
Vaginal Microbiota and Proinflammatory Status in Patients with Polycystic Ovary Syndrome: An Exploratory Study

 , , , , ,
, , , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample
2.3. Location
2.4. Ethical Aspects
2.5. Survey Application
2.6. Patients
2.7. Vaginal Discharge Samples
2.7.1. DNA Extraction
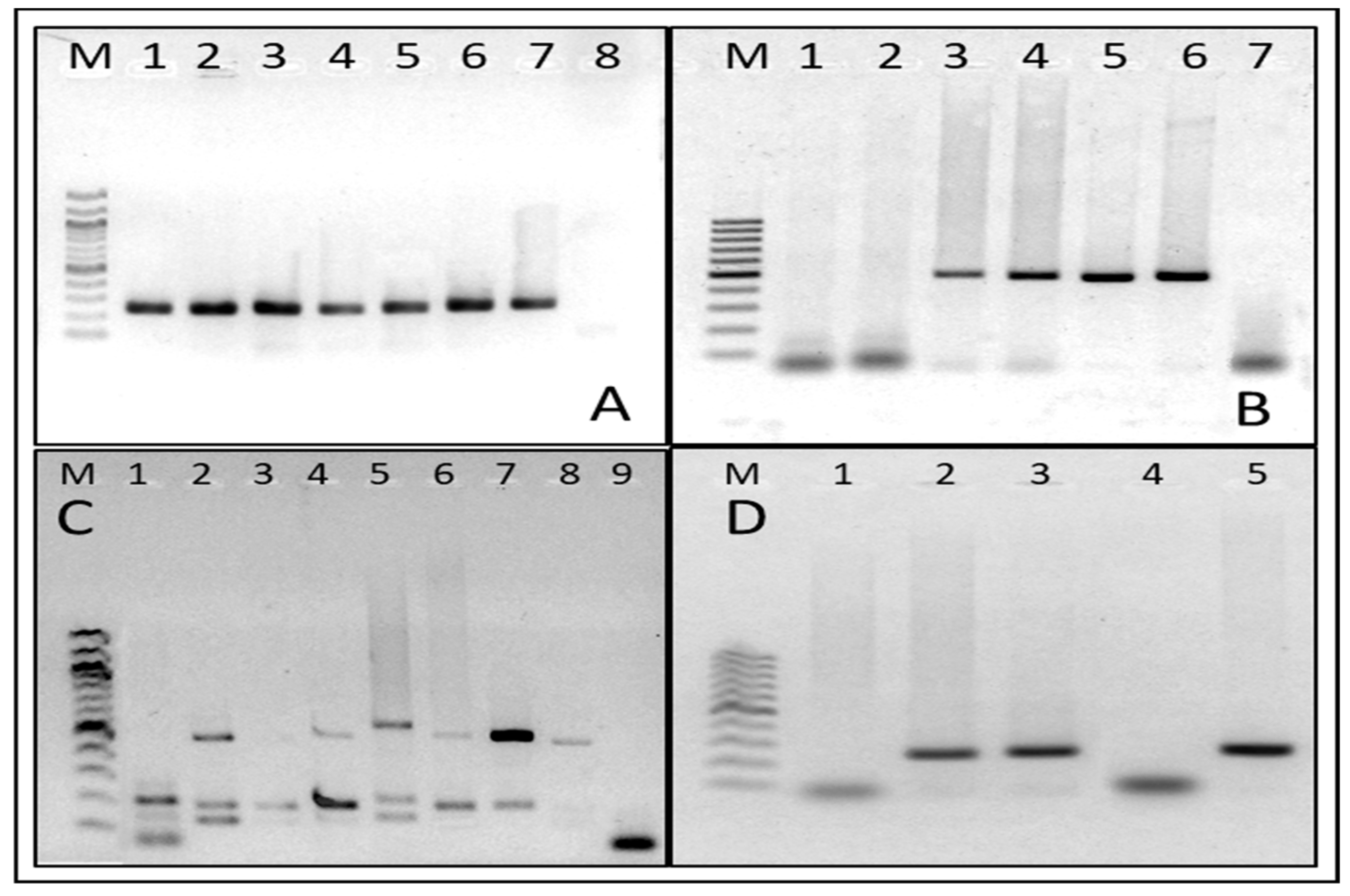
2.7.2. Microorganism DNA Detection
2.8. Analysis of Vaginal Discharge Smears
2.8.1. Gram Stain
2.8.2. Proinflammatory State
2.8.3. Vaginal Inflammatory Reaction (VIR)
2.8.4. Interpretation of Results
Nonspecific Microbial Vaginitis (nMVitis)
Bacterial Vaginosis
Definition of Altered and Normal Microbiota
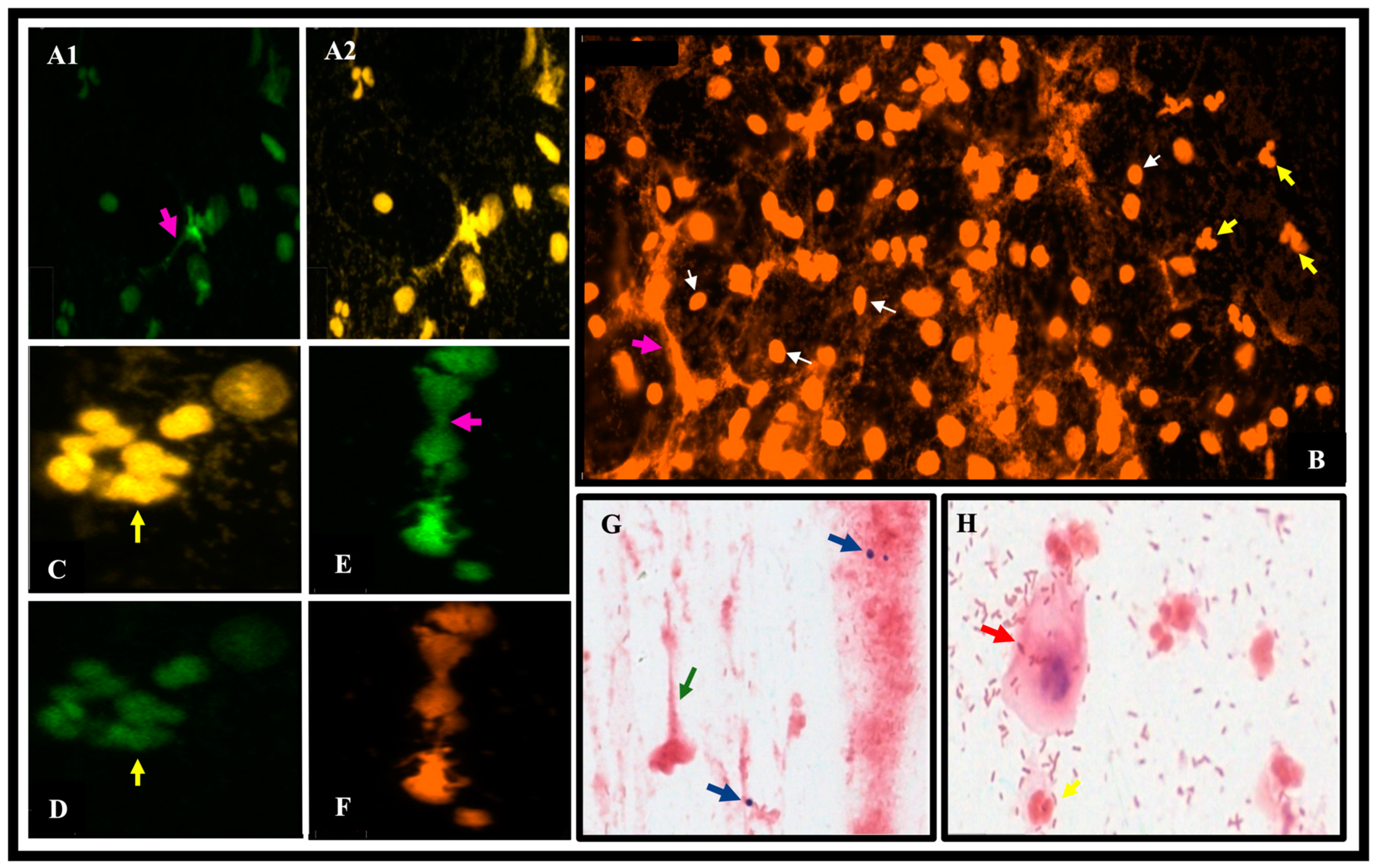
2.8.5. Identification of Neutrophil Extracellular Traps (NETs)
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Louwers, Y.V.; Laven, J.S.E. Characteristics of Polycystic Ovary Syndrome throughout Life. Ther. Adv. Reprod. Health 2020, 14, 263349412091103. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Health, N.; Public, M.; Health, M.; et al. Recomendaciones de La Guía Internacional Basada En La Evidencia Para La Evaluación y El Tratamiento Del Síndrome de Ovario Poliquístico. Health Hum. Serv. 2018, 110, 364–379. [Google Scholar] [CrossRef]
- Righi, G.M.; Ferreira De Oliveira, T.; Cândida, M.; Baracat, P.; Mayumi, G.; Rua, R.; Schmidt, I.; Amaro, S.; Paulo, S. Síndrome Dos Ovários Policísticos e Sua Relação Com a Microbiota Intestinal Polycystic Ovary Syndrome and Its Relationship with the Intestinal Microbiota. Femina 2021, 49, 631–635. [Google Scholar]
- Mora Agüero, S.d.l.Á. Microbiota y Disbiosis Vaginal. Rev. Medica Sinerg. 2019, 4, 3–13. [Google Scholar] [CrossRef]
- Jin, C.; Qin, L.; Liu, Z.; Li, X.; Gao, X.; Cao, Y.; Zhao, S.; Wang, J.; Han, T.; Yan, L.; et al. Comparative Analysis of the Vaginal Microbiome of Healthy and Polycystic Ovary Syndrome Women: A Large Cross-Sectional Study. Reprod. Biomed. Online 2023, 46, 1005–1016. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.; Wojtowicz, M.; Baranski, K.; Galczynska, D.; Daniluk, J.; Pluta, D. The Correlation of Vitamin D Level with Body Mass Index in Women with Polycystic Ovary Syndrome. Ginekol. Pol. 2023, 94, 883–888. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O.C. Female Gut and Genital Tract Microbiota-Induced Crosstalk and Differential Effects of Short-Chain Fatty Acids on Immune Sequelae. Front. Immunol. 2020, 11, 553047. [Google Scholar] [CrossRef]
- Tu, Y.; Zheng, G.; Ding, G.; Wu, Y.; Xi, J.; Ge, Y.; Gu, H.; Wang, Y.; Sheng, J.; Liu, X.; et al. Comparative Analysis of Lower Genital Tract Microbiome Between PCOS and Healthy Women. Front. Physiol. 2020, 11, 563753. [Google Scholar] [CrossRef]
- Leliefeld, P.H.C.; Koenderman, L.; Pillay, J. How Neutrophils Shape Adaptive Immune Responses. Front. Immunol. 2015, 6, 160811. [Google Scholar] [CrossRef]
- Zawrotniak, M.; Rapala-Kozik, M. Neutrophil Extracellular Traps (NETs)-Formation and Implications. Acta Biochim. Pol. 2013, 60, 277–284. [Google Scholar] [CrossRef]
- Mortaz, E.; Alipoor, S.D.; Adcock, I.M.; Mumby, S.; Koenderman, L. Update on Neutrophil Function in Severe Inflammation. Front. Immunol. 2018, 9, 411381. [Google Scholar] [CrossRef]
- Papayannopoulos, V. Neutrophil Extracellular Traps in Immunity and Disease. Nat. Rev. Immunol. 2018, 18, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Torres, P.J.; Siakowska, M.; Banaszewska, B.; Pawelczyk, L.; Duleba, A.J.; Kelley, S.T.; Thackray, V.G. Gut Microbial Diversity in Women with Polycystic Ovary Syndrome Correlates with Hyperandrogenism. J. Clin. Endocrinol. Metab. 2018, 103, 1502–1511. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Shao, J.; Yang, Y.; Niu, X.; Liao, J.; Zhao, Q.; Wang, D.; Li, S.; Hu, J. Gut Microbiota in Patients with Polycystic Ovary Syndrome: A Systematic Review. Reprod. Sci. 2022, 29, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Di, N.; Li, L.; Yang, D. Gut Microbiota Alterations Reveal Potential Gut–Brain Axis Changes in Polycystic Ovary Syndrome. J. Endocrinol. Investig. 2021, 44, 1727–1737. [Google Scholar] [CrossRef] [PubMed]
- Saucedo de la Llata, E.; Moraga Sánchez, M.R.; Menchón López, M.; Obed Carmona Ruiz, I. Vaginosis Bacteriana y Candidiasis Vaginal: Análisis de Una Nueva Alternativa Terapéutica. Rev. Iberoam. Fertil. Reprod. Hum. 2020, 37, 1–7. [Google Scholar]
- Hong, X.; Qin, P.; Yin, J.; Shi, Y.; Xuan, Y.; Chen, Z.; Zhou, X.; Yu, H.; Peng, D.; Wang, B. Clinical Manifestations of Polycystic Ovary Syndrome and Associations with the Vaginal Microbiome: A Cross-Sectional Based Exploratory Study. Front. Endocrinol. 2021, 12, 662725. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Flores, A.E.; Luque-Ramírez, M.; Escobar-Morreale, H.F. Polycystic Ovary Syndrome in Adult Women. Med. Clin. 2019, 152, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Burgener-Kairuz, P.; Zuber, J.P.; Jaunin, P.; Buchman, T.G.; Bille, J.; Rossier, M. Rapid Detection and Identification of Candida Albicans and Torulopsis (Candida) Glabrata in Clinical Specimens by Species-Specific Nested PCR Amplification of a Cytochrome P-450 Lanosterol-α-Demethylase (L1A1) Gene Fragment. J. Clin. Microbiol. 1994, 32, 1902–1907. [Google Scholar] [CrossRef]
- Pačes, J.; Urbánková, V.; Urbánek, P. Cloning and Characterization of a Repetitive DNA Sequence Specific for Trichomonas Vaginalis. Mol. Biochem. Parasitol. 1992, 54, 247–255. [Google Scholar] [CrossRef]
- Zariffard, M.R.; Saifuddin, M.; Sha, B.E.; Spear, G.T. Detection of Bacterial Vaginosis-Related Organisms by Real-Time PCR for Lactobacilli, Gardnerella Vaginalis and Mycoplasma Hominis. FEMS Immunol. Med. Microbiol. 2002, 34, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Fredricks, D.N.; Fiedler, T.L.; Thomas, K.K.; Oakley, B.B.; Marrazzo, J.M. Targeted PCR for Detection of Vaginal Bacteria Associated with Bacterial Vaginosis. J. Clin. Microbiol. 2007, 45, 3270–3276. [Google Scholar] [CrossRef] [PubMed]
- Monroy, V.S.; Mata, A.E.T.; Magdaleno, J.D.A.V. Diagnóstico de Infección Por Chlamydia Trachomatis Mediante PCR En Pacientes Que Acuden a La Clínica de Especialidades de La Mujer de La Secretaría de La Defensa Nacional. Ginecol. Obstet. Mex. 2009, 77, 13–18. [Google Scholar]
- Palaoro, L.B. Manual de Procedimiento Bacova Erige; Prosar: Segunda, Argentina, 2018. [Google Scholar]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of Diagnosing Bacterial Vaginosis Is Improved by a Standardized Method of Gram Stain Interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef]
- Gu, Y.; Zhou, G.; Zhou, F.; Li, Y.; Wu, Q.; He, H.; Zhang, Y.; Ma, C.; Ding, J.; Hua, K. Gut and Vaginal Microbiomes in PCOS: Implications for Women’s Health. Front. Endocrinol. 2022, 13, 808508. [Google Scholar] [CrossRef] [PubMed]
- Clabaut, M.; Suet, A.; Racine, P.J.; Tahrioui, A.; Verdon, J.; Barreau, M.; Maillot, O.; Le Tirant, A.; Karsybayeva, M.; Kremser, C.; et al. Effect of 17β-Estradiol on a Human Vaginal Lactobacillus Crispatus Strain. Sci. Rep. 2021, 11, 7133. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Qin, P.; Huang, K.; Ding, X.; Ma, J.; Xuan, Y.; Zhu, X.; Peng, D.; Wang, B. Association between Polycystic Ovary Syndrome and the Vaginal Microbiome: A Case-Control Study. Clin. Endocrinol. 2020, 93, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Kraut, R.; Carvallo, F.D.; Golonka, R.; Campbell, S.M.; Rehmani, A.; Babenko, O.; Lee, M.C.; Vieira-Baptista, P. Scoping Review of Cytolytic Vaginosis Literature. PLoS ONE 2023, 18, e0280954. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, F.; Melo, A.; Rivera-Concha, R.; Schulz, M.; Uribe, P.; Fonseca-Salamanca, F.; Ossa, X.; Taubert, A.; Hermosilla, C.; Sánchez, R. High Presence of NETotic Cells and Neutrophil Extracellular Traps in Vaginal Discharges of Women with Vaginitis: An Exploratory Study. Cells 2022, 11, 3185. [Google Scholar] [CrossRef]
- Papayannopoulos, V.; Metzler, K.D.; Hakkim, A.; Zychlinsky, A. Neutrophil Elastase and Myeloperoxidase Regulate the Formation of Neutrophil Extracellular Traps. J. Cell Biol. 2010, 191, 677–691. [Google Scholar] [CrossRef]
- Lu, C.; Wang, H.; Yang, J.; Zhang, X.; Chen, Y.; Feng, R.; Qian, Y. Changes in Vaginal Microbiome Diversity in Women with Polycystic Ovary Syndrome. Front. Cell. Infect. Microbiol. 2021, 11, 1–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Micro-Organism | Primers | Sequence 5′-3′ | Fragment Base Pairs | Reference | GenBank |
|---|---|---|---|---|---|
| Chlamydia trachomatis | Forward | tccggagcgagttacgaaga | 241 | Sánchez V. 2009 [23] | NZ_CP009926.1 |
| Reverse | aatcaatgcccgggattggt | ||||
| Candida albicans | Forward | atgggtggtcaacatac tacatctatgtctaccacc | 496 | Burgener-kairuz 1994 [19] | X13296.1 |
| Reverse | |||||
| Trichomonas vaginalis | Forward | attgtcgaacattggtcttaccctc | 262 | Pačes J, 1992 [20] | L23861.1 |
| Reverse | tctgtgccgtcttcaagtatgc | ||||
| Gardnerella vaginalis | Forward | gcgggctagagtgca acccgtggaatgggcc | 206 | Zariffard MR, 2002 [21] | GenBank: AY738665.1 |
| Reverse | |||||
| Atopobium vaginae | Forward | gcagggacgaggccgcaa | 558 | Fredricks D. 2007 [22] | AY738657.1 |
| Reverse | gtgtttccactgcttcacctaa | ||||
| Megasphaera phylotype 1 | Forward | gatgccaacagtatccgtccg | 144 | Fredricks D. 2007 [22] | AY738672.1 |
| Reverse | Acagacttaccgaaccgcct |
| BVS in Women’s Childbearing Age | NV | VIR |
|---|---|---|
| I Normal microbiota Predominance of Lactobacilli | 0–3 | No |
| II Normal microbiota + VIR Predominance of Lactobacilli with vaginal inflammatory reaction present. | 0–3 | Yes |
| III Intermediate microbiota Equilibrium of Lactobacilli and anaerobic Bacteria | 4–6 | No |
| IV Bacterial vaginosis Predominance of anaerobic bacteria | 7–10 | No |
| V Nonspecific Microbial Vaginitis Alteration of the ratio of Lactobacilli and anaerobic bacteria, or presence of foreign bacterial morphotypes with inflammatory reaction. | 4–10 | Yes |
| Vaginal Microbiota (%) | |||||
|---|---|---|---|---|---|
| Variables | n | Normal | Altered | OR (IC) | p-Value |
| Phenotypes | 2.29(0.50; 10.50) | 0.283 | |||
| A and B | 21(63.6) | 5(23.8) | 16(76.2) | ||
| C and D | 12(36.4) | 5(41.7) | 7(58.3) | ||
| Age of onset of sexual intercourse (years) | 0.27(0.04; 1.57) | 0.133 | |||
| ≤18 | 20(60.6) | 8(40.0) | 12(60.0) | ||
| >18 | 13(39.4) | 2(15.4) | 11(84.6) | ||
| Number of sexual partners | 0.35(0.06; 2.15) | 0.246 | |||
| None | 6(18.18) | 3(50.0) | 3(50.0) | ||
| More than 1 sexual partner | 27(81.82) | 7(25.93) | 20(74.07) | ||
| Active STI | 6.68(1.18; 37.78) | * 0.023 | |||
| Yes | 25(75.8) | 5(20.0) | 20(80.0) | ||
| No | 8(24.2) | 5(62.5) | 3(37.5) | ||
| Oral contraceptives use | 0.47(0.10; 2.27) | 0.341 | |||
| Yes | 19(57.6) | 7(36.8) | 12(63.2) | ||
| No | 14(42.4) | 3(21.4) | 11(78.5) | ||
| Oligomenorrhea | 2.86(0.46; 17.58) | 0.246 | |||
| Yes | 27(81.8) | 7(25.9) | 20(74.1) | ||
| No | 6(18.2) | 3(50.0) | 3(50.0) | ||
| Vaginal Microbiota (%) | |||||
|---|---|---|---|---|---|
| Hormonal Variables | N | Normal | Altered | OR (IC) | p-Value |
| HOMA | 0.52(0.10; 2.60) | 0.429 | |||
| Normal | 12(40.0) | 5(25.0) | 9(75.0) | ||
| Altered | 18(60.0) | 7(38.9) | 7(61.1) | ||
| Insulin | _ | 0.002 | |||
| Normal | 26(86.7) | 6(23.1) | 20(76.9) | ||
| Altered | 4(15.3) | 4(100.0) | _ | ||
| Total Testosterone | 0.28(0.06; 0.35) | 0.103 | |||
| Normal | 16(48.5) | 7(43.8) | 9(56.3) | ||
| Altered | 17(51.5) | 3(17.6) | 14(82.4) | ||
| DHEAS | _ | 0.220 | |||
| Normal | 26(89.7) | 9(34.6) | 17(65.4) | ||
| Altered | 3(10.3) | - | 3(100.0) | ||
| 17-OH progesterone | 2.22(0.43; 11.6) | 0.339 | |||
| Normal | 15(53.6) | 6(40.0) | 9(60.0) | ||
| Altered | 13(46.4) | 3(23.1) | 10(76.9) | ||
| Androstenedione | 1.07(0.2; 5.7) | 0.930 | |||
| Normal | 20(69.0) | 7(35.0) | 13(65.0) | ||
| Altered | 9(31.0) | 3(33.3) | 6(66.7) | ||
| LH | 1.36(0.29; 6.28) | 0.690 | |||
| Normal | 17(54,8) | 6(35.3) | 11(64.7) | ||
| Altered | 14(45.2) | 4(28.6) | 10(71.4) | ||
| AMH | 2.42(0.13; 44.50) | 0.540 | |||
| Normal | 2(7.7) | 1(50.0) | 1(50.0) | ||
| Altered | 24(92.3) | 7(29.2) | 17(70.8) | ||
| Vitamin D | 0.23(0.03; 2.61) | 0.234 | |||
| Normal | 20(71.4) | 7(35.0) | 13(65.0) | ||
| Altered | 8(28.6) | 1(12.5) | 7(87.5) | ||
| Proinflammatory State (%) | ||||
|---|---|---|---|---|
| Vaginal Microbiota | n (%) | Absent | Present | p-Value |
| Normal | 10(30.3) | 0 | 10(100.0) | * 0.021 |
| Altered | 23(33.3) | 9(39.1) | 14(60.9) | |
| Total | 33(100.0) | 9(27.3) | 24(72.7) | |
| Cases with VIR | Phenotypes | Proinflammatory State | Vaginal Microbiota |
|---|---|---|---|
| 1 | D | Scarce | MN |
| 2 | A | Intense | nMVitis |
| 3 | D | Intense | nMVitis |
| 4 | A | Moderate | nMVitis |
| 5 | A | Moderate | nMVitis |
| 6 | C | Intense | nMVitis |
| 7 | A | Absent | nMVitis |
| 8 | A | Intense | nMVitis |
| Micro-Organisms | PCR Results | |
|---|---|---|
| Positive | Negative | |
| Gardnerella vaginalis | 22(66.7) | 11(33.3) |
| Atopobium vaginae | 10(30.3) | 23(69.7) |
| Megasphaera type 1 | 4(12.1) | 29(87.9) |
| Trichomonas vaginalis | 0 | 0 |
| Chlamydia trachomatis | 2(6.1) | 31(93.9) |
| Candida albicans | 4(12.1) | 29(87.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espinosa, M.E.; Melo, A.; Leon, M.; Bautista-Valarezo, E.; Zambrano, F.; Uribe, P.; Bravo, A.; Taubert, A.; Hermosilla, C.; Iturrieta, V.; et al. Vaginal Microbiota and Proinflammatory Status in Patients with Polycystic Ovary Syndrome: An Exploratory Study. J. Clin. Med. 2024, 13, 2278. https://doi.org/10.3390/jcm13082278
Espinosa ME, Melo A, Leon M, Bautista-Valarezo E, Zambrano F, Uribe P, Bravo A, Taubert A, Hermosilla C, Iturrieta V, et al. Vaginal Microbiota and Proinflammatory Status in Patients with Polycystic Ovary Syndrome: An Exploratory Study. Journal of Clinical Medicine. 2024; 13(8):2278. https://doi.org/10.3390/jcm13082278
Chicago/Turabian StyleEspinosa, María Elena, Angélica Melo, Marion Leon, Estefanía Bautista-Valarezo, Fabiola Zambrano, Pamela Uribe, Anita Bravo, Anja Taubert, Carlos Hermosilla, Virginia Iturrieta, and et al. 2024. "Vaginal Microbiota and Proinflammatory Status in Patients with Polycystic Ovary Syndrome: An Exploratory Study" Journal of Clinical Medicine 13, no. 8: 2278. https://doi.org/10.3390/jcm13082278
APA StyleEspinosa, M. E., Melo, A., Leon, M., Bautista-Valarezo, E., Zambrano, F., Uribe, P., Bravo, A., Taubert, A., Hermosilla, C., Iturrieta, V., & Sánchez, R. (2024). Vaginal Microbiota and Proinflammatory Status in Patients with Polycystic Ovary Syndrome: An Exploratory Study. Journal of Clinical Medicine, 13(8), 2278. https://doi.org/10.3390/jcm13082278