
Revisiting the Checkerboard to Inform Development of β-Lactam/β-Lactamase Inhibitor Combinations


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
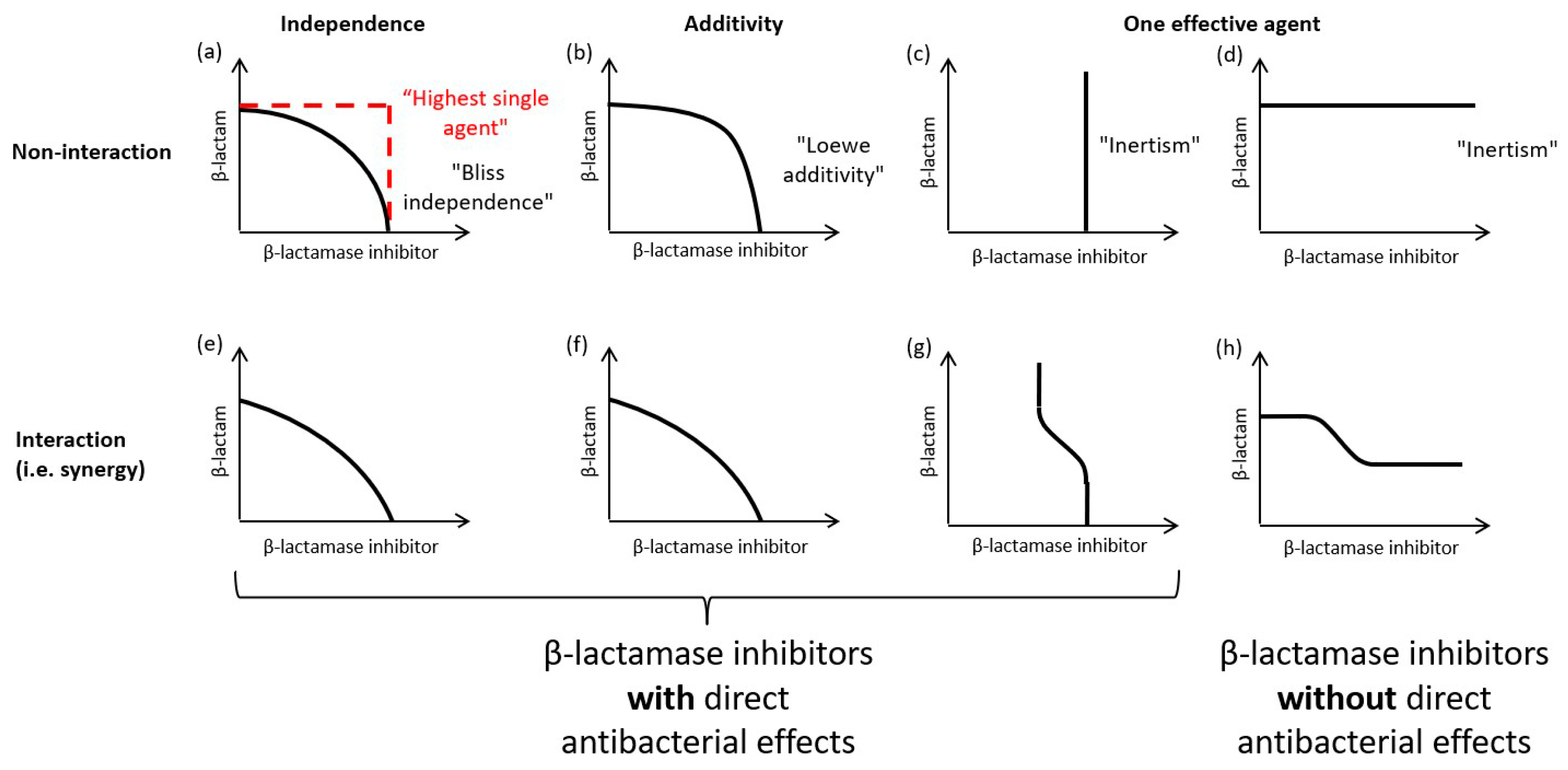
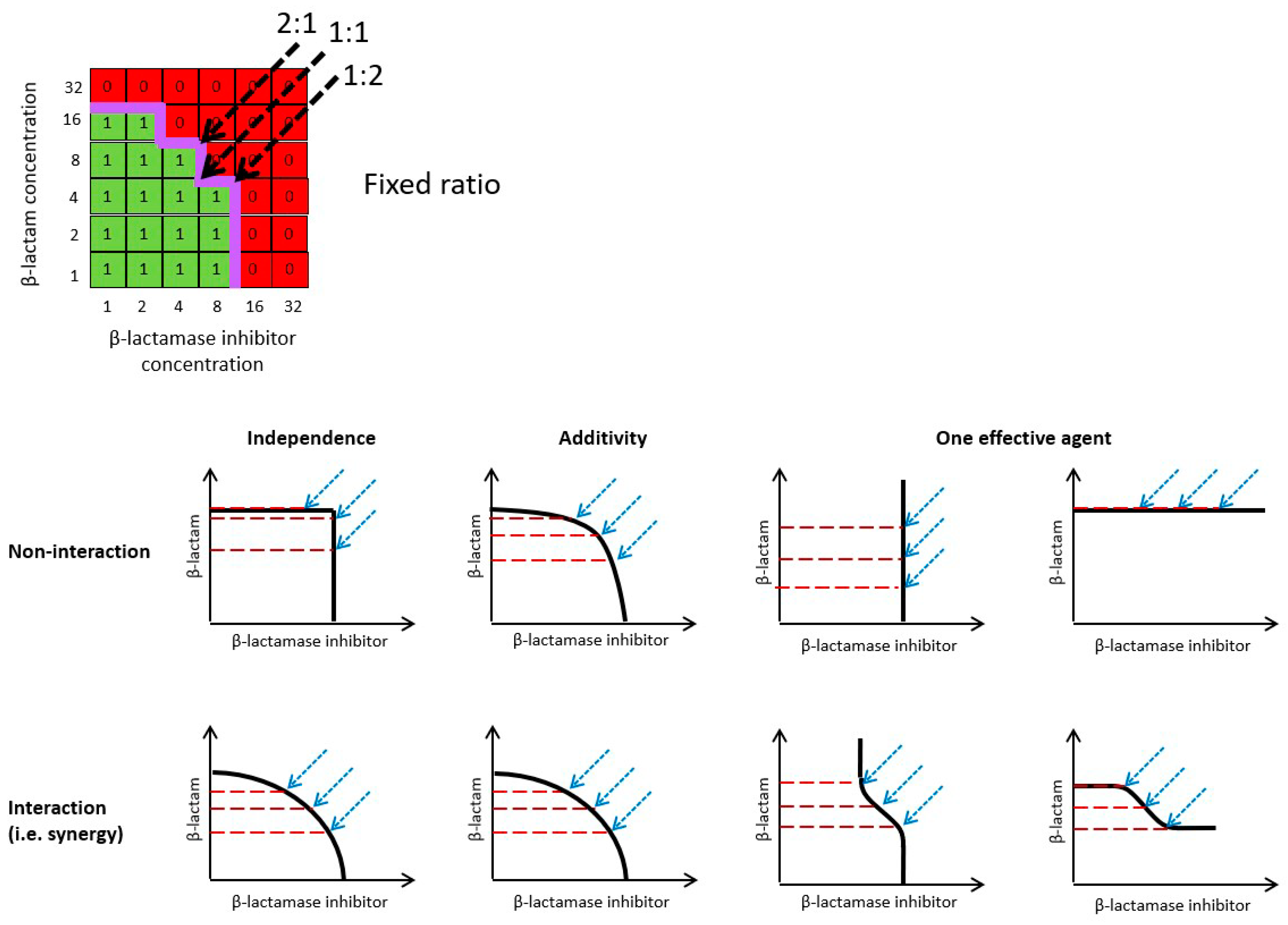
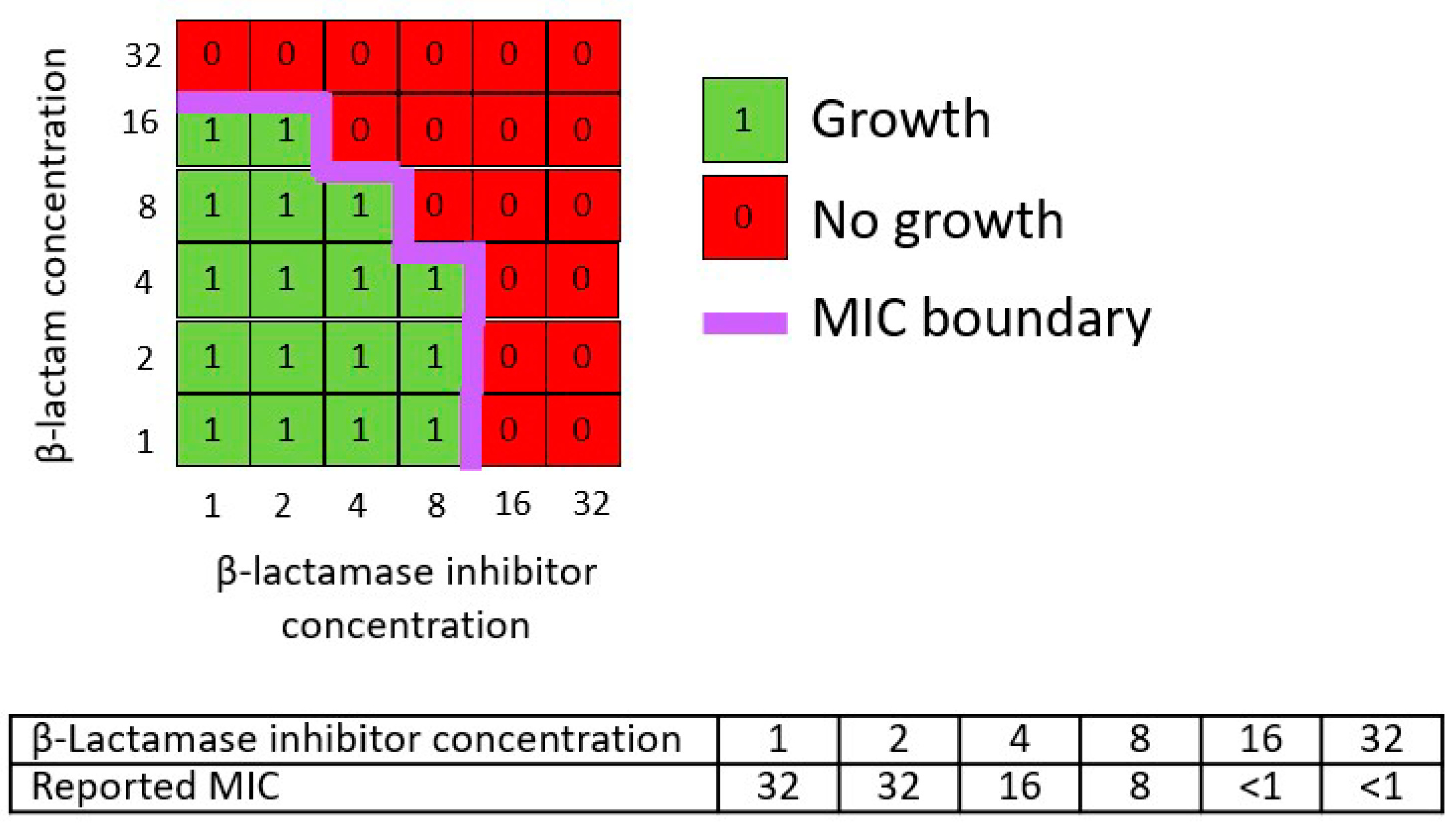
2.1. Representation of Checkerboard Data and Combination Response Models
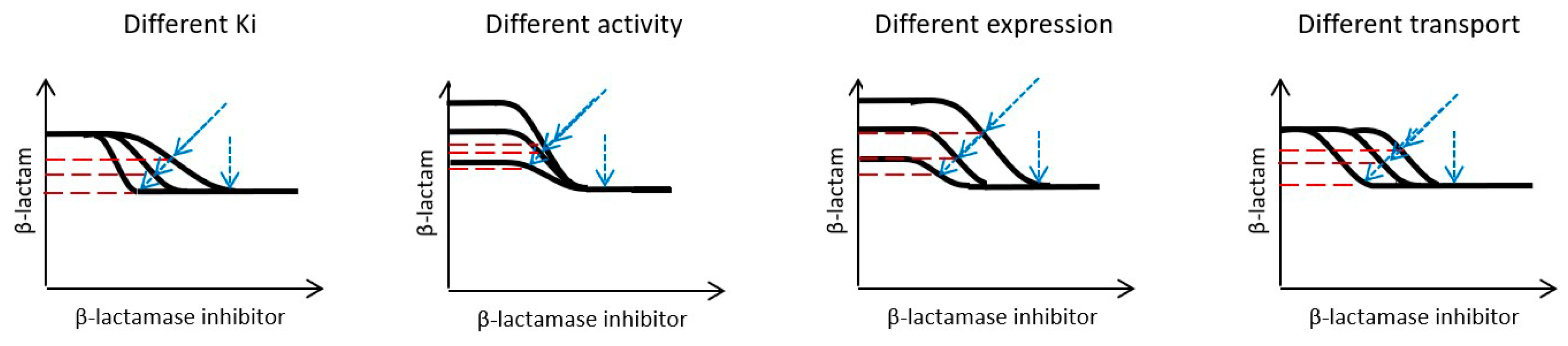
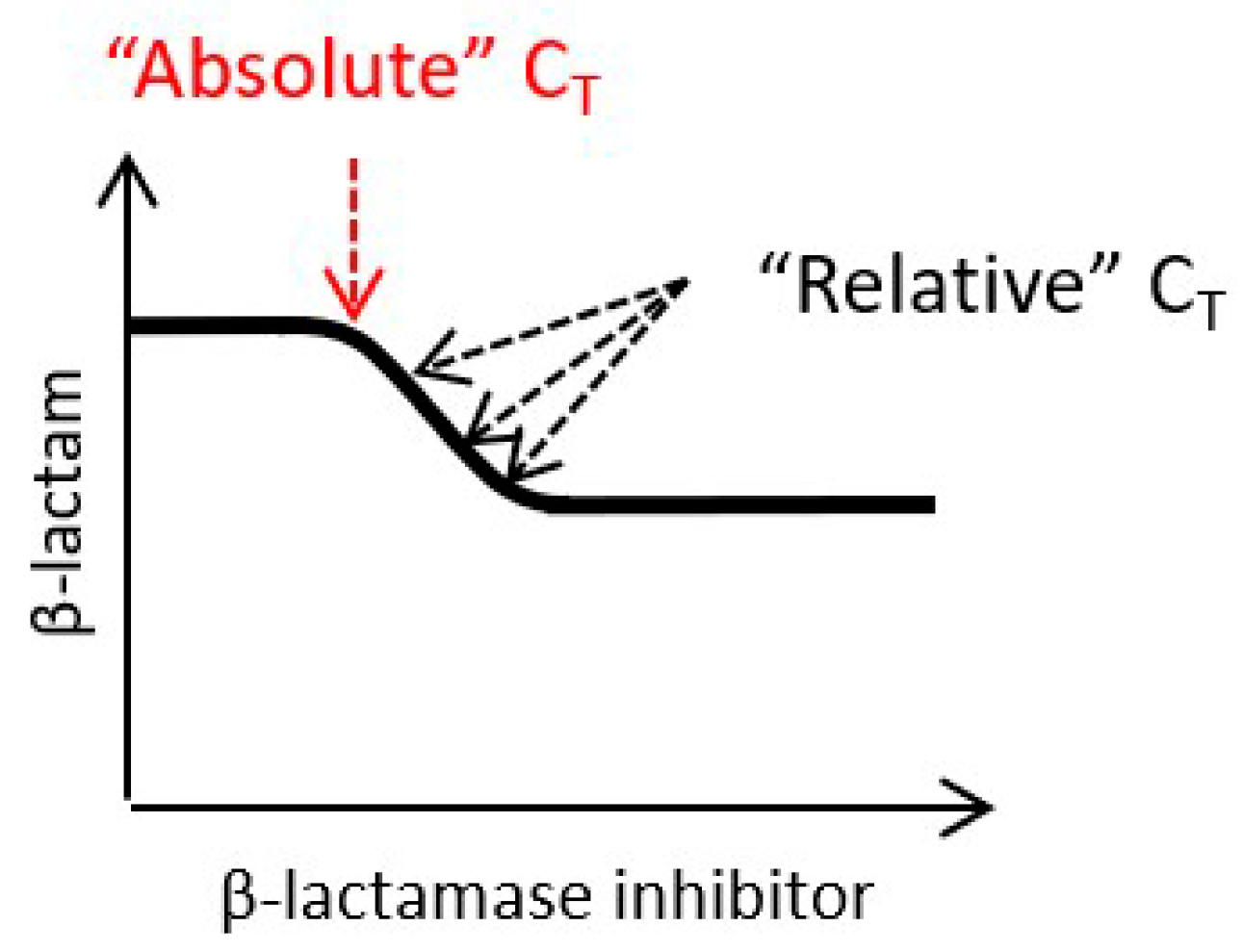
2.2. β-Lactamase Inhibitor Dose Selection
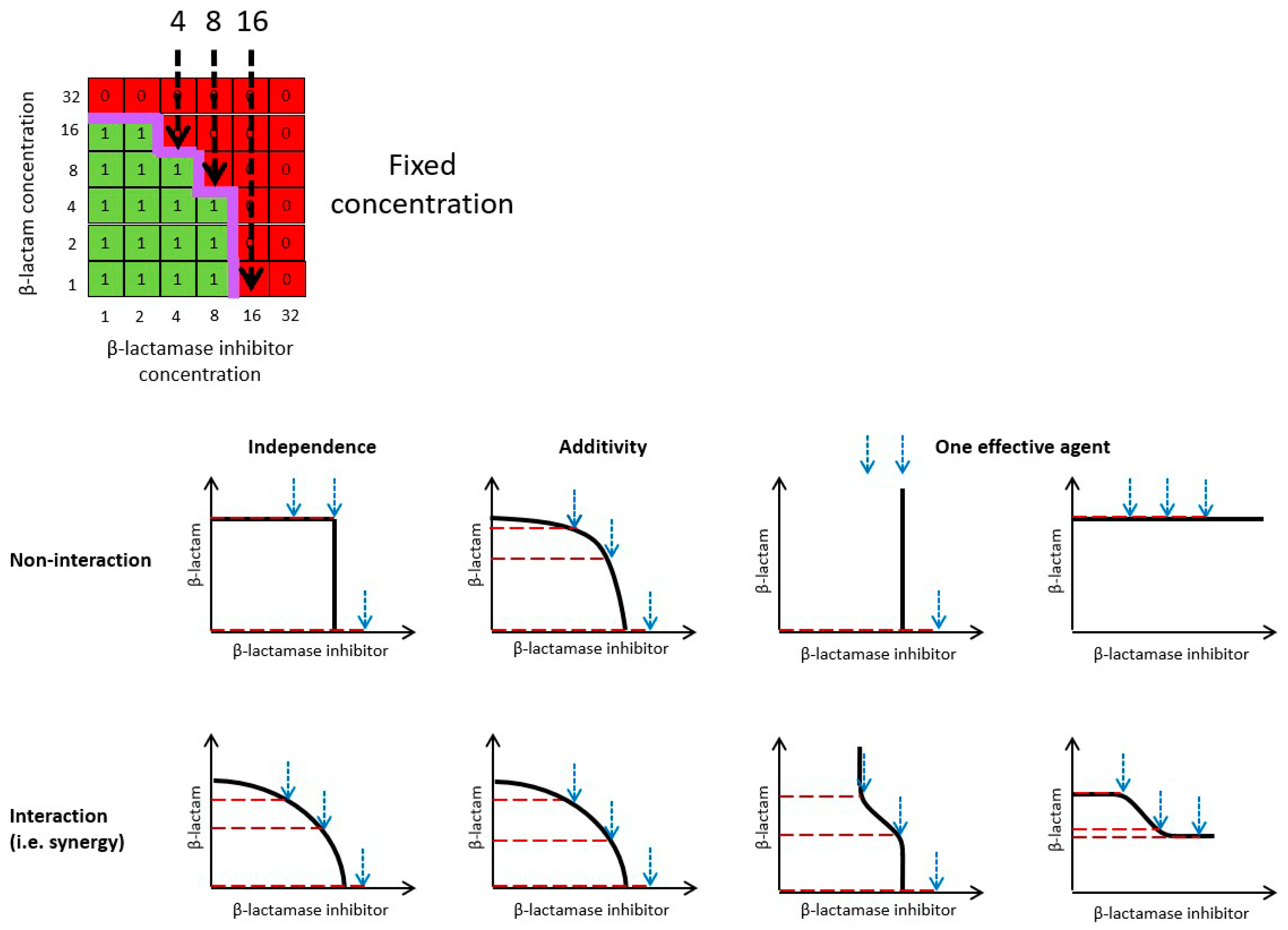
2.3. Drug Susceptibility Testing Methods
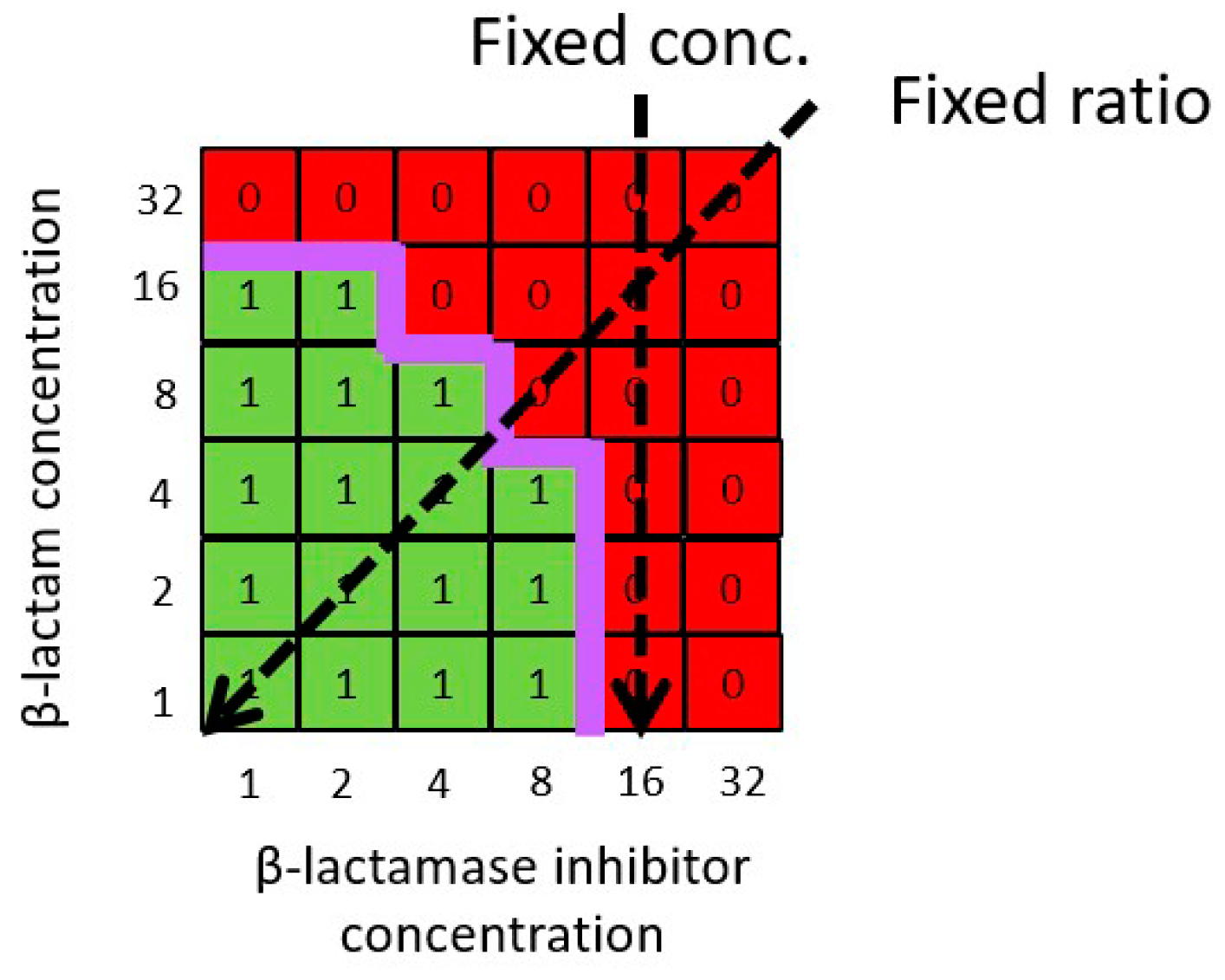
2.3.1. “Fixed Concentration” Method
2.3.2. “Fixed Ratio” Method
3. Discussion
4. Materials and Methods
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papp-Wallace, K.M. The latest advances in β-lactam/β-lactamase inhibitor combinations for the treatment of Gram-negative bacterial infections. Expert. Opin. Pharmacother. 2019, 20, 2169–2184. [Google Scholar] [CrossRef] [PubMed]
- Bush, K.; Bradford, P.A. Interplay between β-lactamases and new β-lactamase inhibitors. Nat. Rev. Microbiol. 2019, 17, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Jalde, S.S.; Choi, H.K. Recent advances in the development of β-lactamase inhibitors. J. Microbiol. 2020, 58, 633–647. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Giske, C.G.; Grāmatniece, A.; Abodakpi, H.; Tam, V.H.; Leibovici, L. New β-lactam–β-lactamase inhibitor combinations. Clin. Microbiol. Rev. 2020, 34, e00115-20. [Google Scholar] [CrossRef] [PubMed]
- Arer, V.; Kar, D. Biochemical exploration of β-lactamase inhibitors. Front. Genet. 2022, 13, 1060736. [Google Scholar] [CrossRef] [PubMed]
- Narendrakumar, L.; Chakraborty, M.; Kumari, S.; Paul, D.; Das, B. β-Lactam potentiators to re-sensitize resistant pathogens: Discovery, development, clinical use and the way forward. Front. Microbiol. 2022, 13, 1092556. [Google Scholar] [CrossRef] [PubMed]
- Mackow, N.A.; van Duin, D. Reviewing novel treatment options for carbapenem-resistant Enterobacterales. Expert. Rev. Anti Infect. Ther. 2024, 22, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.S.; Henderson, I.R.; Capon, R.J.; Blaskovich, M.A.T. Antibiotics in the clinical pipeline as of December 2022. J. Antibiot. 2023, 76, 431–473. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 1998, 26, 1–10; quiz 11-2. [Google Scholar] [CrossRef]
- Sy, S.K.; Zhuang, L.; Derendorf, H. Pharmacokinetics and pharmacodynamics in antibiotic dose optimization. Expert. Opin. Drug Metab. Toxicol. 2016, 12, 93–114. [Google Scholar] [CrossRef]
- Tängdén, T.; Lundberg, C.V.; Friberg, L.E.; Huttner, A. How preclinical infection models help define antibiotic doses in the clinic. Int. J. Antimicrob. Agents 2020, 56, 106008. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Gascon, A.; Solinis, M.A.; Isla, A. The role of PK/PD analysis in the development and evaluation of antimicrobials. Pharmaceutics 2021, 13, 833. [Google Scholar] [CrossRef] [PubMed]
- Bissantz, C.; Zampaloni, C.; David-Pierson, P.; Dieppois, G.; Guenther, A.; Trauner, A.; Winther, L.; Stubbings, W. Translational PK/PD for the development of novel antibiotics—A drug developer’s perspective. Antibiotics 2024, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA); Committee for Medicinal Products for Human Use (CHMP). Guideline on the Use of Pharmacokinetics and Pharmacodynamics in the Development of Antimicrobial Medicinal Products. EMA/CHMP/594085/2015. 21 July 2016. Available online: https://www.ema.europa.eu/en/use-pharmacokinetics-pharmacodynamics-development-antibacterial-medicinal-products-scientific-guideline (accessed on 5 April 2024).
- Greco, W.R.; Bravo, G.; Parsons, J.C. The search for synergy: A critical review from a response surface perspective. Pharmacol. Rev. 1995, 47, 331–385. [Google Scholar] [PubMed]
- Lee, S.I. Drug interaction: Focusing on response surface models. Korean J. Anesthesiol. 2010, 58, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Geary, N. Understanding synergy. Am. J. Physiol. Endocrinol. Metab. 2013, 304, E237–E253. [Google Scholar] [CrossRef] [PubMed]
- Tallarida, R.J. Drug combinations: Tests and analysis with isoboles. Curr. Protoc. Pharmacol. 2016, 72, 9.19.1–9.19.19. [Google Scholar] [CrossRef] [PubMed]
- Wicha, S.G.; Chen, C.; Clewe, O.; Simonsson, U.S.H. A general pharmacodynamic interaction model identifies perpetrators and victims in drug interactions. Nat. Commun. 2017, 8, 2129. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.Y.; Pei, L.; Liu, Q.; Chen, S.; Dou, H.; Shu, G.; Yuan, Z.X.; Lin, J.; Peng, G.; Zhang, W.; et al. Isobologram analysis: A comprehensive review of methodology and current research. Front. Pharmacol. 2019, 10, 1222. [Google Scholar] [CrossRef]
- Kroemer, N.; Aubry, R.; Couet, W.; Gregoire, N.; Wicha, S.G. Optimized rhombic experimental dynamic checkerboard designs to elucidate pharmacodynamic drug interactions of antibiotics. Pharm. Res. 2022, 39, 3267–3277. [Google Scholar] [CrossRef]
- Morinaka, A.; Tsutsumi, Y.; Yamada, M.; Suzuki, K.; Watanabe, T.; Abe, T.; Furuuchi, T.; Inamura, S.; Sakamaki, Y.; Mitsuhashi, N.; et al. OP0595, a new diazabicyclooctane: Mode of action as a serine beta-lactamase inhibitor, antibiotic and beta-lactam ‘enhancer’. J. Antimicrob. Chemother. 2015, 70, 2779–2786. [Google Scholar] [CrossRef] [PubMed]
- Chauzy, A.; Gaelzer Silva Torres, B.; Buyck, J.; de Jonge, B.; Adier, C.; Marchand, S.; Couet, W.; Grégoire, N. Semimechanistic pharmacodynamic modeling of aztreonam-avibactam combination to understand its antimicrobial activity against multidrug-resistant Gram-negative bacteria. CPT Pharmacomet. Syst. Pharmacol. 2019, 8, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Lehar, J.; Zimmermann, G.R.; Krueger, A.S.; Molnar, R.A.; Ledell, J.T.; Heilbut, A.M.; Short, G.F., 3rd; Giusti, L.C.; Nolan, G.P.; Magid, O.A.; et al. Chemical combination effects predict connectivity in biological systems. Mol. Syst. Biol. 2007, 3, 80. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.; Levasseur, P.; Girard, A.M.; Borgonovi, M.; Miossec, C.; Merdjan, H.; Drusano, G.; Shlaes, D.; Nichols, W.W. Activities of ceftazidime and avibactam against β-lactamase-producing Enterobacteriaceae in a hollow-fiber pharmacodynamic model. Antimicrob. Agents Chemother. 2014, 58, 3366–3372. [Google Scholar] [CrossRef]
- Morinaka, A.; Tsutsumi, Y.; Yamada, K.; Takayama, Y.; Sakakibara, S.; Takata, T.; Abe, T.; Furuuchi, T.; Inamura, S.; Sakamaki, Y.; et al. In vitro and in vivo activities of OP0595, a new diazabicyclooctane, against CTX-M-15-positive Escherichia coli and KPC-positive Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2016, 60, 3001–3006. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.; Rubio-Aparicio, D.; Sun, D.; Dudley, M.; Lomovskaya, O. In vitro activity of the ultrabroad-spectrum-beta-lactamase inhibitor QPX7728 against carbapenem-resistant Enterobacterales with varying intrinsic and acquired resistance mechanisms. Antimicrob. Agents Chemother. 2020, 64, e00757-20. [Google Scholar] [CrossRef] [PubMed]
- Landersdorfer, C.B.; Nation, R.L. Limitations of antibiotic MIC-based PK-PD metrics: Looking back to move forward. Front. Pharmacol. 2021, 12, 770518. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.W.; Dudley, M.N.; Cars, O.; Derendorf, H.; Drusano, G.L. Standardization of pharmacokinetic/pharmacodynamic (PK/PD) terminology for anti-infective drugs: An update. J. Antimicrob. Chemother. 2005, 55, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.W.; Brown, D.F.; Apfalter, P.; Canton, R.; Giske, C.G.; Ivanova, M.; MacGowan, A.P.; Rodloff, A.; Soussy, C.J.; Steinbakk, M.; et al. The role of pharmacokinetics/pharmacodynamics in setting clinical MIC breakpoints: The EUCAST approach. Clin. Microbiol. Infect. 2012, 18, E37–E45. [Google Scholar] [CrossRef]
- Nielsen, E.I.; Friberg, L.E. Pharmacokinetic-pharmacodynamic modeling of antibacterial drugs. Pharmacol. Rev. 2013, 65, 1053–1090. [Google Scholar] [CrossRef]
- Meletiadis, J.; Verweij, P.E.; Te Dorsthorst, D.T.A.; Meis, J.F.G.M.; Mouton, J.W. Assessing in vitro combinations of antifungal drugs against yeasts and filamentous fungi: Comparison of different drug interaction models. Med. Mycol. 2005, 43, 133–152. [Google Scholar] [CrossRef] [PubMed]
- Sinzger, M.; Vanhoefer, J.; Loos, C.; Hasenauer, J. Comparison of null models for combination drug therapy reveals Hand model as biochemically most plausible. Sci. Rep. 2019, 9, 3002. [Google Scholar] [CrossRef] [PubMed]
- Pearson, R.A.; Wicha, S.G.; Okour, M. Drug combination modeling: Methods and applications in drug development. J. Clin. Pharmacol. 2023, 63, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Prichard, M.N.; Shipman, C. A three-dimensional model to analyze drug-drug interactions. Antivir. Res. 1990, 14, 181–206. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, M.C. What is synergy? Pharmacol. Rev. 1989, 41, 93–141. [Google Scholar] [PubMed]
- Montaner, M.; Lopez-Arguello, S.; Oliver, A.; Moya, B. PBP target profiling by β-lactam and β-lactamase inhibitors in intact Pseudomonas aeruginosa: Effects of the intrinsic and acquired resistance determinants on the periplasmic drug availability. Microbiol. Spectr. 2023, 11, e0303822. [Google Scholar] [CrossRef]
- Kristoffersson, A.N.; Bissantz, C.; Okujava, R.; Haldimann, A.; Walter, I.; Shi, T.; Zampaloni, C.; Nielsen, E.I. A novel mechanism-based pharmacokinetic-pharmacodynamic (PKPD) model describing ceftazidime/avibactam efficacy against β-lactamase-producing Gram-negative bacteria. J. Antimicrob. Chemother. 2020, 75, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Nichols, W.W.; Newell, P.; Critchley, I.A.; Riccobene, T.; Das, S. Avibactam pharmacokinetic/pharmacodynamic targets. Antimicrob. Agents Chemother. 2018, 62, e02446-17. [Google Scholar] [CrossRef] [PubMed]
- Bhagunde, P.; Chang, K.T.; Hirsch, E.B.; Ledesma, K.R.; Nikolaou, M.; Tam, V.H. Novel modeling framework to guide design of optimal dosing strategies for beta-lactamase inhibitors. Antimicrob. Agents Chemother. 2012, 56, 2237–2240. [Google Scholar] [CrossRef]
- Wu, J.; Racine, F.; Wismer, M.K.; Young, K.; Carr, D.M.; Xiao, J.C.; Katwaru, R.; Si, Q.; Harradine, P.; Motyl, M.; et al. Exploring the pharmacokinetic/pharmacodynamic relationship of relebactam (MK-7655) in combination with imipenem in a hollow-fiber infection model. Antimicrob. Agents Chemother. 2018, 62, e02323-17. [Google Scholar] [CrossRef]
- Abodakpi, H.; Chang, K.T.; Zhou, J.; Byerly, C.; Tam, V.H. A novel framework to compare the effectiveness of β-lactamase inhibitors against extended-spectrum β-lactamase-producing Enterobacteriaceae. Clin. Microbiol. Infect. 2019, 25, 1154.e9–1154.e14. [Google Scholar] [CrossRef] [PubMed]
- Chauzy, A.; Buyck, J.; de Jonge, B.L.M.; Marchand, S.; Gregoire, N.; Couet, W. Pharmacodynamic modelling of β-lactam/β-lactamase inhibitor checkerboard data: Illustration with aztreonam-avibactam. Clin. Microbiol. Infect. 2019, 25, 515.e1–515.e4. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, Y.; Takemura, W.; Liu, X.; Kojima, N.; Morita, T.; Chuang, V.T.G.; Enoki, Y.; Taguchi, K.; Matsumoto, K. Development of an optimized and practical pharmacokinetics/pharmacodynamics analysis method for aztreonam/nacubactam against carbapenemase-producing K. pneumoniae. J. Antimicrob. Chemother. 2023, 78, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Hagihara, M.; Kato, H.; Sugano, T.; Okade, H.; Sato, N.; Shibata, Y.; Sakanashi, D.; Asai, N.; Koizumi, Y.; Suematsu, H.; et al. Pharmacodynamic evaluation of meropenem, cefepime, or aztreonam combined with a novel β-lactamase inhibitor, nacubactam, against carbapenem-resistant and/or carbapenemase-producing Klebsiella pneumoniae and Escherichia coli using a murine thigh-infection model. Int. J. Antimicrob. Agents 2021, 57, 106330. [Google Scholar] [PubMed]
- Sy, S.; Zhuang, L.; Xia, H.; Beaudoin, M.E.; Schuck, V.J.; Derendorf, H. Prediction of in vivo and in vitro infection model results using a semimechanistic model of avibactam and aztreonam combination against multidrug resistant organisms. CPT Pharmacomet. Syst. Pharmacol. 2017, 6, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Brill, M.J.E.; Kristoffersson, A.N.; Zhao, C.; Nielsen, E.I.; Friberg, L.E. Semi-mechanistic pharmacokinetic-pharmacodynamic modelling of antibiotic drug combinations. Clin. Microbiol. Infect. 2018, 24, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Minichmayr, I.K.; Aranzana-Climent, V.; Friberg, L.E. Pharmacokinetic/pharmacodynamic models for time courses of antibiotic effects. Int. J. Antimicrob. Agents 2022, 60, 106616. [Google Scholar] [CrossRef]
- Mouton, J.W.; Muller, A.E.; Canton, R.; Giske, C.G.; Kahlmeter, G.; Turnidge, J. MIC-based dose adjustment: Facts and fables. J. Antimicrob. Chemother. 2018, 73, 564–568. [Google Scholar] [CrossRef]
- Abodakpi, H.; Wanger, A.; Tam, V.H. What the clinical microbiologist should know about pharmacokinetics/pharmacodynamics in the era of emerging multidrug resistance: Focusing on beta-lactam/beta-lactamase inhibitor combinations. Clin. Lab. Med. 2019, 39, 473–485. [Google Scholar] [CrossRef]
- Assefa, G.M.; Roberts, J.A.; Mohammed, S.A.; Sime, F.B. What are the optimal pharmacokinetic/pharmacodynamic targets for beta-lactamase inhibitors? A systematic review. J. Antimicrob. Chemother. 2024. [Google Scholar] [CrossRef]
- Roell, K.R.; Reif, D.M.; Motsinger-Reif, A.A. An introduction to terminology and methodology of chemical synergy-perspectives from across disciplines. Front. Pharmacol. 2017, 8, 158. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bentley, D.J. Revisiting the Checkerboard to Inform Development of β-Lactam/β-Lactamase Inhibitor Combinations. Antibiotics 2024, 13, 337. https://doi.org/10.3390/antibiotics13040337
Bentley DJ. Revisiting the Checkerboard to Inform Development of β-Lactam/β-Lactamase Inhibitor Combinations. Antibiotics. 2024; 13(4):337. https://doi.org/10.3390/antibiotics13040337
Chicago/Turabian StyleBentley, Darren J. 2024. "Revisiting the Checkerboard to Inform Development of β-Lactam/β-Lactamase Inhibitor Combinations" Antibiotics 13, no. 4: 337. https://doi.org/10.3390/antibiotics13040337
APA StyleBentley, D. J. (2024). Revisiting the Checkerboard to Inform Development of β-Lactam/β-Lactamase Inhibitor Combinations. Antibiotics, 13(4), 337. https://doi.org/10.3390/antibiotics13040337