meta-analysis. Dig. Dis. 2022, 40, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.H.; Huang, K.C. Association between metabolic factors and chronic hepatitis B virus infection. World J. Gastroenterol. 2014, 20, 7213–7216. [Google Scholar] [CrossRef] [PubMed]
- Patmore, L.A.; Katwaroe, W.K.; van der Spek, D.; Choi, H.S.J.; Patel, K.; Brakenhoff, S.; van der Meer, A.J.; Brouwer, W.P.; van Kleef, L.A.; de Knegt, R.J. Association between the presence of metabolic comorbidities and liver-related events in patients with chronic hepatitis B. Clin. Gastroenterol. Hepatol. 2023, 21, 3089–3096.e1. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Lu, C.W.; Liu, Y.L.; Chiang, C.H.; Lee, L.T.; Huang, K.C. Relationship between chronic hepatitis B and metabolic syndrome: A structural equation modeling approach. Obesity 2016, 24, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Jee, H. Prevalence of metabolic syndrome in the Gulf Cooperation Council countries: Meta-analysis of cross-sectional studies. J. Exerc. Rehabil. 2020, 16, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Al-Shafaee, M.A.; Ganguly, S.S.; Bhargava, K.; Duttagupta, K.K. Prevalence of metabolic syndrome among prediabetic Omani adults: A preliminary study. Metab. Syndr. Relat. Disord. 2008, 6, 275–279. [Google Scholar] [CrossRef]
- Al-Lawati, J.A.; Mohammed, A.J.; Al-Hinai, H.Q.; Jousilahti, P. Prevalence of the metabolic syndrome among Omani adults. Diabetes Care 2003, 26, 1781–1785. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Cui, Y.; Deng, H.; Yu, J. Association between hepatitis B virus infection and metabolic syndrome: A retrospective cohort study in Shanghai, China. BMC Public Health 2014, 14, 516. [Google Scholar] [CrossRef] [PubMed]
- Katoonizadeh, A.; Ghoroghi, S.; Sharafkhah, M.; Khoshnia, M.; Mirzaei, S.; Shayanrad, A.; Poustchi, H.; Malekzadeh, R. Chronic hepatitis B infection is not associated with increased risk of vascular mortality while having an association with metabolic syndrome. J. Med. Virol. 2016, 88, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Razi, B.; Alizadeh, S.; Omidkhoda, A.; Imani, D.; Rezaei, R. Association of chronic hepatitis B infection with metabolic syndrome and its components: Meta-analysis of observational studies. Diabetes Metab. Syndr. 2017, 11, S939–S947. [Google Scholar] [CrossRef] [PubMed]
- Khalili, M.; Shuhart, M.C.; Lombardero, M.; Feld, J.J.; Kleiner, D.E.; Chung, R.T.; Hepatitis B Research Network (HBRN); Harvard Consortium; Terrault, N.A.; Lisker-Melman, M.; et al. Relationship between metabolic syndrome, alanine aminotransferase levels, and liver disease severity in a multiethnic North American cohort with chronic hepatitis B. Diabetes Care 2018, 41, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Jarcuska, P.; Drazilova, S.; Fedacko, J.; Pella, D.; Janicko, M. Association between hepatitis B and metabolic syndrome: Current state of the art. World J. Gastroenterol. 2016, 22, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Jarčuška, P.; Janičko, M.; Kružliak, P.; Novák, M.; Veselíny, E.; Fedačko, J.; HepaMeta Study Group; Senajová, G.; Dražilová, S.; Madarasová-Gecková, A.; et al. Hepatitis B virus infection in patients with metabolic syndrome: A complicated relationship. Results of a population based study. Eur. J. Intern. Med. 2014, 25, 286–291. [Google Scholar] [CrossRef]
- Wang, C.C.; Cheng, P.N.; Kao, J.H. Systematic review: Chronic viral hepatitis and metabolic derangement. Aliment. Pharmacol. Ther. 2020, 51, 216–230. [Google Scholar] [CrossRef] [PubMed]
- Moussa, F.R. Prevalence of diabetes mellitus among hepatitis B infected patients attending communicable disease research and training center, Suez City, Egypt. Suez Canal Univ. Med. J. 2018, 21, 113–119. [Google Scholar] [CrossRef]
- Al-Lawati, J.A.; Panduranga, P.; Al-Shaikh, H.A.; Morsi, M.; Mohsin, N.; Khandekar, R.B.; Al-Lawati, H.J.; Bayoumi, R.A. Epidemiology of diabetes mellitus in Oman: Results from two decades of research. Sultan Qaboos Univ. Med. J. 2015, 15, e226–e233. [Google Scholar] [PubMed]
- International Diabetes Federation. Oman. Available online: https://idf.org/our-network/regions-and-members/middle-east-and-north-africa/members/oman/ (accessed on 13 June 2024).
- Al-Mawali, A.; Al-Harrasi, A.; Jayapal, S.K.; Morsi, M.; Pinto, A.D.; Al-Shekaili, W.; Al-Kharusi, H.; Al-Balushi, Z.; Idikula, J. Prevalence and risk factors of diabetes in a large community-based study in the Sultanate of Oman: STEPS survey 2017. BMC Endocr. Disord. 2021, 21, 42. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Zeng, J.; Wu, H.; Shi, R.; Wei, M.; Gao, Y.; Ma, W. Association between hepatitis B virus infection and diabetes mellitus: A meta-analysis. Exp. Ther. Med. 2015, 10, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.C.; Kao, J.H. The interplay between chronic hepatitis B and diabetes mellitus: A narrative and concise review. Kaohsiung J. Med. Sci. 2024, 40, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Zhang, J.; Cai, H.; Shao, J.G.; Zhang, Y.Y.; Liu, Y.M.; Qin, G.; Qin, Y. Identifying patients with chronic hepatitis B at high risk of type 2 diabetes mellitus: A cross-sectional study with pair-matched controls. BMC Gastroenterol. 2015, 15, 32. [Google Scholar] [CrossRef] [PubMed]
- Estakhri, A.; Sari, A.A.; Nedjat, S.N.; Rohban, M.; Rakhshani, N.; Tavangar, S.M.; Malekzadeh, R.; Montazeri, G. The effect of NAFLD (non-alcoholic fatty liver disease) on long-term outcome of chronic hepatitis B in Iranian patients. Open J. Gastroenterol. 2012, 2, 18–21. [Google Scholar] [CrossRef]
- Wong, S.W.; Chan, W.K.; Mohamed, R. Fatty liver is associated with advanced fibrosis but does not predict adverse outcomes in patients with chronic hepatitis B. J. Viral Hepat. 2020, 27, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.J.; Chang, Y.; Yeom, J.S.; Ryu, S. Hepatitis B virus infection and decreased risk of nonalcoholic fatty liver disease: A cohort study. Hepatology 2017, 65, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Chen, C.; Liu, X.; Huang, C.; Yan, D.; Zhang, X.; Zhou, Y.; Lin, Y.; Zhou, Y.; Guan, Z.; et al. Concurrence and impact of hepatic steatosis on chronic hepatitis B patients: A systematic review and meta-analysis. Ann. Transl. Med. 2021, 9, 1718. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.V.; Oliveira, A.G.; Cortez-Pinto, H. Hepatic steatosis in hepatitis B virus infected patients: Meta-analysis of risk factors and comparison with hepatitis C infected patients. J. Gastroenterol. Hepatol. 2011, 26, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Torgerson, S.; Hayashi, P.H. The natural history of nonalcoholic fatty liver disease: A clinical histopathological study. Am. J. Gastroenterol. 2003, 98, 2042–2047. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Zhou, J.; Wang, W.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Zhu, L.; Cai, J.; Li, H. Unexpected rapid increase in the burden of NAFLD in China from 2008 to 2018: A systematic review and meta-analysis. Hepatology 2019, 70, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Wang, H.Y.; Chang, W.H.; Lin, S.C.; Chu, C.H.; Wang, T.E.; Liu, C.C.; Shih, S.C. Nonalcoholic fatty liver disease: Prevalence, influence on age and sex, and relationship with metabolic syndrome and insulin resistance. Int. J. Gerontol. 2013, 7, 194–198. [Google Scholar] [CrossRef]
- Shimizu, I.; Kohno, N.; Tamaki, K.; Shono, M.; Huang, H.W.; He, J.H.; Yao, D.F. Female hepatology: Favorable role of estrogen in chronic liver disease with hepatitis B virus infection. World J. Gastroenterol. 2007, 13, 4295–4305. [Google Scholar] [CrossRef] [PubMed]
- Diao, Y.; Hu, D.; Hu, X.; Wang, P.; Wang, X.; Luo, X.; Wang, H.; Ning, Q. The role of metabolic factors and steatosis in treatment-naïve patients with chronic hepatitis B and normal alanine aminotransferase. Infect. Dis. Ther. 2022, 11, 1133–1148. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.G.; Tian, N.; Xie, W.N. Total cholesterol to high-density lipoprotein ratio and nonalcoholic fatty liver disease in a population with chronic hepatitis B. World J. Hepatol. 2022, 14, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Akha, O.; Fakheri, H.; Abdi, R.; Mahdavi, M.R. Evaluation of the correlation between non-alcoholic fatty liver disease and insulin resistance. Iran. Red. Crescent Med. J. 2010, 12, 282–286. [Google Scholar]
- Fujii, H.; Kawada, N.; Japan Study Group of Nafld Jsg-Nafld. The role of insulin resistance and diabetes in nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2020, 21, 3863. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Zhang, H.; Wang, Y.; Wang, A.; Bian, J.; Huang, H.; Zheng, Y.; Sang, X.; Xu, Y.; Lu, X.; et al. Hepatitis B virus infection and the risk of nonalcoholic fatty liver disease: A meta-analysis. Oncotarget 2017, 8, 107295–107302. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.J.; Zhu, P.; Liang, Y.; Yin, W.G.; Xiao, J.H. Hepatitis B virus induces expression of cholesterol metabolism-related genes via TLR2 in HepG2 cells. World J. Gastroenterol. 2013, 19, 2262–2269. [Google Scholar] [CrossRef] [PubMed]
- Oehler, N.; Volz, T.; Bhadra, O.D.; Kah, J.; Allweiss, L.; Giersch, K.; Bierwolf, J.; Riecken, K.; Pollok, J.M.; Lohse, A.W.; et al. Binding of hepatitis B virus to its cellular receptor alters the expression profile of genes of bile acid metabolism. Hepatology 2014, 60, 1483–1493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, P.; Zhang, Y.; Nie, Y.; Zhu, X. Low high-density lipoprotein cholesterol levels predicting poor outcomes in patients with hepatitis B virus-related acute-on-chronic liver failure. Front. Med. 2022, 9, 1001411. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Liu, X.; Peng, S.; Han, Z.; Shen, J.; Cai, M. Association of low high-density lipoprotein cholesterol levels with poor outcomes in hepatitis B-associated decompensated cirrhosis patients. Biomed. Res. Int. 2021, 27, 9927330. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Álvarez, M.; Córdova-Ramírez, A.C.; Elías-De-La-Cruz, G.D.; Murrieta-Álvarez, I.; León-Peña, A.A.; Cantero-Fortiz, Y.; Olivares-Gazca, J.C.; Ruiz-Delgado, G.J.; Ruiz-Argüelles, G.J. Non-alcoholic fatty liver disease and thrombocytopenia IV: Its association with granulocytopenia. Hematol. Transfus. Cell Ther. 2022, 44, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Dasanu, C.A.; Lamana, S.; Trikudanathan, G. Thrombocytopenia in NAFLD: Is thrombopoietin involved? S. Med. J. 2010, 103, 1278–1279. [Google Scholar] [CrossRef] [PubMed]
- Olivares-Gazca, J.C.; Nuñez-Cortes, A.K.; Mendez-Huerta, M.A.; Cantero-Fortiz, Y.; Orea-Martinez, J.G.; Ruiz-Argüelles, G.J. More on the thrombocytopenia of the non-alcoholic fatty liver disease. Hematology 2017, 22, 316–319. [Google Scholar] [CrossRef] [PubMed]
- López-Trujillo, M.A.; Olivares-Gazca, J.M.; Cantero-Fortiz, Y.; García-Navarrete, Y.I.; Cruz-Mora, A.; Olivares-Gazca, J.C.; Murrieta-Álvarez, I.; León-Peña, A.A.; Ruiz-Delgado, G.J.; Ruiz-Argüelles, G.J. Nonalcoholic fatty liver disease and thrombocytopenia III: Its association with insulin resistance. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619888694. [Google Scholar] [CrossRef] [PubMed]
- Juárez-Hernández, E.; Chávez-Tapia, N.C.; Brizuela-Alcántara, D.C.; Uribe, M.; Ramos-Ostos, M.H.; Nuño-Lámbarri, N. Association between serum hemoglobin levels and non alcoholic fatty liver disease in a Mexican population. Ann. Hepatol. 2018, 17, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Tanoglu, A.; Kara, M. Nonalcoholic fatty liver disease-related cardiovascular risk: Is there an association with blood hemoglobin levels? Eur. J. Gastroenterol. Hepatol. 2015, 27, 1126–1129. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Xu, C.F.; Yu, C.H.; Miao, M.; Li, Y.M. Haemoglobin and non-alcoholic fatty liver disease: Further evidence from a population-based study. Gut 2009, 58, 1706–1707. [Google Scholar] [CrossRef] [PubMed]
- Bai, C.H.; Wu, M.S.; Owaga, E.; Cheng, S.Y.; Pan, W.H.; Chang, J.S. Relationship between hemoglobin levels and risk for suspected non-alcoholic fatty liver in Taiwanese adults. Chin. J. Physiol. 2014, 57, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Chung, G.E.; Yim, J.Y.; Kim, D.; Kwak, M.S.; Yang, J.I.; Chung, S.J.; Yang, S.Y.; Kim, J.S. Associations between hemoglobin concentrations and the development of incidental metabolic syndrome or nonalcoholic fatty liver disease. Dig. Liver Dis. 2017, 49, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.X.; Dou, X.G. [Optimal timing significance and clinical implications for the treatment of chronic HBV-infected patients with normal ALT]. Zhonghua Gan Zang Bing Za Zhi 2020, 28, 985–987. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Liu, S.; Zhang, J.; Dong, M.; Wang, Y.; Wang, M.; Xin, Y. Proportion of NAFLD patients with normal ALT value in overall NAFLD patients: A systematic review and meta-analysis. BMC Gastroenterol. 2020, 20, 10. [Google Scholar] [CrossRef]
- Verma, S.; Jensen, D.; Hart, J.; Mohanty, S.R. Predictive value of ALT levels for non-alcoholic steatohepatitis (NASH) and advanced fibrosis in non-alcoholic fatty liver disease (NAFLD). Liver Int. 2013, 33, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Xu, C.F.; Wan, X.Y.; Yu, C.H.; Shen, C.; Chen, P.; Xu, G.Y.; Li, Y.M. Association between serum alpha-fetoprotein levels and fatty liver disease: A cross-sectional study. World J. Gastroenterol. 2014, 20, 11865–11870. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhao, Y.; Feng, L.; Zhang, J.; Zhang, J.; Feng, G. Association between alpha-fetoprotein and metabolic syndrome in a Chinese asymptomatic population: A cross-sectional study. Lipids Health Dis. 2016, 15, 85. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cui, X.; Zhang, H.; Ding, X.; Hu, D.; Song, Y.; Chen, L.; Xin, Y. Elevated serum alpha-fetoprotein levels in non-alcoholic steatohepatitis: Possible molecular mechanisms and potential clinical significance. Gene Expr. 2023, 22, 135–140. [Google Scholar] [CrossRef]
- Babalı, A.; Cakal, E.; Purnak, T.; Bıyıkoğlu, I.; Cakal, B.; Yüksel, O.; Köklü, S. Serum α-fetoprotein levels in liver steatosis. Hepatol. Int. 2009, 3, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Choi, G.H.; Chang, W.; Jang, E.S.; Kim, J.W.; Jeong, S.H. Elevated alpha-fetoprotein in asymptomatic adults: Clinical features, outcome, and association with body composition. PLoS ONE 2022, 17, e0271407. [Google Scholar] [CrossRef]
- Huang, Y.; Gan, Q.; Lai, R.; Wang, W.; Guo, S.; Sheng, Z.; Chen, L.; Guo, Q.; Cai, W.; Wang, H.; et al. Application of fatty liver inhibition of progression algorithm and steatosis, activity, and fibrosis score to assess the impact of non-alcoholic fatty liver on untreated chronic hepatitis B patients. Front. Cell Infect. Microbiol. 2022, 11, 733348. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.N.; Xu, C.F.; Pan, H.Y.; Chen, M.J.; Yu, C.H. Fatty liver is associated with significant liver inflammation and increases the burden of advanced fibrosis in chronic HBV infection. BMC Infect. Dis. 2023, 23, 637. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Wei, L. Impact of NAFLD on the outcome of patients with chronic hepatitis B in Asia. Liver Int. 2022, 42, 1981–1990. [Google Scholar] [CrossRef] [PubMed]
- You, H.; Kong, Y.; Hou, J.; Wei, L.; Zhang, Y.; Niu, J.; Han, T.; Ou, X.; Dou, X.; Shang, J.; et al. Female gender lost protective effect against disease progression in elderly patients with chronic hepatitis B. Sci. Rep. 2016, 6, 37498. [Google Scholar] [CrossRef]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef] [PubMed]
- Codes, L.; Asselah, T.; Cazals-Hatem, D.; Tubach, F.; Vidaud, D.; Paraná, R.; Bedossa, P.; Valla, D.; Marcellin, P. Liver fibrosis in women with chronic hepatitis C: Evidence for the negative role of the menopause and steatosis and the potential benefit of hormone replacement therapy. Gut 2007, 56, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Abdelmalek, M.F.; Pang, H.; Guy, C.D.; Smith, A.D.; Diehl, A.M.; Suzuki, A. Gender and menopause impact severity of fibrosis among patients with nonalcoholic steatohepatitis. Hepatology 2014, 59, 1406–1414. [Google Scholar] [CrossRef]
- Xi, B.; He, D.; Hu, Y.; Zhou, D. Prevalence of metabolic syndrome and its influencing factors among the Chinese adults: The China Health and Nutrition Survey in 2009. Prev. Med. 2013, 57, 867–871. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.W.; Chang, H.C.; Chang, S.C.; Liaw, Y.F.; Lin, S.M.; Liu, C.J.; Lee, S.D.; Lin, C.L.; Chen, P.J.; Lin, S.C.; et al. Role of reproductive factors in hepatocellular carcinoma: Impact on hepatitis B- and C-related risk. Hepatology 2003, 38, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wu, J.; Pu, D.; Zhao, Y.; Wan, C.; Sun, L.; Shen, C.E.; Sun, W.; Yuan, Z.; Shen, Q.; et al. Factors associated with the age of natural menopause and menopausal symptoms in Chinese women. Maturitas 2012, 73, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; De, A.; Chowdhury, A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl. Gastroenterol. Hepatol. 2020, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Sheedfar, F.; Di Biase, S.; Koonen, D.; Vinciguerra, M. Liver diseases and aging: Friends or foes? Aging Cell 2013, 12, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.W.; Ting, Y.W.; Yong, Y.K.; Tan, H.Y.; Barathan, M.; Riazalhosseini, B.; Bee, C.J.; Tee, K.K.; Larsson, M.; Velu, V.; et al. Chronic inflammation involves CCL11 and IL-13 to facilitate the development of liver cirrhosis and fibrosis in chronic hepatitis B virus infection. Scand. J. Clin. Lab. Investig. 2021, 81, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Thong, V.D.; Quynh, B.T.H. Correlation of Serum transaminase levels with liver fibrosis assessed by transient elastography in Vietnamese patients with nonalcoholic fatty liver disease. Int. J. Gen. Med. 2021, 14, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, P.; Demirturk, N.; Batırel, A.; Yardimci, A.C.; Cagir, U.; Nemli, S.A.; Korkmaz, f.; Akcam, F.Z.; Barut, H.S.; Bayrak, B.; et al. Noninvasive models to predict liver fibrosis in patients with chronic hepatitis B: A study from Turkey. Hepat. Mon. 2017, 17, e60266. [Google Scholar] [CrossRef]
- Nyarko, E.N.Y.; Obirikorang, C.; Owiredu, W.K.B.A.; Adu, E.A.; Acheampong, E. Assessment of the performance of haematological and non-invasive fibrotic indices for the monitoring of chronic HBV infection: A pilot study in a Ghanaian population. BMC Res. Notes 2023, 16, 312. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhou, Y.; Yu, P.; Liu, Y.; Mei, M.; Bian, Z.; Shao, W.; Lv, J.; Li, X.; Lu, W.; et al. Retrospective evaluation of non-invasive assessment based on routine laboratory markers for assessing advanced liver fibrosis in chronic hepatitis B patients. Int. J. Gen. Med. 2022, 15, 5159–5171. [Google Scholar] [CrossRef] [PubMed]
- Giorgio, V.; Mosca, A.; Alterio, A.; Alisi, A.; Grieco, A.; Nobili, V.; Miele, L. Elevated hemoglobin level is associated with advanced fibrosis in pediatric nonalcoholic fatty liver disease. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.T.; Wang, L.L.; Yan, L.T.; Zhang, L.T.; Zhou, W.; Chen, Q.F.; Chen, Y.; Zheng, S.J.; Duan, Z.P.; Li, J.F. Platelet count is closely associated with the severity of liver injury in patients with chronic hepatitis B virus infection: A cross-sectional study. Exp. Ther. Med. 2020, 20, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.E.; Chang, J.J.; Wu, Y.Y.; Huang, S.H.; Chen, W.M.; Hsu, C.C.; Hung, C.H.; Shi, C.S.; Lee, K.D.; Chen, C.C.; et al. Different impacts of common risk factors associated with thrombocytopenia in patients with hepatitis B virus and hepatitis C virus infection. Biomed. J. 2022, 45, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.; Ryan, J.D.; Tsochatzis, E.A. Fibrosis assessment in patients with chronic hepatitis B virus (HBV) infection. Ann. Transl. Med. 2017, 5, 40. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).