1. Introduction
Microalgae are photosynthetic organisms that grow in various aquatic habitats in a range of conditions [
1]. Specific species of microalgae are known to be used in human nutrition for years due to their high nutritional value [
1]. Spirulina (
Arthrospira platensis and
Arthrospira maxima) is a blue-green, filamentous, sustainable, and ecofriendly cyanobacterium [
1]. It contains high amounts of protein (60–70% of its dry weight), 4–7% lipids, and 13.5% carbohydrates [
1]. It also contains, among others, B vitamins, iron, calcium, and antioxidants [
1]. The Food and Drug Administration (FDA) approved spirulina as GRAS (Generally Recognized as Safe) food without toxicological effects on human health [
2]. The main pigment-protein complexes of spirulina are C-phycocyanin and allophycocyanin [
2]. According to the World Health Organization (WHO)/Food and Agriculture Organization of the United Nations (FAO) the total dietary exposure of spirulina from use as a food ingredient is estimated at 2000 g/person per day, expressed as phycocyanin, and 2–10 g/day of spirulina taken as dietary supplement [
3]. Few studies have examined the addition of spirulina to foods. The results from a study examining the addition of spirulina flour to the dough of durum wheat semolina spaghetti at two different concentrations, 5% and 10%, reported: a significant increase in protein and dietary fiber content; a spirulina dose-dependent decline of the in vitro starch digestibility; but also a dose-dependent decline of pasta overall sensory quality [
4]. Another study reported that adding spirulina (0.5, 1.0, and 2.0 g/100 g DW) to semolina flour produced spaghetti richer than the control in fatty acids, and enhanced the nutritional and sensorial quality of pasta, although firmness was positively affected by spirulina inclusion [
5]. Similar results were reported with handmade ice cream containing microencapsulated spirulina (1% biomass in relation to ice cream mass), producing ice cream with 35% to 53% more protein [
6].
The glycemic index (GI) is a tool developed to classify carbohydrate containing foods according to their time integrated effects on postprandial glycemia [
7]. The GI depicts both the standardized and relative postprandial glucose response based on an equal amount of available carbohydrate and relative to a referent food [
7]. Foods containing carbohydrate that is digested, absorbed, and metabolized quickly are considered high GI foods (GI ≥ 70 on glucose scale); whereas those that are digested, absorbed, and metabolized slowly are considered low GI foods (GI ≤ 55 on glucose scale) [
7]. The consumption of high GI foods is associated with increased chronic disease risk [
8,
9,
10]; whereas low to medium GI foods is associated with lower chronic disease risk [
11]. Results from one study examining the acute effects of adding 2.5 g spirulina in cereal bars, compared to conventional and cereals bars with brewers spent grain and dehydrated apple, reported lower blood glucose peaks after spirulina consumption, but a similar and gradual release of glucose in blood between the test cereals under study [
12]. Another study examining the effects of four Indian regional meals all supplemented with 2.5 g of spray dried spirulina powder in healthy adults, reported inconclusive effects of spirulina on postprandial glycemia [
13].
Results from a systematic review assessing the effects of spirulina supplementation on metabolic syndrome components, hepatic, and related inflammatory markers from 22 randomized clinical trials (RCTs), reported that oral dosage ranging from 1–19 g/day for 0.5–6 months had positive effects on metabolic syndrome components, although determining the optimal dosage still needs further investigation [
14]. Regarding the effects of spirulina supplementation on blood pressure (BP), the results from RCTs in healthy individuals, overweight or obese elderly, people with type 2 diabetes, and people with non-alcoholic fatty liver disease (NAFLD), short-term (few hours) or longer-term (up to 3 months), were inconclusive and the optimal dose is still unknown [
15,
16,
17,
18,
19,
20,
21]. Spirulina supplementation for 3 months has also been reported to reduce appetite [
22,
23].
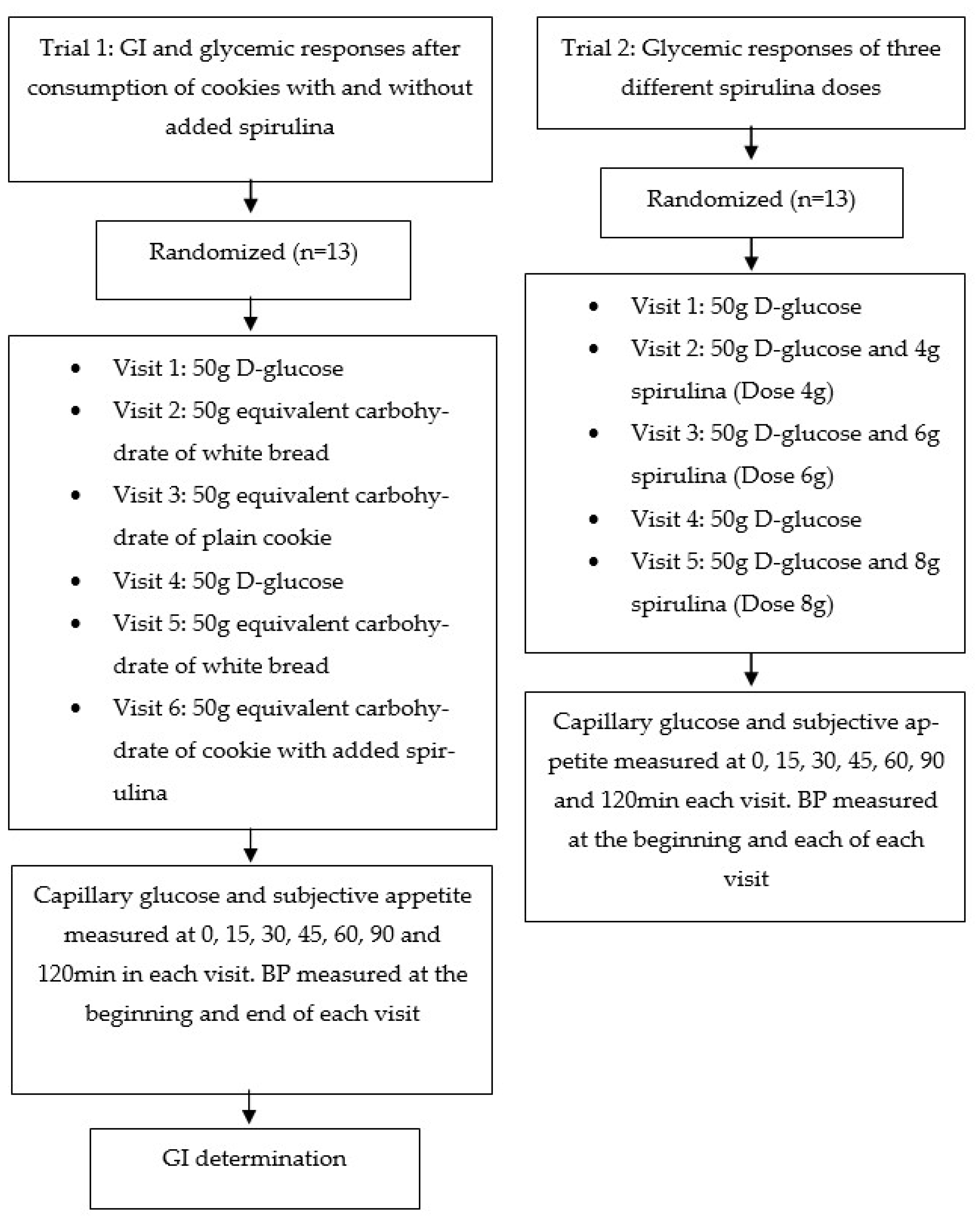
Based on the literature, a dose of 2.5 g spirulina added in foods showed some promising effects on health indices. Therefore, in order to evaluate the short-term effects of spirulina consumption from foods on postprandial glycemic responses, BP, and subjective appetite, in metabolically healthy adults, two cross-over, randomized clinical trials were carried out: (a) to examine the effects of added spirulina in cookies; and (b) to examine the effects of three different doses of spirulina consumed as glucose beverages in the aforementioned health indices.
4. Discussion
Spirulina is a functional ingredient and has gained significant scientific interest in the past few years. To the best of our knowledge, our two current investigations examined for the first time: (a) the effects of adding 3.12 g of spirulina per 100 g to cookies, thus examining the dose of 2.5 g spirulina per 50 g available carbohydrates on the GI, following the ISO 26642:2010 International Organization for Standardization [
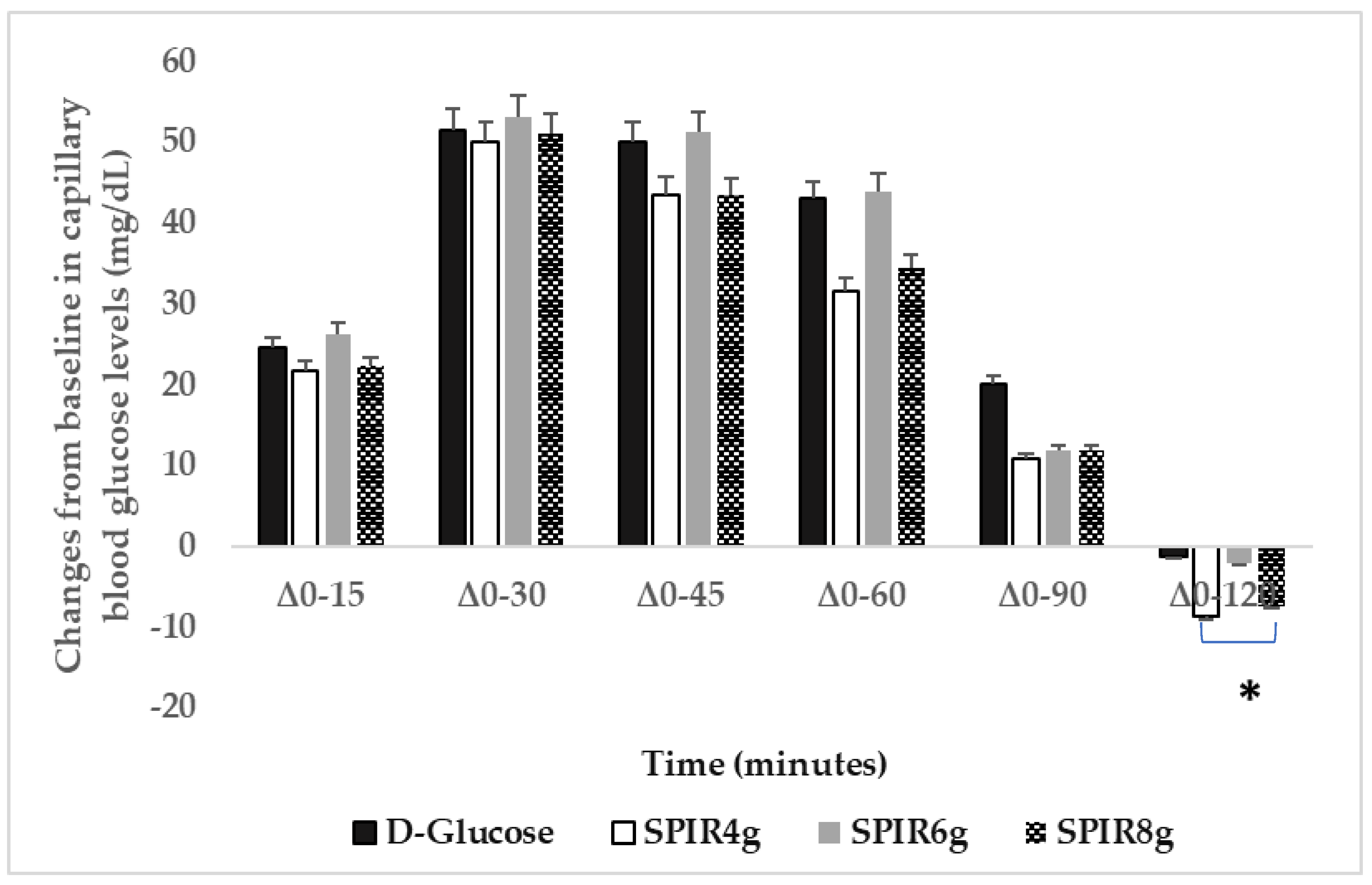
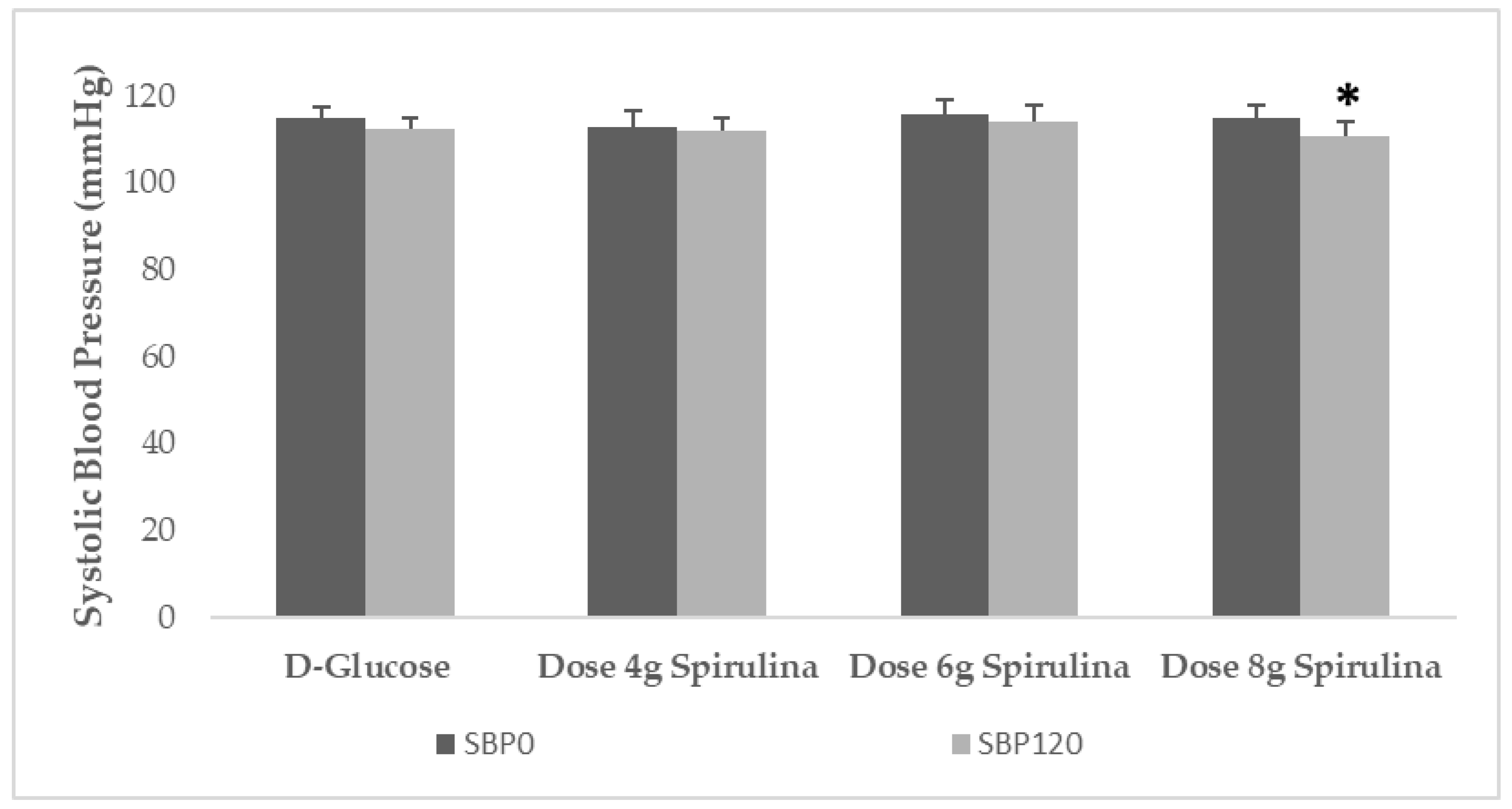
7] method and procedures, and on the glycemic responses; and (b) the effects of three doses of spirulina, namely 4 g, 6 g, and 8 g, added in glucose beverages containing 50 g D-glucose on the postprandial glycemic responses in young healthy adults. The main findings of the two trials were that: (a) contrary to our first hypothesis, adding spirulina to cookies did not produce lower GI or ameliorated postprandial glycemic responses compared to plain cookies prepared with exactly the same recipe and containing the same amount and type of carbohydrates, although both cookies produced medium GI values and significantly lower postprandial blood glucose levels compared to the reference food D-glucose; and (b) in the second investigation, we found that only the glucose beverage containing 8 g of spirulina lowered significantly postprandial glucose concentrations at 90 to 120 min posttest beverage consumption of approximately −9 mg/dL compared to D-glucose, 4 g, and 6 g spirulina. Moreover, only the glucose beverage containing 8 g spirulina decreased significantly SBP by 4.2 mmHg or approximately 4% at 120 min posttest beverage consumption in normotensive healthy young adults.
Hyperglycemia and hypertension are key risk factors for the development of atherosclerotic cardiovascular diseases (CVD) in humans [
27]. Therefore, the assessment of glycemic and BP effects of functional foods or ingredients, such as spirulina, may be considered a crucial element for an effective primary and secondary CVD prevention. It has been suggested that a dose of 2–14 g of spirulina supplementation is a safe approach as complementary treatment for chronic diseases [
28]. Adding spirulina to foods, such as pasta, at three levels, 5, 10, and 20 g/100 g, was reported to provide high amounts of proteins and phenolic compounds with antioxidant properties, without producing significant changes in estimated in vitro GI values of the tested pasta products, compared to conventional ones [
29], which is in partial agreement to findings from our first trial. Two studies examining the addition of 2.5 g spray dried spirulina powder to five Indian rice recipes and four Indian regional meals on glycemic responses of healthy participants, reported varying GIs of the tested meals and claimed potential spirulina induced blood glucose lowering effects when compared to the reference food D-glucose [
13,
30], which is also in partial agreement with our first trial.
Regarding results from our second current investigation reporting that the dose of 8 g of spirulina consumption as beverage decreased significantly more postprandial glycemic responses acutely, compared to the other doses, 2.5 g in cookies, 4 g as beverage, and 6 g as beverage, adds value to the limited randomized clinical trials (RCTs) literature. However, the optimal dose of spirulina consumption is still unknown, and the results from the few available RCTs are contradictory. The results from three available studies examining the effects of 8 g spirulina supplementation for 12 weeks reported contradictory results, with two studies showing no changes in fasting blood glucose in elderly and people with type 2 diabetes [
15,
16], and no changes in fasting insulin levels and HbA1c in people with type 2 diabetes [
16]; one study showed decreased fasting blood glucose levels in people with type 2 diabetes after spirulina supplementation [
31]. The results from the only one available study examining the effects of 6 g spirulina supplementation for 6 months in people with NAFLD showed a significant ~20% reduction in insulin resistance after spirulina supplementation [
17]. The results from two studies examining the effects of 4–4.5 g spirulina supplementation from 6 to 12 weeks in people with overweight or obesity, or with type 2 diabetes, showed no changes in fasting blood glucose or insulin levels after spirulina supplementation [
19,
32]. The results from four available studies examining the effects of 2 g spirulina supplementation from 8 to 12 weeks in overweight or obese individuals, or in people with type 2 diabetes or with NAFLD were also contradictory, with two studies reporting decreased insulin resistance in overweight or obese individuals and people with NAFLD, without changes in fasting blood glucose and insulin levels, after spirulina supplementation [
18,
22]; three studies showed significant decreases in fasting blood glucose and postprandial blood glucose levels in people with type 2 diabetes [
33,
34,
35], and decreased HbA1c [
33]. The possible beneficial effects of spirulina consumption on lowering blood glucose concentrations may be due to the fact that spirulina has been suggested to act as an insulin-like protein, or to stimulate the pancreatic β-cells by increasing insulin production and decreasing blood glucose concentrations [
28], possibly in a concentration dependent manner as has been shown in animal models [
36]. The contradictory results regarding the effects of spirulina supplementation on the indices of glycemic control are evident in systematic reviews and meta-analyses. The results from a recent systematic review and meta-analysis of seven randomized clinical trials (RCTs) (
n = 338) reported that a daily dose of 8 g of spirulina supplementation decreased significantly plasma triglyceride levels in adults with obesity or diabetes mellitus, but not fasting or postprandial blood glucose levels or HbA1c [
28]. Another recent systematic review and meta-analysis of eight RCTs (nine arms) in people with type 2 diabetes reported a significant reduction in fasting blood glucose levels, but no effect on HbA1c or postprandial blood glucose fluctuations after spirulina supplementation in doses of 0.8 to 8 g/day and duration from 45 to 90 days [
37]. Another recent systematic review and meta-analysis of seven clinical trials in humans and 27 animal studies reported that spirulina supplementation decreased significantly fasting blood glucose levels in people with type 2 diabetes, and fasting blood glucose levels and HbA1c in diabetic animals, but without changes in body weight, fasting insulin levels, and insulin resistance [
38]. Sub-group analyses showed that short-term trials with a duration of less than 2 months and the consumption of a spirulina dose of less than 2 g showed significant improvements in terms of lowering fasting blood glucose in humans [
38]. Another systematic review and meta-analysis of 12 RCTs reported that participants taking 2 or more g spirulina/day for 12 or more weeks had significantly lower triglyceride and fasting blood glucose levels, HbA1c, and SBP/DBP [
39]. In contrast, another systematic review and meta-analysis reported a significant reduction in fasting blood glucose levels following spirulina supplementation; however, this was observed only in populations with type 2 diabetes older than 45 years, overweight or obese, and those that used spirulina in dosages of 4 or lower g/day [
40]. Interestingly, and contrary to fasting blood glucose, this meta-analysis also reported a significant increase in HbA1c concentrations after spirulina supplementation in studies that used less than 4 g/day and those with a duration less than 12 weeks; whereas a significant reduction in HbA1c levels was observed only in studies using spirulina in doses of 4 or more g/day, that lasted 12 or more weeks, and had a sample size of fewer than 40 participants [
40]. In addition, pooled analysis from three studies showed a significant reduction in insulin concentrations after intake of spirulina supplements, without data on spirulina dosage [
40].
A decrease in glycated hemoglobin A1c (HbA1c) has been suggested to be expected with spirulina consumption or supplementation due to the high iron content of spirulina that could increase hemoglobin levels lowering consequently blood glucose concentrations [
41]. It has been suggested that the blood glucose lowering effects may be due to spirulina’s fiber content, protein, and bioactive polypeptides produced after digestion, which may increase insulin secretion and lower glucose absorption [
42] and postprandial blood glucose levels even in patients with type 2 diabetes [
42,
43]. Spirulina consumption has been reported to improve C-peptide and plasma insulin levels [
44]. Increased glucokinase activity in the liver cells of rats treated with spirulina suggested increased glucose uptake from the circulation [
44]. Spirulina produced high levels of NADP+, resulting in reduced lipogenesis, less oxidative stress, and lowering resistance levels to diabetes [
44]. A study in rats with type 2 diabetes examining the effects of ethanol extract and butanol fraction of spirulina on insulin release and glucose homeostasis reported that the ethanol extract and butanol fraction stimulated insulin release from the pancreatic β-cells in a concentration dependent manner [
36]. The butanol fraction also similarly stimulated insulin release from perfused rat pancreas by inhibiting dipeptidyl peptidase-4 (DPP-4) activity [
36]. This is an important effect of spirulina since DPP-4 is a cytokine secreted from the adipocytes, and has been shown to suppress insulin signaling and induce insulin resistance in muscle in vitro; furthermore, its plasma levels are increased in obesity and correlate positively with all parameters of the metabolic syndrome [
45]. Spirulina was also reported to significantly decrease postprandial hyperglycemia after oral sucrose load and increase unabsorbed sucrose content throughout the gut [
36]. During in situ intestinal perfusion with glucose, the butanol fraction reduced glucose absorption and promoted gut motility [
36]. Moreover, in rats with type 2 diabetes, chronic oral administration of butanol fraction for 28 days significantly decreased blood glucose, increased plasma insulin, pancreatic insulin stored, liver glycogen, and improved lipid profile [
36]. Lastly, a study using insulin resistant-HepG2 cell model, reported that spirulina protein had anti-diabetes effects in insulin resistant cell models, with 11 anti-diabetes peptides being identified, and LRSELAAWSR displaying the best activities on DPP-4 [
46].
Regarding BP, the results from the two current investigations showed that only the dose of 8 g spirulina as beverage lowered significantly SBP, but not DBP, acutely in 120 min posttest beverage consumption. Our results are in disagreement with one trial showing no BP effects in overweight or obese elderly after 12 weeks of 8 g spirulina supplementation [
15], and one trial showing significant decrease only in DBP in people with type 2 diabetes after 12 weeks of 8 g spirulina supplementation [
16]. Our results regarding lower doses are in partial agreement with two trials showing no BP effects in people with NAFLD, after 2 g or 6 g of spirulina supplementation [
17,
18]. Our results are in partial agreement with two trials showing significant decreases in SBP and DBP in overweight individuals after 6 weeks of 4.5 g spirulina supplementation [
19], and another trial showing significant decreases in SBP, but not DBP, in people with systemic arterial hypertension after 12 weeks of 4.5 g spirulina supplementation [
21]. Our results are also in partial agreement with a trial showing significant decreases in SBP, but not DBP, in people with hypertension and overweight without other cardiovascular disease risk factors after 3 months of 2 g spirulina supplementation [
20]. It has been reported that the BP beneficial changes are observed in both sexes, and that youngest people were more BP responsive to spirulina than the other age groups [
19]. A diet supplemented with spirulina has been suggested to prevent the synthesis and release of vasoconstricting metabolites to arachidonic acid induced by fructose and attenuated tension development in response to phenylephrine [
47]. Vasoconstriction is a fundamental mechanism contributing to the development of atherosclerosis [
48]. Others have also shown increased spirulina-induced nitric oxide endothelium synthesis and release, a well-known vasodilator metabolite [
49]. Moreover, it has been reported that the C-phycocyanin content in spirulina inhibited platelet aggregation through inhibition of calcium mobilization and mediation of free radicals released by platelet [
50]. It has also been proposed that high potassium and low sodium contents of spirulina may have positive effects on BP. A pooled data analysis reported that spirulina consumption was associated with a significant decrease in DBP [
39]. In an ex vivo vessel model, the peptide fraction isolated from spirulina showed direct endothelium-dependent vasodilation. This mechanism was proposed to be through a phosphoinositide-3-kinase (PI3K)/AKT (serine/threonine kinase AKT) pathway that converges on nitric oxide release [
51]. The peptide induced a significant reduction in BP in vivo [
51]. Substances, such as the tripeptide lle-Gln-Pro (IQP) present in spirulina also showed antihypertensive activity by inhibiting angiotensin converting enzymes [
52]. A meta-analysis of 5 RCTs that included 230 people to examine spirulina’s effects on BP as supplement, in doses from 1 to 8 g spirulina/day, for 2 to 12 weeks, reported that spirulina decreased SBP by about 4.6 mmHg and DBP by 7 mmHg [
53], which is in partial agreement with our results.
Results from our current investigations showed no changes in acute appetite scores after consumption of different doses of spirulina. Our findings disagree with two other studies using 1–2 g spirulina supplementation for 12 weeks in overweight or obese individuals showing significantly lower appetite scores after spirulina supplementation [
22,
23]. The lack of reported beneficial effects on appetite scores in our current investigations may be due to the short duration of the trials, which should be further investigated.



 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}