
Reliability of a New Digital Tool for Photographic Analysis in Quantifying Body Asymmetry in Scoliosis
 , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
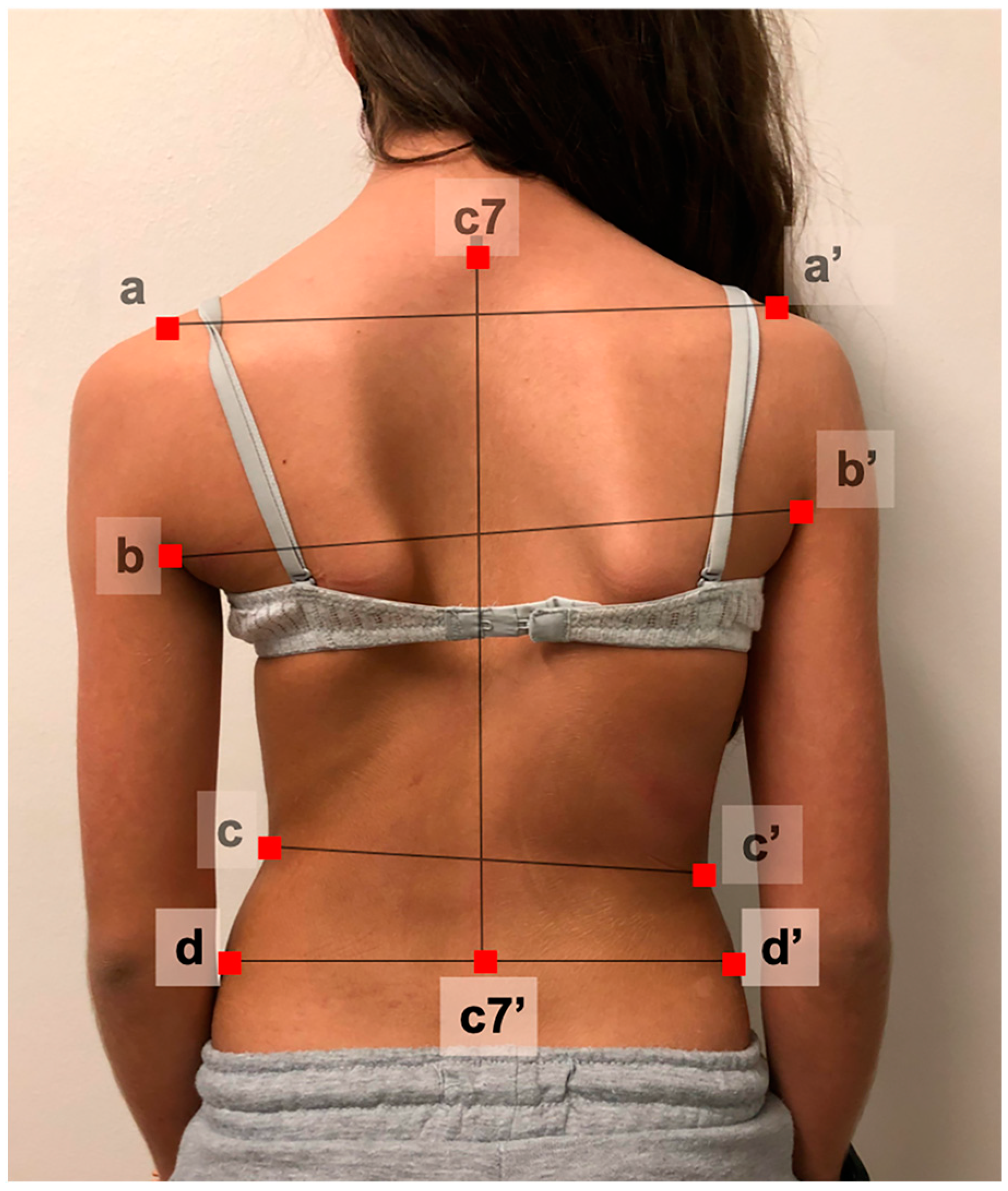
2.2. Photograph Acquisition
2.3. Designing the Digital Measuring Tool
2.4. Observer Training
2.5. Reliability, Reproducibility, and Repeatability Tests
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bengtsson, G.; Fällström, K.; Jansson, B.; Nachemson, A. A psychological and psychiatric investigation of the adjustment of female scoliosis patients. Acta Psychiatr. Scand. 1974, 50, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.L.; Donaldson, S.; Hedden, D.; Alman, B.; Howard, A.; Stephens, D.; Wright, J.G. Parents’ and patients’ perceptions of postoperative appearance in adolescent idiopathic scoliosis. Spine 2006, 31, 2367–2374. [Google Scholar] [CrossRef] [PubMed]
- Cochran, T.; Irstam, L.; Nachemson, A. Long-term anatomic and functional changes in patients with adolescent idiopathic scoliosis treated by Harrington rod fusion. Spine 1983, 8, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Shufflebarger, H.L.; Lenke, L.G.; Lowe, T.G.; Betz, R.R.; Bassett, G.S. Parents’ and patients’ preferences and concerns in idiopathic adolescent scoliosis: A cross-sectional preoperative analysis. Spine 2000, 25, 2392–2399. [Google Scholar] [CrossRef] [PubMed]
- Dubousset, J.; Charpak, G.; Skalli, W.; Kalifa, G.; Lazennec, J.Y. EOS stereo-radiography system: Whole-body simultaneous anteroposterior and lateral radiographs with very low radiation dose. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2007, 93, 141–143. [Google Scholar] [CrossRef]
- Ronckers, C.M.; Land, C.E.; Miller, J.S.; Stovall, M.; Lonstein, J.E.; Doody, M.M. Cancer mortality among women frequently exposed to radiographic examinations for spinal disorders. Radiat. Res. 2010, 174, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Knott, P.; Pappo, E.; Cameron, M.; Demauroy, J.; Rivard, C.; Kotwicki, T.; Zaina, F.; Wynne, J.; Stikeleather, L.; Bettany-Saltikov, J.; et al. SOSORT 2012 consensus paper: Reducing x-ray exposure in pediatric patients with scoliosis. Scoliosis 2014, 9, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Betsch, M.; Wild, M.; Jungbluth, P.; Hakimi, M.; Windolf, J.; Haex, B.; Horstmann, T.; Rapp, W. Reliability and validity of 4D rasterstereography under dynamic conditions. Comput. Biol. Med. 2011, 41, 308–312. [Google Scholar] [CrossRef]
- Knott, P.; Sturm, P.; Lonner, B.; Cahill, P.; Betsch, M.; McCarthy, R.; Kelly, M.; Lenke, L.; Betz, R. Multicenter Comparison of 3D Spinal Measurements Using Surface Topography with Those from Conventional Radiography. Spine Deform. 2016, 4, 98–103. [Google Scholar] [CrossRef]
- Koo, T.K.; Guo, J.-Y.; Ippolito, C.; Bedle, J.C. Assessment of scoliotic deformity using spinous processes: Comparison of different analysis methods of an ultrasonographic system. J. Manip. Physiol. Ther. 2014, 37, 667–677. [Google Scholar] [CrossRef]
- Zheng, R.; Young, M.; Hill, D.; Le, L.; Hedden, D.; Moreau, M.; Mahood, J.; Southon, S.; Lou, E. Improvement on the Accuracy and Reliability of Ultrasound Coronal Curvature Measurement on Adolescent Idiopathic Scoliosis with the Aid of Previous Radiographs. Spine 2016, 41, 404–411. [Google Scholar] [CrossRef]
- Patias, P.; Grivas, T.B.; Kaspiris, A.; Aggouris, C.; Drakoutos, E. A review of the trunk surface metrics used as Scoliosis and other deformities evaluation indices. Scoliosis 2010, 5, 12. [Google Scholar] [CrossRef]
- Thakur, A.; Groisser, B.; Hillstrom, H.J.; Cunningham, M.E.; Hresko, M.T.; Otremski, H.; Morse, K.W.; Page, K.; Gmelich, C.; Kimmel, R.; et al. 3D surface topographic measurements for idiopathic scoliosis are highly correlative to patient self-image questionnaires. Spine Deform. 2023, 11, 871–880. [Google Scholar] [CrossRef]
- Gardner, A.; Berryman, F.; Pynsent, P. The effects of scoliosis and subsequent surgery on the shape of the torso. Scoliosis Spinal Disord. 2017, 12, 31. [Google Scholar] [CrossRef]
- González-Ruiz, J.M.; Pérez-Núñez, M.I.; García-Alfaro, M.D.; Bastir, M. Geometric morphometrics of adolescent idiopathic scoliosis: A prospective observational study. Eur. Spine J. 2021, 30, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Dong, R.; Wen, Z.; Liu, Y. Reliability and Validity of Scoliosis Measurements Obtained with Surface Topography Techniques: A Systematic Review. J. Clin. Med. 2022, 11, 6998. [Google Scholar] [CrossRef] [PubMed]
- Fortin, C.; Feldman, D.E.; Cheriet, F.; Labelle, H. Clinical methods for quantifying body segment posture: A literature review. Disabil. Rehabil. 2011, 33, 367–383. [Google Scholar] [CrossRef]
- Bago, J.; Pizones, J.; Matamalas, A.; D’Agata, E. Clinical photography in severe idiopathic scoliosis candidate for surgery: Is it a useful tool to differentiate among Lenke patterns? Eur. Spine J. 2019, 28, 3018–3025. [Google Scholar] [CrossRef] [PubMed]
- Stolinski, L.; Kozinoga, M.; Czaprowski, D.; Tyrakowski, M.; Cerny, P.; Suzuki, N.; Kotwicki, T. Two-dimensional digital photography for child body posture evaluation: Standardized technique, reliable parameters and normative data for age 7–10 years. Scoliosis Spinal Disord. 2017, 12, 38. [Google Scholar] [CrossRef]
- Qiu, X.-S.; Ma, W.-W.; Li, W.-G.; Wang, B.; Yu, Y.; Zhu, Z.-Z.; Qian, B.-P.; Zhu, F.; Sun, X.; Ng, B.K.W.; et al. Discrepancy between radiographic shoulder balance and cosmetic shoulder balance in adolescent idiopathic scoliosis patients with double thoracic curve. Eur. Spine J. 2009, 18, 45–51. [Google Scholar] [CrossRef]
- Qiu, Y.; Qiu, X.-S.; Ma, W.-W.; Wang, B.; Yu, Y.; Zhu, Z.-Z.; Qian, B.-P.; Zhu, F.; Sun, X.; Ng, B.K.W.; et al. How well do radiological measurements correlate with cosmetic indices in adolescent idiopathic scoliosis with Lenke 5, 6 curve types? Spine 2010, 35, E882–E888. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Andersen, T.; Wu, C.; Sun, H.; Wang, Y.; Hansen, E.S.; Bünger, C.E. How well do Radiologic Assessments of Truncal and Shoulder Balance Correlate with Cosmetic Assessment Indices in Lenke 1C Adolescent Idiopathic Scoliosis? Clin. Spine Surg. 2016, 29, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Matamalas, A.; Bagó, J.; D’agata, E.; Pellisé, F. Reliability and validity study of measurements on digital photography to evaluate shoulder balance in idiopathic scoliosis. Scoliosis 2014, 9, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Matamalas, A.; Bago, J.; D’ Agata, E.; Pellise, F. Validity and reliability of photographic measures to evaluate waistline asymmetry in idiopathic scoliosis. Eur. Spine J. 2016, 25, 3170–3179. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Popović, Z.B.; Thomas, J.D. Assessing observer variability: A user’s guide. Cardiovasc. Diagn. Ther. 2017, 7, 317–324. [Google Scholar] [CrossRef]
- Bago, J.; Climent, J.M.; Pérez-Grueso, F.J.S.; Pellise, F. Outcome instruments to assess scoliosis surgery. Eur. Spine J. 2013, 22 (Suppl. 2), S195–S202. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, S.; Hedden, D.; Stephens, D.; Alman, B.; Howard, A.; Narayanan, U.; Wright, J.G. Surgeon reliability in rating physical deformity in adolescent idiopathic scoliosis. Spine 2007, 32, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Iwahara, T.; Imai, M.; Atsuta, Y. Quantification of cosmesis for patients affected by adolescent idiopathic scoliosis. Eur. Spine J. 1998, 7, 12–15. [Google Scholar] [CrossRef]
- Drerup, B. Rasterstereographic measurement of scoliotic deformity. Scoliosis 2014, 9, 22. [Google Scholar] [CrossRef]
- Wu, H.-D.; Liu, W.; Wong, M.S. Reliability and validity of lateral curvature assessments using clinical ultrasound for the patients with scoliosis: A systematic review. Eur. Spine J. 2020, 29, 717–725. [Google Scholar] [CrossRef]
- Lee, T.T.-Y.; Lai, K.K.-L.; Cheng, J.C.-Y.; Castelein, R.M.; Lam, T.-P.; Zheng, Y.-P. 3D ultrasound imaging provides reliable angle measurement with validity comparable to X-ray in patients with adolescent idiopathic scoliosis. J. Orthop. Transl. 2021, 29, 51–59. [Google Scholar] [CrossRef]
- Zheng, R.; Chan, A.C.; Chen, W.; Hill, D.L.; Le, L.H.; Hedden, D.; Moreau, M.; Mahood, J.; Southon, S.; Lou, E. Intra- and Inter-rater Reliability of Coronal Curvature Measurement for Adolescent Idiopathic Scoliosis Using Ultrasonic Imaging Method—A Pilot Study. Spine Deform. 2015, 3, 151–158. [Google Scholar] [CrossRef]
- Mehta, B.; Chockalingam, N.; Shannon, T.; Jevtic, N.; Lazic, F.; Jasani, V.; Eddison, N.; Healy, A.; Needham, R. Non-Invasive Assessment of Back Surface Topography: Technologies, Techniques and Clinical Utility. Sensors 2023, 23, 8485. [Google Scholar] [CrossRef]
- Porto, F.; Gurgel, J.L.; Russomano, T.; Farinatti, P.D.T.V. Moiré topography: Characteristics and clinical application. Gait Posture 2010, 32, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Pazos, V.; Cheriet, F.; Danserau, J.; Ronsky, J.; Zernicke, R.F.; Labelle, H. Reliability of trunk shape measurements based on 3-D surface reconstructions. Eur. Spine J. 2007, 16, 1882–1891. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.; D’Agata, E. Comparison between subjective perception of trunk deformity (TAPS) and objective assessment of back asymmetry (surface topography). Scoliosis 2013, 8, O9. [Google Scholar] [CrossRef]
- Zheng, Q.; Xie, L.; Xu, J.; Xia, N.; Ma, C.Z.-H. A feasibility study of applying two-dimensional photogrammetry for screening and monitoring of patients with adolescent idiopathic scoliosis in clinical practice. Sci. Rep. 2023, 13, 14273. [Google Scholar] [CrossRef]
- Komeili, A.; Westover, L.M.; Parent, E.C.; Moreau, M.; El-Rich, M.; Adeeb, S. Surface topography asymmetry maps categorizing external deformity in scoliosis. Spine J. 2014, 14, 973–983.e2. [Google Scholar] [CrossRef]
- Groisser, B.N.; Hillstrom, H.J.; Thakur, A.; Morse, K.W.; Cunningham, M.; Hresko, M.T.; Kimmel, R.; Wolf, A.; Widmann, R.F. Reliability of automated topographic measurements for spine deformity. Spine Deform. 2022, 10, 1035–1045. [Google Scholar] [CrossRef]
- Applebaum, A.; Cho, W.; Nessim, A.; Kim, K.; Tarpada, S.P.; Yoon, S.H.; Pujar, B.; Kim, D.; Kim, S.Y. Establishing the validity of surface topography for assessment of scoliosis: A prospective study. Spine Deform. 2021, 9, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Chowanska, J.; Kotwicki, T.; Rosadzinski, K.; Sliwinski, Z. School screening for scoliosis: Can surface topography replace examination with scoliometer? Scoliosis 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- E Amendt, L.; Ause-Ellias, K.L.; Eybers, J.L.; Wadsworth, C.T.; Nielsen, D.H.; Weinstein, S.L. Validity and reliability testing of the Scoliometer. Phys. Ther. 1990, 70, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, J.; Xu, R.; Chen, T.G.; Zhou, K.S.; Zhang, H.H. Measurement of scoliosis Cobb angle by end vertebra tilt angle method. J. Orthop. Surg. Res. 2018, 13, 223–227. [Google Scholar] [CrossRef]
- Jin, C.; Wang, S.; Yang, G.; Li, E.; Liang, Z. A Review of the Methods on Cobb Angle Measurements for Spinal Curvature. Sensors 2022, 22, 3258. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N | Minimum | Maximum | Mean ± SD | Median (IR) | SEM | |
|---|---|---|---|---|---|---|
| SHA (°) | 15 | −7.5 | 2.43 | −2.5 ± 2.6 | −2.8 (3.83) | 0.30 |
| AHA (°) | 15 | −7.8 | −0.85 | −4.4 ± 2.2 | −3.9 (3) | 1.17 |
| WHA (°) | 15 | −3.1 | 6.58 | 2.0 ± 3.0 | 1.7 (3.7) | 0.57 |
| LWA (°) | 15 | 128.4 | 157.18 | 144.8 ± 9.5 | 145.9 (17.4) | 0.95 |
| RWA (°) | 15 | 132.3 | 163.58 | 147.9 ± 8.1 | 146.7 (12.1) | 1.3 |
| WAD (°) | 15 | −35.2 | 24.88 | −3.1 ± 14.9 | −6.4 (21.8) | 1.15 |
| SA px2 | 15 | 0.80 | 1.14 | 0.94 ± 0.09 | 0.93 (0.1) | 0.02 |
| WA px2 | 15 | 0.52 | 0.93 | 0.71 ± 0.12 | 0.69 (0.2) | 0.06 |
| PA px2 | 15 | 0.45 | 1.69 | 0.83 ± 0.3 | 0.78 (0.3) | 0.12 |
| TA px2 | 15 | 0.64 | 1.06 | 0.81 ± 0.12 | 0.81 (0.2) | 0.05 |
| Inter-Observer | Intraclass Correlation | 95% Confidence Interval | F Test | ||
|---|---|---|---|---|---|
| Lower Bound | Higher Bound | Value | Sig | ||
| SHA | 0.986 | 0.972 | 0.994 | 81.5 | 0.000 |
| AHA | 0.973 | 0.942 | 0.990 | 62.9 | 0.000 |
| WHA | 0.963 | 0.929 | 0.986 | 28.0 | 0.000 |
| LWA | 0.990 | 0.979 | 0.996 | 124.7 | 0.000 |
| RWA | 0.972 | 0.946 | 0.989 | 37.0 | 0.000 |
| WAD | 0.994 | 0.988 | 0.998 | 161.2 | 0.000 |
| SA | 0.976 | 0.951 | 0.991 | 56.8 | 0.000 |
| WA | 0.987 | 0.975 | 0.995 | 89.7 | 0.000 |
| PA | 0.986 | 0.973 | 0.995 | 77.3 | 0.000 |
| TA | 0.988 | 0.977 | 0.995 | 100 | 0.000 |
| Total Mean | 0.981 | 0.963 | 0.992 | ||
| Observer | SHA | AHA | WHA | LWA | RWA | WAD | SA | WA | PA | TA |
|---|---|---|---|---|---|---|---|---|---|---|
| Obsv1 | 0.946 | 0.985 | 0.955 | 0.977 | 0.99 | 0.988 | 0.927 | 0.977 | 0.98 | 0.969 |
| Obsv2 | 0.953 | 0.978 | 0.926 | 0.918 | 0.934 | 0.997 | 0.962 | 0.972 | 0.994 | 0.988 |
| Obsv3 | 0.752 | 0.791 | 0.734 | 0.946 | 0.887 | 0.968 | 0.785 | 0.899 | 0.931 | 0.86 |
| Obsv4 | 0.992 | 0.99 | 0.637 | 0.99 | 0.988 | 0.997 | 0.966 | 0.979 | 0.989 | 0.98 |
| Obsv5 | 0.908 | 0.954 | 0.943 | 0.98 | 0.815 | 0.947 | 0.966 | 0.957 | 0.961 | 0.959 |
| Obsv6 | 0.96 | 0.975 | 0.926 | 0.963 | 0.979 | 0.98 | 0.934 | 0.98 | 0.865 | 0.986 |
| Obsv7 | 0.931 | 0.973 | 0.881 | 0.973 | 0.974 | 0.994 | 0.901 | 0.957 | 0.984 | 0.971 |
| Obsv8 | 0.962 | 0.974 | 0.985 | 0.983 | 0.98 | 0.99 | 0.879 | 0.945 | 0.989 | 0.952 |
| Obsv9 | 0.962 | 0.985 | 0.987 | 0.986 | 0.941 | 0.994 | 0.937 | 0.978 | 0.991 | 0.976 |
| Obsv10 | 0.993 | 0.989 | 0.982 | 0.993 | 0.997 | 0.996 | 0.941 | 0.975 | 0.994 | 0.975 |
| Obsv11 | 0.921 | 0.818 | 0.655 | 0.923 | 0.609 | 0.931 | 0.894 | 0.92 | 0.946 | 0.951 |
| Obsv12 | 0.913 | 0.966 | 0.535 | 0.778 | 0.796 | 0.916 | 0.919 | 0.974 | 0.969 | 0.973 |
| Variable | Mean | Standard Deviation | Range | |
|---|---|---|---|---|
| Minimum | Maximum | |||
| SHA | 0.93 | 0.06 | 0.752 | 0.993 |
| AHA | 0.95 | 0.06 | 0.791 | 0.990 |
| WHA | 0.84 | 0.16 | 0.535 | 0.987 |
| LWA | 0.95 | 0.06 | 0.778 | 0.993 |
| RWA | 0.91 | 0.12 | 0.609 | 0.997 |
| WAD | 0.97 | 0.03 | 0.916 | 0.997 |
| SA | 0.92 | 0.05 | 0.785 | 0.966 |
| WA | 0.96 | 0.03 | 0.899 | 0.980 |
| PA | 0.97 | 0.04 | 0.865 | 0.994 |
| TA | 0.96 | 0.03 | 0.860 | 0.988 |
| Total Mean | 0.937 | 0.06 | 0.779 | 0.988 |
| Variable | Researchers | Surgeons | Sig |
|---|---|---|---|
| SHA | 0.96 ± 0.03 | 0.90 ± 0.08 | 0.126 |
| AHA | 0.98 ± 0.01 | 0.92 ± 0.09 | 0.154 |
| WHA | 0.83 ± 0.19 | 0.86 ± 0.13 | 0.784 |
| LWA | 0.94 ± 0.08 | 0.96 ± 0.02 | 0.479 |
| RWA | 0.94 ± 0.08 | 0.87 ± 0.14 | 0.283 |
| WAD | 0.98 ± 0.03 | 0.97 ± 0.03 | 0.609 |
| SA | 0.93 ± 0.03 | 0.90 ± 0.63 | 0.303 |
| WA | 0.97 ± 0.01 | 0.95 ± 0.03 | 0.151 |
| PA | 0.97 ± 0.05 | 0.96 ± 0.02 | 0.961 |
| TA | 0.97 ± 0.01 | 0.95 ± 0.44 | 0.186 |
| Total Mean | 0.948 ± 0.04 | 0.925 ± 0.05 | 0.410 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pizones, J.; Moreno-Manzanaro, L.; Pupak, A.; Núñez-Pereira, S.; Larrieu, D.; Boissiere, L.; Richner-Wunderlin, S.; Loibl, M.; Zulemyan, T.; Yücekul, A.; et al. Reliability of a New Digital Tool for Photographic Analysis in Quantifying Body Asymmetry in Scoliosis. J. Clin. Med. 2024, 13, 2114. https://doi.org/10.3390/jcm13072114
Pizones J, Moreno-Manzanaro L, Pupak A, Núñez-Pereira S, Larrieu D, Boissiere L, Richner-Wunderlin S, Loibl M, Zulemyan T, Yücekul A, et al. Reliability of a New Digital Tool for Photographic Analysis in Quantifying Body Asymmetry in Scoliosis. Journal of Clinical Medicine. 2024; 13(7):2114. https://doi.org/10.3390/jcm13072114
Chicago/Turabian StylePizones, Javier, Lucía Moreno-Manzanaro, Anika Pupak, Susana Núñez-Pereira, Daniel Larrieu, Louis Boissiere, Sarah Richner-Wunderlin, Markus Loibl, Tais Zulemyan, Altug Yücekul, and et al. 2024. "Reliability of a New Digital Tool for Photographic Analysis in Quantifying Body Asymmetry in Scoliosis" Journal of Clinical Medicine 13, no. 7: 2114. https://doi.org/10.3390/jcm13072114