

Effects of Seven Weeks of Combined Physical Training on High-Density Lipoprotein Functionality in Overweight/Obese Subjects
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
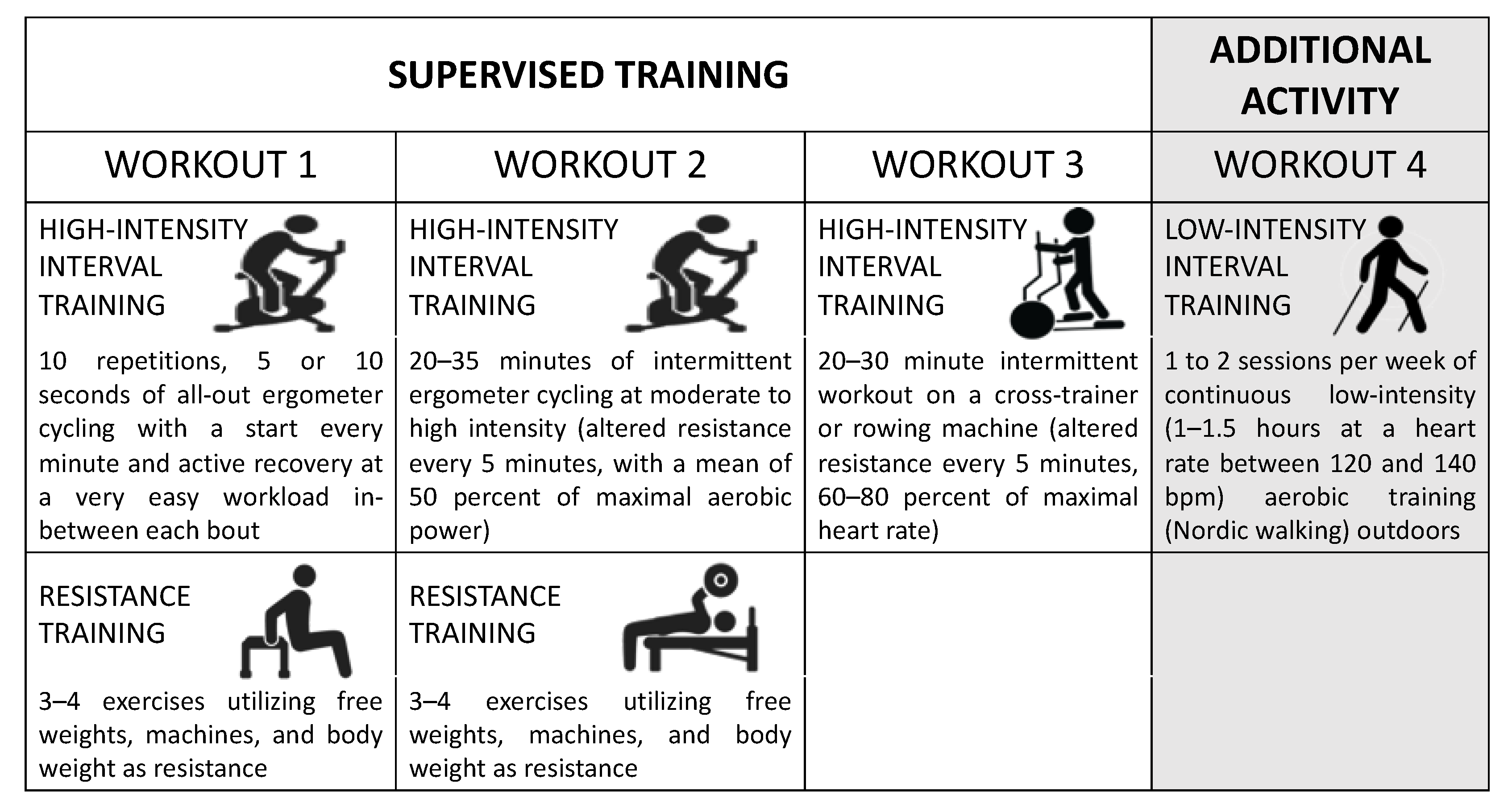
2.2. Exercise Training
- A total of 10 repetitions of 5 or 10 s (varied from week to week) of all-out ergometer cycling, with a start every minute and active recovery at a very easy workload in between each bout.
- A total of 20–35 min of intermittent ergometer cycling at moderate-to-high intensity (altered resistance every 5 min, with a mean of 50 per cent of maximal aerobic power).
- One 20–30 min intermittent workout with a cross-trainer or rowing machine (altered resistance every 5 min, with 60–80 per cent of maximal heart rate).
2.3. Test for Aerobic Capacity and Muscle Strength
2.4. Levels of Lipoproteins, Insulin, Glucose and hsCRP
2.5. Serum Total Antioxidant Potential (PAT)
2.6. Levels of Oxidized LDL (ox-LDL)
2.7. Myeloperoxidase (MPO) Levels
2.8. Paraoxonase-1 (PON1) Activity
2.9. HDL Redox Activity
2.10. Statistical Analysis
3. Results
3.1. Anthropometric and Biochemical Characteristics
3.2. Serum PON1 Activity and MPO Levels
3.3. HDL Redox Activity
3.4. Serum Lipid Peroxidation and Antioxidant Potential
3.5. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, T.; Chen, J.; Tang, X.; Luo, Q.; Xu, D.; Yu, B. Interaction between adipocytes and high-density lipoprotein:new insights into the mechanism of obesity-induced dyslipidemia and atherosclerosis. Lipids Health Dis. 2019, 18, 223. [Google Scholar] [CrossRef]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef]
- Luo, L.; Liu, M. Adipose tissue in control of metabolism. J. Endocrinol. 2016, 231, R77–R99. [Google Scholar] [CrossRef]
- Reho, J.J.; Rahmouni, K. Oxidative and inflammatory signals in obesity-associated vascular abnormalities. Clin. Sci. 2017, 131, 1689–1700. [Google Scholar] [CrossRef]
- Wang, H.; Peng, D.Q. New insights into the mechanism of low high-density lipoprotein cholesterol in obesity. Lipids Health Dis. 2011, 10, 176. [Google Scholar] [CrossRef]
- Stadler, J.T.; Lackner, S.; Morkl, S.; Trakaki, A.; Scharnagl, H.; Borenich, A.; Wonisch, W.; Mangge, H.; Zelzer, S.; Meier-Allard, N.; et al. Obesity Affects HDL Metabolism, Composition and Subclass Distribution. Biomedicines 2021, 9, 242. [Google Scholar] [CrossRef]
- Stadler, J.T.; Marsche, G. Obesity-Related Changes in High-Density Lipoprotein Metabolism and Function. Int. J. Mol. Sci. 2020, 21, 8985. [Google Scholar] [CrossRef]
- Azmi, S.; Ferdousi, M.; Liu, Y.; Adam, S.; Siahmansur, T.; Ponirakis, G.; Marshall, A.; Petropoulos, I.N.; Ho, J.H.; Syed, A.A.; et al. The role of abnormalities of lipoproteins and HDL functionality in small fibre dysfunction in people with severe obesity. Sci. Rep. 2021, 11, 12573. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T.; Masciangelo, S.; Bicchiega, V. HDL-paraoxonase and membrane lipid peroxidation: A comparison between healthy and obese subjects. Obesity 2010, 18, 1079–1084. [Google Scholar] [CrossRef]
- Dogan, K.; Senes, M.; Karaca, A.; Kayalp, D.; Kan, S.; Gulcelik, N.E.; Aral, Y.; Yucel, D. HDL subgroups and their paraoxonase-1 activity in the obese, overweight and normal weight subjects. Int. J. Clin. Pract. 2021, 75, e14969. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T.; Masciangelo, S.; Grugni, G.; Bicchiega, V. Altered inflammation, paraoxonase-1 activity and HDL physicochemical properties in obese humans with and without Prader-Willi syndrome. Dis. Model. Mech. 2012, 5, 698–705. [Google Scholar] [CrossRef]
- Khalil, A.; Kamtchueng Simo, O.; Ikhlef, S.; Berrougui, H. The role of paraoxonase 1 in regulating high-density lipoprotein functionality during aging. Can. J. Physiol. Pharmacol. 2017, 95, 1254–1262. [Google Scholar] [CrossRef]
- Bacchetti, T.; Ferretti, G.; Sahebkar, A. The role of paraoxonase in cancer. Semin. Cancer Biol. 2019, 56, 72–86. [Google Scholar] [CrossRef]
- Kotur-Stevuljevic, J.; Vekic, J.; Stefanovic, A.; Zeljkovic, A.; Ninic, A.; Ivanisevic, J.; Miljkovic, M.; Sopic, M.; Munjas, J.; Mihajlovic, M.; et al. Paraoxonase 1 and atherosclerosis-related diseases. Biofactors 2020, 46, 193–205. [Google Scholar] [CrossRef]
- Olza, J.; Aguilera, C.M.; Gil-Campos, M.; Leis, R.; Bueno, G.; Martinez-Jimenez, M.D.; Valle, M.; Canete, R.; Tojo, R.; Moreno, L.A.; et al. Myeloperoxidase is an early biomarker of inflammation and cardiovascular risk in prepubertal obese children. Diabetes Care 2012, 35, 2373–2376. [Google Scholar] [CrossRef]
- Qaddoumi, M.G.; Alanbaei, M.; Hammad, M.M.; Al Khairi, I.; Cherian, P.; Channanath, A.; Thanaraj, T.A.; Al-Mulla, F.; Abu-Farha, M.; Abubaker, J. Investigating the Role of Myeloperoxidase and Angiopoietin-like Protein 6 in Obesity and Diabetes. Sci. Rep. 2020, 10, 6170. [Google Scholar] [CrossRef]
- Bergt, C.; Pennathur, S.; Fu, X.; Byun, J.; O’Brien, K.; McDonald, T.O.; Singh, P.; Anantharamaiah, G.M.; Chait, A.; Brunzell, J.; et al. The myeloperoxidase product hypochlorous acid oxidizes HDL in the human artery wall and impairs ABCA1-dependent cholesterol transport. Proc. Natl. Acad. Sci. USA 2004, 101, 13032–13037. [Google Scholar] [CrossRef]
- Bacchetti, T.; Ferretti, G.; Carbone, F.; Ministrini, S.; Montecucco, F.; Jamialahmadi, T.; Sahebkar, A. Dysfunctional High-density Lipoprotein: The Role of Myeloperoxidase and Paraoxonase-1. Curr. Med. Chem. 2021, 28, 2842–2850. [Google Scholar] [CrossRef]
- Marsche, G.; Stadler, J.T.; Kargl, J.; Holzer, M. Understanding Myeloperoxidase-Induced Damage to HDL Structure and Function in the Vessel Wall: Implications for HDL-Based Therapies. Antioxidants 2022, 11, 556. [Google Scholar] [CrossRef]
- Jin, Z.; Zhou, L.; Tian, R.; Lu, N. Myeloperoxidase Targets Apolipoprotein A-I for Site-Specific Tyrosine Chlorination in Atherosclerotic Lesions and Generates Dysfunctional High-Density Lipoprotein. Chem. Res. Toxicol. 2021, 34, 1672–1680. [Google Scholar] [CrossRef]
- Haraguchi, Y.; Toh, R.; Hasokawa, M.; Nakajima, H.; Honjo, T.; Otsui, K.; Mori, K.; Miyamoto-Sasaki, M.; Shinohara, M.; Nishimura, K.; et al. Serum myeloperoxidase/paraoxonase 1 ratio as potential indicator of dysfunctional high-density lipoprotein and risk stratification in coronary artery disease. Atherosclerosis 2014, 234, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Ertek, S. High-density Lipoprotein (HDL) Dysfunction and the Future of HDL. Curr. Vasc. Pharmacol. 2018, 16, 490–498. [Google Scholar] [CrossRef]
- Zvintzou, E.; Xepapadaki, E.; Skroubis, G.; Mparnia, V.; Giannatou, K.; Benabdellah, K.; Kypreos, K.E. High-Density Lipoprotein in Metabolic Disorders and Beyond: An Exciting New World Full of Challenges and Opportunities. Pharmaceuticals 2023, 16, 855. [Google Scholar] [CrossRef] [PubMed]
- Tsompanidi, E.M.; Brinkmeier, M.S.; Fotiadou, E.H.; Giakoumi, S.M.; Kypreos, K.E. HDL biogenesis and functions: Role of HDL quality and quantity in atherosclerosis. Atherosclerosis 2010, 208, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H. The Current Status of Research on High-Density Lipoproteins (HDL): A Paradigm Shift from HDL Quantity to HDL Quality and HDL Functionality. Int. J. Mol. Sci. 2022, 23, 3967. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.H.; Yang, H.Y.; Shun, S.C. Effect of exercise intervention dosage on reducing visceral adipose tissue: A systematic review and network meta-analysis of randomized controlled trials. Int. J. Obes. 2021, 45, 982–997. [Google Scholar] [CrossRef]
- Rao, S.; Pandey, A.; Garg, S.; Park, B.; Mayo, H.; Despres, J.P.; Kumbhani, D.; de Lemos, J.A.; Neeland, I.J. Effect of Exercise and Pharmacological Interventions on Visceral Adiposity: A Systematic Review and Meta-analysis of Long-term Randomized Controlled Trials. Mayo Clin. Proc. 2019, 94, 211–224. [Google Scholar] [CrossRef]
- Khalafi, M.; Sakhaei, M.H.; Kazeminasab, F.; Rosenkranz, S.K.; Symonds, M.E. Exercise training, dietary intervention, or combined interventions and their effects on lipid profiles in adults with overweight and obesity: A systematic review and meta-analysis of randomized clinical trials. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1662–1683. [Google Scholar] [CrossRef]
- Jamka, M.; Makarewicz-Bukowska, A.; Bokayeva, K.; Smidowicz, A.; Geltz, J.; Kokot, M.; Kaczmarek, N.; Zok, A.; Kononets, V.; Cielecka-Piontek, J.; et al. Comparison of the Effect of Endurance, Strength and Endurance-Strength Training on Glucose and Insulin Homeostasis and the Lipid Profile of Overweight and Obese Subjects: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14928. [Google Scholar] [CrossRef]
- Franczyk, B.; Gluba-Brzozka, A.; Cialkowska-Rysz, A.; Lawinski, J.; Rysz, J. The Impact of Aerobic Exercise on HDL Quantity and Quality: A Narrative Review. Int. J. Mol. Sci. 2023, 24, 4653. [Google Scholar] [CrossRef]
- Cho, K.H.; Nam, H.S.; Kang, D.J.; Zee, S.; Park, M.H. Enhancement of High-Density Lipoprotein (HDL) Quantity and Quality by Regular and Habitual Exercise in Middle-Aged Women with Improvements in Lipid and Apolipoprotein Profiles: Larger Particle Size and Higher Antioxidant Ability of HDL. Int. J. Mol. Sci. 2023, 24, 1151. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ramie, J.J.; Barber, J.L.; Sarzynski, M.A. Effects of exercise on HDL functionality. Curr. Opin. Lipidol. 2019, 30, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Ridefelt, P.; Hagstrom, E.; Svensson, M.K.; Akerfeldt, T.; Larsson, A. Age- and sex-specific reference values for non-HDL cholesterol and remnant cholesterol derived from the Nordic Reference Interval Project (NORIP). Scand. J. Clin. Lab. Investig. 2019, 79, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Bacchetti, T.; Tullii, D.; Masciangelo, S.; Brugè, F.; Silvestri, S.; Orlando, P.; Tiano, L.; Ferretti, G. Correlation between plasma levels of carotenoid and oxidized low density lipoproteins: A short human intervention study. Integr. Food Nutr. Metab. 2016, 3, 283–288. [Google Scholar] [CrossRef]
- Aviram, M.; Rosenblat, M. Paraoxonases (PON1, PON2, PON3) analyses in vitro and in vivo in relation to cardiovascular diseases. Methods Mol. Biol. 2008, 477, 259–276. [Google Scholar] [CrossRef]
- Kelesidis, T.; Currier, J.S.; Huynh, D.; Meriwether, D.; Charles-Schoeman, C.; Reddy, S.T.; Fogelman, A.M.; Navab, M.; Yang, O.O. A biochemical fluorometric method for assessing the oxidative properties of HDL. J. Lipid Res. 2011, 52, 2341–2351. [Google Scholar] [CrossRef]
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [CrossRef]
- Variji, A.; Shokri, Y.; Fallahpour, S.; Zargari, M.; Bagheri, B.; Abediankenari, S.; Alizadeh, A.; Mahrooz, A. The combined utility of myeloperoxidase (MPO) and paraoxonase 1 (PON1) as two important HDL-associated enzymes in coronary artery disease: Which has a stronger predictive role? Atherosclerosis 2019, 280, 7–13. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports, M. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Greene, N.P.; Martin, S.E.; Crouse, S.F. Acute exercise and training alter blood lipid and lipoprotein profiles differently in overweight and obese men and women. Obesity 2012, 20, 1618–1627. [Google Scholar] [CrossRef] [PubMed]
- Wedell-Neergaard, A.S.; Eriksen, L.; Gronbaek, M.; Pedersen, B.K.; Krogh-Madsen, R.; Tolstrup, J. Low fitness is associated with abdominal adiposity and low-grade inflammation independent of BMI. PLoS ONE 2018, 13, e0190645. [Google Scholar] [CrossRef]
- Mathew, A.V.; Li, L.; Byun, J.; Guo, Y.; Michailidis, G.; Jaiswal, M.; Chen, Y.E.; Pop-Busui, R.; Pennathur, S. Therapeutic Lifestyle Changes Improve HDL Function by Inhibiting Myeloperoxidase-Mediated Oxidation in Patients With Metabolic Syndrome. Diabetes Care 2018, 41, 2431–2437. [Google Scholar] [CrossRef] [PubMed]
- Petric, B.; Kunej, T.; Bavec, A. A Multi-Omics Analysis of PON1 Lactonase Activity in Relation to Human Health and Disease. OMICS 2021, 25, 38–51. [Google Scholar] [CrossRef]
- Cirilli, I.; Silvestri, S.; Marcheggiani, F.; Olivieri, F.; Galeazzi, R.; Antonicelli, R.; Recchioni, R.; Marcheselli, F.; Bacchetti, T.; Tiano, L.; et al. Three Months Monitored Metabolic Fitness Modulates Cardiovascular Risk Factors in Diabetic Patients. Diabetes Metab. J. 2019, 43, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Evelson, P.; Gambino, G.; Travacio, M.; Jaita, G.; Verona, J.; Maroncelli, C.; Wikinski, R.; Llesuy, S.; Brites, F. Higher antioxidant defences in plasma and low density lipoproteins from rugby players. Eur. J. Clin. Investig. 2002, 32, 818–825. [Google Scholar] [CrossRef]
- Goldhammer, E.; Ben-Sira, D.; Zaid, G.; Biniamini, Y.; Maor, I.; Lanir, A.; Sagiv, M. Paraoxonase activity following exercise-based cardiac rehabilitation program. J. Cardiopulm. Rehabil. Prev. 2007, 27, 151–154. [Google Scholar] [CrossRef]
- Hematinezhad Touli, M.; Elmieh, A.; Hosseinpour, A. The Effect of Six-Week Aerobic Exercise Combined with ease max Incr2Green Tea Consumption on PON1 and VOand Apelin, Blood Pressure, and Blood Lipids Reduction in Young Obese Men. Arch. Razi Inst. 2022, 77, 2115–2123. [Google Scholar] [CrossRef]
- Streb, A.R.; Braga, P.G.S.; de Melo, R.F.; Botelho, L.J.; Maranhao, R.C.; Del Duca, G.F. Effects of combined physical exercise on plasma lipid variables, paraoxonase 1 activity, and inflammation parameters in adults with obesity: A randomized clinical trial. J. Endocrinol. Investig. 2022, 45, 1991–1997. [Google Scholar] [CrossRef]
- Woudberg, N.J.; Mendham, A.E.; Katz, A.A.; Goedecke, J.H.; Lecour, S. Exercise intervention alters HDL subclass distribution and function in obese women. Lipids Health Dis. 2018, 17, 232. [Google Scholar] [CrossRef]
- Roberts, C.K.; Ng, C.; Hama, S.; Eliseo, A.J.; Barnard, R.J. Effect of a short-term diet and exercise intervention on inflammatory/anti-inflammatory properties of HDL in overweight/obese men with cardiovascular risk factors. J. Appl. Physiol. 2006, 101, 1727–1732. [Google Scholar] [CrossRef] [PubMed]
- Otocka-Kmiecik, A.; Orlowska-Majdak, M. The role of genetic (PON1 polymorphism) and environmental factors, especially physical activity, in antioxidant function of paraoxonase. Postep. Hig. Med. Dosw. 2009, 63, 668–677. [Google Scholar]
- Fuhrman, B. Regulation of hepatic paraoxonase-1 expression. J. Lipids 2012, 2012, 684010. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, G.; Bacchetti, T. Effect of dietary lipids on paraoxonase-1 activity and gene expression. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 88–94. [Google Scholar] [CrossRef]
- Aviram, M.; Rosenblat, M.; Bisgaier, C.L.; Newton, R.S.; Primo-Parmo, S.L.; La Du, B.N. Paraoxonase inhibits high-density lipoprotein oxidation and preserves its functions. A possible peroxidative role for paraoxonase. J. Clin. Investig. 1998, 101, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wu, Z.; Riwanto, M.; Gao, S.; Levison, B.S.; Gu, X.; Fu, X.; Wagner, M.A.; Besler, C.; Gerstenecker, G.; et al. Myeloperoxidase, paraoxonase-1, and HDL form a functional ternary complex. J. Clin. Investig. 2013, 123, 3815–3828. [Google Scholar] [CrossRef]
- Malle, E.; Marsche, G.; Panzenboeck, U.; Sattler, W. Myeloperoxidase-mediated oxidation of high-density lipoproteins: Fingerprints of newly recognized potential proatherogenic lipoproteins. Arch. Biochem. Biophys. 2006, 445, 245–255. [Google Scholar] [CrossRef]
- Oh, E.G.; Bang, S.Y.; Kim, S.H.; Hyun, S.S.; Chu, S.H.; Jeon, J.Y.; Im, J.A.; Lee, J.E.; Lee, M.K. Therapeutic lifestyle modification program reduces plasma levels of the chemokines CRP and MCP-1 in subjects with metabolic syndrome. Biol. Res. Nurs. 2013, 15, 48–55. [Google Scholar] [CrossRef]
- Pennathur, S.; Jaiswal, M.; Vivekanandan-Giri, A.; White, E.A.; Ang, L.; Raffel, D.M.; Rubenfire, M.; Pop-Busui, R. Structured lifestyle intervention in patients with the metabolic syndrome mitigates oxidative stress but fails to improve measures of cardiovascular autonomic neuropathy. J. Diabetes Complicat. 2017, 31, 1437–1443. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| PRE (Mean ± SD) | POST (Mean ± SD) | p Value | |
|---|---|---|---|
| Anthropometrics | |||
| Body weight (kg) | 93.2 ± 12.5 | 93.3 ± 12.4 | 0.990 |
| BMI (kg‧m−2) | 30.3 ± 2.5 | 30.3 ± 2.6 | 0.867 |
| Fat mass (kg) | 37.1 ± 8.2 | 35.7 ± 8.3 | <0.001 |
| FMI (kg‧m−2) | 12.1 ± 2.6 | 11.6 ± 2.6 | <0.001 |
| Lean mass (kg) | 52.3 ± 8.6 | 54.4 ± 8.6 | <0.0001 |
| LMI (kg‧m−2) | 17.2 ± 1.6 | 17.6 ± 1.7 | 0.0002 |
| Visceral fat mass (kg) | 1.1 ± 0.6 | 0.9 ± 0.8 | 0.0076 |
| Waist circumference (cm) | 95.6 ± 8.6 | 93.8 ± 8.3 | 0.0081 |
| Aerobic capacity and muscle strength | |||
| VO2max (L‧min−1) | 3.3 ± 0.7 | 3.7 ± 0.8 | 0.0002 |
| Leg press (kg) | 280.0 ± 86.7 | 483.3 ± 177.4 | <0.0001 |
| Biochemical parameters | |||
| TGs (mmol/L) | 1.38 ± 0.72 | 1.39 ± 0.77 | 0.89 |
| TC (mmol/L) | 5.07 ± 0.99 | 4.61 ± 1.48 | 0.031 |
| HDL-C (mmol/L) | 1.54 ± 0.29 | 1.47 ± 0.32 | 0.123 |
| Non-HDL cholesterol (mmol/L) | 3.53 ± 1.01 | 3.14 ± 1.45 | 0.059 |
| Apo AI (g/L) | 1.62 ± 0.22 | 1.56 ± 0.19 | 0.44 |
| Apo B (g/L) | 0.92 ± 0.26 | 0.90 ± 0.31 | 0.66 |
| hsCRP (mg/L) | 3.39 ± 3,51 | 2.59 ± 2.17 | 0.348 |
| HOMA-IR | 3.72 ± 2,09 | 2.99 ± 1.93 | 0.106 |
| Fasting glucose (mmol/L) | 5.27 ± 0.46 | 5.52 ± 0.56 | 0.189 |
| Fasting insulin (mUI/L) | 16.40 ± 11.36 | 11.84 ± 6.56 | 0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bacchetti, T.; Morresi, C.; Ferretti, G.; Larsson, A.; Åkerfeldt, T.; Svensson, M. Effects of Seven Weeks of Combined Physical Training on High-Density Lipoprotein Functionality in Overweight/Obese Subjects. Metabolites 2023, 13, 1068. https://doi.org/10.3390/metabo13101068
Bacchetti T, Morresi C, Ferretti G, Larsson A, Åkerfeldt T, Svensson M. Effects of Seven Weeks of Combined Physical Training on High-Density Lipoprotein Functionality in Overweight/Obese Subjects. Metabolites. 2023; 13(10):1068. https://doi.org/10.3390/metabo13101068
Chicago/Turabian StyleBacchetti, Tiziana, Camilla Morresi, Gianna Ferretti, Anders Larsson, Torbjörn Åkerfeldt, and Michael Svensson. 2023. "Effects of Seven Weeks of Combined Physical Training on High-Density Lipoprotein Functionality in Overweight/Obese Subjects" Metabolites 13, no. 10: 1068. https://doi.org/10.3390/metabo13101068