Blending Hyaluronic Acid and Calcium Hydroxylapatite for Injectable Facial Dermal Fillers: A Clinical and Ultrasonography Assessment


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
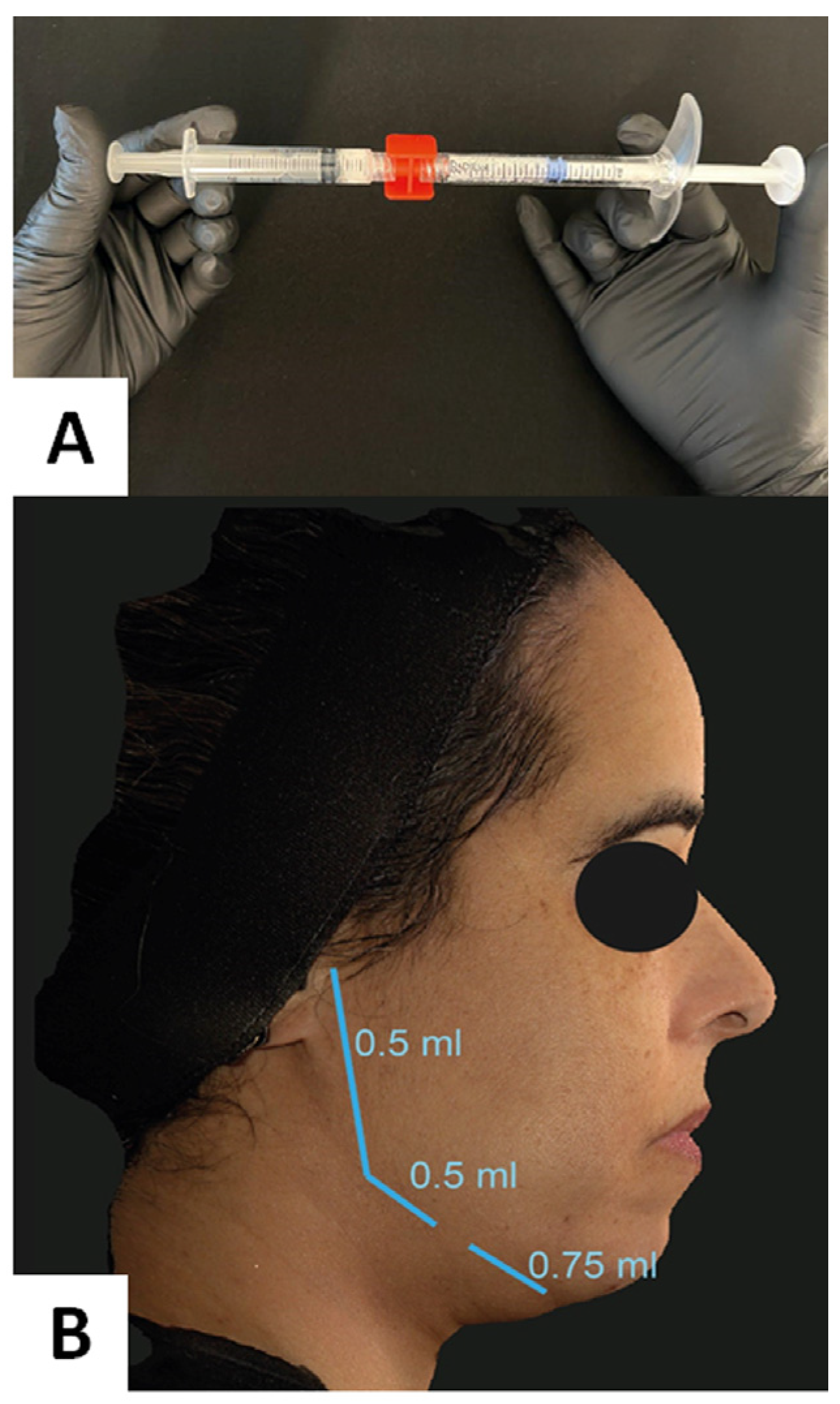
2.1. Technical Procedure
2.2. Data Analysis
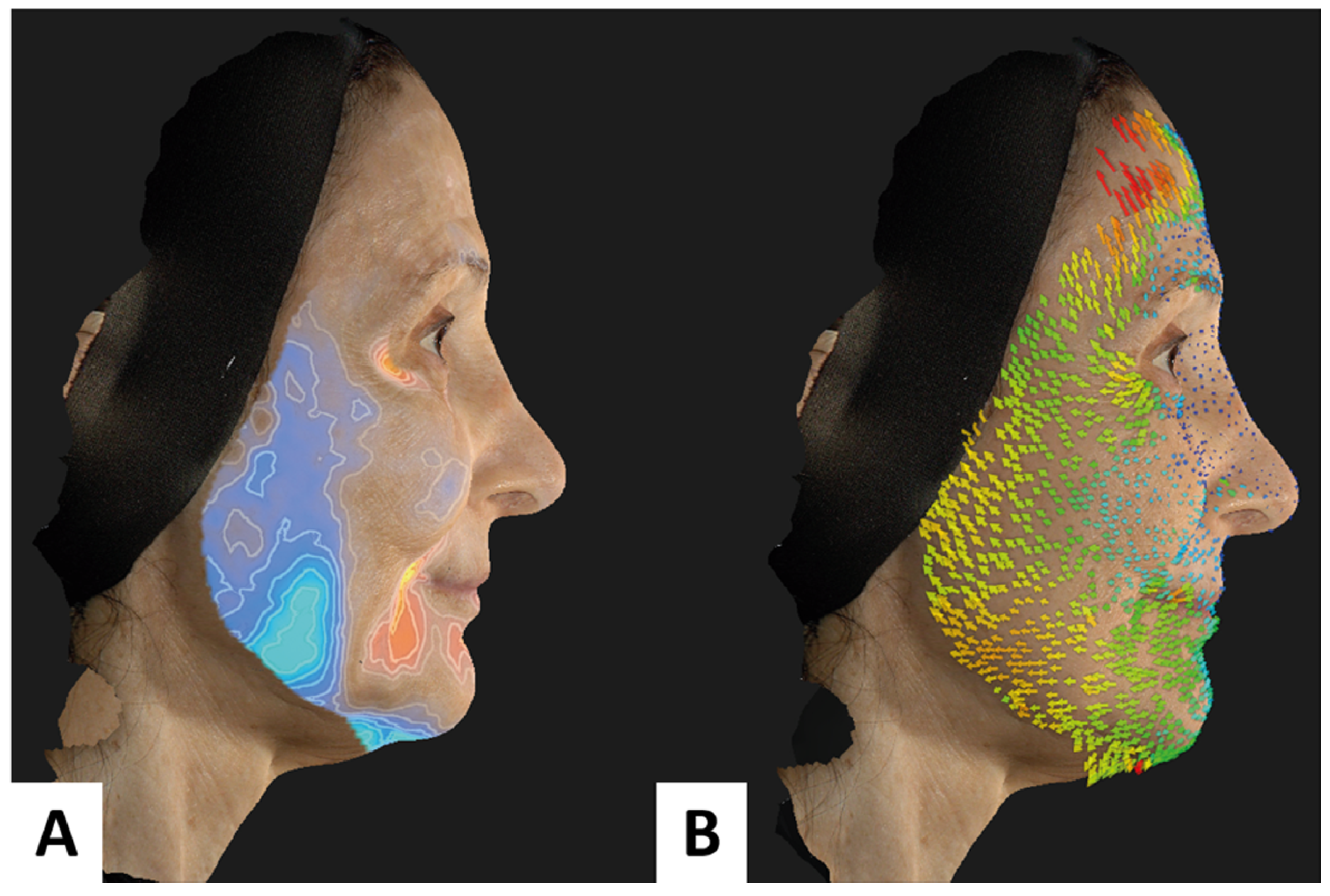
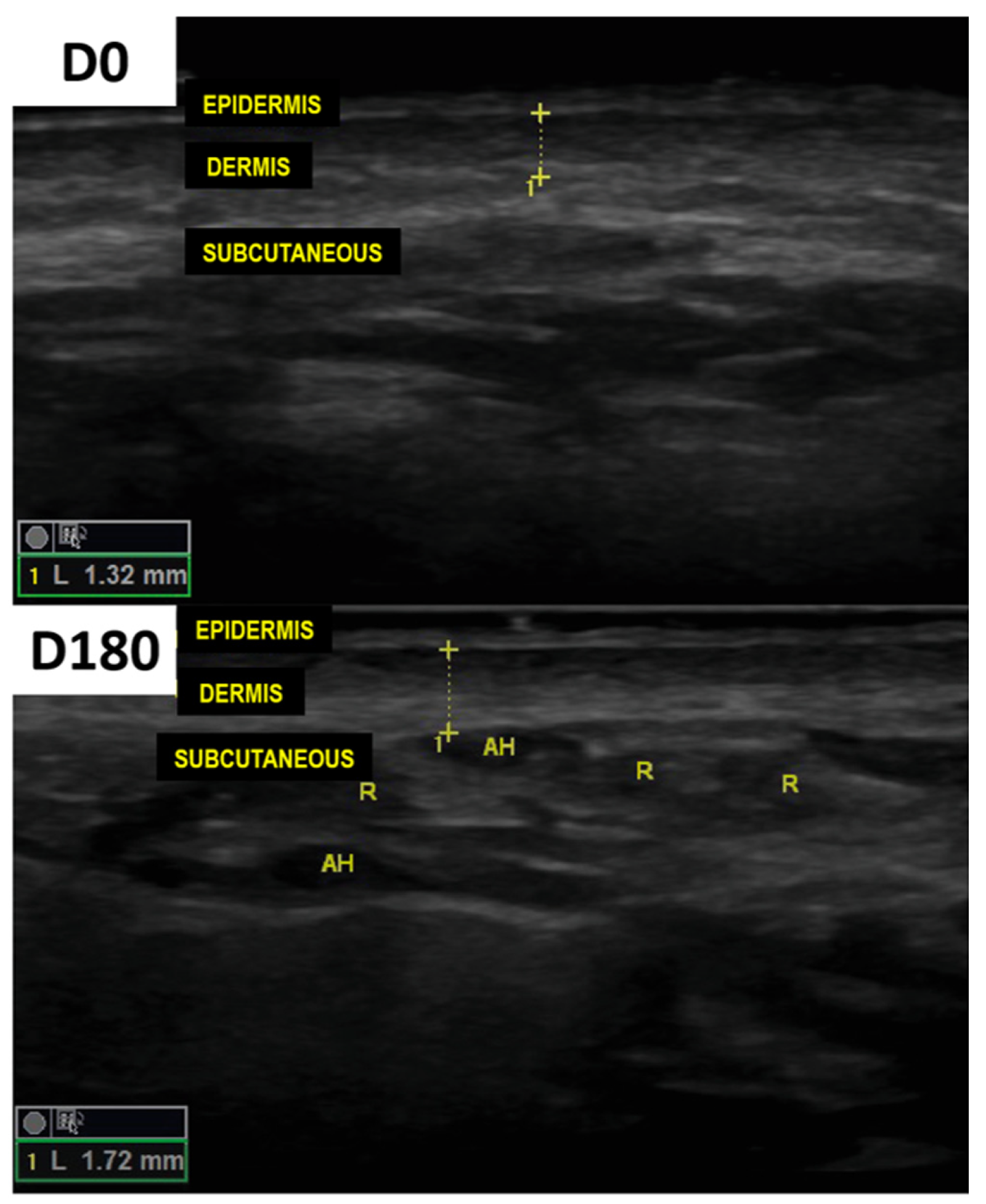
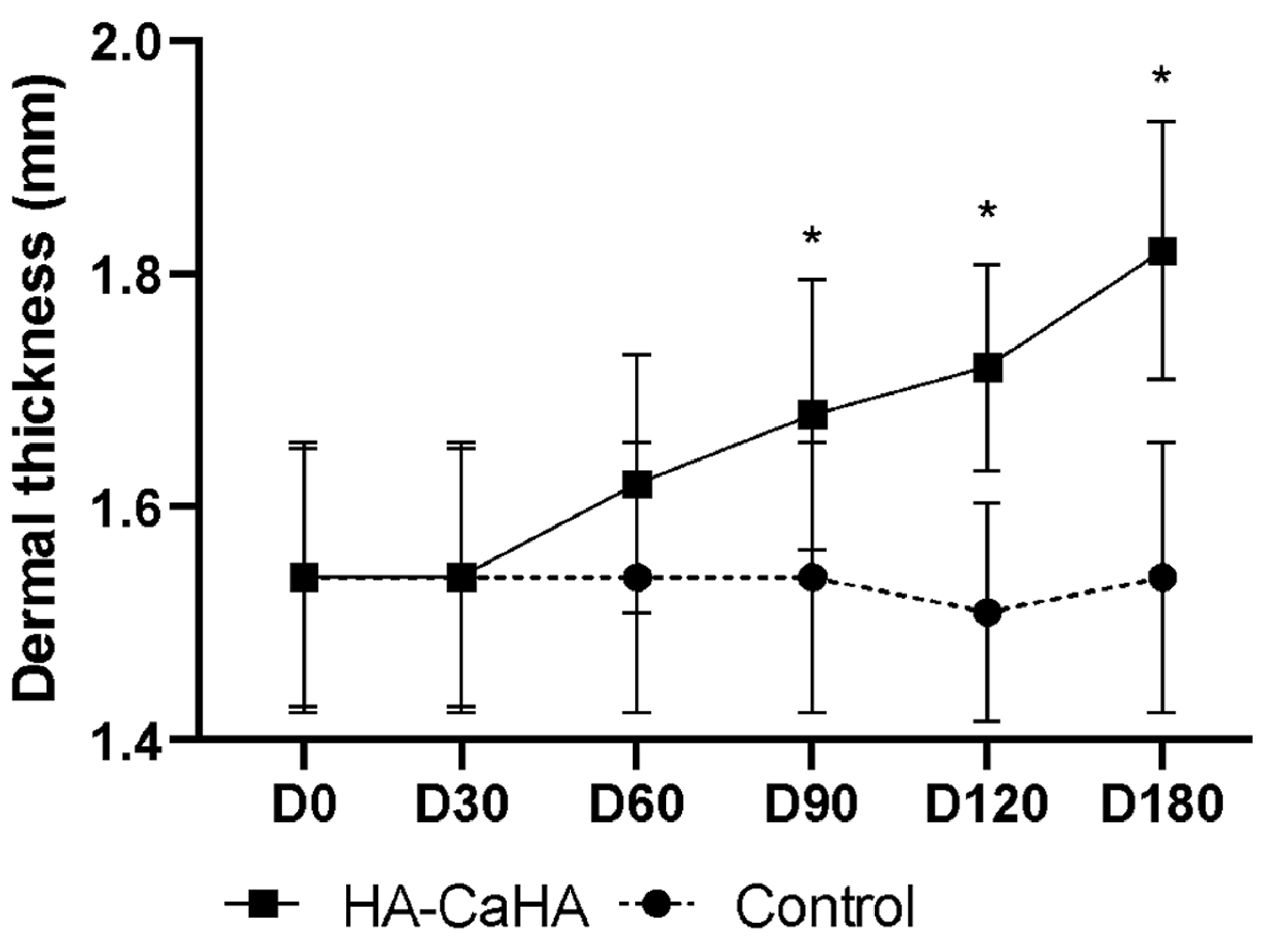
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Devgan, L.; Singh, P.; Durairaj, K. Minimally Invasive Facial Cosmetic Procedures. Otolaryngol. Clin. N. Am. 2019, 52, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Felix Bravo, B.; Bezerra de Menezes Penedo, L.; de Melo Carvalho, R.; Amante Miot, H.; Calomeni Elias, M. Improvement of Facial Skin Laxity by a Combined Technique With Hyaluronic Acid and Calcium Hydroxylapatite Fillers: A Clinical and Ultrasonography Analysis. J. Drugs Dermatol. 2022, 21, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Lizzul, P.F.; Narurkar, V.A. The role of calcium hydroxylapatite (Radiesse) in nonsurgical aesthetic rejuvenation. J. Drugs Dermatol. 2010, 9, 446–450. [Google Scholar] [PubMed]
- de Almeida, A.T.; Figueredo, V.; da Cunha, A.L.G.; Casabona, G.; de Faria, J.R.C.; Alves, E.V.; Sato, M.; Branco, A.; Guarnieri, C.; Palermo, E. Consensus Recommendations for the Use of Hyperdiluted Calcium Hydroxyapatite (Radiesse) as a Face and Body Biostimulatory Agent. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2160. [Google Scholar] [CrossRef] [PubMed]
- van Loghem, J.; Sattler, S.; Casabona, G.; Cotofana, S.; Fabi, S.G.; Goldie, K.; Gout, U.; Kerscher, M.; Lim, T.S.; de Sanctis Pecora, C.; et al. Consensus on the Use of Hyaluronic Acid Fillers from the Cohesive Polydensified Matrix Range: Best Practice in Specific Facial Indications. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1175–1199. [Google Scholar] [CrossRef] [PubMed]
- Keen, M.A. Hyaluronic Acid in Dermatology. Skinmed 2017, 15, 441–448. [Google Scholar] [PubMed]
- Lorenc, Z.P.; Bass, L.M.; Fitzgerald, R.; Goldberg, D.J.; Graivier, M.H. Composite Facial Volumization with Calcium Hydroxylapatite (CaHA) for the Treatment of Aging. Aesthet. Surg. J. 2018, 38, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Miola, A.C.; Miot, H.A. Comparing categorical variables in clinical and experimental studies. J. Vasc. Bras. 2022, 21, e20210225. [Google Scholar] [CrossRef] [PubMed]
- Miot, H.A. Assessing normality of data in clinical and experimental trials. J. Vasc. Bras. 2017, 16, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Miola, A.C.; Miot, H.A. P-value and effect-size in clinical and experimental studies. J. Vasc. Bras. 2021, 20, e20210038. [Google Scholar] [CrossRef] [PubMed]
- Akinbiyi, T.; Othman, S.; Familusi, O.; Calvert, C.; Card, E.B.; Percec, I. Better Results in Facial Rejuvenation with Fillers. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2763. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U.; Goldman, A. Long lasting facial rejuvenation by repeated placement of calcium hydroxylapatite in elderly women. Dermatol. Ther. 2020, 33, e14183. [Google Scholar] [CrossRef] [PubMed]
- Dallara, J.M.; Baspeyras, M.; Bui, P.; Cartier, H.; Charavel, M.H.; Dumas, L. Calcium hydroxylapatite for jawline rejuvenation: Consensus recommendations. J. Cosmet. Dermatol. 2014, 13, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Vazirnia, A.; Braz, A.; Fabi, S.G. Nonsurgical jawline rejuvenation using injectable fillers. J. Cosmet. Dermatol. 2020, 19, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- Waldman, S.R. Aesthetic Treatment of the Jawline and Perioral Area. Facial Plast. Surg. 2019, 35, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Fakih-Gomez, N.; Kadouch, J. Combining Calcium Hydroxylapatite and Hyaluronic Acid Fillers for Aesthetic Indications: Efficacy of an Innovative Hybrid Filler. Aesthetic Plast. Surg. 2022, 46, 373–381. [Google Scholar] [CrossRef] [PubMed]
- de Caetano, V.N.L.; Soares, J.L.; Bagatin, E.; Miot, H.A. Reliable assessment of forearm photoageing by high-frequency ultrasound: A cross-sectional study. Int. J. Cosmet. Sci. 2016, 38, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Pavicic, T.; Few, J.W.; Huber-Vorländer, J. A novel, multistep, combination facial rejuvenation procedure for treatment of the whole face with incobotulinumtoxinA, and two dermal fillers-calcium hydroxylapatite and a monophasic, polydensified hyaluronic acid filler. J. Drugs Dermatol. 2013, 12, 978–984. [Google Scholar] [PubMed]
- Viscomi, B.; Faria, G.; Hernandez, C.A.; Perez, L.; Spada, J.; De la Fuente, V.; Muniz, M. Contouring Plus: A Comprehensive Approach of the Lower Third of the Face with Calcium Hydroxylapatite and Hyaluronic Acid. Clin. Cosmet. Investig. Dermatol. 2023, 16, 911–924. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravo, B.; Carvalho, R.; Bravo, L.; Penedo, L.; Elias, M. Blending Hyaluronic Acid and Calcium Hydroxylapatite for Injectable Facial Dermal Fillers: A Clinical and Ultrasonography Assessment. Cosmetics 2024, 11, 61. https://doi.org/10.3390/cosmetics11020061
Bravo B, Carvalho R, Bravo L, Penedo L, Elias M. Blending Hyaluronic Acid and Calcium Hydroxylapatite for Injectable Facial Dermal Fillers: A Clinical and Ultrasonography Assessment. Cosmetics. 2024; 11(2):61. https://doi.org/10.3390/cosmetics11020061
Chicago/Turabian StyleBravo, Bruna, Raquel Carvalho, Leonardo Bravo, Laís Penedo, and Mariana Elias. 2024. "Blending Hyaluronic Acid and Calcium Hydroxylapatite for Injectable Facial Dermal Fillers: A Clinical and Ultrasonography Assessment" Cosmetics 11, no. 2: 61. https://doi.org/10.3390/cosmetics11020061
APA StyleBravo, B., Carvalho, R., Bravo, L., Penedo, L., & Elias, M. (2024). Blending Hyaluronic Acid and Calcium Hydroxylapatite for Injectable Facial Dermal Fillers: A Clinical and Ultrasonography Assessment. Cosmetics, 11(2), 61. https://doi.org/10.3390/cosmetics11020061