
Novel Dental Low-Shrinkage-Stress Composite with Antibacterial Dimethylaminododecyl Methacrylate Monomer
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Formation of Composites Containing Different Mass Fractions of DMADDM
- Heliomolar (designated as “Commercial Control”);
- 30% UV + 0% DMADDM + 70% glass (designated as “Experimental UV control”);
- 28.5% UV + 1.5% DMADDM + 70% glass (designated as “UV + 1.5% DMADDM”);
- 27% UV + 3% DMADDM + 70% glass (designated as “UV + 3% DMADDM”);
- 25% UV + 5% DMADDM + 70% glass (designated as “UV + 5% DMADDM”).
2.2. Mechanical Properties
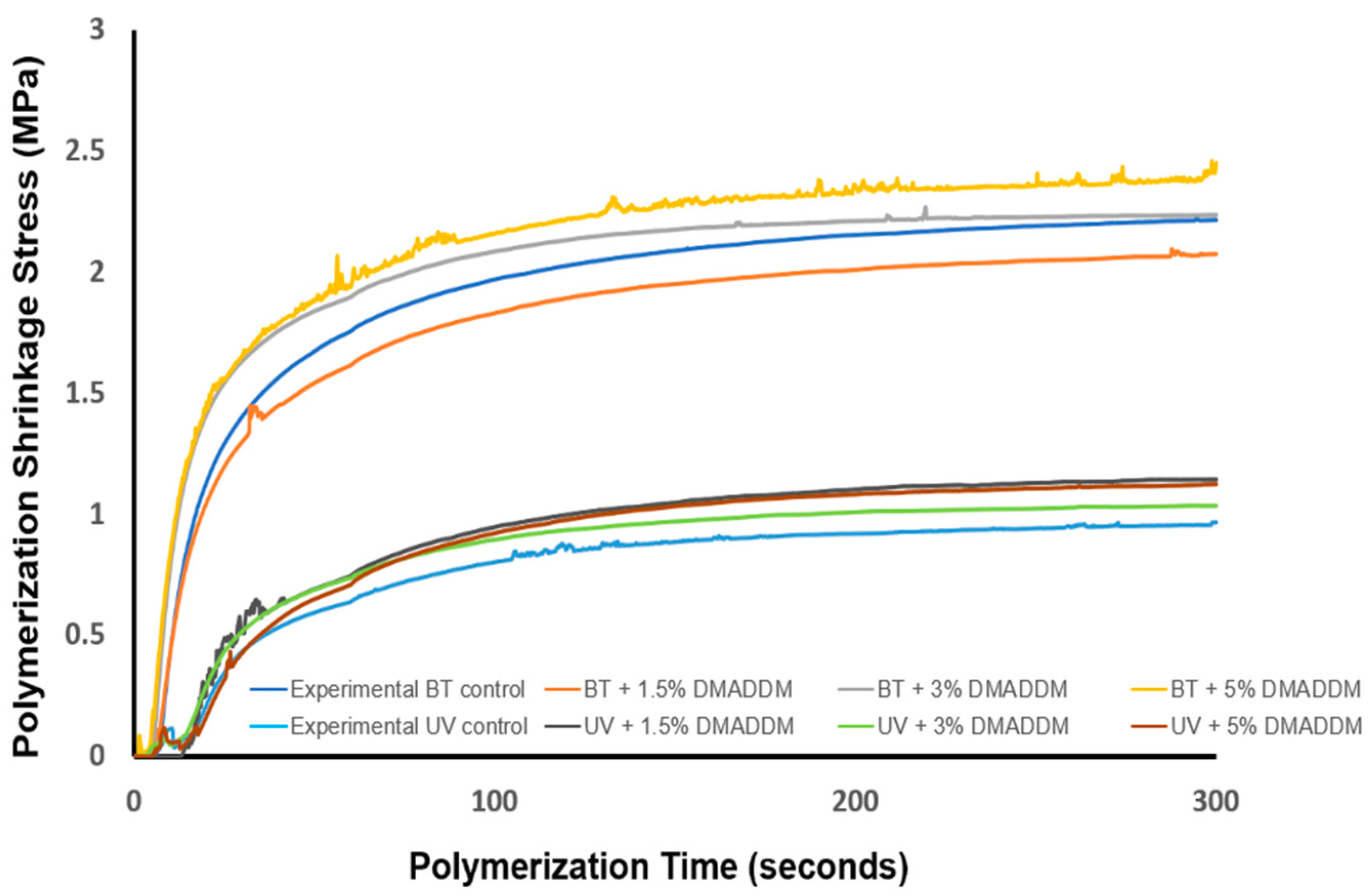
2.3. Polymerization Shrinkage Stress and Degree of Conversion
- (1)
- 30% BT + 70% glass (designated as “Experimental BT control”);
- (2)
- 28.5% BT + 1.5% DMADDM + 70% glass (designated as “BT + 1.5% DMADDM”);
- (3)
- 27% BT + 3% DMADDM + 70% glass (designated as “BT + 3% DMADDM”);
- (4)
- 25% BT + 5% DMADDM + 70% glass (designated as “BT + 5% DMADDM”);
- (5)
- 30% UV + 70% glass (designated as “Experimental UV control”);
- (6)
- 28.5% UV + 1.5% DMADDM + 70% glass (designated as “UV + 1.5% DMADDM”);
- (7)
- 27% UV + 3% DMADDM + 70% glass (designated as “UV + 3% DMADDM”);
- (8)
- 25% UV + 5% DMADDM + 70% glass (designated as “UV + 5% DMADDM”).
2.4. Streptococcus mutans (S. mutans) Biofilm Model
2.4.1. Composite Samples for Biofilm Testing
2.4.2. Bacteria Inoculation and Biofilm Formation
2.4.3. Live/Dead Staining of Biofilms
2.4.4. Biofilm Colony-Forming Units Counts
2.4.5. Biofilm Metabolic Activity
2.4.6. Lactic Acid Production by Biofilms
2.4.7. Scanning Electron Microscopy (SEM)
2.5. Statistical Analysis
3. Results
3.1. Mechanical Properties
3.2. Polymerization Shrinkage Stress and Degree of Conversion
3.3. Live/dead Staining of S. mutans Biofilms
3.4. Biofilm Colony-Forming Units Counts
3.5. MTT Assay of Metabolic Activity of S. mutans Biofilms
3.6. Lactic Acid Production by S. mutans Biofilms
3.7. SEM Examination of Composites and Biofilms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bayne, S.C.; Ferracane, J.L.; Marshall, G.W.; Marshall, S.J.; van Noort, R. The Evolution of Dental Materials over the Past Century: Silver and Gold to Tooth Color and Beyond. J. Dent. Res. 2019, 98, 257–265. [Google Scholar] [CrossRef]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J.M. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef]
- Braga, R.; Ballester, R.; Ferracane, J. Factors involved in the development of polymerization shrinkage stress in resin-composites: A systematic review. Dent. Mater. 2005, 21, 962–970. [Google Scholar] [CrossRef]
- Soares, C.J.; Faria-E-Silva, A.L.; Rodrigues, M.D.P.; Vilela, A.B.F.; Pfeifer, C.S.; Tantbirojn, D.; Versluis, A. Polymerization shrinkage stress of composite resins and resin cements–What do we need to know? Braz. Oral Res. 2017, 31, e62. [Google Scholar] [CrossRef]
- Pereira, R.; Valdívia, A.; Bicalho, A.; Franco, S.; Tantbirojn, D.; Versluis, A.; Soares, C. Effect of Photoactivation Timing on the Mechanical Properties of Resin Cements and Bond Strength of Fiberglass Post to Root Dentin. Oper. Dent. 2015, 40, E206–E221. [Google Scholar] [CrossRef]
- Bicalho, A.; Pereira, R.; Zanatta, R.; Franco, S.; Tantbirojn, D.; Versluis, A.; Soares, C. Incremental Filling Technique and Composite Material—Part I: Cuspal Deformation, Bond Strength, and Physical Properties. Oper. Dent. 2014, 39, e71–e82. [Google Scholar] [CrossRef] [PubMed]
- Bicalho, A.; Valdívia, A.; Barreto, B.; Tantbirojn, D.; Versluis, A.; Soares, C. Incremental Filling Technique and Composite Material—Part II: Shrinkage and Shrinkage Stresses. Oper. Dent. 2014, 39, e83–e92. [Google Scholar] [CrossRef] [PubMed]
- Rosatto, C.; Bicalho, A.; Veríssimo, C.; Bragança, G.; Rodrigues, M.; Tantbirojn, D.; Versluis, A.; Soares, C. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J. Dent. 2015, 43, 1519–1528. [Google Scholar] [CrossRef]
- Soares, C.; Bicalho, A.; Verissimo, C.; Soares, P.; Tantbirojn, D.; Versluis, A. Delayed Photo-activation Effects on Mechanical Properties of Dual Cured Resin Cements and Finite Element Analysis of Shrinkage Stresses in Teeth Restored With Ceramic Inlays. Oper. Dent. 2016, 41, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Balhaddad, A.; Garcia, I.; Mokeem, L.; Ibrahim, M.; Collares, F.; Weir, M.; Xu, H.; Melo, M. Bifunctional Composites for Biofilms Modulation on Cervical Restorations. J. Dent. Res. 2021, 100, 1063–1071. [Google Scholar] [CrossRef]
- Moraes, R.R.; Garcia, J.W.; Barros, M.D.; Lewis, S.H.; Pfeifer, C.S.; Liu, J.; Stansbury, J.W. Control of polymerization shrinkage and stress in nanogel-modified monomer and composite materials. Dent. Mater. 2011, 27, 509–519. [Google Scholar] [CrossRef]
- Shah, P.K.; Stansbury, J.W. Photopolymerization shrinkage-stress reduction in polymer-based dental restoratives by surface modification of fillers. Dent. Mater. 2021, 37, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.-H.; Chen, R.-S.; Chang, Y.-L.; Chen, M.-H.; Cheng, K.-C.; Su, W.-F. Biphenyl liquid crystalline epoxy resin as a low-shrinkage resin-based dental restorative nanocomposite. Acta Biomater. 2012, 8, 4151–4161. [Google Scholar] [CrossRef] [PubMed]
- Arrais, C.A.G.; De Oliveira, M.T.; Mettenburg, D.; Rueggeberg, F.; Giannini, M. Silorane- and high filled-based"low-shrinkage" resin composites: Shrinkage, flexural strength and modulus. Braz. Oral Res. 2013, 27, 97–102. [Google Scholar] [CrossRef]
- Lu, H.; Carioscia, J.A.; Stansbury, J.W.; Bowman, C.N. Investigations of step-growth thiol-ene polymerizations for novel dental restoratives. Dent. Mater. 2005, 21, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Urbas, A.; Gonzalez-Bonet, A.; Sheridan, R.J.; Seppala, J.E.; Beers, K.L.; Sun, J. A composition-controlled cross-linking resin network through rapid visible-light photo-copolymerization. Polym. Chem. 2016, 7, 5023–5030. [Google Scholar] [CrossRef]
- Wang, X.; Huyang, G.; Palagummi, S.V.; Liu, X.; Skrtic, D.; Beauchamp, C.; Bowen, R.; Sun, J. High performance dental resin composites with hydrolytically stable monomers. Dent. Mater. 2018, 34, 228–237. [Google Scholar] [CrossRef]
- Yamauchi, S.; Wang, X.; Egusa, H.; Sun, J. High-Performance Dental Adhesives Containing an Ether-Based Monomer. J. Dent. Res. 2020, 99, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Zhang, K.; Zhang, N.; Melo, M.; Weir, M.; Zhou, X.; Bai, Y.; Reynolds, M.; Xu, H. Developing a New Generation of Antimicrobial and Bioactive Dental Resins. J. Dent. Res. 2017, 96, 855–863. [Google Scholar] [CrossRef]
- Han, Q.; Li, B.; Zhou, X.; Ge, Y.; Wang, S.; Li, M.; Ren, B.; Wang, H.; Zhang, K.; Xu, H.H.K.; et al. Anti-Caries Effects of Dental Adhesives Containing Quaternary Ammonium Methacrylates with Different Chain Lengths. Materials 2017, 10, 643. [Google Scholar] [CrossRef]
- Li, F.; Weir, M.D.; Xu, H.H.K. Effects of quaternary ammonium chain length on antibacterial bonding agents. J. Dent. Res. 2013, 92, 932–938. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, F.J.D.; Filho, P.S.F.d.S.; Costa, M.J.F.; Caldas, M.R.G.R.; Borges, B.C.D.; de Araújo, D.F.G. A comprehensive review of the antibacterial activity of dimethylaminohexadecyl methacrylate (DMAHDM) and its influence on mechanical properties of resin-based dental materials. Jpn. Dent. Sci. Rev. 2021, 57, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Balhaddad, A.A.; Ibrahim, M.S.; Weir, M.D.; Xu, H.H.; Melo, M.A.S. Concentration dependence of quaternary ammonium monomer on the design of high-performance bioactive composite for root caries restorations. Dent. Mater. 2020, 36, e266–e278. [Google Scholar] [CrossRef] [PubMed]
- Bhadila, G.; Menon, D.; Wang, X.; Vila, T.; Melo, M.A.S.; Montaner, S.; Arola, D.D.; Weir, M.D.; Sun, J.K.; Xu, H.H.; et al. Long-term antibacterial activity and cytocompatibility of novel low-shrinkage-stress, remineralizing composites. J. Biomater. Sci. Polym. Ed. 2021, 32, 886–905. [Google Scholar] [CrossRef]
- Namba, N.; Yoshida, Y.; Nagaoka, N.; Takashima, S.; Matsuura-Yoshimoto, K.; Maeda, H.; Van Meerbeek, B.; Suzuki, K.; Takashiba, S. Antibacterial effect of bactericide immobilized in resin matrix. Dent. Mater. 2009, 25, 424–430. [Google Scholar] [CrossRef]
- Cheng, L.; Weir, M.D.; Zhang, K.; Arola, D.D.; Zhou, X.; Xu, H.H. Dental primer and adhesive containing a new antibacterial quaternary ammonium monomer dimethylaminododecyl methacrylate. J. Dent. 2013, 41, 345–355. [Google Scholar] [CrossRef]
- Zhou, C.; Weir, M.D.; Zhang, K.; Deng, D.; Cheng, L.; Xu, H.H. Synthesis of new antibacterial quaternary ammonium monomer for incorporation into CaP nanocomposite. Dent. Mater. 2013, 29, 859–870. [Google Scholar] [CrossRef]
- Zhang, K.; Ren, B.; Zhou, X.; Xu, H.H.K.; Chen, Y.; Han, Q.; Li, B.; Weir, M.D.; Li, M.; Feng, M.; et al. Effect of Antimicrobial Denture Base Resin on Multi-Species Biofilm Formation. Int. J. Mol. Sci. 2016, 17, 1033. [Google Scholar] [CrossRef]
- Li, B.; Ge, Y.; Wu, Y.; Chen, J.; Xu, H.H.K.; Yang, M.; Li, M.; Ren, B.; Feng, M.; Weir, M.D.; et al. Anti-Bacterial and Microecosystem-Regulating Effects of Dental Implant Coated with Dimethylaminododecyl Methacrylate. Molecules 2017, 22, 2013. [Google Scholar] [CrossRef]
- Bhadila, G.; Wang, X.; Zhou, W.; Menon, D.; Melo, M.A.S.; Montaner, S.; Oates, T.W.; Weir, M.D.; Sun, J.; Xu, H.H. Novel low-shrinkage-stress nanocomposite with remineralization and antibacterial abilities to protect marginal enamel under biofilm. J. Dent. 2020, 99, 103406. [Google Scholar] [CrossRef]
- Ferracane, J.L. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent. Mater. 2005, 21, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Filemban, H.; Bhadila, G.; Wang, X.; Melo, M.A.S.; Oates, T.W.; Weir, M.D.; Sun, J.; Xu, H.H. Novel low-shrinkage-stress bioactive nanocomposite with anti-biofilm and remineralization capabilities to inhibit caries. J. Dent. Sci. 2021, 17, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Weir, M.D.; Cheng, L.; Lin, N.J.; Lin-Gibson, S.; Chow, L.C.; Zhou, X.; Xu, H.H. Antibacterial activity and ion release of bonding agent containing amorphous calcium phosphate nanoparticles. Dent. Mater. 2014, 30, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Bhadila, G.; Wang, X.; Weir, M.D.; Melo, M.A.S.; Martinho, F.; Fay, G.G.; Oates, T.W.; Sun, J.; Xu, H.H.K. Low-shrinkage-stress nanocomposite: An insight into shrinkage stress, antibacterial, and ion release properties. J. Biomed. Mater. Res. Part B Appl. Biomater. 2021, 109, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Antonucci, J.M.; Zeiger, D.N.; Tang, K.; Lin-Gibson, S.; Fowler, B.O.; Lin, N.J. Synthesis and characterization of dimethacrylates containing quaternary ammonium functionalities for dental applications. Dent. Mater. 2012, 28, 219–228. [Google Scholar] [CrossRef]
- Cheng, L.; Weir, M.D.; Xu, H.H.; Antonucci, J.M.; Kraigsley, A.M.; Lin, N.J.; Lin-Gibson, S.; Zhou, X. Antibacterial amorphous calcium phosphate nanocomposites with a quaternary ammonium dimethacrylate and silver nanoparticles. Dent. Mater. 2012, 28, 561–572. [Google Scholar] [CrossRef]
- Xu, H.H.; Moreau, J.L.; Sun, L.; Chow, L.C. Nanocomposite containing amorphous calcium phosphate nanoparticles for caries inhibition. Dent. Mater. 2011, 27, 762–769. [Google Scholar] [CrossRef]
- Chiang, M.Y.; Giuseppetti, A.A.; Qian, J.; Dunkers, J.P.; Antonucci, J.M.; Schumacher, G.E.; Gibson, S.-L. Analyses of a cantilever-beam based instrument for evaluating the development of polymerization stresses. Dent. Mater. 2011, 27, 899–905. [Google Scholar] [CrossRef]
- Wang, Z.; Landis, F.A.; Giuseppetti, A.A.; Lin-Gibson, S.; Chiang, M.Y. Simultaneous measurement of polymerization stress and curing kinetics for photo-polymerized composites with high filler contents. Dent. Mater. 2014, 30, 1316–1324. [Google Scholar] [CrossRef]
- Bhadila, G.; Baras, B.H.; Weir, M.D.; Wang, H.; Melo, M.A.S.; Hack, G.D.; Bai, Y.; Xu, H.H.K. Novel antibacterial calcium phosphate nanocomposite with long-term ion recharge and re-release to inhibit caries. Dent. Mater. J. 2020, 39, 678–689. [Google Scholar] [CrossRef]
- Wang, L.; Xie, X.; Qi, M.; Weir, M.D.; Reynolds, M.A.; Li, C.; Zhou, C.; Xu, H.H. Effects of single species versus multispecies periodontal biofilms on the antibacterial efficacy of a novel bioactive Class-V nanocomposite. Dent. Mater. 2019, 35, 847–861. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhou, C.; Ren, B.; Li, X.; Weir, M.D.; Masri, R.M.; Oates, T.W.; Cheng, L.; Xu, H.K.H. Formation of persisters in Streptococcus mutans biofilms induced by antibacterial dental monomer. J. Mater. Sci. Mater. Med. 2017, 28, 178. [Google Scholar] [CrossRef] [PubMed]
- Bhadila, G.; Filemban, H.; Wang, X.; Melo, M.A.S.; Arola, D.D.; Tay, F.R.; Oates, T.W.; Weir, M.D.; Sun, J.; Xu, H.H. Bioactive low-shrinkage-stress nanocomposite suppresses S. mutans biofilm and preserves tooth dentin hardness. Acta Biomater. 2020, 114, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Mitwalli, H.; Balhaddad, A.A.; AlSahafi, R.; Oates, T.W.; Melo, M.A.S.; Xu, H.H.K.; Weir, M.D. Novel CaF2 Nanocomposites with Antibacterial Function and Fluoride and Calcium Ion Release to Inhibit Oral Biofilm and Protect Teeth. J. Funct. Biomater. 2020, 11, 56. [Google Scholar] [CrossRef] [PubMed]
- Al-Dulaijan, Y.A.; Cheng, L.; Weir, M.D.; Melo, M.A.S.; Liu, H.; Oates, T.W.; Wang, L.; Xu, H.H. Novel rechargeable calcium phosphate nanocomposite with antibacterial activity to suppress biofilm acids and dental caries. J. Dent. 2018, 72, 44–52. [Google Scholar] [CrossRef]
- Beyth, N.; Domb, A.J.; Weiss, E.I. An in vitro quantitative antibacterial analysis of amalgam and composite resins. J. Dent. 2007, 35, 201–206. [Google Scholar] [CrossRef]
- Beyth, N.; Yudovin-Farber, I.; Bahir, R.; Domb, A.J.; Weiss, E.I. Antibacterial activity of dental composites containing quaternary ammonium polyethylenimine nanoparticles against Streptococcus mutans. Biomaterials 2006, 27, 3995–4002. [Google Scholar] [CrossRef]
- Carioscia, J.A.; Lu, H.; Stanbury, J.W.; Bowman, C.N. Thiol-ene oligomers as dental restorative materials. Dent. Mater. 2005, 21, 1137–1143. [Google Scholar] [CrossRef]
- He, J.; Cai, L.; Chen, Y.; He, Y.; Wang, M.; Tang, J.; Guan, H.; Wang, J.; Peng, X. Antitumor and radiosensitizing effects of SKLB-163, a novel benzothiazole-2-thiol derivative, on nasopharyngeal carcinoma by affecting the RhoGDI/JNK-1 signaling pathway. Radiother. Oncol. 2018, 129, 30–37. [Google Scholar] [CrossRef]
- Kruly, P.; Giannini, M.; Pascotto, R.C.; Tokubo, L.M.; Suga, U.S.G.; Marques, A.D.C.R.; Terada, R.S.S. Meta-analysis of the clinical behavior of posterior direct resin restorations: Low polymerization shrinkage resin in comparison to methacrylate composite resin. PLoS ONE 2018, 13, e0191942. [Google Scholar] [CrossRef]
- Imazato, S.; Ebi, N.; Takahashi, Y.; Kaneko, T.; Ebisu, S.; Russell, R.R.B. Antibacterial activity of bactericide-immobilized filler for resin-based restoratives. Biomaterials 2003, 24, 3605–3609. [Google Scholar] [CrossRef]
- Braga, R.R.; Ferracane, J.L. Contraction stress related to degree of conversion and reaction kinetics. J. Dent. Res. 2002, 81, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Lovell, L.G.; Lu, H.; Elliott, J.E.; Stansbury, J.W.; Bowman, C.N. The effect of cure rate on the mechanical properties of dental resins. Dent. Mater. 2001, 17, 504–511. [Google Scholar] [CrossRef]
- Hansel, C.; Leyhausen, G.; Mai, U.; Geurtsen, W. Effects of Various Resin Composite (Co)monomers and Extracts on Two Caries-associated Micro-organisms in vitro. J. Dent. Res. 1998, 77, 60–67. [Google Scholar] [CrossRef]
- Khalichi, P.; Cvitkovitch, D.; Santerre, J. Effect of composite resin biodegradation products on oral streptococcal growth. Biomaterials 2004, 25, 5467–5472. [Google Scholar] [CrossRef]
- Barbosa, R.P.D.S.; Pereira-Cenci, T.; da Silva, W.M.; Coelho-De-Souza, F.H.; Demarco, F.F.; Cenci, M.S. Effect of cariogenic biofilm challenge on the surface hardness of direct restorative materials in situ. J. Dent. 2012, 40, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Aljabo, A.; Xia, W.; Liaqat, S.; Khan, M.A.; Knowles, J.C.; Ashley, P.; Young, A.M. Conversion, shrinkage, water sorption, flexural strength and modulus of re-mineralizing dental composites. Dent. Mater. 2015, 31, 1279–1289. [Google Scholar] [CrossRef]
- Melo, M.A.; Guedes, S.F.; Xu, H.H.; Rodrigues, L.K. Nanotechnology-based restorative materials for dental caries management. Trends Biotechnol. 2013, 31, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, S.; Cheng, L.; Jiang, Y.; Melo, M.A.S.; Weir, M.D.; Oates, T.W.; Zhou, X.; Xu, H.H. Novel dental composite with capability to suppress cariogenic species and promote non-cariogenic species in oral biofilms. Mater. Sci. Eng. C 2019, 94, 587–596. [Google Scholar] [CrossRef]
- Zhang, K.; Cheng, L.; Wu, E.J.; Weir, M.D.; Bai, Y.; Xu, H.H. Effect of water-ageing on dentine bond strength and anti-biofilm activity of bonding agent containing new monomer dimethylaminododecyl methacrylate. J. Dent. 2013, 41, 504–513. [Google Scholar] [CrossRef]
- Li, F.; Wang, P.; Weir, M.D.; Fouad, A.F.; Xu, H.H. Evaluation of antibacterial and remineralizing nanocomposite and adhesive in rat tooth cavity model. Acta Biomater. 2014, 10, 2804–2813. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composition | Experimental UV Control (Weight %) | UV + 1.5% DMADDM (Weight %) | UV + 3% DMADDM (Weight %) | UV + 5% DMADDM (Weight %) |
|---|---|---|---|---|
| Urethane dimethacrylate (UDMA) | 16.57% | 15.74% | 14.92% | 13.81% |
| Triethylene glycol divinylbenzyl ether (TEG-DVBE) | 13.13% | 12.46% | 11.82% | 10.94% |
| Camphorquinone | 0.06% | 0.06% | 0.06% | 0.06% |
| 4-N, N-dimethylaminobenzoate | 0.24% | 0.24% | 0.24% | 0.24% |
| Dimethylaminododecyl methacrylate (DMADDM) | 0% | 1.5% | 3% | 5% |
| Silanized barium boroaluminosilicate glass particles | 70% | 70% | 70% | 70% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhussein, A.; Alsahafi, R.; Wang, X.; Mitwalli, H.; Filemban, H.; Hack, G.D.; Oates, T.W.; Sun, J.; Weir, M.D.; Xu, H.H.K. Novel Dental Low-Shrinkage-Stress Composite with Antibacterial Dimethylaminododecyl Methacrylate Monomer. J. Funct. Biomater. 2023, 14, 335. https://doi.org/10.3390/jfb14070335
Alhussein A, Alsahafi R, Wang X, Mitwalli H, Filemban H, Hack GD, Oates TW, Sun J, Weir MD, Xu HHK. Novel Dental Low-Shrinkage-Stress Composite with Antibacterial Dimethylaminododecyl Methacrylate Monomer. Journal of Functional Biomaterials. 2023; 14(7):335. https://doi.org/10.3390/jfb14070335
Chicago/Turabian StyleAlhussein, Abdullah, Rashed Alsahafi, Xiaohong Wang, Heba Mitwalli, Hanan Filemban, Gary D. Hack, Thomas W. Oates, Jirun Sun, Michael D. Weir, and Hockin H. K. Xu. 2023. "Novel Dental Low-Shrinkage-Stress Composite with Antibacterial Dimethylaminododecyl Methacrylate Monomer" Journal of Functional Biomaterials 14, no. 7: 335. https://doi.org/10.3390/jfb14070335