Abstract
We propose a pilot, prospective, translational study with the aim of identifying possible molecular markers underlying metastatic prostate cancer (PC) evolution with the use of liquid biopsy. Twenty-eight castrate sensitive, oligometastatic PC patients undergoing bone and/or nodal stereotactic body radiotherapy (SBRT) were recruited. Peripheral blood samples were collected before the commencement of SBRT, then they were processed for circulating cell free DNA (cfDNA) extraction. Deep targeted sequencing was performed using a custom gene panel. The primary endpoint was to identify differences in the molecular contribution between the oligometastatic and polymetastatic evolution of PC to same-first oligo-recurrent disease presentation. Seventy-seven mutations were detected in 25/28 cfDNA samples: ATM in 14 (50%) cases, BRCA2 11 (39%), BRCA1 6 (21%), AR 13 (46%), ETV4, and ETV6 2 (7%). SBRT failure was associated with an increased risk of harboring the BRCA1 mutation (OR 10.5) (p = 0.043). The median cfDNA concentration was 24.02 ng/mL for ATM mutation carriers vs. 40.04 ng/mL for non-carriers (p = 0.039). Real-time molecular characterization of oligometastatic PC may allow for the identification of a true oligometastatic phenotype, with a stable disease over a long time being more likely to benefit from local, curative treatments or the achievement of long-term disease control. A prospective validation of our promising findings is desirable for a better understanding of the real impact of liquid biopsy in detecting tumor aggressiveness and clonal evolution.
1. Introduction
Oligometastatic prostate cancer (OPC) is a heterogeneous disease encompassing a broad spectrum of clinical states and related outcomes, such as de novo oligometastatic, oligorecurrent, and oligoprogressive disease [,,,]. The oligometastases theory was proposed for the first time in 1995 by Hellman and Weichselbaum, suggesting that metastatic dissemination occurs along an only apparent continuum from localized cancer to extensively metastatic disease [,]. Oligometastatic disease has been described to show a relatively limited metastatic potential []. In the natural history of prostate cancer, OPC may represent the initial step of an unavoidable, rapid progression to a polymetastatic state, or it may be the expression of a true oligometastatic phenotype; hence, a stable disease for a long time, and amenable to curative treatment or the achievement of long-term disease control [,,]. To date, OPC is mainly defined according to a maximum number of distant metastatic lesions (usually 1 to 3) []. In the oligometastatic setting, the adoption of stereotactic body radiation therapy (SBRT) has proven to be a potentially curative treatment option. A large amount of retrospective, national, and international studies have already described SBRT as being safe and effective in terms of local control of disease and freedom from failure [,,,,,,,,,,,,,,,,,,,,,], owing to the postponement of the need for androgen deprivation therapy (ADT) prescription, which still represents the standard of care for metastatic prostate cancer. Such findings were recently confirmed by prospective series, and they definitely supported the role of metastases-directed therapy in OPC patients relapsing after a local treatment with a limited number of metastases [,,,].
Despite significant advances in understanding the clinical meaning of OPC, no biomarkers that differentiate between the oligometastatic and the polymetastatic state have been currently validated, and biological investigations for OPC patient stratification are still lacking in literature. Over the past years, molecular profiling has improved our knowledge regarding the genomic landscape of advanced prostate cancer [,]. For this purpose, the so-called “liquid biopsy” approach may provide a powerful tool for identifying predictive biomarkers and therapeutic targets in a non-invasive manner []. Moreover, molecular biology techniques such as next-generation sequencing (NGS) have emerged as a promising issue for characterizing the oligometastatic-state heterogeneity [,]. We present our pilot study, the translational analysis of serum-derived circulating cell free DNA (cfDNA) in a population of OPC patients, using a deep target sequencing approach, with the aim of tracking metastatic prostate cancer spread from a molecular point of view, the possible identification of biomarkers that are predictive for a true oligometastatic state, and we assess whether any molecular characterization of OPC may also contribute to select patients that are more likely to benefit from local, metastasis-directed SBRT [].
2. Materials and Methods
2.1. Patients Selection and Treatment
The present study received final approval by the Institutional Ethical Committee, and it was performed in accordance with the principles of good clinical practice (GCP) with respect to the ICH GCP guidelines and the ethical principles contained in the Helsinki declaration [].
The study population included adult patients with castrate-sensitive OPC, consecutively evaluated at our institution for SBRT on bone lesions (30 Gy/3 fractions, biological effective dose (BED) 108 Gy, considering α/ß 3 Gy) or nodal metastases (36 Gy/6 fractions, BED 100 Gy considering α/ß 1.5 Gy for cancer and 3 Gy for late-responder normal tissue). Inclusion criteria are reported in Table 1.

Table 1.
Patient selection criteria.
All of the metastatic lesions (bone and lymph nodes) had been detected by restaging 11C-Choline PET/CT scan, and/or 68Ga-Prostate-Specific Membrane Antigen (PSMA) PET/CT scan, at the time of biochemical failure after primary treatment with curative intent according to the European Association of Urology (EAU) guidelines [].
Radiotherapy planning and treatment delivery are fully described in Appendix A—Radiotherapy Procedures.
Following SBRT, all the enrolled patients underwent clinical follow up as per usual, according to disease-specific, internationally accepted clinical practice [] (details in Appendix A—Radiotherapy Procedures). For the purpose of the present protocol, data collection continued for a planned observation period of 36 months after the treatment of OPC.
2.2. Biological Experimental Plan
2.2.1. cfDNA Extraction and Sequencing
Per each enrolled patient, peripheral blood samples were collected in 2 × 4.9 mL clot activator tubes (S-Monovette Sarstedt) before the start of SBRT, and kept at room temperature for 30–60 min to allow for clotting, and then centrifuged at 2000× g for 15 at 4 °C. Circulating cell free DNA (cfDNA) was purified from serum using QIAamp Circulating Nucleic Acid kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. cfDNA was quantified using QuantiT™ Oligreen® ssDNA kit (Thermofisher, Waltham, MA, USA) and Infinite200 plate reader (Tecan, Männedorf, Switzerland).
2.2.2. Library Preparation and NGS Analysis
After extraction, cfDNA from serum immediately underwent end-repair, A-tailing, and ligation to Illumina indexed adapters.
A custom-targeted gene panel was designed following the evidences reported in the literature regarding the molecular characterization of prostate cancer [,], using the NimbleDesign tool (Roche, Basel, Switzerland), and included the coding sequence (exons) of the genes showed in Table 2.
Table 2.
Genetic panel for bioinformatics analysis.
Once the DNA libraries were indexed, they were PCR-amplified, quantified, and pooled before hybridization to a custom NimbleGen SeqCap EZ Choice Library (Roche) of oligonucleotide DNA probes that were complementary to the coding sequences of the 37 selected genes (Table 2). Regulatory sequences and splicing sites were also included. The pooling strategy was 8 samples per pool. The hybridization was performed over-night for 18 h. After stringent washing, the captured libraries were PCR-amplified and sequenced to generate 2 × 150 bp paired-end reads with a MiSeq platform (Illumina, San Diego, CA, USA). Finally, the resulting DNA sequences were automatically demultiplexed and aligned to the human reference genome Hg19. Sequence variants were detected and annotated by Webannovar.
The thresholds for the candidate variants were 1000× for locus coverage, and 50 total reads (25 reads on both sequenced DNA strands) reporting the variant [].
Common polymorphisms (≥1% in the general population) were discarded by comparison with NCBI, dbSNP, 1000 genomes, and EXAC, and then automatically investigated by Webannovar. However, since these databases contain known disease-associated mutations, all detected variants were compared with the gene-specific mutation databases, ClinVar and COSMIC. Then, we screened for mutations that could give rise to premature protein-truncating mutations or those with a high impact on the protein structure, such as, stop mutations, missense variants, mutations on splice sites, and exonic indels.
Unknown variants were automatically ranked by Webannovar pipeline. This ranking was based upon the evolutionary conservation and potential level of danger of the affected nucleotide locus, using Sift, Polyphen2, Mutation tester, FATHMM, ProVean, MetaSVM, and M-CAP [].
Mutation rates (per megabase) was determined dividing the mutation count for each sample by the extension gene panel (0.1092 Mb).
2.3. Statistical Analysis
The database was formatted using Microsoft Excel® software and later imported from IBM-SPSS® software ver. 26.0.1 (IBM SPSS Inc. Chicago, IL, USA). The use of the Stata® software ver. 16.0 (Stata Corporation, College Station, TX, USA) was also considered for comparisons or implementations of the test output.
Normality of the Distributions as Assessed Using the Kolmogorov–Smirnov Test
Categorical variables were presented as frequencies or percentages, and compared with the use of the Chi-Square test and the Fisher’s exact test, as appropriate; associations of the crosstabs were verified using standardized adjusted residuals.
Continuous variables were presented as means ± standard deviation (SD) (in the case of a normal distribution), or medians, and min/max (in the case of a skewed distribution) and compared with the use of Student’s T-test, ANOVA, or the Mann–Whitney and Kruskal–Wallis test; correlations among variables were analyzed by the Pearson’s or Spearman’s rank correlation test. A stepwise logistic regression analysis including all variables with probability values < 0.05 in the univariate analysis was used to determine independent predictors; ATM no/yes was the dependent variable, and overall ADT treatment time, FOXA1 yes/no, site of recurrence after primary treatment (nodal, bone or both), local control disease yes/no, BRCA1 yes/no, POLD1 yes/no, were the independent variables. The results are presented as an odds ratio (OR) with 95% confidence intervals. A two-sided α level of 0.05 was used for all tests. The authors had full access to and take full responsibility for the integrity of the data.
3. Results
3.1. Population Clinical Characteristics and Outcomes
A total of 28 patients with castrate sensitive, oligorecurrent prostate cancer were considered suitable for this study between November 2017 and July 2018 at the Spedali Civili Hospital of Brescia. The median age was 67 years (52–75). Population characteristics and treatment outcomes are summarized in Table 3.
Table 3.
Population characteristics.
All of the treated lesions were detected by 11C-Choline PET-TC, then used to support radiation treatment planning. Nodal metastases were recorded in 20 (71.5%) patients, while 6 (21.4%) of them had bone lesions; both nodal and bone involvement were reported in 2 (7.1%) cases.
At the end of the observation period, a median follow-up of 34.9 months (range 17.4–43.7) was reported. We recorded an 83% local control of disease after the first SBRT; grade 1 acute bladder toxicity in 1 case; grade 2 late bowel toxicity; no grade ≥ 3 acute or late toxicity. The median ADT-free survival was 19.5 months (range 5.5–43.9).
3.2. Genomic Landscape of Oligometastatic Prostate Cancer
Blood samples were collected from all patients before radiation treatment and approximately 2.5 mL of serum were processed for cfDNA. The median [cfDNA] was 30.2 ng/mL (range 4.2–171.6 ng/mL) (Figure 1).
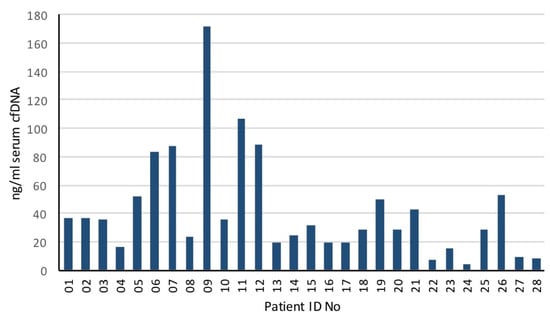
Figure 1.
Serum cfDNA concentration (ng/mL) in oligometastatic prostate cancer patients.
Deep targeted DNA sequencing of 37 prostate cancer relevant genes was performed, and a total of 77 mutations were detected in 25 of 28 cfDNA samples (Figure 2). A detailed list of the detected mutations is reported in Appendix B, Table A2.
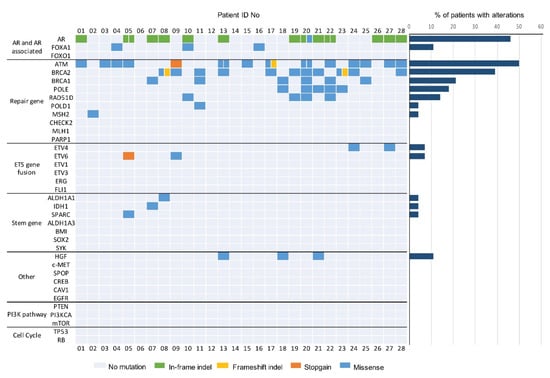
Figure 2.
Genomic landscape of oligometastatic prostate cancer from targeted serum cfDNA sequencing. Oncoprint shows genomic alterations identified in cfDNA of patients with oligometastatic prostate cancer. Genes are grouped by pathway (37 genes shown). Mutational frequency for each gene in the targeted panel is provided on the right.
The median tumor mutational load was 27.5/Mb (range, 0–73.3 mutations/Mb) (Figure 3).
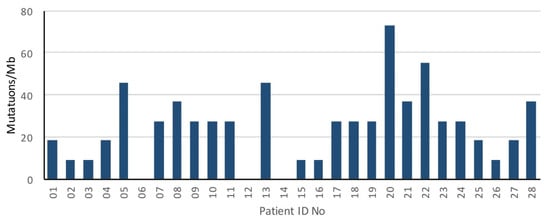
Figure 3.
Mutation rate of oligometastatic prostate cancer patients.
Genomic alterations mainly occurred in the AR and DNA repair gene pathways. Nine different deletions, two insertions, and one missense mutation regarding AR genes were identified in 13 (46.4%) patients. Among these, four (30.8%) patients carried the 171_176 deletions and two (15.4%) others, the 171_182 deletion. Furthermore, alterations in the FOXA1 gene were detected (3 (10.7%) cases). ATM mutations were identified in 14 (50.0%) patients in the cohort, and most of them were missense mutations. Intriguingly, six (42.9%) patients harbored the 5557 G > A mutation, two (14.3%) of them carried the 3161 G > C mutation, one (7.1%) patient had a stopgain mutation, and one (7.1%) a frameshift deletion. We observed frameshift deletions and missense mutations in BRCA2 in 11 (39.3%) patients, eight of whom (72.7%) harbored the 1114 C > A aberration. Patient 08 carried a frameshift deletion in the BRCA2 gene, causing a truncated protein product. Six (21.4%) patients showed missense mutations in th BRCA1 sequence, and three (50.0%) of them harbored the 1936 A > G aberration. POLE mutations were identified in five (17.9%) patients, four (80.0%) of them showing the 755 C > T mutation. Four (14.3%) patients carried a 158 G > A alteration in the RAD51D gene, and one (3.6%) patient harbored a missense mutation in MSH2. A loss of heterozygosis was also observed: two patients harboring the 1114 C > A BRCA2 alteration, one patient carrying the 1936A > G BRCA1 mutation, and one patient with the 158A > G RAD51D variant. Missense mutations in HGF were also observed (three (10.7%) cases). Four (14.3%) patients carried ETS gene fusion variants: two (7.1%) patients with missense mutations in ETV4, and two (7.1%) patients with a missense mutation and a stopgain mutation, respectively. Finally, missense mutations in the IDH1 (one (3.6%) patient), ALDH1A1 (one (3.6%)), and SPARC (one (3.6%)) stemness genes were identified. We did not observe mutations in the PI3KCA pathway, nor in tumor suppressor genes.
When analyzing the interaction between the identified genomic alterations and pre-treatment [cfDNA], we found a lower median [cfDNA] in ETV4 carriers than in ETV4 non-carriers (6.6 ng/mL and 33.35 ng/mL, respectively) (p = 0.021), together with a lower median [cfDNA] in ATM carriers than ATM non-carriers (24.02 ng/mL and 40.035 ng/mL, respectively) (p = 0.039).
The interaction between the identified genomic alterations and clinical parameters was also investigated. There was a trend for an increased risk for ADT prescription requirement in ATM mutation carriers (OR = 0.160, p = 0.057), while SBRT failure was associated with an increased risk of harboring BRCA1 mutations (OR = 10.5, p = 0.043).
4. Discussion
Metastatic prostate cancer has been demonstrated to be molecularly heterogeneous, with clinical heterogeneous behavior [,]. To date, many treatment options are available for the management of metastatic prostate cancer; nevertheless, there are some unmet needs for patient stratification in this setting []. In this scenario, biomarker discovery using liquid biopsy has become an interesting field of study [,]. There is a growing interest for deep targeted cfDNA sequencing as a promising way of identifying evolution markers underlying progressive cancer or the metastases process before clinical onset []. DNA sequencing approaches based on next-generation (NGS) technology have enabled the rapid, high-quality analysis of genes that may be relevant for disease-specific characterization. NGS can generate wide and complete masses of DNA sequence data, and perform quick and cost-effective genetic analysis []. Currently, there is only one Food and Drug Administration (FDA)-approved liquid biopsy assay for the detection of BRCA1, BRCA2, and/or ATM aberrations in patients with metastatic castrate-resistant prostate cancer (mCRPC) who may be appropriate for the treatment with poly(ADP-ribose) polymerase (PARP) inhibitors (PARPi) [,]. Compared to tissue biopsy, liquid biopsy is non-invasive and captures aggregate features from tumor material-releasing metastases, thus providing real-time information on the state of the disease. It may be a useful tool for treatment resistance tracking [,,].
OPC represents a phenotype with limited metastatic potential, and reveals heterogeneity in clinical behavior [,]. Metastases-directed, ablative SBRT has been gaining validation as a safe and effective treatment option for oligorecurrent/oligoprogressive PC []. Beyond the large number of promising findings from retrospective data, the prospective, phase II Observation versus stereotactic ablative RadiatIon for OLigometastatic Prostate CancEr Trial (ORIOLE) recently confirmed SBRT to improve oncologic outcomes in a certain setting of oligometastatic PC patients, with an excellent local control of disease and mild adverse events, with no impact on the patient quality of life []. Preliminary results from the randomized, phase II Surveillance or metastasis-directed Therapy for OligoMetastatic Prostate cancer recurrence (STOMP) trial also supported the utility of metastasis-directed therapy (surgery or SBRT) in the oligometastatic state of PC [,].
Despite the excellent local control and improved survival obtained with such a metastasis-directed treatment approach (i.e., surgery or ablative SBRT), sometimes OPC only represents the initial step of a rapid, unavoidable progression to a polymetastatic disease []. The identification of features that discriminate a true oligometastatic state and a polymetastatic progression phenotype is challenging. Since the nucleic acids released into the blood stream are considered to be cell messengers, information regarding a true oligometastatic condition and/or tumor cell reactions to radiation may be derived []. However, unlike colorectal or lung cancer, there are no recurrent point mutations in PC that can be used to track the disease. Moreover, relevant to intra-patient heterogeneous diseases, different sites of metastases may likely have different DNA release rates, and the ability to detect cfDNA-based features is gene region- and individual dependent [,,,].
We planned a prospective, pilot study since there are no similar biological study designs to compare with for accrual evaluation that have ever been reported in the literature.
The primary endpoints were differences in molecular contribution between the oligometastatic and polymetastatic evolution of prostate cancer to same-first oligorecurrent disease presentation, and their association with ADT-free survival (ADT-FS), defined as the time between the first day of SBRT and the start of palliative ADT. The secondary endpoints were: distant progression-free survival (DPFS, defined as the time between the first day of SBRT and the detection of clinical disease outside the PTV after further biochemical progression); local control (in-field control) of disease (defined as no evidence of disease in the treatment field at the restaging Choline- or PSMA-PET/CT).
Our exploratory analysis revealed that cfDNA concentrations in patients with OPC were relatively low, considering those reported in literature for patients with mCRPC, which is a more advanced and prognostically unfavorable stage of the disease []. Despite the absence of a direct comparison between the two groups in our study, nor in the available literature, taking into account the current biological evidence regarding cancer metastatization [,], we may hypothesize that such lower cfDNA concentration is likely to reflect the limited metastatic potential of the oligometastatic state [].
The distribution of the genomic alterations in our study were highly consistent with the genomic landscape of prostate cancer described in literature [,]. As expected, mutations in the AR and DNA repair genes included in our panel were the most common ones, in particular, the ATM and BRCA1/BRCA2 genes, and they seemed to drive high tumor mutation load and rapid polymetastatic spread after the first oligorecurrence treated with SBRT. In detail, most of the AR aberrations consisted of non-frameshift deletions, and they were located in a possible critical and hotspot region of the N-terminal domain of the receptor. We did not observe mutations in the ligand-binding domain, as is commonly mapped []. BRCA1/2 and ATM aberrations have been reported to be associated with a more aggressive prostate cancer phenotype, with an increased risk of disease recurrence and poorer survival outcomes [,,]. In our cohort, the ATM 3161 G > C variant was associated with an increased prostate cancer risk []. Our findings also showed that the BRCA2 mutation rate was higher than BRCA1, in line with the available literature. BRCA2 mutations are known to be associated with a higher prostate cancer mortality, likely due to the direct involvement of BRCA2 in the homologous recombination process, as it mediates the recruitment of RAD51 to DNA double-strand breaks []. Of note, although not clearly statistically significant, patients in our series with a history of ADT prescription before metastatic onset (concurrent to primary or salvage treatment) were more likely to have an ATM mutation. However, there are not enough elements to establish whether these are germinal mutations probably harboring a poorer prognosis, or somatic alterations induced by ADT itself. Not less important, OPC patients with combined mismatch repair gene and BRCA2 mutations seemed to have a worse prognosis. Nearly half of BRCA1-mutated OPC patients also showed no local control of the disease after the first SBRT course. All this being considered, our preliminary data suggested that the presence of high-risk prostate cancer mutations (regarding ATM, BRCA1, and BRCA2 genes) might be the starting point for identifying a subset of patients who may benefit from systemic treatment and local radiotherapy in combination strategies since the first clinical and radiological evidence of metastatic, castrate-sensitive PC.
In the near future, the PC oligometastatic state should be better characterized based on its molecular features, not only considering the number of metastatic lesions [,,].
To our knowledge, our series may be considered the first prospective one with translational implications in the field of oligometastatic PC.
Unfortunately, the relatively small sample size of our study is the main limitation of our study, and it did not allow much powerful conclusions to be drawn. However, our prospective pilot study provided some promising clinical insights regarding the possible identification of metastatic prostate cancer evolution markers. Whether our results were confirmed for a wider cohort of patients, it would be possible to set up gene clustering for a highly accurate prognostic stratification of patients with metastatic PC.
Tracking molecular evolution markers predictive for a better response to stereotactic irradiation, or for a worse prognosis, which supports the need for systemic therapy, may offer some clues for defining the best radiation treatment features and technological solutions in the rapidly expanding field of stereotactic cancer treatments. Of note, the identification of a true oligometastatic state that is amenable to local, ablative treatment may also allow for the postponement of the need for ADT in a significant number of patients, ensure better patient QoL, a reduction in possible side effects (i.e., metabolic syndrome, climacteric syndrome, etc.) and reduced healthcare costs.
5. Conclusions
We proposed a preliminary, exploratory analysis of serum-derived cfDNA samples collected before SBRT treatment through a deep target sequencing approach. We investigated whether the sequencing of 37 prostate cancer-relevant genes might contribute to the recognition of the heterogeneity of oligometastatic prostate disease, and a better molecular characterization of oligometastatic disease. Moreover, we attempted to examine the obtained molecular data, to predict an eventual polymetastatic progression.
Our study may represent a crucial foundation for the future design of clinical trials owing to provide the stratification of patients with OPC based on a molecular signature. Moreover, the assessment of a molecular fingerprint for OPC may allow for the identification of patients with a true oligometastatic phenotype, and hence, with stable disease for a long time, which are more likely to benefit from local, curative treatments, or the achievement of long-term disease control. The prospective validation of our promising findings on a wider series is desirable for a better understanding of the real impact of liquid biopsy analysis in detecting tumor features. Whether our findings were confirmed on a large scale, liquid biopsy might become a useful source of prognostic and predictive markers of metastatic prostate cancer spread. The real-time molecular characterization of cancer disease by liquid biopsy is also expected to be crucial for setting a patient-tailored therapeutic approach based on tumor aggressiveness and clonal evolution, to be applied a long time before clinical onset and the subsequent clinical appearance of advanced and extended progression of disease.
Author Contributions
Conceptualization, L.T. and S.B.; methodology, S.B. and C.F.; validation, L.T., A.C. and C.F.; formal analysis, S.B. and C.T.; investigation, L.B., A.C. and A.E.G.; resources, L.T. and R.B.; data curation, A.C. and L.B.; writing—original draft preparation, A.C. and L.B.; writing—review and editing, L.B., L.T. and C.F.; visualization, S.B.; supervision, N.P. and R.B.; project administration, D.R. and S.M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of PROVINCIA DI BRESCIA—ASST SPEDALI CIVILI DI BRESCIA (protocol code NP 2813, date of approval 17 November 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to Institutional policies, and the need for the authorization of the Study Coordinator (L.T. and S.M.M.).
Acknowledgments
The authors acknowledge Milena Tartarelli for data management, administrative support, and management of relations with the Ethics Committee.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Appendix A.1. Radiotherapy Procedures
Appendix A.1.1. Target Volume Delineation
A CT-based treatment planning with slice thicknesses of 2–3 mm was performed. Then, target volume delineation by co-registration of the planning CT images with the available morphological and functional images was applied.
The gross tumor volume (GTV) was defined by imaging co-registration between the simulation CT scan and the restaging CT-PET. Then, an isotropic additional margin of 6 mm was applied to the GTV to obtain the Planning Tumor Volume (PTV). In the case of upper abdominal lesions, 4D-CT was used to define the internal target volume (ITV), and the PTV was defined as a 6 mm isotropic expansion from the ITV. The target volume delineation and dose delivery calculation were performed using Pinnacle Treatment Planning System (Pinnacle TPS, Philips Radiation Oncology Systems, Fitchburg, WI, USA).
Appendix A.1.2. Dose Prescription
All patients underwent stereotactic body radiation therapy (SBRT) with image-guided, helical, or volumetric intensity-modulated radiation therapy (IMRT-IGRT). A course of 36 Gy–6 Gy/fraction (fx) was prescribed on nodal lesions, and 30 Gy–10 Gy/fx on bone lesions (36 Gy–6 Gy/fx when the previous schedule was not applicable), with a corresponding tumor biological effective dose (BED) of 144 Gy and an equivalent dose of 2 Gy (EQD2) 72 Gy in the former, with BED 180 Gy–EQD2 90 Gy in the latter (considering α/ß 1.5 Gy).
Appendix A.1.3. Radiotherapy Planning
Radiotherapy planning was performed, combining an accurate dosimetric and radiobiological evaluation, based on the available literature [,,,,,,,,,,]. Large inhomogeneity in dose distribution was allowed to obtain higher maximal doses within the GTV/ITV, but 95% of PTV was required to be covered by the prescribed dose. The maximum acceptable dose (Dmax) in the PTV was 115% of the prescribed dose (Figure A1).

Figure A1.
Dose distribution for nodal (A) and bone (B) SBRT.
Normal tissue dose constraints were as per the Task Group 101 and UK Consensus [,]. These also were the basis for the normal tissue tolerance calculation in 36 Gy in the 6 fx schedule. If normal tissue constraints were beyond tolerance, a 90% PTV coverage was accepted for 30 Gy in the 3 fx schedule, as long as the full coverage of GTV/ITV (≥100% of the prescribed dose) was guaranteed. The reference organs at risk (OAR) dose constraints are reported in Table A1.
Table A1.
OAR dose constraints for nodal/bone SBRT.
Table A1.
OAR dose constraints for nodal/bone SBRT.
| Abdominal targets | Value |
| Spine | Dmax < 18 Gy |
| Kidneys | V15Gy < 35% |
| Stomach | V36Gy < 3%, |
| Duodenum | V36Gy < 1% |
| Bowel bag | V36Gy < 3% |
| Liver | V15Gy < critical volume (700 cc) |
| Pelvic targets | |
| Bowel bag | D1cc < 21 Gy |
| Rectum | Dmax < 100% of prescription dose |
| Bladder/Urethra | Dmax < 120% of prescription dose |
| Bone targets | |
| Spine | Dmax < 21.9 Gy |
| D0.035cc < 18 Gy | |
| D1-2cc 12.3 Gy | |
| Spinal nerve roots | D3cc < 20.4 Gy |
| D0.035cc < 24 Gy | |
| Descending aorta | Dmax < 30 Gy |
| Ileum | Dmax < 25.2 Gy |
| Spine | D5cc < 17.7 Gy |
Appendix A.1.4. Follow Up
Following SBRT, patients commenced clinical follow up (FU): clinical examination and PSA detection every 3 months for the first year, then every 6 months until progression of disease (PD); interview for PC-related symptoms, gastrointestinal (GI) and genitourinary (GU) toxicity (according to CT-CAE classification—v4.02 []) every 3 months for the first year, then every 6 months until PD. In the case of biochemical progression, restaging with 11C-Choline/68Ga-PSMA PET was required. For the purpose of the present protocol, data collection continued for a planned observation period of 36 months after the treatment of OPC.
Appendix B
Table A2.
List of the 77 detected mutations from the DNA sequencing of 37 prostate cancer-relevant genes (nucleotide aberrations).
Table A2.
List of the 77 detected mutations from the DNA sequencing of 37 prostate cancer-relevant genes (nucleotide aberrations).
| Sample | Chromosome | Start | End | Reference Nucleotide | Altered Nucleotide | Gene | Effect | Evolution Disease |
|---|---|---|---|---|---|---|---|---|
| 1 | chr11 | 108272729 | 108272729 | C | G | ATM | missense | Polymetastatic disease |
| chrX | 67545317 | 67545319 | GCA | - | AR | nonframeshift deletion | ||
| 2 | chr2 | 47512394 | 47512394 | G | A | MSH2 | missense | Oligometastatic disease |
| 3 | chr11 | 108249096 | 108249096 | T | C | ATM | missense | Polymetastatic disease |
| 4 | chr11 | 108310287 | 108310287 | A | G | ATM | missense | Oligometastatic disease |
| chr14 | 37594904 | 37594904 | C | G | FOXA1 | missense | ||
| 5 | chr5 | 151663550 | 151663550 | C | T | SPARC | missense | Oligometastatic disease |
| chr11 | 108249096 | 108249096 | T | C | ATM | missense | ||
| chr12 | 11891545 | 11891545 | C | T | ETV6 | UTR3 | ||
| chrX | 67546515 | 67546529 | GGCGGCGGCGGCGGC | - | AR | nonframeshift deletion | ||
| chrX | 67546518 | 67546529 | GGCGGCGGCGGC | - | AR | nonframeshift deletion | ||
| 6 | - | - | - | - | - | - | - | Oligometastatic disease |
| 7 | chr2 | 208243577 | 208243577 | A | G | IDH1 | missense | Oligometastatic disease |
| chr17 | 43074471 | 43074471 | G | T | BRCA1 | missense | ||
| chrX | 67545316 | 67545316 | - | GCA | AR | nonframeshift insertion | ||
| 8 | chr9 | 72952984 | 72952984 | C | T | ALDH1A1 | missense | Oligometastatic disease |
| chr13 | 32329468 | 32329469 | TG | - | BRCA2 | frameshift deletion | ||
| chr13 | 32340099 | 32340099 | C | T | BRCA2 | missense | ||
| chrX | 67545317 | 67545322 | GCAGCA | - | AR | nonframeshift deletion | ||
| 9 | chr11 | 108244873 | 108244873 | C | T | ATM | stopgain | Oligometastatic disease |
| chr12 | 11890993 | 11890993 | C | G | ETV6 | missense | ||
| chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | ||
| 10 | chr14 | 37591441 | 37591441 | G | A | FOXA1 | missense | Polymetastatic disease |
| chr17 | 35106468 | 35106468 | G | A | RAD51D | missense | ||
| chrX | 67545317 | 67545322 | GCAGCA | - | AR | nonframeshift deletion | ||
| 11 | chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | Polymetastatic disease |
| chr17 | 43092412 | 43092412 | G | A | BRCA1 | missense | ||
| chr19 | 50413766 | 50413766 | G | A | POLD1 | missense | ||
| 12 | - | - | - | - | - | - | Oligometastatic disease | |
| 13 | chr7 | 81745064 | 81745064 | T | G | HGF | missense | Polymetastatic disease |
| chr11 | 108272849 | 108272849 | A | G | ATM | missense | ||
| chr11 | 108304735 | 108304735 | G | A | ATM | missense | ||
| chr13 | 32338416 | 32338416 | C | T | BRCA2 | missense | ||
| chrX | 67545317 | 67545328 | GCAGCAGCAGCA | - | AR | nonframeshift deletion | ||
| 14 | - | - | - | - | - | - | Polymetastatic disease | |
| 15 | chr11 | 108304735 | 108304735 | G | A | ATM | missense | Polymetastatic disease |
| 16 | chr14 | 37592342 | 37592342 | C | G | FOXA1 | missense | Oligometastatic disease |
| 17 | chr11 | 108289623 | 108289623 | C | T | ATM | missense | Oligometastatic disease |
| chr11 | 108279497 | 108279497 | C | - | ATM | frameshift deletion | ||
| chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | ||
| 18 | chr12 | 132677409 | 132677409 | C | T | POLE | missense | Polymetastatic disease |
| chr7 | 81729735 | 81729735 | G | A | HGF | missense | ||
| chr17 | 43093454 | 43093454 | G | A | BRCA1 | missense | ||
| 19 | chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | Oligometastatic disease |
| chr17 | 35106468 | 35106468 | G | A | RAD51D | missense | ||
| chrX | 67545317 | 67545322 | GCAGCA | - | AR | nonframeshift deletion | ||
| 20 | chr11 | 108272729 | 108272729 | C | G | ATM | missense | Oligometastatic disease |
| chr11 | 108267276 | 108267276 | T | C | ATM | missense | ||
| chr12 | 132677409 | 132677409 | C | T | POLE | missense | ||
| chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | ||
| chr17 | 43093454 | 43093454 | G | A | BRCA1 | missense | ||
| chr17 | 35106468 | 35106468 | G | A | RAD51D | missense | ||
| chrX | 67546514 | 67546514 | - | GGC | AR | nonframeshift insertion | ||
| chrX | 67545319 | 67545319 | A | T | AR | missense | ||
| 21 | chr7 | 81729735 | 81729735 | G | A | HGF | missense | Oligometastatic disease |
| chr12 | 132676174 | 132676174 | T | G | POLE | missense | ||
| chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | ||
| chrX | 67545317 | 67545325 | GCAGCAGCA | - | AR | nonframeshift deletion | ||
| 22 | chr11 | 108304735 | 108304735 | G | A | ATM | missense | Oligometastatic disease |
| chr12 | 132677409 | 132677409 | C | T | POLE | missense | ||
| chr17 | 43070958 | 43070958 | G | A | BRCA1 | missense | ||
| chr17 | 35106468 | 35106468 | G | A | RAD51D | missense | ||
| chrX | 67546515 | 67546520 | GGCGGC | - | AR | nonframeshift deletion | ||
| chrX | 67545317 | 67545334 | GCAGCAGCAGCAGCAGCA | - | AR | nonframeshift deletion | ||
| 23 | chr12 | 132677409 | 132677409 | C | T | POLE | missense | Oligometastatic disease |
| chr13 | 32336400 | 32336401 | TC | - | BRCA2 | frameshift deletion | ||
| chr13 | 32338613 | 32338613 | G | T | BRCA2 | missense | ||
| 24 | chr11 | 108304735 | 108304735 | G | A | ATM | missense | Oligometastatic disease |
| chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | ||
| chr17 | 43528665 | 43528665 | C | T | ETV4 | missense | ||
| 25 | chr11 | 108304735 | 108304735 | G | A | ATM | missense | Oligometastatic disease |
| chr17 | 43093454 | 43093454 | G | A | BRCA1 | missense | ||
| 26 | chrX | 67545317 | 67545346 | GCAGCAGCAGCAGCAGCAGCAGCAGCAGCA | - | AR | nonframeshift deletion | Oligometastatic disease |
| 27 | chr11 | 108254034 | 108254034 | T | C | ATM | missense | Oligometastatic disease |
| chr17 | 43533863 | 43533863 | T | C | ETV4 | missense | ||
| chrX | 67545317 | 67545322 | GCAGCA | - | AR | nonframeshift deletion | ||
| 28 | chr11 | 108304735 | 108304735 | G | A | ATM | missense | Oligometastatic disease |
| chr13 | 32332456 | 32332456 | C | A | BRCA2 | missense | ||
| chr13 | 32332592 | 32332592 | A | C | BRCA2 | missense | ||
| chrX | 67545317 | 67545328 | GCAGCAGCAGCA | - | AR | nonframeshift deletion |
References
- Foster, C.C.; Weichselbaum, R.R.; Pitroda, S.P. Oligometastatic Prostate Cancer: Reality or Figment of Imagination? Cancer 2019, 125, 340–352. [Google Scholar] [CrossRef] [PubMed]
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Hellman, S.; Weichselbaum, R.R. Oligometastases Revised. Nat. Rev. Clin. Oncol. 2011, 8, 378–382. [Google Scholar] [CrossRef]
- Reyes, D.K.; Pienta, K.J. The biology and treatment of oligometastatic cancer. Oncotarget 2015, 6, 8491–8524. [Google Scholar] [CrossRef] [PubMed]
- Soloway, M.S.; Hardeman, S.W.; Hickey, D.; Todd, B.; Soloway, S.; Raymond, J.; Moinuddin, M. Stratification of patients with metastatic prostate cancer based on extent of disease on initial bone scan. Cancer 1988, 61, 195–202. [Google Scholar] [CrossRef]
- Singh, D.; Yi, W.S.; A Brasacchio, R.; Muhs, A.G.; Smudzin, T.; Williams, J.P.; Messing, E.; Okunieff, P. Is there a favorable subset of patients with prostate cancer who develop oligometastases? Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 3–10. [Google Scholar] [CrossRef]
- Tosoian, J.J.; Gorin, M.A.; Ross, A.E.; Pienta, K.J.; Tran, P.T.; Schaeffer, E.M. Oligometastatic prostate cancer: Definitions, clinical outcomes, and treatment considerations. Nat. Rev. Urol. 2017, 14, 15–25. [Google Scholar] [CrossRef]
- Gillessen, S.; Omlin, A.; Attard, G.; de Bono, J.S.; Efstathiou, E.; Fizazi, K.; Halabi, S.; Nelson, P.S.; Sartor, O.; Smith, M.R.; et al. Management of patients with advanced prostate cancer: Recommendations of the St Gallen Advanced Prostate Cancer Consensus Conference (APCCC). Ann. Oncol. 2015, 26, 1589–1604. [Google Scholar] [CrossRef]
- Casamassima, F.; Masi, L.; Menichelli, C.; Bonucci, I.; Casamassima, E.; Lazzeri, M.; Gulisano, M.; Aterini, S. Efficacy of eradicative radiotherapy for limited nodal metastases detected with choline PET scan in prostate cancer patients. Tumori 2011, 97, 49–55. [Google Scholar] [CrossRef]
- Jereczek-Fossa, B.A.; Beltramo, G.; Fariselli, L.; Fodor, C.; Santoro, L.; Vavassori, A.; Zerini, D.; Gherardi, F.; Ascione, C.; Bossi-Zanetti, I.; et al. Robotic image-guided stereotactic radiotherapy, for isolated recurrent primary, lymph node or metastatic prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 889–897. [Google Scholar] [CrossRef]
- Muacevic, A.; Kufeld, M.; Rist, C.; Wowra, B.; Stief, C.; Staehler, M. Safety and feasibility of image-guided robotic radiosurgery for patients with limited bone metastases of prostate cancer. Urol. Oncol. 2013, 31, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.A.; Barney, B.M.; Davis, B.J.; Park, S.S.; Kwon, E.D.; Olivier, K.R. Stereotactic body radiation therapy in the treatment of oligometastatic prostate cancer. Front. Oncol. 2013, 2, 215. [Google Scholar] [CrossRef] [PubMed]
- Berkovic, P.; De Meerleer, G.; Delrue, L.; Lambert, B.; Fonteyne, V.; Lumen, N.; Decaestecker, K.; Villeirs, G.; Vuye, P.; Ost, P. Salvage stereotactic body radiotherapy for patients with limited prostate cancer metastases: Deferring androgen deprivation therapy. Clin. Genitourin. Cancer 2013, 11, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Schick, U.; Jorcano, S.; Nouet, P.; Rouzaud, M.; Vees, H.; Zilli, T.; Ratib, O.; Weber, D.C.; Miralbell, R. Androgen deprivation and high-dose radiotherapy for oligometastatic prostate cancer patients with less than five regional and/or distant metastases. Acta Oncol. 2013, 52, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Decaestecker, K.; De Meerleer, G.; Lambert, B.; Delrue, L.; Fonteyne, V.; Claeys, T.; De Vos, F.; Huysse, W.; Hautekiet, A.; Maes, G.; et al. Repeated stereotactic body radiotherapy for oligometastatic prostate cancer recurrence. Radiat. Oncol. 2014, 9, 135. [Google Scholar] [CrossRef]
- Detti, B.; Bonomo, P.; Masi, L.; Doro, R.; Cipressi, S.; Iermano, C.; Bonucci, I.; Franceschini, D.; Di Brina, L.; Bakhi, M.; et al. Stereotactic radiotherapy for isolated nodal recurrence of prostate cancer. World J. Urol. 2015, 33, 1197–1203. [Google Scholar] [CrossRef]
- Ost, P.; Jereczek-Fossa, B.; Van As, N.; Zilli, T.; Muacevic, A.; Brown, L.; Casamassima, F.; Orecchia, R.; Henderson, D.; Olivier, K.; et al. A multi-institutional analysis of stereotactic body radiotherapy for oligometastatic prostate cancer recurrence. Eur. Urol. Suppl. 2015, 14, e447. [Google Scholar] [CrossRef]
- Henderson, D.R.; Tree, A.; Taylor, H.; Khoo, V.; Van As, N.J. Oligometastatic prostate cancer: An evaluation of stereotactic body radiotherapy (SBRT) as an alternative to palliative androgen deprivation therapy. J. Clin. Oncol. 2015, 33 (Suppl. 1), 696–702. [Google Scholar] [CrossRef]
- Muldermans, J.L.; Romak, L.B.; Kwon, E.D.; Park, S.S.; Olivier, K.R. Stereotactic Body Radiation Therapy for Oligometastatic Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 696–702. [Google Scholar] [CrossRef]
- Ost, P.; Jereczek-Fossa, B.A.; Van As, N.; Zilli, T.; Muacevic, A.; Olivier, K.; Henderson, D.; Casamassima, F.; Orecchia, R.; Surgo, A.; et al. Progression-free Survival Following Stereotactic Body Radiotherapy for Oligometastatic Prostate Cancer Treatment-naive Recurrence: A Multi-institutional Analysis. Eur. Urol. 2016, 69, 9–12. [Google Scholar] [CrossRef]
- Ost, P.; Jereczek-Fossa, B.A.; Van As, N.; Zilli, T.; Tree, A.; Henderson, D.; Orecchia, R.; Casamassima, F.; Surgo, A.; Miralbell, R.; et al. Pattern of Progression after Stereotactic Body Radiotherapy for Oligometastatic Prostate Cancer Nodal Recurrences. Clin. Oncol. 2016, 28, e115–e120. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.; Radwan, N.; Ross, A.; Reyes, D.; Wright, J.; Song, D.; Deville, C.; Deweese, T.; Carducci, M.; Schaeffer, E.; et al. Stereotactic ablative radiation therapy for the treatment of oligometastatic prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96 (Suppl. 1), E248. [Google Scholar] [CrossRef][Green Version]
- Oehler, C.; Zimmermann, M.; Curschmann, J.; Sumila, M.; Strebel, R.; Li, Q.; Schneider, U.; Zwahlen, D. Factors predicting the benefit of stereotactic body radiation therapy for oligometastatic lymph node recurrence in prostate cancer: A single institution experience. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99 (Suppl. 1), E282. [Google Scholar] [CrossRef]
- Jereczek-Fossa, B.A.; Fanetti, G.; Fodor, C.I.; Ciardo, D.; Santoro, L.; Francia, C.M.; Muto, M.; Surgo, A.; Zerini, D.; Marvaso, G.; et al. Salvage Stereotactic Body Radiotherapy for Isolated Lymph Node Recurrent Prostate Cancer: Single Institution Series of 94 Consecutive Patients and 124 Lymph Nodes. Clin. Genitourin. Cancer 2017, 15, e623–e632. [Google Scholar] [CrossRef]
- Ingrosso, G.; Trippa, F.; Maranzano, E.; Maranzano, E.; Carosi, A.; Ponti, E.; Arcidiacono, F.; Draghini, L.; Di Murro, L.; Lancia, A.; et al. Stereotactic body radiotherapy in oligometastatic prostate cancer patients with isolated lymph nodes involvement: A two-institution experience. World J. Urol. 2017, 35, 45–49. [Google Scholar] [CrossRef]
- Triggiani, L.; Alongi, F.; Buglione, M.; Detti, B.; Santoni, R.; Bruni, A.; Maranzano, E.; Lohr, F.; D’Angelillo, R.; Magli, A.; et al. Efficacy of stereotactic body radiotherapy in oligorecurrent and in oligoprogressive prostate cancer: New evidence from a multicentric study. Br. J. Cancer 2017, 116, 1520–1525. [Google Scholar] [CrossRef]
- Ponti, E.; Lancia, A.; Ost, P.; Trippa, F.; Triggiani, L.; Detti, B.; Ingrosso, G. Exploring All Avenues for Radiotherapy in Oligorecurrent Prostate Cancer Disease Limited to Lymph Nodes: A Systemic Review of the Role of Stereotactic Body Radiotherapy. Eur. Urol. Focus 2017, 3, 538–544. [Google Scholar] [CrossRef]
- Triggiani, L.; Mazzola, R.; Tomasini, D.; Bruni, A.; Alicino, G.; Matrone, F.; Bortolus, R.; Francolini, G.; Detti, B.; Magli, A.; et al. Upfront metastasis-directed therapy in oligorecurrent prostate cancer does not decrease the time from initiation of androgen deprivation therapy to castration resistance. Med. Oncol. 2021, 38, 72. [Google Scholar] [CrossRef]
- Mazzola, R.; Francolini, G.; Triggiani, L.; Napoli, G.; Cuccia, F.; Nicosia, L.; Livi, L.; Magrini, S.M.; Salgarello, M.; Alongi, F. Metastasis-directed Therapy (SBRT) Guided by PET-CT 18F-CHOLINE Versus PET-CT 68Ga-PSMA in Castration-sensitive Oligorecurrent Prostate Cancer: A Comparative Analysis of Effectiveness. Clin. Genitourin. Cancer 2021, 19, 230–236. [Google Scholar] [CrossRef]
- Mazzola, R.; Cuccia, F.; Pastorello, E.; Salgarello, M.; Francolini, G.; Livi, L.; Triggiani, L.; Magrini, S.M.; Ingrosso, G.; Aristei, C.; et al. PSMA-guided metastases directed therapy for bone castration sensitive oligometastatic prostate cancer: A multi-institutional study. Clin. Exp. Metastasis 2022, 39, 443–448. [Google Scholar] [CrossRef]
- Decaestecker, K.; Meerleer, G.D.; Ameye, F.; Fonteyne, V.; Lambert, B.; Joniau, S.; Delrue, L.; Billiet, I.; Duthoy, W.; Junius, S.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence (STOMP): Study protocol for a randomized Phase II Trial. BMC Cancer 2014, 14, 671. [Google Scholar] [CrossRef] [PubMed]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Claeys, T.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. 2018, 36, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ros, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs. Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Research Network. The Molecular Taxonomy of Primary Prostate Cancer. Cell 2015, 163, 1011–1025. [Google Scholar] [CrossRef] [PubMed]
- Foroni, C.; Zarovni, N.; Bianciardi, L.; Bernardi, S.; Triggiani, L.; Zocco, D.; Venturella, M.; Chiesi, A.; Valcamonico, F.; Berruti, A. When Less Is More: Specific Capture and Analysis of Tumor Exosomes in Plasma Increases the Sensitivity of Liquid Biopsy for Comprehensive Detection of Multiple Androgen Receptor Phenotypes in Advanced Prostate Cancer Patients. Biomedicine 2020, 8, 131. [Google Scholar] [CrossRef] [PubMed]
- Bardelli, A.; Pantel, K. Liquid Biopsies, What We Do Not Know (Yet). Cancer Cell 2017, 31, 172–179. [Google Scholar] [CrossRef]
- Shyr, D.; Liu, Q. Next generation sequencing in cancer research and clinical application. Biol. Proced. Online 2013, 15, 4. [Google Scholar] [CrossRef]
- Beltran, H.; Yelensky, R.; Frampton, G.M.; Park, K.; Downing, S.R.; MacDonald, T.Y.; Jarosz, M.; Lipson, D.; Tagawa, S.T.; Nanus, D.M.; et al. Targeted Next-generation Sequencing of Advanced Prostate Cancer Identifies Potential Therapeutic Targets and Disease Heterogeneity. Eur. Urol. 2013, 63, 920–926. [Google Scholar] [CrossRef]
- Triggiani, L.; Bardoscia, L.; Colosini, A.; Bernardi, S.; Bresciani, R.; Foroni, C.; Pasinetti, N.; Borghetti, P.; Caraffini, B.; Orizio, F.; et al. Oligometastatic prostate cancer patients stratification: A molecular signature identified by liquid biopsy. J. Clin. Oncol. 2018, 36 (Suppl. 6), TPS400. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; Bellmunt, J.; Bolla, M.; Briers, E.; De Santis, M.; Gross, T.; Henry, A.M.; Joniau, S.; Lam, T.B.; Mason, M.D.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part II: Treatment of Relapsing, Metastatic, and Castration-Resistant Prostate Cancer. Eur. Urol. 2017, 71, 630–642. [Google Scholar] [CrossRef] [PubMed]
- Van Etten, J.L.; Dehm, S.M. Clonal origin and spread of metastatic prostate cancer. Endocr. Relat. Cancer 2016, 23, R207–R217. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Farina, M.; Zanaglio, C.; Cattina, F.; Polverelli, N.; Schieppati, F.; Re, F.; Foroni, C.; Malagola, M.; Dunbar, A.J.; et al. ETV6: A Candidate Gene for Predisposition to “Blend Pedigrees”? A Case Report from the NEXT-Famly Clinical Trial. Case Rep Hematol. 2020, 2020, 2795656. [Google Scholar] [CrossRef] [PubMed]
- Arora, K.; Barbieri, C.E. Molecular Subtypes of Prostate Cancer. Curr. Oncol. Rep. 2018, 20, 58. [Google Scholar] [CrossRef]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; Attard, G.; et al. Integrative Clinical Genomics of Advanced Prostate Cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef]
- Sumanasuriya, S.; De Bono, J. Treatment of Advanced Prostate Cancer—A Review of Current Therapies and Future Promise. Cold Spring Harb. Perspect. Med. 2018, 8, a030635. [Google Scholar] [CrossRef]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef]
- Clarke, N.; Wienchno, P.; Alekseev, B.; Sala, N.; Jones, R.; Kocak, I.; Chiuri, V.E.; Jassem, J.; Flechon, A.; Redfern, C.; et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2018, 19, 975–986. [Google Scholar] [CrossRef]
- Carr, T.H.; Adelman, C.; Barnicle, A.; Kozarewa, I.; Luke, S.; Lai, Z.; Hollis, S.; Dougherty, B.; Harrington, E.A.; Kang, J.; et al. Homologous Recombination Repair Gene Mutation Characterization by Liquid Biopsy: A Phase II Trial of Olaparib and Abiraterone in Metastatic Castrate-Resistant Prostate Cancer. Cancers 2021, 13, 5830. [Google Scholar] [CrossRef]
- Zocco, D.; Bernardi, S.; Novelli, M.; Astrua, C.; Fava, P.; Zarovni, N.; Carpi, F.M.; Bianciardi, L.; Malavenda, O.; Quaglino, P.; et al. Isolation of extracellular vesicles improves the detection of mutant DNA from plasma of metastatic melanoma patients. Sci. Rep. 2020, 10, 15745. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, L.; Chapman, E.; Khoo, V.; Suh, Y.E.; Tunariu, N.; Wang, Y.; van As, N. Metastasis-directed Therapy in Prostate Cancer: Prognostic Significance of the ESTRO/EORTC Classification in Oligometastatic Bone Disease. Clin. Oncol. 2022, 34, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Stelcer, E.; Konkol, M.; Głeboka, A.; Suchorska, W.M. Liquid Biopsy in Oligometastatic Prostate Cancer—A Biologist’s Point of View. Front. Oncol. 2019, 9, 775. [Google Scholar] [CrossRef] [PubMed]
- Gorges, T.M.; Kuske, A.; Rock, K.; Mauermann, O.; Muller, V.; Peine, S.; Verpoort, K.; Novosadova, V.; Kubista, M.; Riethdorf, S.; et al. Accession of tumor heterogeneity by multiplex transcriptome profiling of single circulating tumor cells. Clin. Chem 2016, 62, 1504–1515. [Google Scholar] [CrossRef]
- Scher, H.I.; Graf, R.P.; Schreiber, N.A.; McLaughlin, B.; Jendrisak, A.; Wang, Y.; Lee, J.; Greene, S.; Krupa, R.; Lu, D.; et al. Phenotypic heterogeneity of circulating tumor cells informs clinical decisions between AR signaling inhibitors and taxanes in metastatic prostate cancer. Cancer Res. 2017, 77, 5687–5698. [Google Scholar] [CrossRef]
- Pereira, B.; Chen, C.T.; Goyal, L.; Walmsley, C.; Pinto, C.J.; Baiev, I.; Allen, R.; Henderson, L.; Saha, S.; Reyes, S.; et al. Cell-free DNA captures tumor heterogeneity and driver alterations in rapid autopsies with pre-treated metastatic cancer. Nat. Commun. 2021, 12, 3199. [Google Scholar] [CrossRef]
- Tsui, D.W.Y.; Cheng, M.L.; Shady, M.; Yang, J.L.; Stephens, D.; Won, H.; Srinivasan, P.; Huberman, K.; Meng, F.; Jing, X.; et al. Tumor fraction-guided cell-free DNA profiling in metastatic solid tumor patients. Genome Med. 2021, 13, 96. [Google Scholar] [CrossRef]
- Perkins, G.; Yap, T.A.; Pope, L.; Cassidy, A.M.; Dukes, J.P.; Riisnaes, R.; Massard, C.; Cassier, P.A.; Miranda, S.; Clark, J.; et al. Multi-Purpose Utility of Circulating Plasma DNA Testing in Patients with Advanced Cancers. PLoS ONE 2012, 7, e47020. [Google Scholar] [CrossRef]
- Tan, M.H.E.; Jun, L.I.; Xu, H.E.; Melcher, K.; Yong, E.L. Androgen receptor: Structure, role in prostate cancer and drug discovery. Acta Pharmacol. Sin. 2015, 36, 3–23. [Google Scholar] [CrossRef]
- Oh, M.; Alkhushaym, N.; Fallatah, S.; Althagafi, A.; Aljadeed, R.; Alsowaida, Y.; Jeter, J.; Martin, J.R.; Babiker, H.M.; McBride, A.; et al. The association of BRCA1 and BRCA2 mutations with prostate cancer risk, frequency, and mortality: A meta-analysis. Prostate 2019, 79, 880–895. [Google Scholar] [CrossRef]
- Annala, M.; Vandekerkhove, G.; Khalaf, D.; Taavitsainen, S.; Beja, K.; Warner, E.W.; Sunderland, K.; Kollmannsberger, C.; Eigl, B.J.; Finch, D.; et al. Criculating Tumor DNA Genomics Correlate with Resistance to Abiraterone and Enzalutamide in Prostate Cancer. Cancer Discov. 2018, 8, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.B.; Helfand, B.; Mamawala, M.; Wu, Y.; Landis, P.; HYu, H.; Wiley, K.; Na, R.; Shi, Z.; Petkewicz, J.; et al. Germline Mutations in ATM and BRCA1/2 Are Associated with Grade Reclassification in Men on Active Surveillance for Prosate Cancer. Eur. Urol. 2019, 75, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Wilhelm, B.; Dork, T.; Bremer, M.; Baumann, R.; Karstens, H.J.; Machtens, S. ATM missense variant P1054R predispose to prostate cancer. Radiother. Oncol. 2007, 83, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Pitroda, S.P.; Weichselbaum, R.R. Integrated molecular and clinical staging defines the spectrum of metastatic cancer. Nat Rev Clin. Oncol. 2019, 16, 581–588. [Google Scholar] [CrossRef]
- Bignardi, M.; Cozzi, L.; Fogliata, A.; Lattuada, P.; Mancosu, P.; Navarria, P.; Urso, G.; Vigorito, S.; Scorsetti, M. Critical appraisal of volumetric modulated arc therapy in stereotactic body radiation therapy for metastases to abdominal lymph nodes. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1570–1577. [Google Scholar] [CrossRef]
- Jereczek-Fossa, B.A.; Fariselli, L.; Beltramo, G.; Catalano, G.; Serafini, F.; Garibaldi, C.; Cambria, R.; Brait, L.; Possanzini, M.; Bianchi, L.C.; et al. Linac-based or robotic image-guided stereotactic radiotherapy for isolated lymph node recurrent prostate cancer. Radiother. Oncol. 2009, 93, 14–17. [Google Scholar] [CrossRef]
- Benedict, S.H.; Yenice, K.M.; Followill, D.; Galvin, J.M.; Hinson, W.; Kavanagh, B.; Keall, P.; Lovelock, M.; Meeks, S.; Papiez, L.; et al. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Med. Phys. 2010, 37, 4078–4101. [Google Scholar] [CrossRef]
- Bignardi, M.; Navarria, P.; Mancosu, P.; Cozzi, L.; Fogliata, A.; Tozzi, A.; Castiglioni, S.; Carnaghi, C.; Tronconi, M.C.; Santoro, A.; et al. Clinical outcome of hypofractionated stereotactic radiotherapy for abdominal lymph node metastases. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 831–838. [Google Scholar] [CrossRef]
- Alongi, F.; Fogliata, A.; Clerici, E.; Navarria, P.; Tozzi, A.; Comito, T.; Ascolese, A.M.; Clivio, A.; Lobefalo, F.; Reggiori, G.; et al. Volumetric modulated arc therapy with flattening filter free beams for isolated abdominal/pelvic lymph nodes: Report of dosimetric and early clinical results in oligometastatic patients. Radiat. Oncol. 2012, 7, 204. [Google Scholar] [CrossRef][Green Version]
- Jereczek-Fossa, B.A.; Piperno, G.; Ronchi, S.; Catalano, G.; Fodor, C.; Cambria, R.; Ing, P.F.; Gherardi, F.; Alterio, D.; Zerini, D.; et al. Linac-based stereotactic body radiotherapy for oligometastatic patients with single abdominal lymph node recurrent cancer. Am. J. Clin. Oncol. 2014, 37, 227–233. [Google Scholar] [CrossRef]
- Hanna, G.; Murray, L.; Patel, R.; Jain, S.; Aitken, K.; Franks, K.; van As, N.; Tree, A.; Hatfield, P.; Harrow, S.; et al. UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy. Clin. Oncol. 2018, 30, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE)—Version 4.0 Published: 28 May 2009 (v4.02: 15 September 2009)—U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Available online: https://www.eortc.be/services/doc/ctc/ctcae_4.03_2010-06-14_quickreference_5x7.pdf (accessed on 28 May 2009).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).