
Reconstructive Surgery of the Head and Neck in Organ Transplant Recipients: A Case Report and a Review of the Literature

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
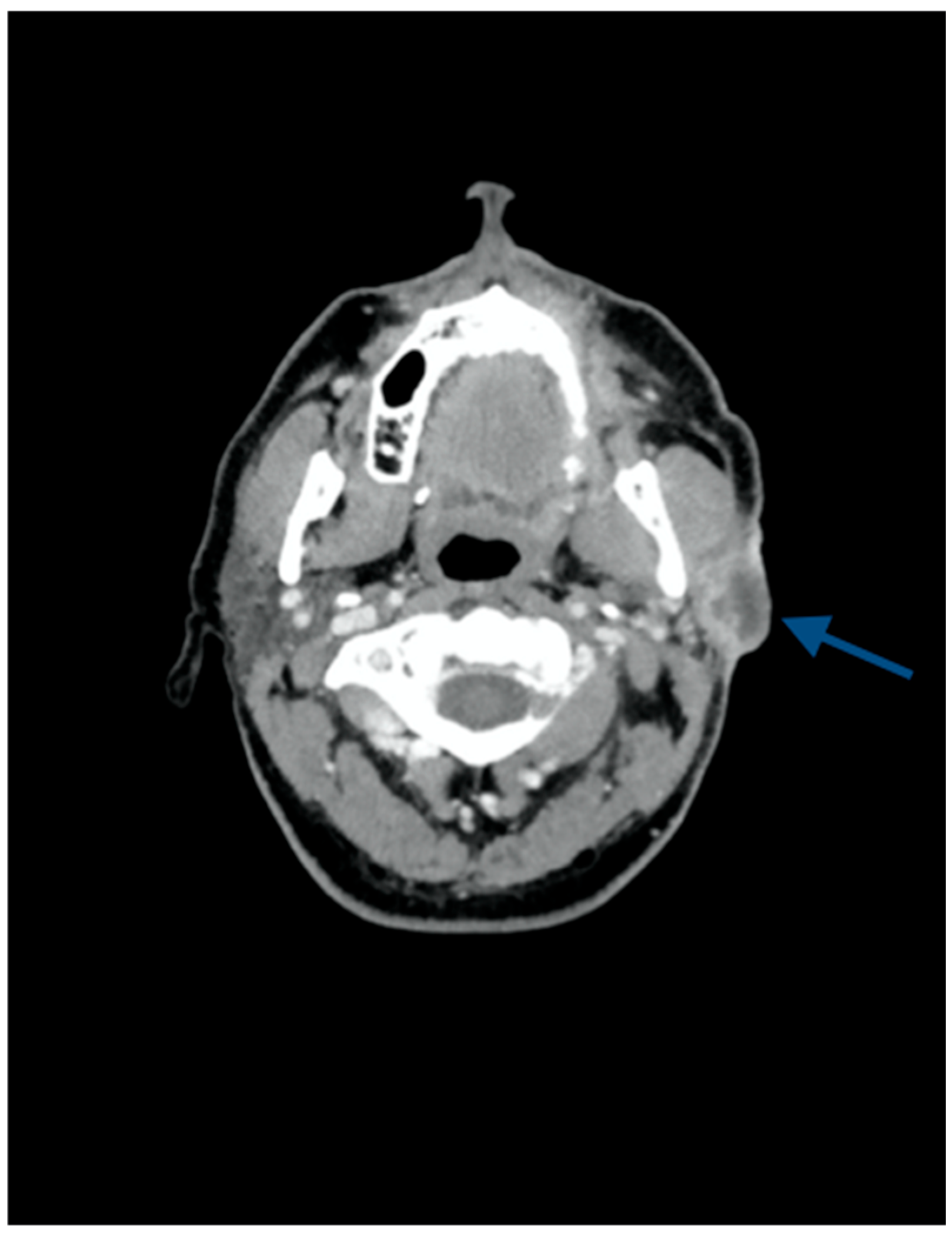
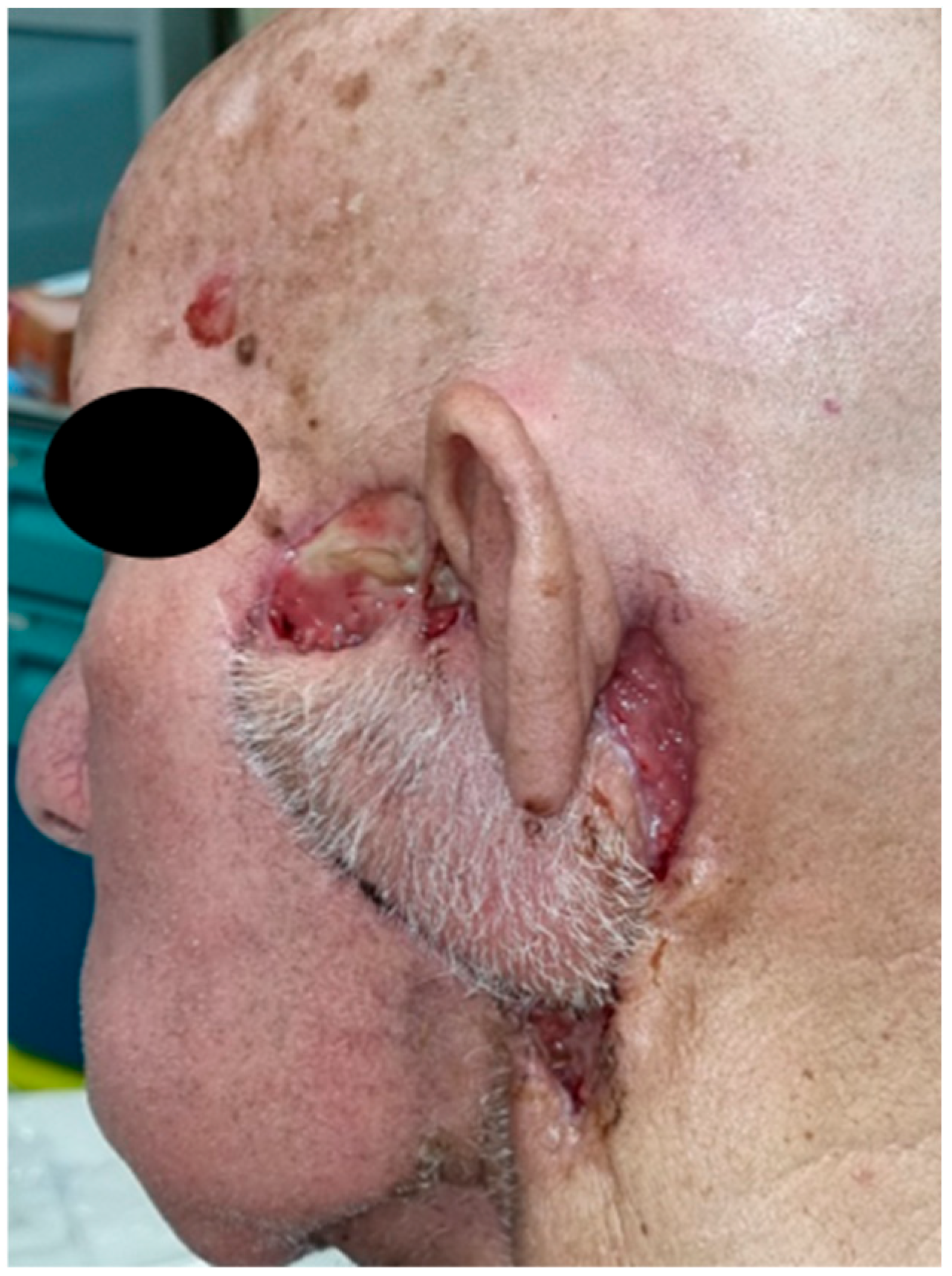
2. Case Presentation
3. Discussion
3.1. Epidemiology and Etiology of Cancers in SOTRs
3.2. Surgical Approach
3.3. Immunosuppressant Therapy and Wound Healing
3.4. Wound Healing Management in SOTRs: A Pragmatic Approach
4. Conclusions and Future Perspectives
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mowery, A.J.; Conlin, M.J.; Clayburgh, D.R. Elevated Incidence of Head and Neck Cancer in Solid Organ Transplant Recipients. Head Neck 2019, 41, 4009–4017. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.P.; Sexton, D.J.; O’Leary, E.; O’Kelly, P.; Murray, S.; Deady, S.; Daly, F.; Williams, Y.; Dean, B.; Fitzgerald, C.; et al. Post-Transplant Malignancy in Solid Organ Transplant Recipients in Ireland, The Irish Transplant Cancer Group. Clin. Transplant. 2019, 33, e13669. [Google Scholar] [CrossRef] [PubMed]
- Ajithkumar, T.V.; Parkinson, C.A.; Butler, A.; Hatcher, H.M. Management of Solid Tumours in Organ-Transplant Recipients. Lancet Oncol. 2007, 8, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Engels, E.A. Cancer in Solid Organ Transplant Recipients: There Is Still Much to Learn and Do. Am. J. Transplant. 2017, 17, 1967–1969. [Google Scholar] [CrossRef] [PubMed]
- Al-Qurayshi, Z.; Walsh, J.; Owen, S.; Randolph, G.; Kandil, E. Outcomes of Head and Neck Surgery in Patients with a History of Solid Organ Transplantation. Laryngoscope 2020, 130, E89–E97. [Google Scholar] [CrossRef] [PubMed]
- Tekin, H.G.; Eskandarani, H.A.; Iversen, L.; Juel, J. Immunosuppressive Therapy and Post-Operative Wound Healing. Ugeskr. Laeger 2021, 183, V07200544. [Google Scholar] [PubMed]
- Ueno, P.; Felipe, C.; Ferreira, A.; Cristelli, M.; Viana, L.; Mansur, J.; Basso, G.; Hannun, P.; Aguiar, W.; Tedesco Silva, H.; et al. Wound Healing Complications in Kidney Transplant Recipients Receiving Everolimus. Transplantation 2017, 101, 844–850. [Google Scholar] [CrossRef]
- Guo, S.; Dipietro, L.A. Factors Affecting Wound Healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, H.N.; Hardman, M.J. Wound Healing: Cellular Mechanisms and Pathological Outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef] [PubMed]
- Uberoi, A.; Mccready-Vangi, A.; Grice, E.A. The Wound Microbiota: Microbial Mechanisms of Impaired Wound Healing and Infection. Nat. Rev. Microbiol. 2024, 22, 507–521. [Google Scholar] [CrossRef] [PubMed]
- Truně Cka, P.; Boillot, O.; Seehofer, D.; Pinna, A.D.; Fischer, L.; Ericzon, B.-G.; Troisi, R.I.; Baccarani, U.; Ortiz De Urbina, J.; Wall, W. Once-Daily Prolonged-Release Tacrolimus (ADVAGRAF) Versus Twice-Daily Tacrolimus (PROGRAF) in Liver Transplantation. Am. J. Transplant. 2010, 10, 2313–2323. [Google Scholar] [CrossRef] [PubMed]
- Boudjema, K.; Camus, C.; Saliba, F.; Calmus, Y.; Salamé, E.; Salamé, S.; Pageaux, G.; Ducerf, C.; Duvoux, C.; Mouchel, C.; et al. Reduced-Dose Tacrolimus with Mycophenolate Mofetil vs. Standard-Dose Tacrolimus in Liver Transplantation: A Randomized Study. Am. J. Transplant. 2011, 11, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Røine, E.; Bjørk, I.T.; Øyen, O. Targeting Risk Factors for Impaired Wound Healing and Wound Complications after Kidney Transplantation. Transplant. Proc. 2010, 42, 2542–2546. [Google Scholar] [CrossRef] [PubMed]
- Acuna, S.A. Etiology of Increased Cancer Incidence after Solid Organ Transplantation. Transplant. Rev. 2018, 32, 218–224. [Google Scholar] [CrossRef]
- Liu, Q.; Yan, L.; Xu, C.; Gu, A.; Zhao, P.; Jiang, Z.-Y. Increased Incidence of Head and Neck Cancer in Liver Transplant Recipients: A Meta-Analysis. BMC Cancer 2014, 14, 776. [Google Scholar] [CrossRef] [PubMed]
- Piselli, P.; Burra, P.; Lauro, A.; Baccarani, U.; Ettorre, G.M.; Vizzini, G.B.; Rendina, M.; Rossi, M.; Tisone, G.; Zamboni, F.; et al. Head and Neck and Esophageal Cancers after Liver Transplant: Results from a Multicenter Cohort Study. Italy, 1997–2010. Transpl. Int. 2015, 28, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Galli, A.; Colombo, M.; Prizio, C.; Carrara, G.; Lira Luce, F.; Paesano, P.L.; Della Vecchia, G.; Giordano, L.; Bondi, S.; Tulli, M.; et al. Skeletal Muscle Depletion and Major Postoperative Complications in Locally-Advanced Head and Neck Cancer: A Comparison between Ultrasound of Rectus Femoris Muscle and Neck Cross-Sectional Imaging. Cancers 2022, 14, 347. [Google Scholar] [CrossRef] [PubMed]
- Kruse, A.L.D.; Luebbers, H.T.; Grätz, K.W.; Obwegeser, J.A. Factors Influencing Survival of Free-Flap in Reconstruction for Cancer of the Head and Neck: A Literature Review. Microsurgery 2010, 30, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.W.; Dean, N.R.; Cannady, S.B.; Rosenthal, E.L.; Wax, M.K. Free Tissue Transfer for Head and Neck Reconstruction in Solid Organ Transplant Patients. Head Neck 2012, 34, 1143–1146. [Google Scholar] [CrossRef] [PubMed]
- Sbitany, H.; Xu, X.; Hansen, S.L.; Young, D.M.; Hoffman, W.Y. The Effects of Immunosuppressive Medications on Outcomes in Microvascular Free Tissue Transfer. Plast. Reconstr. Surg. 2014, 133, 552e–558e. [Google Scholar] [CrossRef] [PubMed]
- Schaverien, M.V.; Dean, R.A.; Myers, J.N.; Fang, L.; Largo, R.D.; Yu, P. Outcomes of Microvascular Flap Reconstruction of the Head and Neck in Patients Receiving Systemic Immunosuppressive Therapy for Organ Transplantation. J. Surg. Oncol. 2018, 117, 1575–1583. [Google Scholar] [CrossRef] [PubMed]
- Noone, A.M.; Pfeiffer, R.M.; Dorgan, J.F.; Magder, L.S.; Bromberg, J.S.; Lynch, C.F.; Morris, C.R.; Pawlish, K.S.; Engels, E.A. Cancer-Attributable Mortality among Solid Organ Transplant Recipients in the United States: 1987 through 2014. Cancer 2019, 125, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, P.J.; Schaubel, D.E.; Fenton, S.S.; Shepherd, F.A.; Jiang, Y.; Mao, Y. Cancer Incidence among Canadian Kidney Transplant Recipients. Am. J. Transplant. 2007, 7, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Webster, A.C.; Craig, J.C.; Simpson, J.M.; Jones, M.P.; Chapman, J.R. Identifying High Risk Groups and Quantifying Absolute Risk of Cancer after Kidney Transplantation: A Cohort Study of 15,183 Recipients. Am. J. Transplant. 2007, 7, 2140–2151. [Google Scholar] [CrossRef] [PubMed]
- Rabinovics, N.; Hadar, T.; Mizrachi, A.; Bachar, G.; Purim, O.; Popovtzer, A. Adjuvant Treatment for Head and Neck Cancer in Solid Organ Transplant Recipients. Oral Oncol. 2015, 51, e23–e25. [Google Scholar] [CrossRef] [PubMed]
- Dantal, J.; Hourmant, M.; Cantarovich, D.; Giral, M.; Blancho, G.; Dreno, B.; Soulillou, J.-P. Effect of Long-Term Immunosuppression in Kidney-Graft Recipients on Cancer Incidence: Randomised Comparison of Two Cyclosporin Regimens. Lancet 1998, 351, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Benlloch, S.; Berenguer, M.; Prieto, M.; Moreno, R.; Juan, F.S.; Rayón, M.; Rayón, R.; Mir, J.; Segura, A.; Berenguer, J. De Novo Internal Neoplasms after Liver Transplantation: Increased Risk and Aggressive Behavior in Recent Years? Am. J. Transplant. 2004, 4, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.; Genden, E.M.; de Bree, R.; Rodrigo, J.P.; Rinaldo, A.; Sanabria, A.; Rapidis, A.D.; Takes, R.P.; Ferlito, A. Overcoming Wound Complications in Head and Neck Salvage Surgery. Auris Nasus Larynx 2018, 45, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Nakamizo, M.; Yokoshima, K.; Yagi, T. Use of Free Flaps for Reconstruction in Head and Neck Surgery: A Retrospective Study of 182 Cases. Auris Nasus Larynx 2004, 31, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Bootun, R. Effects of Immunosuppressive Therapy on Wound Healing. Int. Wound J. 2013, 10, 98–104. [Google Scholar] [CrossRef]
- Kearney, L.; Hogan, D.; Conlon, P.; Roche, M.; O’Neill, J.P.; O’Sullivan, J.B. High-Risk Cutaneous Malignancies and Immunosuppression: Challenges for the Reconstructive Surgeon in the Renal Transplant Population. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Ventura-Aguiar, P.; Campistol, M.; Diekmann, F. Expert Opinion on Drug Safety Safety of MTOR Inhibitors in Adult Solid Organ Transplantation Safety of MTOR Inhibitors in Adult Solid Organ Transplantation. Expert Opin. Drug Saf. 2016, 15, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Dean, P.G.; Lund, W.J.; Larson, T.S.; Prieto, M.; Nyeberg, S.L.; Ishitani, M.B.; Kremers, W.K.; Stegall, M.D. Wound-Healing Complication after Kidney Transplantation: A Prospective, Randomized Comparison of Sirolimus and Tacrolimus. Transplantation 2004, 77, 1555–1561. [Google Scholar] [CrossRef] [PubMed]
- Maenaka, A.; Kinoshita, K.; Hara, H.; Cooper, D.K.C. The Case for the Therapeutic Use of Mechanistic/Mammalian Target of Rapamycin (MTOR) Inhibitors in Xenotransplantation. Xenotransplantation 2023, 30, e12802. [Google Scholar] [CrossRef]
- Mehrabi, A.; Fonouni, H.; Wente, M.; Sadeghi, M.; Eisenbach, C.; Encke, J.; Schmied, B.M.; Libicher, M.; Zeier, M.; Weitz, J.; et al. Wound Complications Following Kidney and Liver Transplantation. Clin. Transplant. 2006, 20 (Suppl. S17), 97–110. [Google Scholar] [CrossRef] [PubMed]
- Galli, A.; Giordano, L. ASO Author Reflections: The Role of Indocyanine Green Fluorescence Video Angiography in Enhancing the Accuracy of Head and Neck Surgical Oncology. Ann. Surg. Oncol. 2022, 29, 8362–8363. [Google Scholar] [CrossRef] [PubMed]
- Giordano, L.; Familiari, M.; Galli, A.; Howardson, B.; Bussi, M. Trimming of Facial Artery Myomucosal Flap (FAMM) Using Indocyanine Green Fluorescence Video-Angiography: Operative Nuances. Ann. Surg. Oncol. 2022, 29, 8361. [Google Scholar] [CrossRef] [PubMed]
- Giordano, L.; Galli, A.; Familiari, M.; Canta, D.; Irem, A.; Biafora, M.; Battista, R.A.; Bussi, M. Head and Neck Pedicled Flap Autonomization Using a New High-Resolution Indocyanine Green Fluorescence Video-Angiography Device. Head Neck 2022, 44, 1496–1499. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-K. Innovations and Advances in Wound Healing; Springer: Berlin/Heidelberg, Germany, 2016; ISBN 978-3-662-46586-8. [Google Scholar]
- Rosenthal, E.L.; Blackwell, K.E.; McGrew, B.; Carroll, W.R.; Peters, G.E. Use of Negative Pressure Dressings in Head and Neck Reconstruction. Head Neck 2005, 27, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Marouf, A.; Mortada, H.; Khedr, B.; Halawani, L.; Zino Alarki, S.M.K.; Alghamdi, H. Effectiveness and Safety of Immediate Application of Negative Pressure Wound Therapy in Head and Neck Free Flap Reconstruction: A Systematic Review. Br. J. Oral. Maxillofac. Surg. 2022, 60, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Tatara, A.M.; Kontoyiannis, D.P.; Mikos, A.G. Drug Delivery and Tissue Engineering to Promote Wound Healing in the Immunocompromised Host: Current Challenges and Future Directions. Adv. Drug Deliv. Rev. 2018, 129, 319–329. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rampi, A.; Comini, L.V.; Galli, A.; Howardson, B.O.; Tettamanti, A.; Luparello, P.; Redaelli, G.; Di Santo, D.; Bondi, S. Reconstructive Surgery of the Head and Neck in Organ Transplant Recipients: A Case Report and a Review of the Literature. J. Clin. Med. 2024, 13, 4790. https://doi.org/10.3390/jcm13164790
Rampi A, Comini LV, Galli A, Howardson BO, Tettamanti A, Luparello P, Redaelli G, Di Santo D, Bondi S. Reconstructive Surgery of the Head and Neck in Organ Transplant Recipients: A Case Report and a Review of the Literature. Journal of Clinical Medicine. 2024; 13(16):4790. https://doi.org/10.3390/jcm13164790
Chicago/Turabian StyleRampi, Andrea, Lara Valentina Comini, Andrea Galli, Bright Oworae Howardson, Alberto Tettamanti, Paolo Luparello, Gabriele Redaelli, Davide Di Santo, and Stefano Bondi. 2024. "Reconstructive Surgery of the Head and Neck in Organ Transplant Recipients: A Case Report and a Review of the Literature" Journal of Clinical Medicine 13, no. 16: 4790. https://doi.org/10.3390/jcm13164790
APA StyleRampi, A., Comini, L. V., Galli, A., Howardson, B. O., Tettamanti, A., Luparello, P., Redaelli, G., Di Santo, D., & Bondi, S. (2024). Reconstructive Surgery of the Head and Neck in Organ Transplant Recipients: A Case Report and a Review of the Literature. Journal of Clinical Medicine, 13(16), 4790. https://doi.org/10.3390/jcm13164790