
Relationships between Osteopontin, Osteoprotegerin, and Other Extracellular Matrix Proteins in Calcifying Arteries

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Measurement of Collagens Type I–IV and Elastin Content in Aortas’ Fragments by ELISA
2.2. Measurement of OPN and OPG
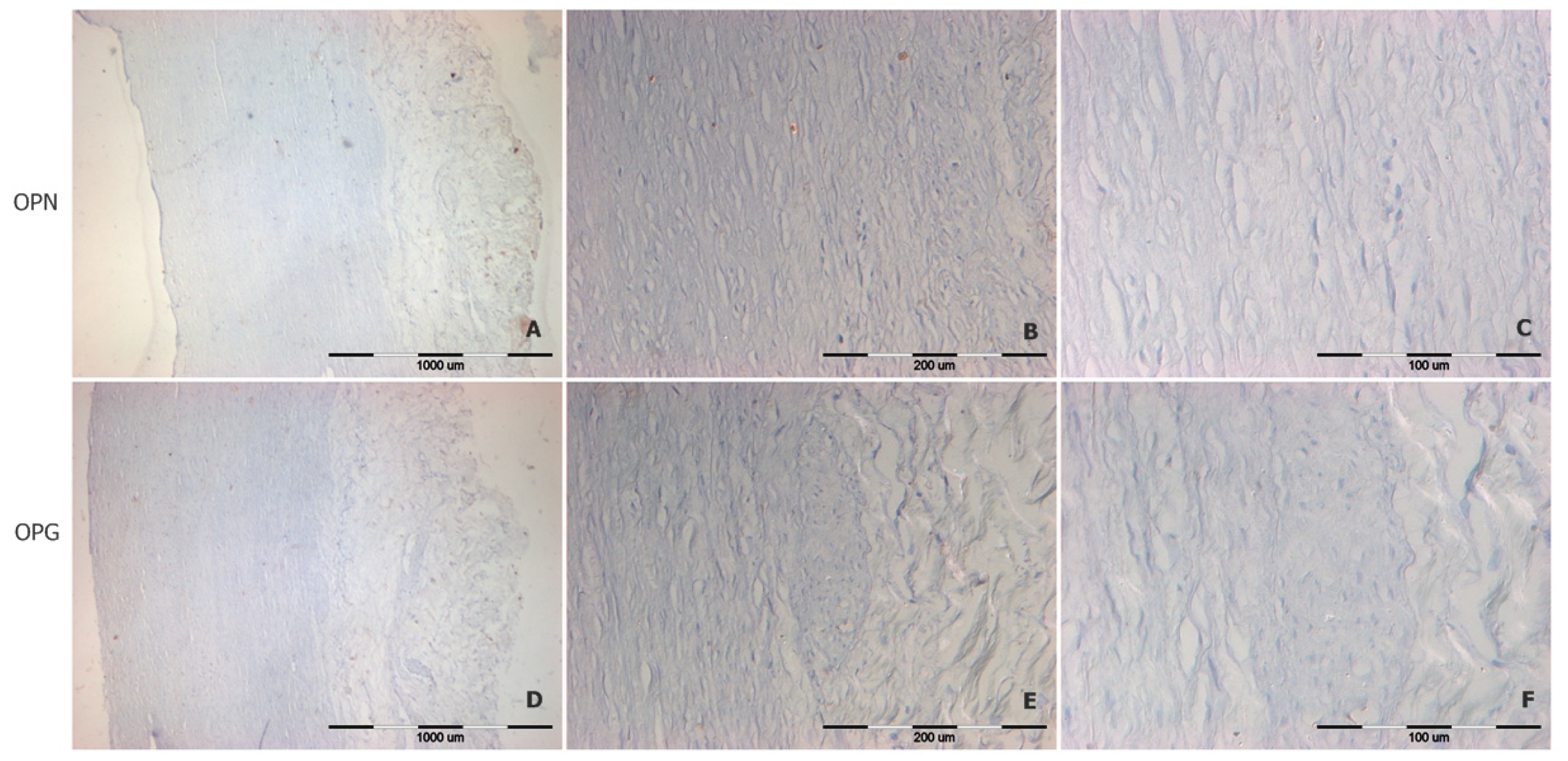
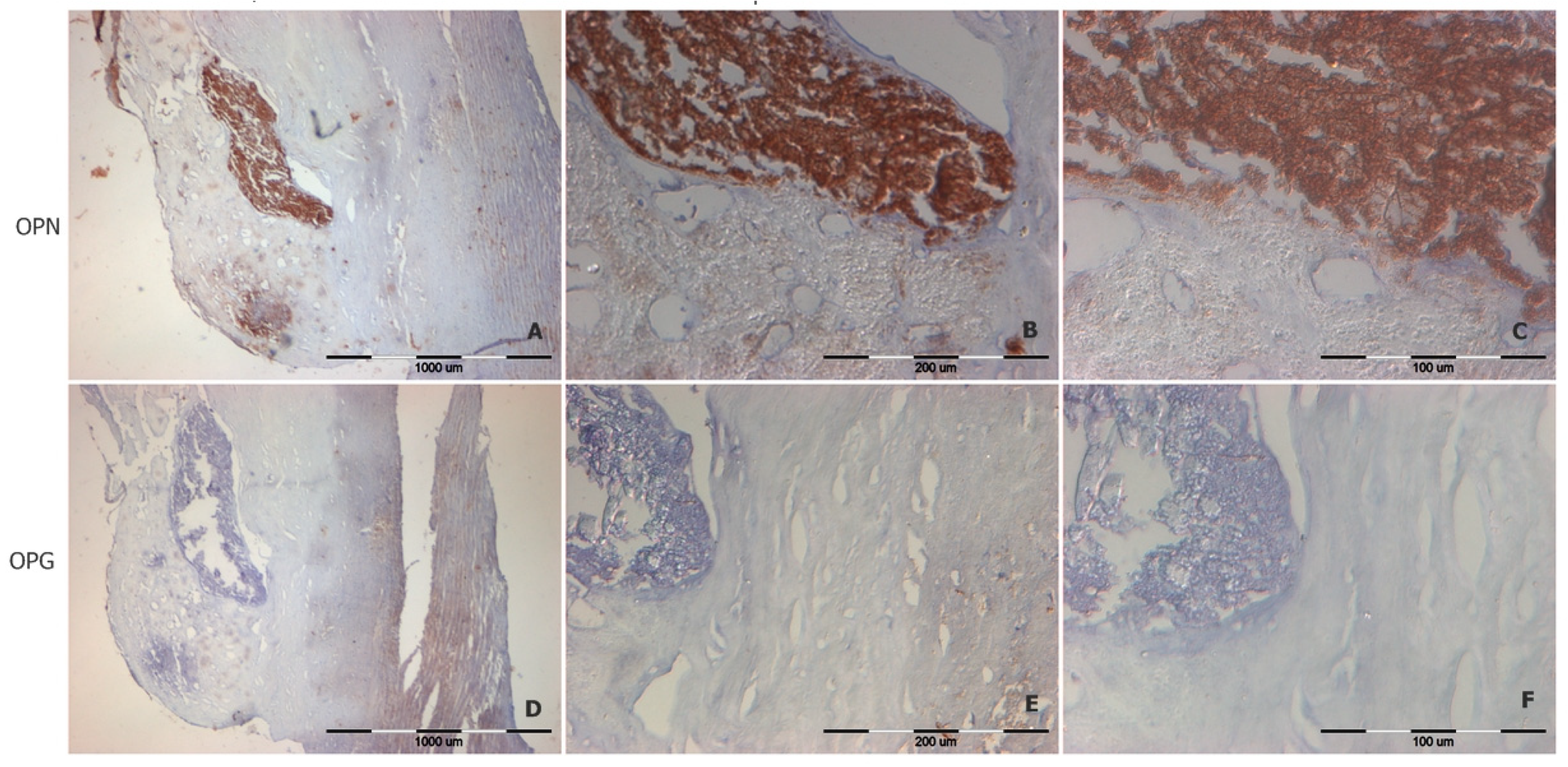
2.3. Immunohistochemical Staining of OPN and OPG
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmad, F.B.; Anderson, R.N. The Leading Causes of Death in the US for 2020. JAMA—J. Am. Med. Assoc. 2021, 325, 1829–1830. [Google Scholar] [CrossRef] [PubMed]
- Icer, M.A.; Gezmen-Karadag, M. The multiple functions and mechanisms of osteopontin. Clin. Biochem. 2018, 59, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; McCann, M.; Mangan, S.; Lam, A.; Karan, M. Osteoprotegerin and Osteopontin Are Expressed at High Concentrations Within Symptomatic Carotid Atherosclerosis. Stroke 2004, 35, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Lok, Z.S.Y.; Lyle, A.N. Osteopontin in Vascular Disease: Friend or Foe? Arterioscler. Thromb. Vasc. Biol. 2019, 39, 613. [Google Scholar] [CrossRef] [PubMed]
- Farrokhi, V.; Chabot, J.R.; Neubert, H.; Yang, Z. Assessing the Feasibility of Neutralizing Osteopontin with Various Therapeutic Antibody Modalities. Nature 2018, 8, 7781. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, Y.; Huang, Z.; Chen, X.; Zhang, B. The roles of osteoprotegerin in cancer, far beyond a bone player. Cell Death Discov. 2022, 8, 252. [Google Scholar] [CrossRef] [PubMed]
- Hetterich, H.; Webber, N.; Willner, M.; Herzen, J.; Birnbacher, L.; Hipp, A.; Marschner, M.; Auweter, S.D.; Habbel, C.; Schüller, U.; et al. AHA classification of coronary and carotid atherosclerotic plaques by grating-based phase-contrast computed tomography. Eur. Radiol. 2016, 26, 3223–3233. [Google Scholar] [CrossRef]
- Kuzan, A.; Wisniewski, J.; Maksymowicz, K.; Kobielarz, M.; Gamian, A.; Chwilkowska, A. Relationship between calcification, atherosclerosis and matrix proteins in the human aorta. Folia Histochem. Cytobiol. 2021, 59, 8–21. [Google Scholar] [CrossRef]
- Kuzan, A.; Chwiłkowska, A.; Pezowicz, C.; Witkiewicz, W.; Gamian, A.; Maksymowicz, K.; Kobielarz, M. The content of collagen type II in human arteries is correlated with the stage of atherosclerosis and calcification foci. Cardiovasc. Pathol. 2017, 28, 21–27. [Google Scholar] [CrossRef]
- Barallobre-Barreiro, J.; Loeys, B.; Mayr, M.; Rienks, M.; Verstraeten, A.; Kovacic, J.C. Extracellular Matrix in Vascular Disease, Part 2/4: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 2189–2203. [Google Scholar] [CrossRef]
- Mammoto, A.; Matus, K.; Mammoto, T. Extracellular Matrix in Aging Aorta. Front. Cell Dev. Biol. 2022, 10, 367. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Shi, G.-P. Vascular wall extracellular matrix proteins and vascular diseases. Biochim. Biophys. Acta 2014, 1842, 2106–2119. [Google Scholar] [CrossRef]
- Tousoulis, D.; Siasos, G.; Maniatis, K.; Oikonomou, E.; Kioufis, S.; Zaromitidou, M.; Paraskevopoulos, T.; Michalea, S.; Kollia, C.; Miliou, A.; et al. Serum osteoprotegerin and osteopontin levels are associated with arterial stiffness and the presence and severity of coronary artery disease. Int. J. Cardiol. 2013, 167, 1924–1928. [Google Scholar] [CrossRef] [PubMed]
- Cottin, Y.; Issa, R.; Benalia, M.; Mouhat, B.; Meloux, A.; Tribouillard, L.; Bichat, F.; Rochette, L.; Vergely, C.; Zeller, M. Association between Serum Osteoprotegerin Levels and Severity of Coronary Artery Disease in Patients with Acute Myocardial Infarction. J. Clin. Med. 2021, 10, 4326. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.E.; Kapetanios, D.; Korakas, E.; Valsami, G.; Tentolouris, N.; Papanas, N.; Lambadiari, V.; Karkos, C. Association of serum levels of osteopontin and osteoprotegerin with adverse outcomes after endovascular revascularisation in peripheral artery disease. Cardiovasc. Diabetol. 2022, 21, 171. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.F.; Wu, S.; Juang, J.J.; Chiang, F.T.; Hsu, L.A.; Teng, M.S.; Cheng, S.T.; Huang, H.L.; Ko, Y.L. Osteoprotegerin and osteopontin levels, but not gene polymorphisms, predict mortality in cardiovascular diseases. Biomark. Med. 2019, 13, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Stępień, E.; Wypasek, E.; Stopyra, K.; Konieczyńska, M.; Przybyło, M.; Pasowicz, M. Increased levels of bone remodeling biomarkers (osteoprotegerin and osteopontin) in hypertensive individuals. Clin. Biochem. 2011, 44, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Basiak, M.; Hachula, M.; Kosowski, M.; Machnik, G.; Maliglowka, M.; Dziubinska-Basiak, M.; Krysiak, R.; Okopien, B. The Effect of PCSK9 Inhibition on the Stabilization of Atherosclerotic Plaque Determined by Biochemical and Diagnostic Imaging Methods. Molecules 2023, 28, 5928. [Google Scholar] [CrossRef] [PubMed]
- Kuzan, A.; Królewicz, E.; Nowakowska, K.; Stach, K.; Kaliszewski, K.; Domosławski, P.; Kotyra, Ł.; Gamian, A.; Kustrzeba-Wójcicka, I. Contribution of Glycation and Oxidative Stress to Thyroid Gland Pathology—A Pilot Study. Biomolecules 2021, 11, 557. [Google Scholar] [CrossRef] [PubMed]
- Wolak, T. Osteopontin—A multi-modal marker and mediator in atherosclerotic vascular disease. Atherosclerosis 2014, 236, 327–337. [Google Scholar] [CrossRef]
- Strobescu-Ciobanu, C.; Giuşcă, S.E.; Căruntu, I.D.; Amălinei, C.; Rusu, A.; Cojocaru, E.; Popa, R.F.; Lupaşcu, C.D. Osteopontin and osteoprotegerin in atherosclerotic plaque—Are they significant markers of plaque vulnerability? Rom. J. Morphol. Embryol. 2020, 61, 793. [Google Scholar] [CrossRef] [PubMed]
- Higgins, C.L.; Isbilir, S.; Basto, P.; Chen, I.Y.; Vaduganathan, M.; Vaduganathan, P.; Reardon, M.J.; Lawrie, G.; Peterson, L.; Morrisett, J.D. Distribution of alkaline phosphatase, osteopontin, RANK ligand and osteoprotegerin in calcified human carotid atheroma. Protein J. 2015, 34, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Giachelli, C.M.; Speer, M.Y.; Li, X.; Rajachar, R.M.; Yang, H. Regulation of vascular calcification: Roles of phosphate and osteopontin. Circ. Res. 2005, 96, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; McKee, M.D.; Steitz, S.; Giachelli, C.M. Calcification of vascular smooth muscle cell cultures: Inhibition by osteopontin. Circ. Res. 1999, 84, 166–178. [Google Scholar] [CrossRef] [PubMed]
- Özkalaycı, F.; Gülmez, Ö.; Uğur-Altun, B.; Pandi-Perumal, S.R.; Altun, A. The Role of Osteoprotegerin as a Cardioprotective Versus Reactive Inflammatory Marker: The Chicken or the Egg Paradox. Balkan Med. J. 2018, 35, 225. [Google Scholar] [CrossRef] [PubMed]
- Scialla, J.J.; Leonard, M.B.; Townsend, R.R.; Appel, L.; Wolf, M.; Budoff, M.J.; Chen, J.; Lustigova, E.; Gadegbeku, C.A.; Glenn, M.; et al. Correlates of osteoprotegerin and association with aortic pulse wave velocity in patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2011, 6, 2612–2619. [Google Scholar] [CrossRef] [PubMed]
- Csiky, B.; Sági, B.; Peti, A.; Lakatos, O.; Prémusz, V.; Sulyok, E. The Impact of Osteocalcin, Osteoprotegerin and Osteopontin on Arterial Stiffness in Chronic Renal Failure Patients on Hemodialysis. Kidney Blood Press. Res. 2017, 42, 1312–1321. [Google Scholar] [CrossRef] [PubMed]
- Nawaz, S.S.; Siddiqui, K.; Mujammami, M.; Alotaibi, O.; Alanazi, S.S.; Rafiullah, M. Determinant of Osteopontin Levels in Microvascular Complications in Patients with Diabetes. Int. J. Gen. Med. 2022, 15, 4433–4440. [Google Scholar] [CrossRef]
- Weber, A.; L Büttner, A.; Rellecke, P.; Petrov, G.; Albert, A.; Sixt, S.U.; Lichtenberg, A.; Akhyari, P. Osteopontin as novel biomarker for reversibility of pressure overload induced left ventricular hypertrophy. Biomark. Med. 2020, 14, 513–523. [Google Scholar] [CrossRef]
- Sbarouni, E.; Georgiadou, P.; Chatzikyriakou, S.; Analitis, A.; Chaidaroglou, A.; Degiannis, D.; Voudris, V. Osteopontin in relation to Prognosis following Coronary Artery Bypass Graft Surgery. Dis. Markers 2016, 2016, 1868739. [Google Scholar] [CrossRef]
- Bazzichi, L.; Ghiadoni, L.; Rossi, A.; Bernardini, M.; Lanza, M.; De Feo, F.; Giacomelli, C.; Mencaroni, I.; Raimo, K.; Rossi, M.; et al. Osteopontin is associated with increased arterial stiffness in rheumatoid arthritis. Mol. Med. 2009, 15, 402–406. [Google Scholar] [CrossRef]
- Bradshaw, A.D. The role of SPARC in extracellular matrix assembly. J. Cell Commun. Signal. 2009, 3, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Hohenester, E.; Göhring, W.; Timpl, R. Crystal structure and mapping by site-directed mutagenesis of the collagen-binding epitope of an activated form of BM-40/SPARC/osteonectin. EMBO J. 1998, 17, 1625–1634. [Google Scholar] [CrossRef] [PubMed]
- Gajewska, J.; Ambroszkiewicz, J.; Laskowska-Klita, T. Osteoprotegerin and C-telopeptide of type I collagen in Polish healthy children and adolescents. Adv. Med. Sci. 2006, 51, 269–272. [Google Scholar] [PubMed]
- Meng, Y.; Tian, C.; Liu, L.; Wang, L.; Chang, Q. Elevated expression of connective tissue growth factor, osteopontin and increased collagen content in human ascending thoracic aortic aneurysms. Vascular 2014, 22, 20–27. [Google Scholar] [CrossRef]
- Cabiati, M.; Svezia, B.; Matteucci, M.; Botta, L.; Pucci, A.; Rinaldi, M.; Caselli, C.; Lionetti, V.; Del Ry, S. Myocardial Expression Analysis of Osteopontin and Its Splice Variants in Patients Affected by End-Stage Idiopathic or Ischemic Dilated Cardiomyopathy. PLoS ONE 2016, 11, e0160110. [Google Scholar] [CrossRef] [PubMed][Green Version]
- López, B.; González, A.; Lindner, D.; Westermann, D.; Ravassa, S.; Beaumont, J.; Gallego, I.; Zudaire, A.; Brugnolaro, C.; Querejeta, R.; et al. Osteopontin-mediated myocardial fibrosis in heart failure: A role for lysyl oxidase? Cardiovasc. Res. 2013, 99, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Strandjord, T.P.; Madtes, D.K.; Weiss, D.J.; Sage, E.H. Collagen accumulation is decreased in SPARC-null mice with bleomycin-induced pulmonary fibrosis. Am. J. Physiol. 1999, 277, L628–L635. [Google Scholar] [CrossRef] [PubMed]
- Carvalheiro, T.; Malvar Fernández, B.; Ottria, A.; Giovannone, B.; Marut, W.; Reedquist, K.A.; Garcia, S.; Radstake, T.R. Extracellular SPARC cooperates with TGF-β signalling to induce pro-fibrotic activation of systemic sclerosis patient dermal fibroblasts. Rheumatology 2020, 59, 2258–2263. [Google Scholar] [CrossRef]
- Rekhter, M.D. Collagen synthesis in atherosclerosis: Too much and not enough. Cardiovasc. Res. 1999, 41, 376–384. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Mean | Minimum | Maximum | Standard Dev. | |
|---|---|---|---|---|---|
| Gender [0—women; 1—men] | 100 | 0.710 | 0.000 | 1.000 | 0.456 |
| age | 101 | 55.396 | 18.000 | 90.000 | 15.868 |
| Calcification [0—no, 1—yes] | 76 | 0.408 | 0.000 | 1.000 | 0.495 |
| OPG [µg/mg of tissue] | 101 | 0.004 | 0.000 | 0.019 | 0.003 |
| OPN [µg/mg of tissue] | 100 | 0.004 | 0.000 | 0.041 | 0.006 |
| Collagen Type I [µg/mg of Tissue] | Collagen Type II [µg/mg of Tissue] | Collagen Type III [µg/mg of Tissue] | Collagen Type IV [µg/mg of Tissue] | Elastin [µg/mg of Tissue] | Age [Years] | OPG [µg/mg of Tissue] | |
|---|---|---|---|---|---|---|---|
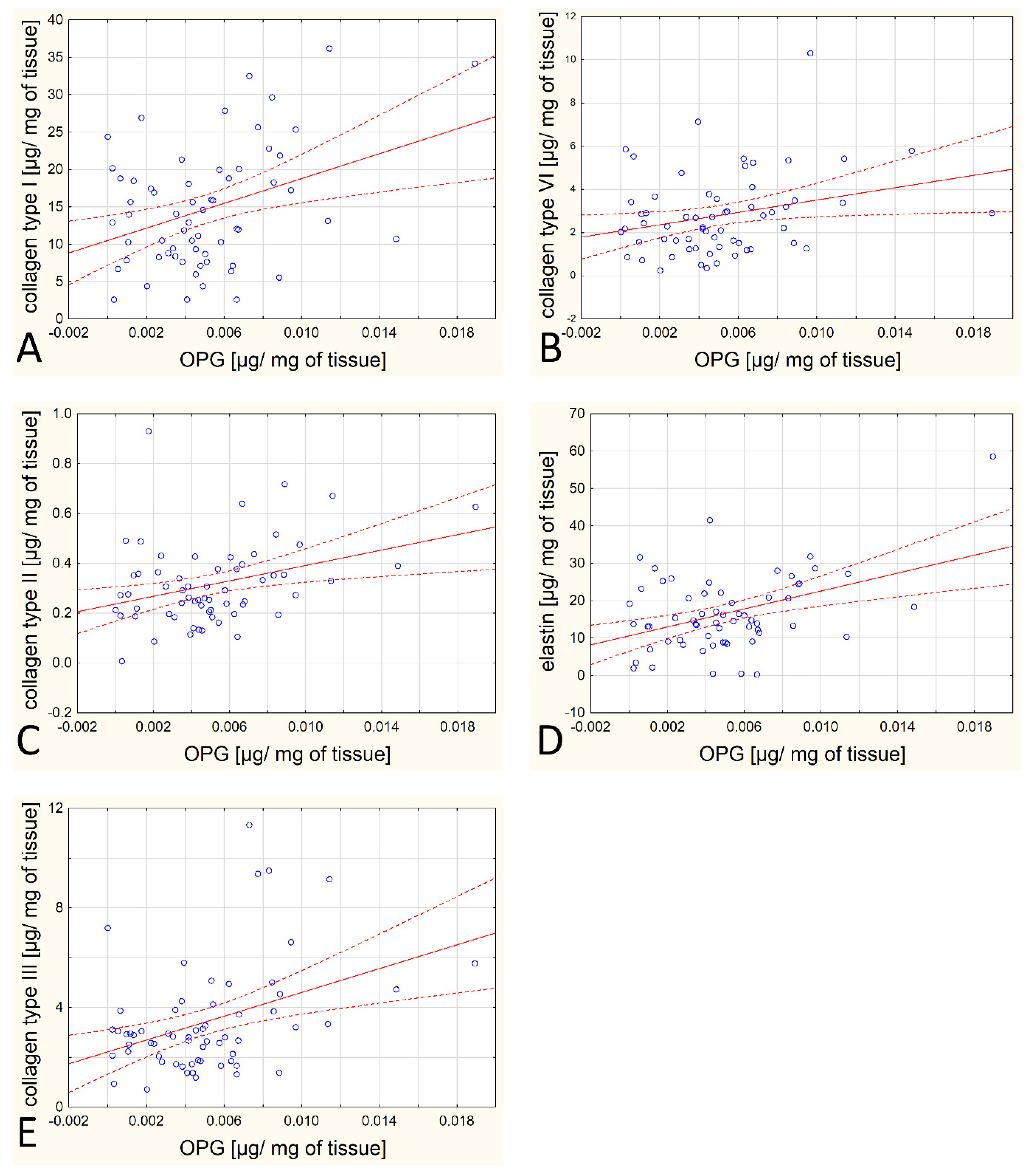
| OPG [µg/mg of tissue] | 0.3696 | 0.3378 | 0.3911 | 0.2746 | 0.4219 | −0.0817 | - |
| p = 0.003 | p = 0.007 | p = 0.002 | p = 0.031 | p = 0.001 | p = 0.528 | - | |
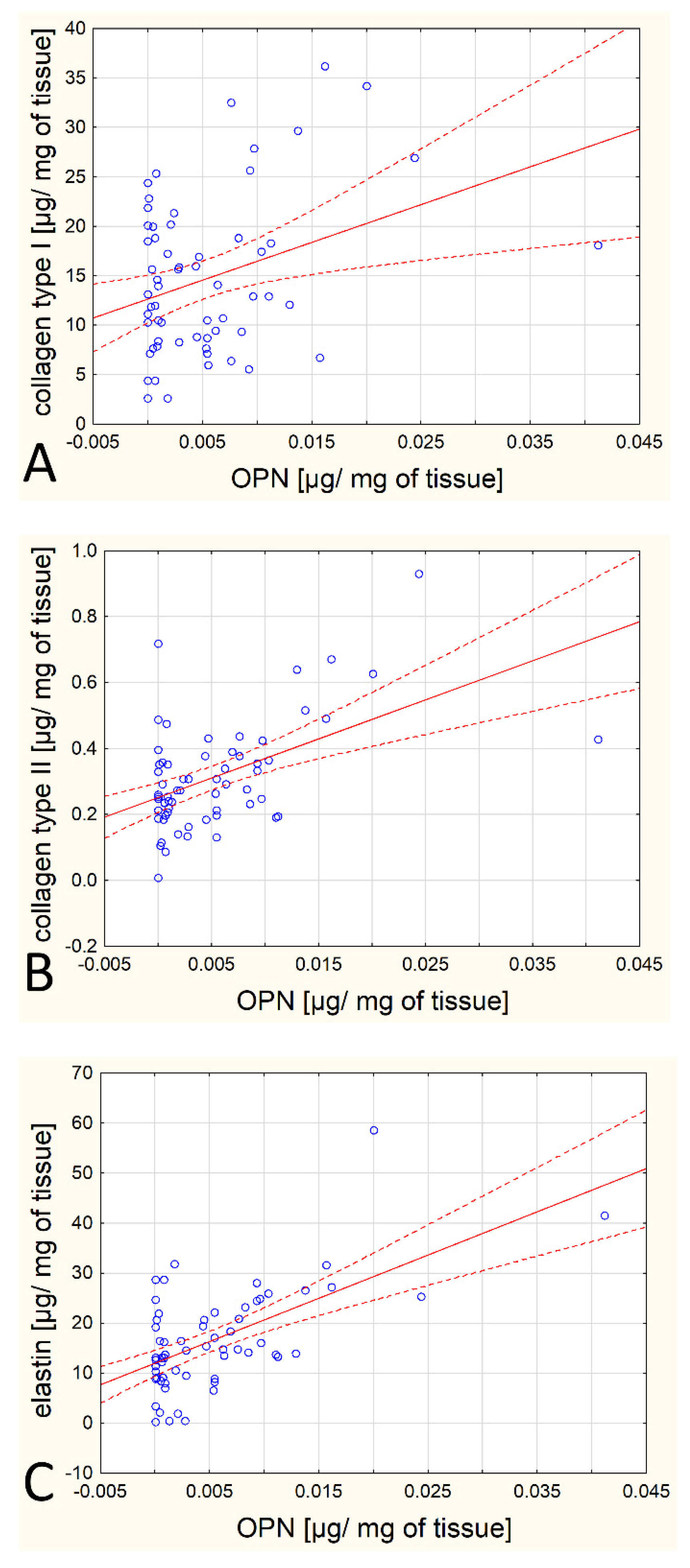
| OPN [µg/mg of tissue] | 0.3401 | 0.5172 | 0.0974 | 0.0851 | 0.6073 | 0.1072 | 0.1567 |
| p = 0.007 | p = 0.000 | p = 0.452 | p = 0.511 | p = 0.000 | p = 0.407 | p = 0.224 |
| Uncalcified | Calcified | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | 25–75 P | Mean | SD | Median | 25–75 P | p-Value | |
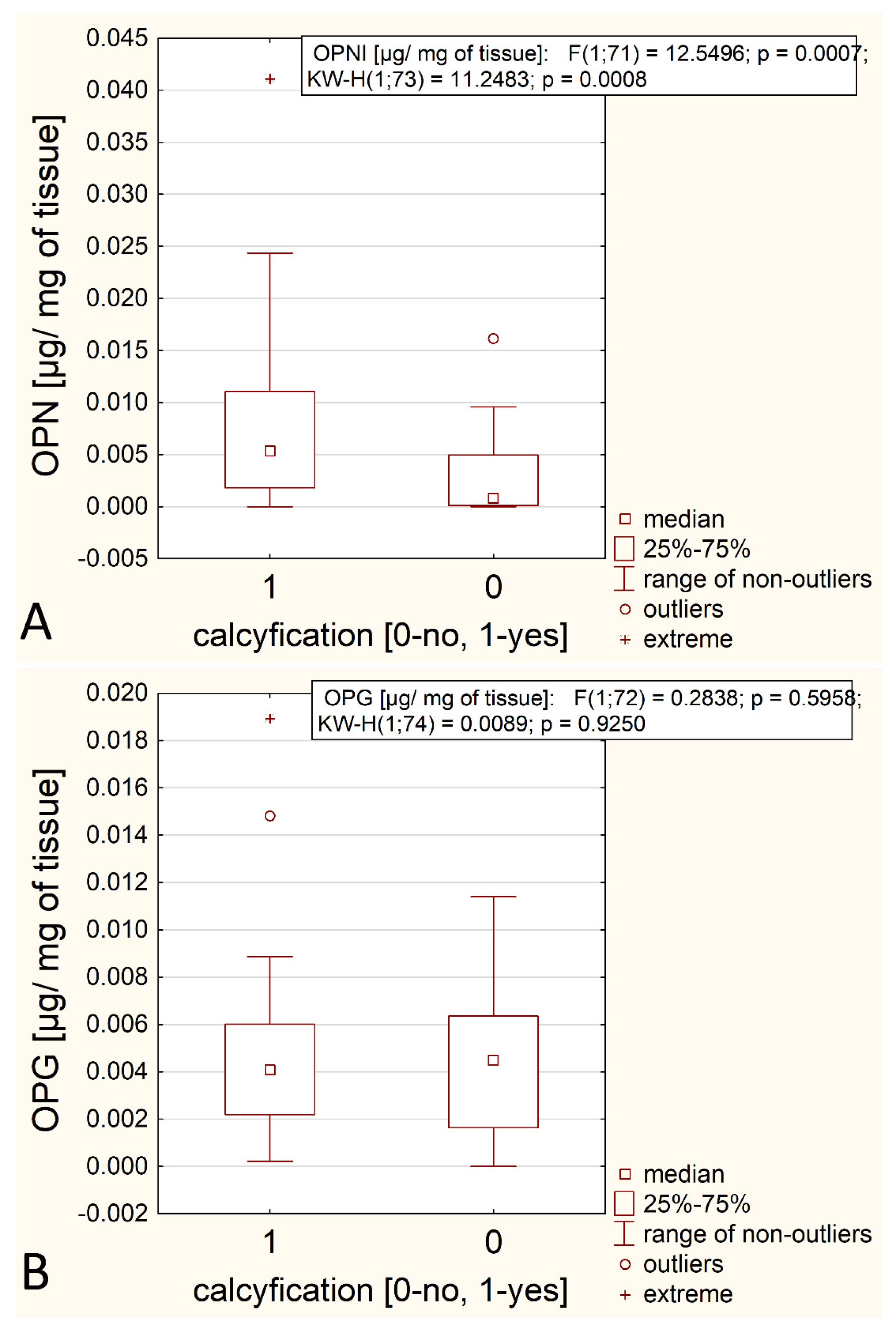
| OPG | 0.005 | 0.003 | 0.005 | 0.002–0.006 | 0.005 | 0.004 | 0.004 | 0.002–0.006 | 0.791 |
| OPN | 0.003 | 0.006 | 0.001 | 0.000–0.005 | 0.008 | 0.009 | 0.005 | 0.002–0.011 | 0.001 |
| Mean | SD | Median | 25–75 P | p-Value | ||
|---|---|---|---|---|---|---|
| OPG [µg/mg of tissue] | Artery | 0.004 | 0.005 | 0.002 | 0.001–0.006 | 0.002 |
| Calcium deposit | 0.001 | 0.004 | 0 | 0.000–0.001 | ||
| OPN [µg/mg of tissue] | Artery | 0.006 | 0.007 | 0.004 | 0.000–0.011 | 0.073 |
| Calcium deposit | 0.017 | 0.020 | 0.011 | 0.006–0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuzan, A.; Chwiłkowska, A.; Maksymowicz, K.; Abramczyk, U.; Gamian, A. Relationships between Osteopontin, Osteoprotegerin, and Other Extracellular Matrix Proteins in Calcifying Arteries. Biomedicines 2024, 12, 847. https://doi.org/10.3390/biomedicines12040847
Kuzan A, Chwiłkowska A, Maksymowicz K, Abramczyk U, Gamian A. Relationships between Osteopontin, Osteoprotegerin, and Other Extracellular Matrix Proteins in Calcifying Arteries. Biomedicines. 2024; 12(4):847. https://doi.org/10.3390/biomedicines12040847
Chicago/Turabian StyleKuzan, Aleksandra, Agnieszka Chwiłkowska, Krzysztof Maksymowicz, Urszula Abramczyk, and Andrzej Gamian. 2024. "Relationships between Osteopontin, Osteoprotegerin, and Other Extracellular Matrix Proteins in Calcifying Arteries" Biomedicines 12, no. 4: 847. https://doi.org/10.3390/biomedicines12040847
APA StyleKuzan, A., Chwiłkowska, A., Maksymowicz, K., Abramczyk, U., & Gamian, A. (2024). Relationships between Osteopontin, Osteoprotegerin, and Other Extracellular Matrix Proteins in Calcifying Arteries. Biomedicines, 12(4), 847. https://doi.org/10.3390/biomedicines12040847