
Evaluation of Anti-Inflammatory Effect of Moringa oleifera Lam. and Cyanthillium cinereum (Less) H. Rob. Lozenges in Volunteer Smokers

 ,
, 
Abstract

1. Introduction
2. Results
2.1. Quality Control of Lozenges
2.2. Total Phenolic Content
2.3. Anti-Oxidant Activity
2.4. Subjects Characteristic and Clinical Laboratory Measurement
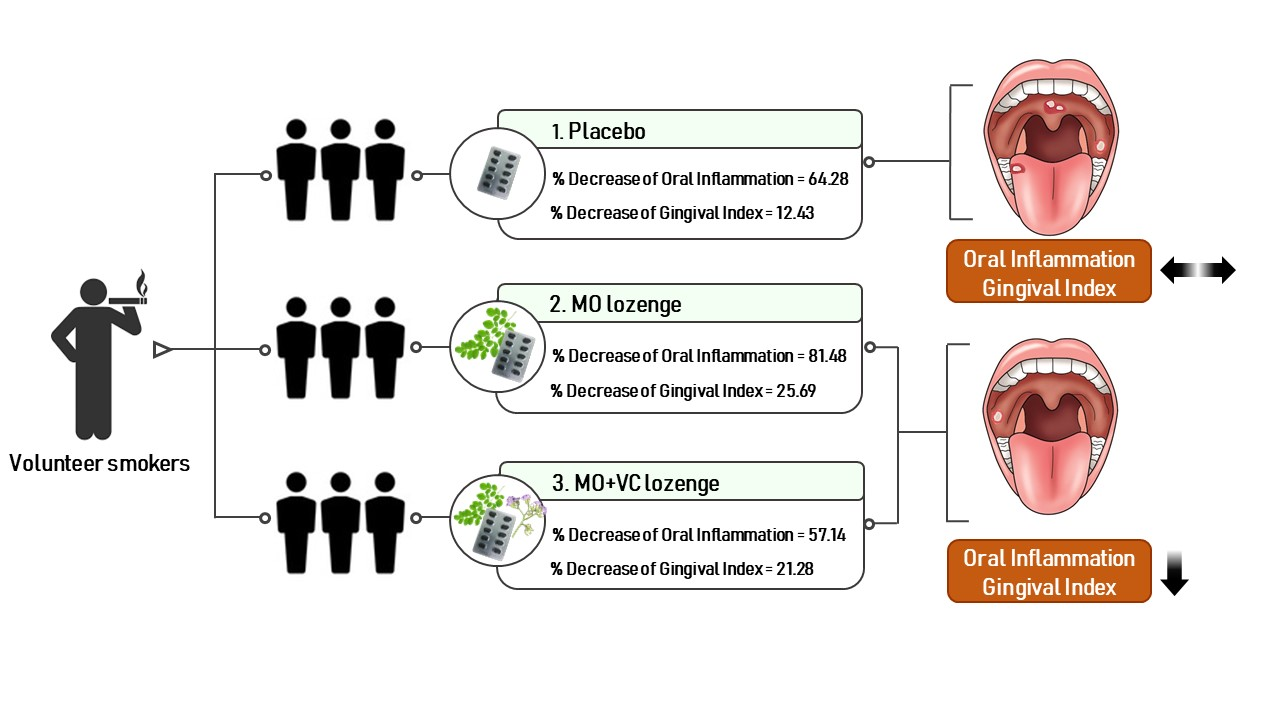
2.5. The Anti-Inflammation of Lozenge in Smokers
2.6. The Satisfaction and Lozenge Usage of Smokers and Control Group
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Plant Extraction
4.3. Dose Calculation of MO and CC Extract in Lozenge
4.4. Lozenge Formulation and Evaluation
4.5. Gas Chromatography Mass Spectroscopy (GC/MS) Analysis
4.6. High Performance Liquid Chromatography (HPLC) Analysis
4.7. Determination of Total Phenolic Contents
4.8. Determination of Antioxidant Activity
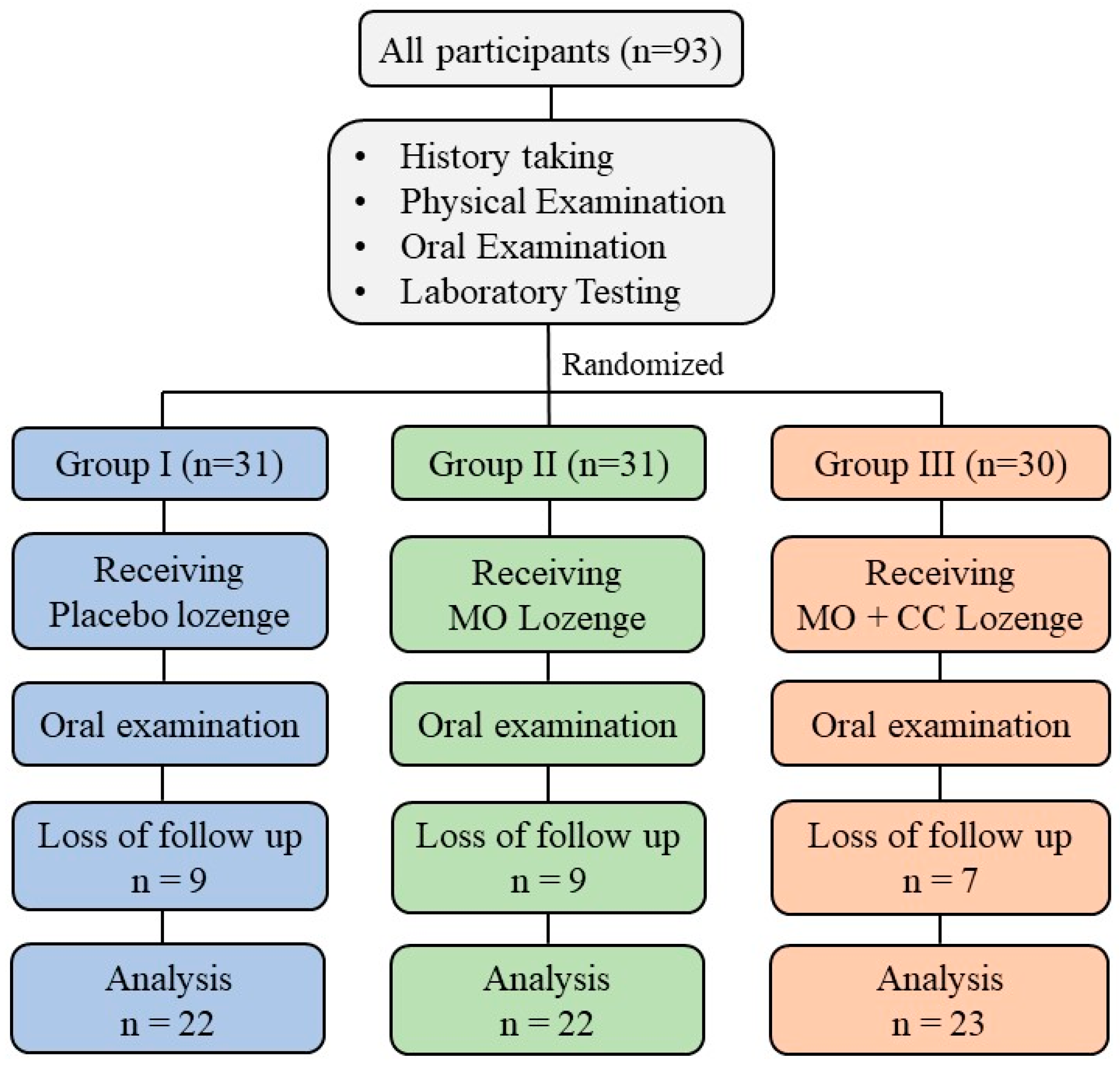
4.9. Study Design
4.10. Subjects
4.11. Sample Size
- n = sample size
- Zα = The critical value from the standard normal distribution, α = 0.05 and Zα = 1.96.
- Zβ = The critical value from the standard normal distribution, β = 0.2 and Zβ= 0.84
- P1 = Mean of population 1 or study group
- P2 = Mean of population 2 or control group
- D = Expected mean difference between the study group and the control group
4.12. Study Procedure
4.13. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cunningham, F.; Fiebelkorn, S.; Johnson, M.; Meredith, C. A novel application of the Margin of Exposure approach: Segregation of tobacco smoke toxicants. Food Chem. Toxicol. 2011, 49, 2921–2933. [Google Scholar] [CrossRef]
- Lee, J.; Taneja, V.; Vassallo, R. Cigarette smoking and inflammation: Cellular and molecular mechanisms. J. Dent. Res. 2012, 91, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Arnson, Y.; Shoenfeld, Y.; Amital, H. Effects of tobacco smoke on immunity, inflammation and autoimmunity. J. Autoimmun. 2010, 34, J258–J265. [Google Scholar] [CrossRef]
- Rom, O.; Avezov, K.; Aizenbud, D.; Reznick, A.Z. Cigarette smoking and inflammation revisited. Respir. Physiol. Neurobiol. 2013, 187, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Reibel, J. Tobacco and oral diseases. Update on the evidence, with recommendations. Med. Princ. Pract. 2003, 12, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Vellappally, S.; Fiala, Z.; Smejkalová, J.; Jacob, V.; Somanathan, R. Smoking related systemic and oral diseases. Acta Med. 2007, 50, 161–166. [Google Scholar] [CrossRef][Green Version]
- Winn, D.M. Tobacco use and oral disease. J. Dent. Educ. 2001, 65, 306–312. [Google Scholar] [CrossRef]
- Hoare, A.; Soto, C.; Rojas-Celis, V.; Bravo, D. Chronic Inflammation as a Link between Periodontitis and Carcinogenesis. Mediat. Inflamm. 2019, 2019, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Evidence-Based Update on Diagnosis and Management of Gingivitis and Periodontitis. Dent. Clin. 2019, 63, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Geisinger, M.L.; Kaur, M.; Basma, H. Nonsurgical Periodontal Therapy: A Review of Current Standards of Care and Innovations to Improve Gingival and Periodontal Health. Curr. Oral Health Rep. 2019, 6, 177–187. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontol. 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Tariq, M.; Iqbal, Z.; Ali, J.; Baboota, S.; Talegaonkar, S.; Ahmad, Z.; Sahni, J.K. Treatment modalities and evaluation models for periodontitis. Int. J. Pharm. Investig. 2012, 2, 106–122. [Google Scholar] [PubMed]
- Arulselvan, P.; Fard, M.T.; Tan, W.S.; Gothai, S.; Fakurazi, S.; Norhaizan, M.E.; Kumar, S.S. Role of Antioxidants and Natural Products in Inflammation. Oxidative Med. Cell. Longev. 2016, 2016, 5276130. [Google Scholar] [CrossRef]
- Hussain, T.; Tan, B.; Yin, Y.; Blachier, F.; Tossou, M.C.; Rahu, N. Oxidative Stress and Inflammation: What Polyphenols Can Do for Us? Oxidative Med. Cell. Longev. 2016, 2016, 7432797. [Google Scholar] [CrossRef]
- Bernstein, N.; Akram, M.; Daniyal, M.; Koltai, H.; Fridlender, M.; Gorelick, J. Antiinflammatory Potential of Medicinal Plants: A Source for Therapeutic Secondary Metabolites. Adv. Agron. 2018, 150, 131–183. [Google Scholar]
- Rao, Y.K.; Fang, S.H.; Tzeng, Y.M. Antiinflammatory activities of flavonoids and a triterpene caffeate isolated from Bauhinia variegata. Phytother. Res. 2008, 22, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Deters, A.M.; Hensel, A. Anti-inflammatory activity of Eupatorium perfoliatum L. extracts, eupafolin, and dimeric guaianolide via iNOS inhibitory activity and modulation of inflammation-related cytokines and chemokines. J. Ethnopharmacol. 2011, 137, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Hodge, G.; Hodge, S.; Han, P. Allium sativum (garlic) suppresses leukocyte inflammatory cytokine production in vitro: Potential therapeutic use in the treatment of inflammatory bowel disease. Cytometry 2002, 48, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.T.; Park, Y.M.; Shin, K.M.; Ha, J.; Choi, J.; Jung, H.J.; Park, H.J.; Lee, K.T. Anti-inflammatory and anti-nociceptive effects of the extract from Kalopanax pictus, Pueraria thunbergiana and Rhus verniciflua. J. Ethnopharmacol. 2004, 94, 165–173. [Google Scholar] [CrossRef]
- Al-Ghamdi, M.S. The anti-inflammatory, analgesic and antipyretic activity of Nigella sativa. J. Ethnopharmacol. 2001, 76, 45–48. [Google Scholar] [CrossRef]
- Lu, C.H.; Li, Y.Y.; Li, L.J.; Liang, L.Y.; Shen, Y.M. Anti-inflammatory activities of fractions from Geranium nepalense and related polyphenols. Drug Discov. Ther. 2012, 6, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.P.; Bitencourt, F.S.; Brito, G.A.; de Alencar, N.M.; Ribeiro, R.A.; Lima-Junior, R.C.; Ramos, M.V.; Vale, M.L. Protein fraction of Calotropis procera latex protects against 5-fluorouracil-induced oral mucositis associated with downregulation of pivotal pro-inflammatory mediators. Naunyn Schmiedeberg’s Arch. Pharmacol. 2012, 385, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Anwar, F.; Latif, S.; Ashraf, M.; Gilani, A.H. Moringa oleifera: A food plant with multiple medicinal uses. Phytother. Res. 2006, 21, 17–252007. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Spada, A.; Battezzati, A.; Schiraldi, A.; Aristil, J.; Bertoli, S. Cultivation, Genetic, Ethnopharmacology, Phytochemistry and Pharmacology of Moringa oleifera Leaves: An Overview. Int. J. Mol. Sci. 2015, 16, 12791–12835. [Google Scholar] [CrossRef]
- Abd Rani, N.Z.; Husain, K.; Kumolosasi, E. Moringa Genus: A Review of Phytochemistry and Pharmacology. Front. Pharmacol. 2018, 9, 108. [Google Scholar] [CrossRef] [PubMed]
- Kou, X.; Li, B.; Olayanju, J.B.; Drake, J.M.; Chen, N. Nutraceutical or Pharmacological Potential of Moringa oleifera Lam. Nutrients 2018, 10, 343. [Google Scholar] [CrossRef]
- de Oliveira, R.G.; Mahon, C.P.; Ascencio, P.G.; Ascencio, S.D.; Balogun, S.O.; de Oliveira Martins, D.T. Evaluation of anti-inflammatory activity of hydroethanolic extract of Dilodendron bipinnatum Radlk. J. Ethnopharmacol. 2014, 155, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.H.; Chao, W.W.; Chen, M.L.; Lin, B.F. Ethyl acetate extracts of alfalfa (Medicago sativa L.) sprouts inhibit lipopolysaccharide-induced inflammation in vitro and in vivo. J. Biomed. Sci. 2009, 16, 64. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.H.; Oh, Y.C.; Cho, W.K.; Lee, B.; Ma, J.Y. Anti-Inflammatory Effects of Melandrii Herba Ethanol Extract via Inhibition of NF-kappaB and MAPK Signaling Pathways and Induction of HO-1 in RAW 264.7 Cells and Mouse Primary Macrophages. Molecules 2016, 21, 818. [Google Scholar] [CrossRef]
- Kooltheat, N.; Sranujit, R.P.; Chumark, P.; Potup, P.; Laytragoon-Lewin, N.; Usuwanthim, K. An ethyl acetate fraction of Moringa oleifera Lam. Inhibits human macrophage cytokine production induced by cigarette smoke. Nutrients 2014, 6, 697–710. [Google Scholar] [CrossRef]
- Luetragoon, T.; Pankla Sranujit, R.; Noysang, C.; Thongsri, Y.; Potup, P.; Suphrom, N.; Nuengchamnong, N.; Usuwanthim, K. Bioactive Compounds in Moringa oleifera Lam. Leaves Inhibit the Pro-Inflammatory Mediators in Lipopolysaccharide-Induced Human Monocyte-Derived Macrophages. Molecules 2020, 25, 191. [Google Scholar] [CrossRef] [PubMed]
- Kooltheat, N.; Sranujit, R.; Luetragoon, T.; Yuchat, M.; Adulyaritthikul, P.; Chaisomboon, C.; Potup, P.; Ferrante, A.; Usuwanthim, K. Moringa oleifera Lam. leaves extract reduces human T-cell hyporesponsiveness and DNA damage induced by oxidative stress. Int. J. Res. Ayurveda Pharm. 2017, 8, 84–90. [Google Scholar] [CrossRef]
- Arulselvan, P.; Tan, W.S.; Gothai, S.; Muniandy, K.; Fakurazi, S.; Esa, N.M.; Alarfaj, A.A.; Kumar, S.S. Anti-Inflammatory Potential of Ethyl Acetate Fraction of Moringa oleifera in Downregulating the NF-kappaB Signaling Pathway in Lipopolysaccharide-Stimulated Macrophages. Molecules 2016, 21, 1452. [Google Scholar] [CrossRef] [PubMed]
- Waterman, C.; Cheng, D.M.; Rojas-Silva, P.; Poulev, A.; Dreifus, J.; Lila, M.A.; Raskin, I. Stable, water extractable isothiocyanates from Moringa oleifera leaves attenuate inflammation in vitro. Phytochemistry 2014, 103, 114–122. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, S.H. Inhibitory effect of astragalin on expression of lipopolysaccharide-induced inflammatory mediators through NF-kappaB in macrophages. Arch. Pharm. Res. 2011, 34, 2101–2107. [Google Scholar] [CrossRef]
- Li, F.; Liang, D.; Yang, Z.; Wang, T.; Wang, W.; Song, X.; Guo, M.; Zhou, E.; Li, D.; Cao, Y.; et al. Astragalin suppresses inflammatory responses via down-regulation of NF-kappaB signaling pathway in lipopolysaccharide-induced mastitis in a murine model. Int. Immunopharmacol. 2013, 17, 478–482. [Google Scholar] [CrossRef]
- Riaz, A.; Rasul, A.; Hussain, G.; Zahoor, M.K.; Jabeen, F.; Subhani, Z.; Younis, T.; Ali, M.; Sarfraz, I.; Selamoglu, Z. Astragalin: A Bioactive Phytochemical with Potential Therapeutic Activities. Adv. Pharmacol. Sci. 2018, 2018, 1–15. [Google Scholar] [CrossRef]
- Engsuwan, J.; Waranuchb, N.; Limpeanchobc, N.; Ingkaninana, B.K. HPLC methods for quality control of Moringa oleifera extract using isothiocyanates and astragalin as bioactive markers. ScienceAsia 2017, 43, 169–174. [Google Scholar] [CrossRef]
- Iwalewa, E.O.; Iwalewa, O.J.; Adeboye, J.O. Analgesic, antipyretic, anti-inflammatory effects of methanol, chloroform and ether extracts of Vernonia cinerea less leaf. J. Ethnopharmacol. 2003, 86, 229–234. [Google Scholar] [CrossRef]
- Joshi, T.; Pandey, S.C.; Maiti, P.; Tripathi, M.; Paliwal, A.; Nand, M.; Sharma, P.; Samant, M.; Pande, V.; Chandra, S. Antimicrobial activity of methanolic extracts of Vernonia cinerea against Xanthomonas oryzae and identification of their compounds using in silico techniques. PLoS ONE 2021, 16, e0252759. [Google Scholar] [CrossRef]
- Yusoff, S.F.; Haron, F.F.; Tengku Muda Mohamed, M.; Asib, N.; Sakimin, S.Z.; Abu Kassim, F.; Ismail, S.I. Antifungal Activity and Phytochemical Screening of Vernonia amygdalina Extract against Botrytis cinerea Causing Gray Mold Disease on Tomato Fruits. Biology 2020, 9, 286. [Google Scholar] [CrossRef]
- Puttarak, P.; Pornpanyanukul, P.; Meetam, T.; Bunditanukul, K.; Chaiyakunapruk, N. Efficacy and safety of Vernonia cinerea (L.) Less. for smoking cessation: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2018, 37, 37–42. [Google Scholar] [CrossRef]
- Wongwiwatthananukit, S.; Benjanakaskul, P.; Songsak, T.; Suwanamajo, S.; Verachai, V. Efficacy of Vernonia cinerea for smoking cessation. J. Health Res. 2009, 23, 31–36. [Google Scholar]
- Singh, A.; Saharan, V.A.; Kumawat, I.C.; Khatri, A.; Bhandari, A. A pharmacognostical study of Vernonia cinerea Less (Asteraceae) and evaluation of anti-inflammatory and antibacterial activities of stem. Egypt Pharm. J. 2014, 13, 104–112. [Google Scholar] [CrossRef]
- Ketsuwan, N.; Leelarungrayub, J.; Kothan, S.; Singhatong, S. Antioxidant compounds and activities of the stem, flower, and leaf extracts of the anti-smoking Thai medicinal plant: Vernonia cinerea Less. Drug Des. Dev. Ther. 2017, 11, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Prasopthum, A.; Pouyfung, P.; Sarapusit, S.; Srisook, E.; Rongnoparut, P. Inhibition effects of Vernonia cinerea active compounds against cytochrome P450 2A6 and human monoamine oxidases, possible targets for reduction of tobacco dependence. Drug Metab. Pharmacokinet. 2015, 30, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Toyang, N.J.; Verpoorte, R. A review of the medicinal potentials of plants of the genus Vernonia (Asteraceae). J. Ethnopharmacol. 2013, 146, 681–723. [Google Scholar] [CrossRef]
- Saraphanchotiwitthaya, A.; Sripalakit, P. Anti-inflammatory activity of a Vernonia cinerea methanolic extract in vitro. ScienceAsia 2015, 41, 392–399. [Google Scholar] [CrossRef]
- Alara, O.R.; Abdurahman, N.H.; Ukaegbu, C.I.; Azhari, N.H. Vernonia cinerea leaves as the source of phenolic compounds, antioxidants, and anti-diabetic activity using microwave-assisted extraction technique. Ind. Crops Prod. 2018, 122, 533–544. [Google Scholar] [CrossRef]
- Sonibare, M.A.; Aremu, O.T.; Okorie, P.N. Antioxidant and antimicrobial activities of solvent fractions of Vernonia cinerea (L.) Less leaf extract. Afr. Health Sci. 2016, 16, 629–639. [Google Scholar] [CrossRef]
- Fitriana, W.D.; Ersam, T.; Shimizu, K.; Fatmawati, S. Antioxidant Activity of Moringa oleifera Extracts. Indones. J. Chem. 2016, 16, 297–301. [Google Scholar] [CrossRef]
- Xu, Y.B.; Chen, G.L.; Guo, M.Q. Antioxidant and Anti-Inflammatory Activities of the Crude Extracts of Moringa oleifera from Kenya and Their Correlations with Flavonoids. Antioxidants 2019, 8, 296. [Google Scholar] [CrossRef]
- Sreelatha, S.; Padma, P.R. Antioxidant activity and total phenolic content of Moringa oleifera leaves in two stages of maturity. Plant. Foods Hum. Nutr. 2009, 64, 303–311. [Google Scholar] [CrossRef]
- Gurenlian, J.R. Inflammation: The relationship between oral health and systemic disease. Dent. Assist. 2009, 78, 8–10, 12–14, 38–40, quiz 41-3. [Google Scholar] [PubMed]
- Elgamily, H.; Moussa, A.; Elboraey, A.; El-Sayed, H.; Al-Moghazy, M.; Abdalla, A. Microbiological Assessment of Moringa Oleifera Extracts and Its Incorporation in Novel Dental Remedies against Some Oral Pathogens. Open Access Maced. J. Med. Sci. 2016, 4, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Jwa, S.K. Efficacy of Moringa oleifera Leaf Extracts against Cariogenic Biofilm. Prev. Nutr. Food Sci. 2019, 24, 308–312. [Google Scholar] [CrossRef]
- Nagarajappa, R.; Bhanushali, N.V.; Ramesh, G.; Bhanushali, P.V.; Aapaliya, P.; Pujara, P. Antimicrobial Activity of Moringa Oleifera Extracts against Common Periodontal Pathogens: Potential Application in the Prevention and Treatment of Oral Diseases. Indian J. Public Health Res. Dev. 2019, 10, 243–248. [Google Scholar] [CrossRef]
- Gupta, M.; Mazumder, U.K.; Manikandan, L.; Haldar, P.K.; Bhattacharya, S.; Kandar, C.C. Antibacterial activity of Vernonia cinerea. Fitoterapia 2003, 74, 148–150. [Google Scholar] [CrossRef]
- Alshwerf, A.O.; Amin, L.S.; Ibrahim, F.; Youssef, J. Protective Effect of Moringa oleifera Extract on Experimentally LPS-induced periodontitis. Int. J. Adv. Res. 2017, 5, 1734–1740. [Google Scholar] [CrossRef]
- Sahrakary, M.; Nazemian, V.; Aghaloo, M.; Akbari, A.; Shadnoush, M.; Nasseri, B.; Zaringhalam, J. Treatment by Moringa Oleifera Extract Can Reduce Gingival Inflammatory Cytokines in the Rat Periodontal Model. Physiol. Pharmacol. 2017, 21, 102–109. [Google Scholar]
- Mohanty, M.; Mohanty, S.; Bhuyan, S.K.; Bhuyan, R. Phytoperspective of Moringa oleifera for oral health care: An innovative ethnomedicinal approach. Phytother. Res. 2020. [Google Scholar] [CrossRef]
- Rozza, A.L.; Meira de Faria, F.; Souza Brito, A.R.; Pellizzon, C.H. The gastroprotective effect of menthol: Involvement of anti-apoptotic, antioxidant and anti-inflammatory activities. PLoS ONE 2014, 9, e86686. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Wang, H.; Wang, J.; Zhou, L.; Yang, P. Chemical Composition and Anti-Inflammatory, Cytotoxic and Antioxidant Activities of Essential Oil from Leaves of Mentha piperita Grown in China. PLoS ONE 2014, 9, e114767. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.J.; Campbell, P.M.; Rees, T.D.; Buschang, P.H. A randomized controlled trial evaluating antioxidant-essential oil gel as a treatment for gingivitis in orthodontic patients. Angle Orthod. 2016, 86, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Bakre, A.G.; Aderibigbe, A.O.; Ademowo, O.G. Studies on neuropharmacological profile of ethanol extract of Moringa oleifera leaves in mice. J. Ethnopharmacol. 2013, 149, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Woo Shin, J.; Seol, I.C.; Son, C.G. Interpretation of Animal Dose and Human Equivalent Dose for Drug Development. J. Korean Med. 2010, 31, 1–7. [Google Scholar]
- Aruna, G.; Jayachandra Reddy, P.; Prabhakaran, V. Safety evaluation of ethanol extract of vernonia cinerea L. in experimental animals. Int. J. Pharm. 2012, 2, 34–38. [Google Scholar]
- Majekodunmi, S.O. A Review on Lozenges. Am. J. Med. Med. Sci. 2015, 5, 99–104. [Google Scholar]
- Medina-Remon, A.; Barrionuevo-Gonzalez, A.; Zamora-Ros, R.; Andres-Lacueva, C.; Estruch, R.; Martinez-Gonzalez, M.A.; Diez-Espino, J.; Lamuela-Raventos, R.M. Rapid Folin-Ciocalteu method using microtiter 96-well plate cartridges for solid phase extraction to assess urinary total phenolic compounds, as a biomarker of total polyphenols intake. Anal. Chim. Acta 2009, 634, 54–60. [Google Scholar] [CrossRef]
- Clarke, G.; Ting, K.N.; Wiart, C.; Fry, J. High Correlation of 2,2-diphenyl-1-picrylhydrazyl (DPPH) Radical Scavenging, Ferric Reducing Activity Potential and Total Phenolics Content Indicates Redundancy in Use of All Three Assays to Screen for Antioxidant Activity of Extracts of Plants from the Malaysian Rainforest. Antioxidants 2013, 2, 1–10. [Google Scholar]
- Zheng, J.Z.; Li, Y.; Lin, T.; Estrada, A.; Lu, X.; Feng, C. Sample Size Calculations for Comparing Groups with Continuous Outcomes. Shanghai Arch. Psychiatry 2017, 29, 250–256. [Google Scholar] [PubMed]
- Sonis, S.T.; Eilers, J.P.; Epstein, J.B.; LeVeque, F.G.; Liggett, W.H., Jr.; Mulagha, M.T.; Peterson, D.E.; Rose, A.H.; Schubert, M.M.; Spijkervet, F.K.; et al. Validation of a new scoring system for the assessment of clinical trial research of oral mucositis induced by radiation or chemotherapy. Mucositis Study Group. Cancer 1999, 85, 2103–2113. [Google Scholar] [CrossRef]
- Tobias, G.; Spanier, A.B. Modified Gingival Index (MGI) Classification Using Dental Selfies. Appl. Sci. 2020, 10, 8923. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Residual Solvent | |
|---|---|---|
| % (w/v) | ppm | |
| MO leaf extract | 5.74 | 57,400 |
| CC extract | 2.88 | 28,800 |
| Placebo | Not detected | - |
| MO lozenge | Not detected | - |
| MO + CC lozenge | Not detected | - |
| Sample | Astragalin Content |
|---|---|
| MO leaf extract (µg/g extract) | 5914.70 ± 260.36 |
| CC extract (µg/g extract) | 245.72 ± 8.81 |
| MO lozenge (µg/tablet) | 215.87 ± 19.57 |
| MO + CC lozenge (µg/tablet) | 176.69 ± 21.17 |
| Placebo | MO Lozenge | MO + CC Lozenge | p-Value | |
|---|---|---|---|---|
| (n = 22) | (n = 22) | (n = 24) | ||
| Sex: Male | 22 | 22 | 23 | |
| Age (years) | 37.14 ± 10.06 | 39.77 ± 11.93 | 29.13 ± 10.25 | ns |
| BMI (kg/m2) | 21.68 ± 4.6 | 20.72 ± 3.59 | 23.48 ± 4.05 | ns |
| Parameters | Placebo (n = 22) | p-Value | MO Lozenge (n = 22) | p-Value | MO + CC Lozenge (n = 23) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 4 | Baseline | Week 4 | Baseline | Week 4 | |||||
| BP (mmHg) | Systolic | 132.25 ± 15.3 | 124.37 ± 11.46 | ns | 134 ± 14.92 | 139.63 ± 12.73 | ns | 133.81 ± 12.04 | 131.73 ± 17.41 | ns |
| Diastolic | 90.75 ± 14.91 | 82.12 ± 9.73 | ns | 87.63 ± 11.55 | 92.63 ± 10.08 | ns | 88.06 ± 12.28 | 79.6 ± 23.1 | ns | |
| HR | 84.87 ± 18.19 | 88 ± 12.99 | ns | 90.72 ± 18.34 | 95.36 ± 17.23 | ns | 95.81 ± 18.41 | 92.06 ± 21.11 | ns | |
| FBS (mg/dL) | 89 ± 11.95 | 92.62 ± 25.11 | ns | 96.54 ± 21.69 | 103.54 ± 19.30 | ns | 97.93 ± 9.65 | 99.38 ± 15.24 | ns | |
| AST (U/L) | 58 ± 85.78 | 29.62 ± 11.78 | ns | 66.18 ± 83.59 | 55.45 ± 70.01 | ns | 36.81 ± 30.03 | 29.87 ± 10.36 | ns | |
| ALT (U/L) | 30.12 ± 25.44 | 24.87 ± 14.97 | ns | 48.27 ± 50.88 | 38.09 ± 32.34 | ns | 36.75 ± 41 | 25.68 ± 30.26 | ns | |
| ALP (U/L) | 123.75 ± 73.24 | 104.75 ± 67.03 | ns | 99 ± 59.15 | 106.48.10 | ns | 86.81 ± 42.95 | 95.18 ± 62.25 | ns | |
| BUN (mg/dL) | 11.97 ± 3.46 | 11.98 ± 2.98 | ns | 12.79 ± 2.69 | 11.94 ± 3.23 | ns | 12.35 ± 3.39 | 13.81 ± 3.28 | ns | |
| sCr (mg/dL) | 0.86 ± 0.15 | 0.91 ± 0.14 | ns | 0.98 ± 0.19 | 1 ± 0.2 | ns | 0.98 ± 0.12 | 0.99 ± 0.12 | ns | |
| Parameters | Placebo | MO Lozenge | MO + CC Lozenge | p-Value |
|---|---|---|---|---|
| (n = 22) | (n = 22) | (n = 24) | ||
| Oral Inflammation | ||||
| Baseline | 0.14 ± 0.35 | 0.27± 0.55 | 0.21 ± 0.25 | ns |
| Week 4 | 0.05 ± 0.21 | 0.05 ± 0.22 | 0.09 ± 0.42 | ns |
| p-Value | ns | ns | ns | |
| % Decrease | 64.28 | 81.48 | 57.14 | <0.001 |
| Gingival Index | ||||
| Baseline | 1.77 ± 0.69 | 2.18 ± 1.59 | 1.88 ± 0.61 | ns |
| Week 4 | 1.55 ± 0.51 | 1.62 ± 0.59 | 1.48 ± 0.51 | ns |
| p-Value | ns | ns | <0.05 | |
| % Decrease | 12.43 | 25.69 | 21.28 | <0.001 |
| Parameters | Placebo | MO Lozenge | MO + CC Lozenge | p-Value |
|---|---|---|---|---|
| (n = 22) | (n = 22) | (n = 24) | ||
| Lozenge Usage (%) | 83.64 ± 22.08 | 84.33 ± 20.26 | 78.19 ± 25.99 | ns |
| Lozenge Appearance | 3.91 ± 0.84 | 3.76 ± 0.83 | 3.83 ± 0.83 | ns |
| Flavor | 3.86 ± 0.89 | 3.57 ± 0.87 | 3.43 ± 1.24 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luetragoon, T.; Sranujit, R.P.; Noysang, C.; Thongsri, Y.; Potup, P.; Somboonjun, J.; Maichandi, N.; Suphrom, N.; Sangouam, S.; Usuwanthim, K. Evaluation of Anti-Inflammatory Effect of Moringa oleifera Lam. and Cyanthillium cinereum (Less) H. Rob. Lozenges in Volunteer Smokers. Plants 2021, 10, 1336. https://doi.org/10.3390/plants10071336
Luetragoon T, Sranujit RP, Noysang C, Thongsri Y, Potup P, Somboonjun J, Maichandi N, Suphrom N, Sangouam S, Usuwanthim K. Evaluation of Anti-Inflammatory Effect of Moringa oleifera Lam. and Cyanthillium cinereum (Less) H. Rob. Lozenges in Volunteer Smokers. Plants. 2021; 10(7):1336. https://doi.org/10.3390/plants10071336
Chicago/Turabian StyleLuetragoon, Thitiya, Rungnapa Pankla Sranujit, Chanai Noysang, Yordhathai Thongsri, Pachuen Potup, Jukarin Somboonjun, Nucharee Maichandi, Nungruthai Suphrom, Supaporn Sangouam, and Kanchana Usuwanthim. 2021. "Evaluation of Anti-Inflammatory Effect of Moringa oleifera Lam. and Cyanthillium cinereum (Less) H. Rob. Lozenges in Volunteer Smokers" Plants 10, no. 7: 1336. https://doi.org/10.3390/plants10071336
APA StyleLuetragoon, T., Sranujit, R. P., Noysang, C., Thongsri, Y., Potup, P., Somboonjun, J., Maichandi, N., Suphrom, N., Sangouam, S., & Usuwanthim, K. (2021). Evaluation of Anti-Inflammatory Effect of Moringa oleifera Lam. and Cyanthillium cinereum (Less) H. Rob. Lozenges in Volunteer Smokers. Plants, 10(7), 1336. https://doi.org/10.3390/plants10071336